
Abstract
Background:
Patients with substance use disorders admitted for severe bacterial infection are in a prime position to be screened for important co-infections. However, data suggest that standard screening for co-infections in this population during hospital admission can vary in frequency and type of testing.
Methods:
We performed a retrospective review of patients to evaluate screening for co-infections during admission, followed by a case–control analysis to determine factors associated with lack of any screening.
Results:
We identified 280 patients with 320 eligible admissions. Most were male and Caucasian with unstable housing. Only 67 (23.9%) patients had a primary-care provider. About 89% (n = 250) of our cohort were screened for one or more co-infection during their first admission with one patient never screened despite subsequent admissions. Of those screened, the greatest proportion was HIV (219, 81.4% of those without history of HIV), HCV (94, 79.7% of those without a prior positive HCV antibody), syphilis (206, 73.6%), gonorrhea, and chlamydia (47, 16.8%) with new positive tests identified in 60 (21.4%) people. Screening for all five co-infections was only completed in 15 (14.0%) of the 107 patients who had screening indications. Overall, a high proportion of those screened had a new positive test, including three cases of neurosyphilis, highlighting the importance of screening and treatment initiation. One patient was prescribed HIV pre-exposure prophylaxis at discharge and only 37 (34.6%) of those eligible were referred for HCV treatment or follow-up. In multivariable case–control analysis, non-Medicaid insurance (OR 2.8, 95% CI: 1.2–6.6, p = 0.02), use of only 1 substance (OR 2.9, 95% CI: 1.3–6.5, p < 0.01), and no documented screening recommendations by the infectious disease team (OR 3.7, 95% CI: 1.5–8.8, p < 0.01), were statistically significantly associated with lack of screening for any co-infection during hospital admission.
Conclusion:
Our data suggest additional interventions are needed to improve inpatient screening for co-infections in this population.
Keywords
Background
Over the last decade, Oregon, like most states across the country, has experienced a substantial rise in hospitalizations related to severe bacterial infections as sequelae in patients with substance use disorders (SUDs).1–3 People with SUD are at risk for co-infections related to sexual transmission in addition to injection drug use, as those with SUD engage in more sex without condoms, transactional sex, and sex with partners who inject drugs.4–9 Outbreaks and rates of hepatitis C (HCV), human immunodeficiency virus (HIV), Treponema pallidum (syphilis), Chlamydia trachomatis (chlamydia), and Neisseria gonorrhoeae (gonorrhea) have continued to increase creating a substantial financial and public health burden.5,10–12 In Oregon, there has been a steep increase in HCV, HIV, syphilis, and the number of congenital syphilis cases.5,12,13 Out of the 69 congenital syphilis cases from 2014 to 2020, 32% of the mothers had a history of injection drug use, 52% with methamphetamine use, and 48% experienced housing instability. 5 The highest risk of HCV infection acquisition is now predominantly young persons who inject drugs and screening guidelines have been updated to include all adults greater than 18 years of age.14–16 In addition, unstable housing has also increased among people who inject drugs, which is associated with less access to health insurance and primary-care providers (PCPs) resulting in delayed care and ongoing transmission in the community.17–21 Poverty, unstable housing, and SUD all make people vulnerable to life situations that are higher risk for sexually transmitted infection (STI) acquisition.
Patients with SUD admitted for a severe bacterial infection are in a prime position to be screened for important co-infections. However, data suggest that standard screening for co-infections in this patient population during hospital admission can vary in frequency and type of testing. 22 For patients with SUD requiring hospitalization, the inpatient stay also introduces an opportunity to initiate treatment and prevention measures, including linkage of care for HCV and HIV treatment, and engaging patients with initial discussions and uptake of HIV pre-exposure prophylaxis (PrEP). However, these things can only move forward after appropriate screening takes place.
Our study aims to describe screening for co-infections in patients with SUD admitted to an academic hospital for severe bacterial infection and identify factors associated with being screened or not being screened for at least one important co-infection during their hospital admission.
