
Abstract
A 33-year-old female was admitted for community-acquired pneumonia. On presentation, she was tachypneic and tachycardic and leukocytosis at 28,900/µL. Chest imaging showed dense consolidation on the right upper lobe. Due to refractory worsening respiratory failure, she was intubated with mechanical ventilation. Initial bronchoscopy with culture data was negative. Extracorporeal membrane oxygenation was pursued on the fourth day. Repeat bronchoscopy revealed targetoid ulcerative lesions with erythema in the right middle, lower lobes and left lower lobe. We describe a case of herpes simplex virus pneumonia in an immunocompetent patient that occurred in the setting of acute bacterial infection.
Introduction
Herpes simplex virus type 1 (HSV-1) and type 2 are prevalent pathogens in humans, with more than half a million new cases reported in the United States annually. 1 Viruses are the third most common cause of community-acquired pneumonia. 2 Herpes simplex virus (HSV) can affect both upper and lower respiratory tract. The upper airway infection due to viral organisms such as HSV is more common than the lower respiratory tract and has an incidence rate ranging from 6% to 12%. 2 However, HSV infection of the lower respiratory tract is rare 2 and although ubiquitous, the virus can manifest as a life-threatening illness in immunocompetent hosts. The presentation of severe disease may mimic other common conditions, placing patients with severe HSV infection at high risk of delays in appropriate treatment. Some autopsy studies have estimated that the incidence of lower respiratory tract HSV infection is as low as 0.5% in critically ill patients. 2 One published study of a small number of cases has shown that the patient mortality in HSV pneumonia is high. 3 In addition, it may be a secondary complication of an acute illness from another etiology.
Case presentation
A 33-year-old female with a medical history of asthma and depression presented to the emergency department with a 3-day history of shortness of breath. She reported her shortness of breath occurred at rest and was worse with exertion. She had a cough productive of yellow sputum and a fever of 105° Fahrenheit at home. She reported nausea, vomiting, and anorexia. She denied recent infections, travel, or sick contact. On presentation, her vital signs were as follows: temperature of 98.8° Fahrenheit, heart rate of 117 beats per minute (bpm), blood pressure 86/43 millimeters of mercury (mmHg), respiratory rate of 20 per minute, and oxygen saturation of 97% on 2 l via a nasal cannula. Physical examination at the time of admission revealed a well-developed female patient who was not in any distress. Her oropharynx appeared non-erythematous, and her neck was supple, without cervical lymphadenopathy. She was tachypneic and had crackles in the right posterior lung field, without wheezing. She was tachycardic without murmurs, rubs, or gallops. No rashes or skin lesions were observed. She was neurologically intact.
Initial laboratory results showed an elevated white blood cell count of 28,900/µL, with 83% neutrophils and 7% bands. Her hemoglobin was 12.5 milligrams/dL, and her platelet count was 375,000 platelets per microliter (mcL). The results of the comprehensive metabolic panel were unremarkable. Other laboratory values included a lactic acid of 3.1 mmol/L, an arterial blood gas significant for a pH of 7.4, PaCO2 of 38 mmHg, PaO2 of 98.0 mmHg, and bicarbonate of 24 milliequivalents per liter (mEq/L). Influenza A and B and COVID-19 were all negative. Chest radiography on admission revealed dense consolidation in the right upper lobe (Figure 1).

Chest radiograph with red arrow showing dense consolidation in the right upper lobe.
Chest computed tomography angiography confirmed severe dense consolidation involving the entire right upper lobe with air bronchograms and patchy consolidations in the right middle and lower lobes (Figure 2). Sepsis protocol was initiated, with fluid resuscitation and norepinephrine infusion. Vancomycin, cefepime, and azithromycin were chosen for empiric coverage. The patient was admitted to the ICU.

