
Abstract
Anti-N-methyl-
Introduction
Anti-N-methyl-
Case report
A 22-year-old female student, with no known previous illness or hospitalization presented to our centre with an acute onset of abnormal behaviour and movement. She presented with a 1-day history of orofacial dyskinesia and incoherent speech, which later progressed to mutism. These symptoms were preceded by a 1-week history of fever and lethargy, for which she did not seek medical attention. Upon arrival, she was found to be sub-febrile, with a temperature of 37.2°C, blood pressure of 119/75 mm Hg, and a heart rate of 103 bpm. She was comfortable on room air. She exhibited occasional orofacial dyskinesia and inappropriate laughter. The remaining neurological examination was normal, with no signs of meningism. Initial laboratory investigations showed a raised white cell count (WCC) of 12 × 109/L with mixed neutrophilic and lymphocytic predominance, normal renal profile, and normal thyroid function tests. C-reactive protein (CRP) was 5 mg/L, and the erythrocyte sedimentation rate was only 35 mm/h. Urine toxicology tests were negative.
She was admitted and treated as meningoencephalitis, with adequate intravenous antibiotics and antiviral cover. Urgent cranial computed tomography (CT) showed no obvious abnormality; therefore, a lumbar puncture was performed, revealing a high opening pressure of 45 mm H2O, presumably secondary to inflammation of the central nervous system. The cerebrospinal fluid (CSF) total protein was 351 mg/dL, glucose 3.7 mmol/L (serum glucose 7.2 mmol/L), and a cell count of zero. Culture and sensitivity yielded no growth, while polymerase chain reaction (PCR) testing for herpes virus 1 and 2, as well as enterovirus was negative. Venereal disease research laboratory (VDRL) and tests for acid-fast bacilli (AFB) of the CSF were also negative. Infective screening for hepatitis B, C, and human immunodeficiency virus (HIV) was also negative.
The patient did not respond well to treatment with antibiotics and viral cover (IV ceftriaxone 2 g bd and IV acyclovir 500 mg tds), with non-resolution of the clinical symptoms. A psychiatric assessment was done, with concurrent arrangement of a magnetic resonance imaging (MRI) of the brain. The brain MRI showed areas of T2/FLAIR hyperintensity of the right temporal lobe, concerning for herpes simplex virus (HSV) encephalitis (Figure 1). Due to the discrepancy between the clinical findings and imaging, we had an electroencephalogram (EEG) done, showing generalized slow waves with no alpha waves – which is non-specific. The parents did not consent for a repeat lumbar puncture (LP) for a CSF NMDAR antibody analysis, but the serum for NMDAR antibody came back positive, with a titre of 1:10. We then commenced IV methylprednisolone and IV immunoglobulin. Extensive imaging via ultrasound (US) and CT was carried out to locate an associated neoplasm – both being negative. A pelvic MRI was then pursued, revealing fat signal intensity within both ovaries, suspicious of teratoma (Figure 2).