Methods
We performed a retrospective review of patients age 18 years or older, admitted for a severe bacterial infection requiring at least 2 weeks of antibiotics, an SUD diagnosis (confirmed by chart review) and consultation by infectious diseases (IDs) and addiction medicine between July 2015 and March 2020 [beginning of Coronavirus Disease 2019 (COVID-19) stay at home measures in Oregon]. A descriptive study was performed to evaluate screening for co-infections during admission including HCV, HIV, syphilis, chlamydia, and gonorrhea, followed by a case–control analysis to determine patient-level factors associated with lack of any screening during their initial admission in the study time-period. We also described completion of additional HCV diagnostic testing with HCV viral load needed to confirm chronic HCV infection and eligibility for HCV treatment. We performed chart review to collect variables of interest, including demographics, housing status, type of insurance, details on their primary infection, admitting team, HCV, and HIV status prior to admission, and access to a primary-care provider. All ID consult notes were reviewed to determine which screening tests were recommended by the consulting ID team. SUD characteristics including type of substances used at time of hospital encounter, number of substances used, route of use (injection, inhalation, or ingestion), most recent use, and associated tobacco use was largely identified from the addiction medicine service initial consult note, which also detailed the patient’s Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 V) severity score for each substance used. 23 Subsequent addiction medicine notes were used to determine SUD treatment initiation such as buprenorphine or methadone while inpatient. We reviewed the hospital discharge summary to capture referral for management of chronic infections such as HCV, and referral for PrEP. Laboratory tests and results performed during admission were collected from the electronic medical record via SAP BusinessObjects Enterprise Business Intelligence Platform 4.2 (SAP America, Inc., PA, USA).
We used SAS version 9.4 (SAS Institute Inc., Cary, NC, USA) to perform a descriptive analysis of patient characteristics, completed and recommended screening tests, in addition to positive test results. We compared categorical variables in univariable fashion by the chi-square or Fisher’s exact tests. We calculated crude and adjusted odds ratios (ORs) and 95% confidence intervals (CI) of cases (at least one screening test performed) with each exposure variable compared to the proportion of controls (no screening tests performed) with the exposure variable for the first admission during our study time-period. We used the Student’s t-test to evaluate continuous variables. For multivariable analysis, we performed a stepwise logistic regression analysis with all variables with a p value of .2 or less considered for inclusion. Our final multivariable model included variables with a p value <.05, or if their addition significantly altered the OR of another variable present in the model.
This study was reviewed and approved by the Oregon Health & Science University Institutional Review Board (IRB00003522). This study was conducted under an approved Waiver of Health Insurance Portability and Accountability Act Authorization Requirement.
Results
We identified 280 patients with 320 eligible admissions for severe bacterial infection requiring at least 2 weeks of antibiotics, an SUD, and consultation by ID and addiction medicine between July 2015 and March 2020. Most patients were male (181, 64.6%) and Caucasian (260, 92.9%) with a median age of 38.5 years (range: 19–74 years) and unstable housing (161, 57.5%; Table 1). Opioids (215, 76.8%) followed by methamphetamines (194, 69.3%) were the most common substances used with 199 (71.0%) reporting use of >1 substance. Only 67 (23.9%) patients had a PCP who they had seen at least twice over the preceding 24 months. All but two patients had health insurance. Approximately half (134, 47.9%) of our cohort completed their antibiotic course in an inpatient facility. Over half (144, 51.4%) of patients had an unplanned emergency department visit or admisison within 90 days of hospital discharge, and 7 (2.5%) patients died within 90 days of their initial admission.
Patient characteristics.