Computed tomography angiogram of chest with red arrow showing severe dense consolidation involving the entire right upper lobe with air bronchograms and patchy consolidations in the right middle and lower lobes.
Over the next 4 days, respiratory failure continued to worsen, with persistent leukocytosis. Blood and sputum cultures and urine Legionella antigen were negative. The urine streptococcal antigen test result was positive, confirming a diagnosis of streptococcal pneumonia. A repeat chest radiograph on day 5 showed worsening dense right-sided pneumonia and contralateral consolidation in the left lower lung fields, suggesting worsening pneumonia (Figure 3). She was intubated with mechanical ventilation on a lung-protective strategy in a prone position due to persistent hypoxia. Sedatives, paralytics, and analgesic medications were administered. A bronchoscopy was performed at the bedside to evaluate the worsening clinical state, which showed inflamed mucosa without purulence, lesions, or blood. Bronchoalveolar lavage (BAL) tissue was sent for pathology for routine bacterial culture, fungal staining, and acid-fast bacilli (AFB) staining, which were all negative. The intranuclear inclusions BAL fluid or tissue biopsy were not sent. The HIV test was negative. 2D echocardiogram showed ejection fraction of 55%–60% without any other valve pathology or pericardial effusion. Patient remained in intensive care unit for worsening clinical status and persistent hypoxia. On day 8 of admission, a repeat chest radiograph showed a complete whiteout of both lungs with worsening acute respiratory distress syndrome (ARDS) with poor alveolar recruitment. The PaO2/FiO2 ratio was 98 making it severe ARDS. Extracorporeal membrane oxygenation (ECMO) was performed to allow the lungs to recover. The patient was successfully cannulated for venovenous ECMO with femoral-femoral access under fluoroscopy. Our patient was ventilated on a lung protective setting per ARDS net protocol with a tidal volume of 4–6 ml/kilogram of ideal body weight, positive end-expiratory pressure of 5, Fio2 of 50%, and respiratory rate of 20 as the initial setting. ECMO was managed via cardiothoracic surgery with a pulmonary critical care team and daily circuit checks. Despite broad-spectrum antibiotics, systemic steroids, and vasopressors, the patient showed no meaningful recovery over the next several days. Repeat bronchoscopy revealed targetoid ulcerative lesions, and mild erythema in the right middle and lower lobes. The left lower lobe had significant erythema, edema, and narrowing of the left main-stem bronchus with similar lesions (Figures 4–6). Serum HSV PCR results were positive for HSV deoxyribonucleic acid. The BAL fluid was not checked for a Polymerase chain reaction (PCR) for herpes simplex and revealed mixed inflammatory cells with 60% neutrophils, 25% macrophages, and 15% lymphocytes. The procedure did not include tissue biopsies and histology as serum HSV PCR was positive with bronchoscopic evidence of targetoid lesions. Empirically, we started broad antiviral treatment with ganciclovir for viral pneumonia. The tissue was negative for Gram staining, AFB staining, fungal staining, Epstein-Barr virus, and cytomegalovirus. On reexamination, there were no intraoral, vulvar, perianal, or cutaneous vesicles typical of HSV. The antiviral therapy was changed to acyclovir to target HSV. Despite these interventions, the patient did not show any meaningful improvement and developed multiorgan failure. The family ultimately chose to pursue comfort measures, and the patient died.

Chest radiograph with red arrow showing dense consolidation in the entire right lung field and contralateral consolidation in the left lower lung field.

Bronchoscopic images showing targetoid ulcerative lesions, erythema in the right middle and lower lobes.
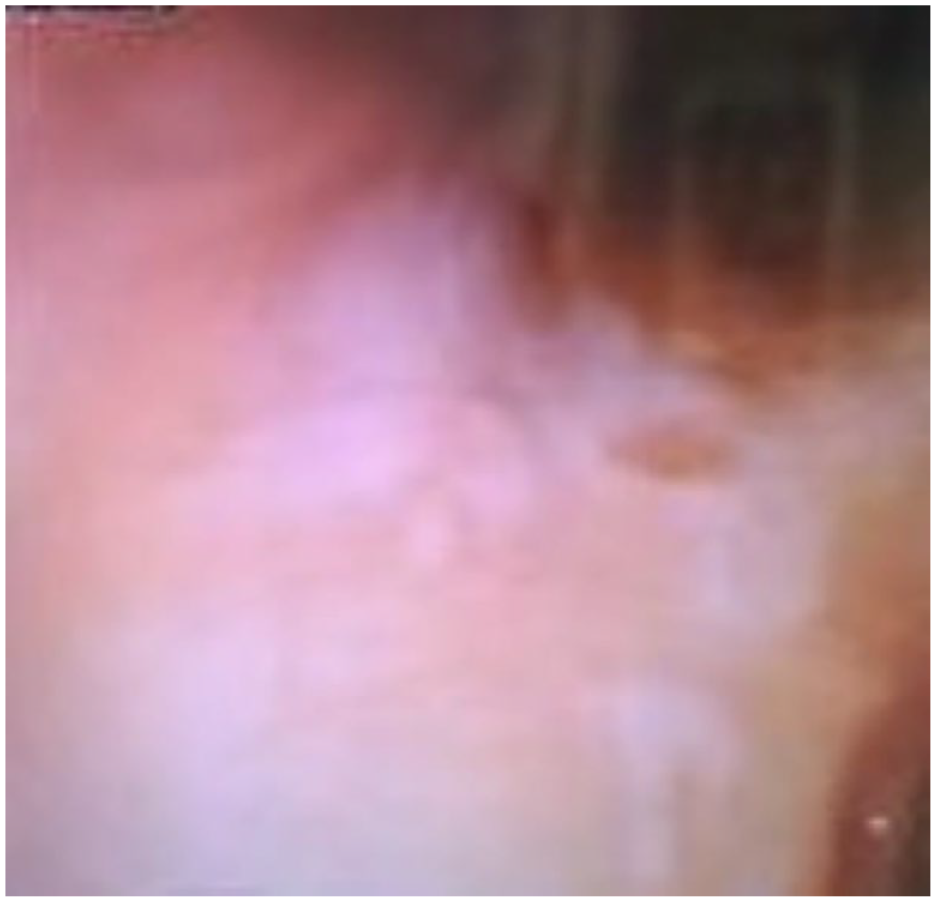
Bronchoscopic images showing targetoid ulcerative lesions, erythema in the right middle and lower lobes.