Brain MRI images, in axial section, showing (a) hyperintense foci (white arrows) are seen at the right temporal lobe on the FLAIR sequence and (b) T2-weighted image, at the same slice, showing hyperintense foci (white arrows).
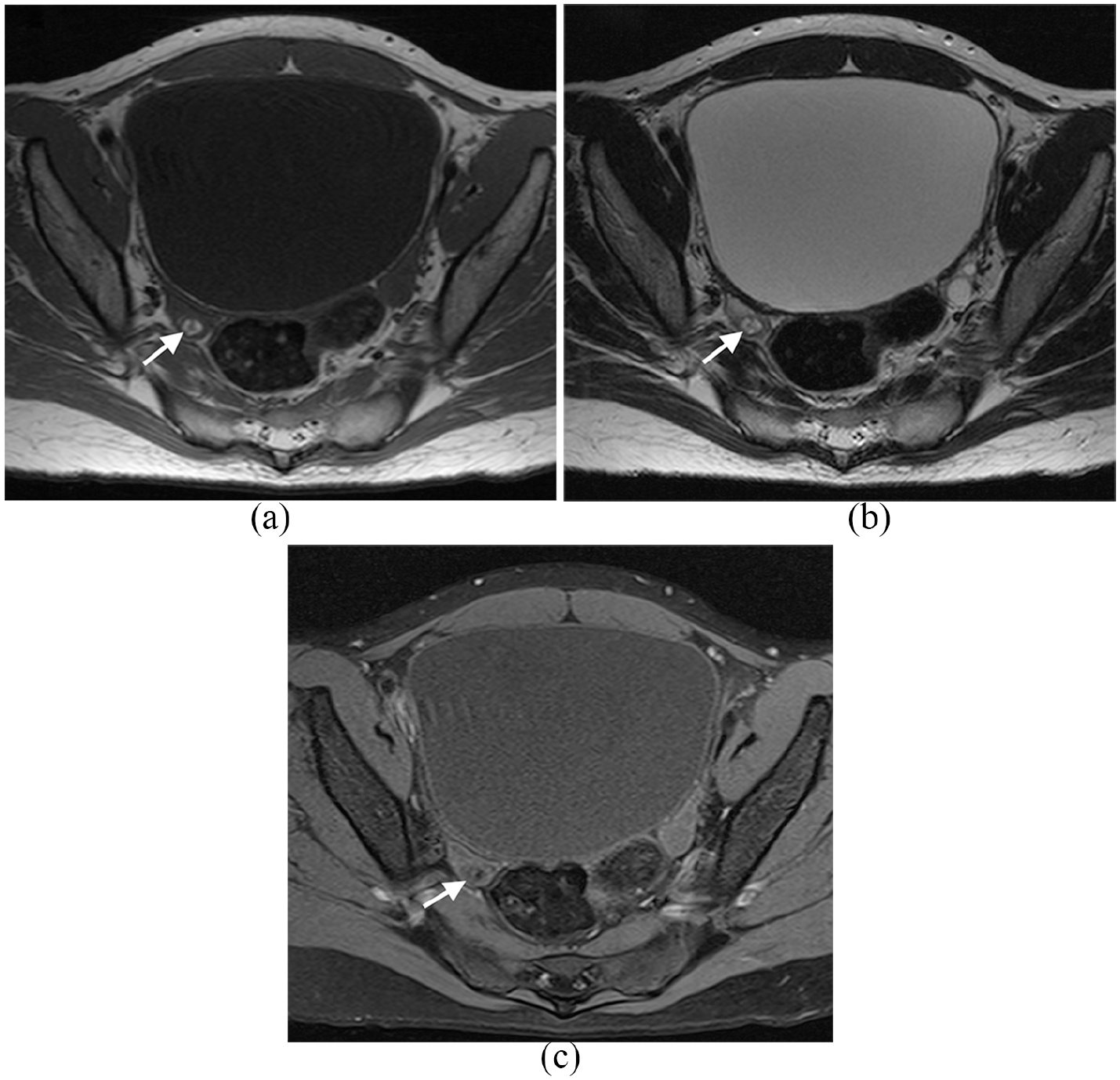
Pelvic MRI images, in axial section, showing the right ovary lesion (left ovarian lesion not demonstrated at this level) (a) and (b) – (a) T1- and (b) T2-weighted images showing focal hyperintensity within the right ovary, which is suspicious for a fat density lesion, possibly a teratoma. (c) T1 fat-suppressed sequence image of the right ovary, showing suppression of the right ovarian lesion signal intensity, confirming a fat density lesion. Surgical resection and pathological examination confirmed a teratoma.
The parents were counselled regarding surgery and fertility preservation, to which they consented. Intraoperatively, bilateral ovarian lesions were found, measuring approximately 1.0 cm × 1.0 cm and 1.0 cm × 0.5 cm on the right and left ovaries, respectively. Bilateral cystectomy was performed, and the histopathological examination confirmed the diagnosis of bilateral mature ovarian teratoma (Figure 3). As margins were complete, with the benign nature of the neoplasm, no adjunct chemotherapy was initiated. Directly after treatment with steroids and IVIG, improvement in the patient’s autonomic dysfunction and cessation of the orofacial dyskinesia were seen; however, her cognition was still limited. Secondary immunosuppression with rituximab was then commenced instead of cyclophosphamide, to avoid the teratogenic effects imposed by cyclophosphamide. At 1-year post treatment, she was able to get to Montreal Cognitive Assessment (MoCA) scale 9 score of 29/30. No baseline MoCA scoring was done, as she was uncooperative during the acute phase of the illness.

(a) Mature cystic teratoma lined by keratinised stratified squamous epithelium with underlying mature skin adnexal structures, adipose tissue, and glial tissue (H&E, ×20). (b) Mature glial tissue (arrow) with mature skin adnexal structures (arrowheads) and mature adipose tissue (fat). No immature neuroepithelial tissue is seen (H&E, ×100). (c) GFAP (glial fibrillary acidic protein) stain highlights the glial tissue (arrow) (GFAP, ×100).