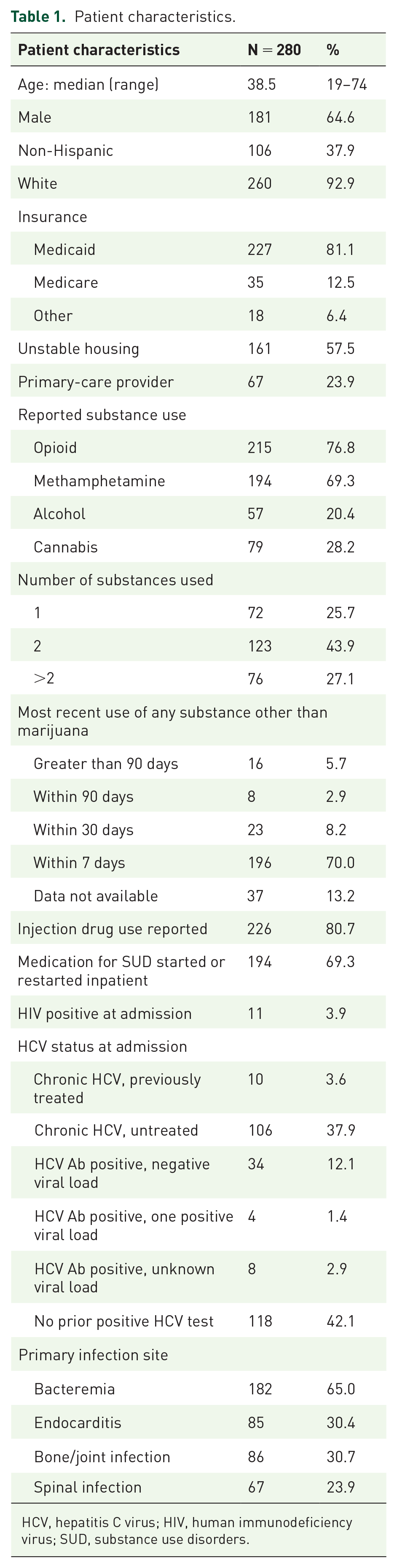
HCV, hepatitis C virus; HIV, human immunodeficiency virus; SUD, substance use disorders.
Screening
Eleven patients (3.9%) had a diagnosis of HIV and 108 (38.7%) had chronic HCV confirmed by two positive HCV viral load tests at least 6 months apart, two of whom had been treated for HCV with ongoing positive viral load or reinfection. Eighty-nine percent (n = 250) of our cohort were screened for one or more co-infections during their first admission with only one patient never screened despite subsequent admissions. Of those screened, the greatest proportion was for HIV (219, 81.4% of those without history of HIV), HCV (94, 79.7% of those without a prior positive HCV antibody), syphilis (206, 73.6%), gonorrhea and chlamydia at any body site (47, 16.8%) with new positive tests identified in 60 (21.4%) people. Screening for all five co-infections was only completed in 15 (14.0%) of the 107 patients who had screening indications. There was not a statistically significant trend in proportion screened over time.
HIV
Screening for HIV was completed in 81.4% (n = 219) of patients with 145 (66.2%) done prior to ID consultation. Of those not screened (n = 50), 11 (22%) patients had recent HIV screening and 22 (44%) patients did not have HIV screening recommendations documented by the ID consult team. Screening was also not completed in 17 of 86 (19.7%) patients where ID providers recommended HIV screening. PrEP was documented as being discussed with only 5 (1.9%) patients prior to discharge with the ID team leading most of these (n = 4). Only one patient was prescribed HIV PrEP at discharge, two declined PrEP and two were referred for PrEP initiation in the outpatient setting.
HCV
Of the 118 patients without a prior HCV antibody test on admission, screening was completed in 94 (79.7%) and the primary team ordered tests in 47 (39.8%) prior to ID consultation. HCV antibody testing was not done in 24 (20.3%). The ID team recommended HCV antibody testing in all but 13 (11.0%) of those not screened. In those who were screened, 26 (22.0%) had a positive HCV antibody test with HCV viral load positive in 24 (20.3%).
Of the 162 patients with confirmed chronic HCV or prior positive HCV antibody test, HCV antibody test was repeated in 78 (48.1%). Sixty-one percent of patients had indications for additional HCV diagnostic testing (viral load) of which 79.7% (n = 135) were completed during their admission.
Of the 54 patients with prior positive HCV antibody testing but without confirmation of chronic HCV or those previously treated for HCV and cured, three (5.6%) had a chronic HCV diagnosis confirmed during their admission, 8 (14.8%) with previous negative HCV viral load tests had a positive HCV viral load, 4 (7.4%) without a prior HCV viral load had a positive HCV viral load and 11 (20.3%) did not have additional viral load testing to confirm their HCV status.