The left lower lobe had significant erythema, edema, and narrowing of the left main-stem bronchus with similar lesions.
Discussion
HSV pneumonia tends to occur in pre-existing lung disease, airway trauma, inhalational lung injury, or immunocompromized state.2,4 Development of this entity is rare in immunocompetent patients. 2 In our patient’s case, pre-existing, previously clinically irrelevant HSV was probably reactivated in the setting of acute bacterial pneumonia, causing secondary HSV pneumonia.
The incidence of HSV-1 reactivation is as high as 32%–68% in patients admitted to the ICU in the setting of septic shock, even in immunocompetent patients. Active external HSV mucosal lesions are not always detected on examination, making the diagnosis challenging. Reactivation of HSV can be associated with a nearly two-fold increase in in-hospital mortality (41% vs. 24%, p = 0.002). 5 HSV can be confirmed by PCR of sputum and is a more sensitive modality than other diagnostic methods such as serologic assays, cultures, and antigen detection. 6 Radiographic changes can include ground-glass opacities with consolidations, but a definitive consensus is yet to be reached regarding any characteristic pattern on imaging. 7 Intranuclear inclusion bodies and HSV-positive immunohistochemical staining can be detected via biopsy. The targetoid ulcerative lesions can be observed endoscopically and are classically not associated with purulent secretions. Here, the diagnosis was based on endoscopic findings of lesions typical of HSV, positive serum HSV PCR, and evidence of no improvement with broad-spectrum antibiotics. There is a significantly higher mortality in viral reactivation in ICUs with a greater mechanical ventilator time and a longer length of hospital stay. 8 Generally, using invasive therapy like ECMO can increase the risk of respiratory infections. There are reported cases of herpes simplex pneumonia in patients who have required ECMO. 9 One narrative review has reported that the prevalence of hospital-acquired infection is 10%–12% relatively frequent in patients requiring ECMO compared to other critically ill patients. 10 There is no evidence of HSV infection and increasing Fio2 requirements. We recommend that patients with a history of HSV should undergo a PCR laboratory investigation on admission. If the bronchoscopic procedure is required, we recommend tissue biopsy, histology, and PCR test from BAL fluid. Acyclovir use has been shown to improve morbidity with reduced ventilator time and vasopressor use in ICU. Despite this evidence, there are currently no specific guidelines for recognizing and treating this complication. 8
Conclusion
HSV reactivation can occur during acute illness, especially in patients with severe burns, a history of trauma, those requiring mechanical ventilation, or those on ECMO. HSV pneumonia can also be acquired by contiguous spread, aspiration, vagal nerve, and hematogenous spread. Our patient had streptococcal pneumonia, evidenced by lung consolidation and a positive urine streptococcal antigen, and later developed HSV pneumonia, most likely due to reactivation of the virus in the setting of acute illness. Antivirals can be effective in cases where viral pneumonia is suspected but are generally not recommended prophylactically when there is no evidence of viral pneumonia. Differential diagnosis should include viral pneumonia when patients do not follow the trajectory of improvement, even if they are immunocompetent. Herein, we describe an exceptional case of HSV-1 reactivation induced by septic shock. As the mortality rate is high, more studies and guidelines are needed to further define the role and duration of antiviral therapy in intensive care settings.
Footnotes
Acknowledgements
All the authors participated equally in the research and preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.