Discussion
Anti-NMDAR encephalitis is the most common cause of autoimmune encephalitis after acute disseminated encephalomyelitis (ADEM). 6 Due to the heterogeneous clinical manifestation, diagnosis is often missed in the early stages. It is important to bear in mind the significant neuropsychiatric symptoms in this disease, which can be striking. As with encephalitis due to other causes, a non-specific prodrome – including low-grade fever, headache, and lethargy may be present. The patient may subsequently develop cognitive dysfunction, memory loss, which can quickly progress to motor dysfunctions such as epileptic seizures and orofacial dyskinesia. 10 Psychiatric symptoms such as agitation, delusions, hallucinations, emotional lability, and catatonia may ensue.10,11 As patients usually present first to the psychiatrists, early diagnosis may be missed, precluding appropriate treatment. Late diagnosis, without treatment, renders patients prone to autonomic instability, most commonly in the form of hypoventilation, necessitating invasive ventilation. 2
In our patient, however, alternative diagnoses were considered after seeing no clinical response despite institution of appropriate treatment. Imaging via MRI, as well as an EEG, was arranged to aid the diagnosis. The MRI showed a right temporal lobe lesion, while diffuse slow waves were seen on the EEG. Incongruence between the MRI and EEG findings was observed; the MRI findings were compatible with HSV encephalitis, whereas the EEG pattern observed was abnormal, but non-specific. In essence, our patient fits the probable criteria for the diagnosis of anti-NMDAR encephalitis, presenting with psychiatric symptoms, speech dysfunction, orofacial dyskinesia, decreased consciousness, and autonomic instability (tachycardia up to 130–140 bpm). The thyroid function test was normal, while the electrocardiogram only showed sinus tachycardia. We were unable to send Ig-G anti-GluN1 (glutamate receptor ionotropic, NMDA 1) as the patient or family did not consent to blood taking.
In the literature, approximately 95% of positive MRI findings in patients with HSV encephalitis are found in the temporal lobe.12,13 However, the typical EEG findings in HSV encephalitis are periodic lateralized epileptiform discharges (PLED). 14 NMDAR encephalitis, on the other hand, has a more variable pattern – almost 45%–53% of cases with normal MRI findings.1,15,16 However, when MRI findings are normal, positron emission tomography (PET) scan findings are usually abnormal.15,16 In most reported cases, the EEG findings in anti-NMDAR encephalitis is a diffuse slowing pattern with no epileptiform discharges.4,17 It is important to keep in mind that the most specific EEG pattern for anti-NMDAR encephalitis is an extreme delta brush pattern. 18
Our case is noteworthy as the MRI and EEG findings were incongruent. However, the clinical presentation of neuropsychiatric symptoms, the clinical symptom of orofacial dyskinesia, which is rather common and specific for anti-NMDAR encephalitis, negative HSV PCR in the CSF, as well as poor response to antiviral medications prompted us to consider the possibility of anti-NMDAR encephalitis. As both serum and CSF antibody is highly specific (96.3%–100%), 19 the positive serum anti-NMDAR antibody was sufficient for diagnostic confirmation. This (antibody diagnostics) is important when MRI and EEG findings are incongruent. Furthermore, MRI of the pelvis revealed bilateral fat signal intensity lesions, suspicious of ovarian teratoma.
The patient had a bilateral cystectomy 4 months after presentation and immunotherapy. She reported marked improvement in the cognitive status, and upon assessment in the clinic, no longer exhibits orofacial dyskinesia. However, mild residual symptoms were still present, 6 months after presentation, despite surgical removal of the bilateral ovarian teratoma. Some authors report a 2-year period after presentation before full recovery. Follow-up is therefore recommended, to monitor the clinical progress, as well as any evidence of relapse, which can occur in 15%–25% of cases. 19 Annual sonographic surveillance (up to 2 years post tumour removal) has been advised, to look for recurrence. 20
Conclusion
Although infrequently reported, anti-NMDAR encephalitis is a common cause of autoimmune encephalitis. It is a typical clinical manifestation, which includes acute neuropsychiatric symptoms in young adults that respond poorly to antibacterial and antiviral therapy, should prompt a high index of suspicion. A multi-faceted approach, including investigations such as MRI, EEG, and lumbar puncture for CSF analysis, significantly facilitates early, accurate diagnosis. Timely diagnosis and treatment enables good clinical outcome.
Footnotes
Author contributions
All authors were involved in patient care, preparation of the manuscript and approved it for submission and publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for the publication of single case reports.
Informed consent
Written informed consent was obtained from parents, available upon request