Of those with confirmed chronic HCV prior to or during their admission, only 37 (34.6%) were referred for HCV treatment or follow-up, with most (29, 27.1%) instructed to follow-up with their PCP, of which only 6 (20.7%) had a PCP, while 8 (7.5%) had a referral placed to gastroenterology/hepatology at the time of discharge. Of the 70 without referral for HCV treatment, unplanned discharges were the most common reason documented (n = 19, 27%) with ongoing substance use documented in 3 (4.3%). Most (n = 44, 62.9%) did not have a reason documented for lack of referral for HCV treatment.
Syphilis
Syphilis screening was completed in 206 (73.6%) patients with 132 (46.9%) tests performed prior to ID consultation. ID recommended screening for an additional 85 patients (30.2%) of which 14 (16.5%) were not completed. Sixty patients (21.4%) did not have recommendations made for syphilis screening, only 10 (16.7%) of which had syphilis testing within the last 12 months. Seven (3.4%) positive RPR tests were identified in the 206 patients screened. Three of these were diagnosed with neurosyphilis, and one with early latent syphilis, with three of the tests determined to be false positives or serofast status by the consulting ID provider. Of the three patients diagnosed with neurosyphilis, two were identified by screening alone while admitted for an unrelated bacterial infection. The third was admitted for a condition thought to be due to a gram-positive bacterial infection with the etiology later determined to be syphilis following ID recommended testing. All were treated during their hospital admission.
Chlamydia and gonorrhea
Only 47 (16.8%) patients in our cohort were screened for gonorrhea and chlamydia at any body site, of which 30 (63.8%) were done prior to ID consultation. A higher proportion of women (28.9%) were screened for gonorrhea and chlamydia compared to men (10.4%). Screening was recommended by ID for an additional 20 (8.6%) patients, and was not completed in 5 (25.0%) of these patients. No ID recommendations for screening were provided in 221 (94.8%) of those not screened with an additional 7 (3.0%) having recent screening performed prior to admission. One case of gonorrhea was identified by screening and treated during hospital admission.
Case–control analysis
In univariable analysis, older age (p = .01), lack of methamphetamine use (p < .01), reported alcohol use (.02), cirrhosis (.03), stable housing (p < .01), insurance other than Medicaid (p < .01), use of only one substance (p < .01), no reported injection drug use (p < .01), no documented screening recommendations by ID (p < .01), and having a PCP (p < .01) were statistically significantly associated with lack of any co-infection screening during the first admission in our study time-frame (Table 2). Other comorbidities, duration of hospitalization, admitting service, or site of their primary infection were not associated with a lack of screening. In multivariable analysis, non-Medicaid insurance (OR 2.8, 95% CI: 1.2–6.6, p = .02), use of only 1 substance (OR 2.9, 95% CI: 1.3–6.5, p < 0.01), and no documented screening recommendations by ID (OR 3.7, 95% CI: 1.5–8.8, p < .01), were statistically significantly associated with lack of screening for co-infection during hospital admission.
Case–control analysis: factors associated with not being screened for any co-infection.

ID, infectious diseases.
Discussion
Limited published data are available evaluating screening for co-infections in patients with SUD during inpatient admission. 22 We describe missed opportunities to screen for co-infections in 20–80% of patients with SUD admitted for a serious bacterial infection, despite multiple guidelines recommending repeated screening in this population.15,16,24–27 Screening for all five co-infections was completed in only a few patients who had screening indications. Even when ID consultation recommended screening tests, approximately 20% were not performed, and a majority of patients not screened did not have screening recommendations documented by ID, which was the strongest association with lack of screening. We did not identify a trend in proportion screened over time. In our study, use of only one substance, non-Medicaid insurance and lack of screening recommendations by the ID team were all more common in those with lack of co-infection screening. Additional factors identified as significant in univariable analysis (lack of methamphetamine use, stable housing, PCP, etc.) suggest that provider teams potentially perceived lower risks for co-infections in these groups. However, of those not screened, half had evidence of exposure to HCV and nearly three-quarters had used a substance within 7 days of their admission suggesting ongoing risk in this population not being screened. Overall, a high proportion of those screened had a new positive test during their admission, including three cases of neurosyphilis, highlighting the importance of regular screening and initiation of inpatient treatment to prevent community spread. Oregon has had recent increases in congenital syphilis and rates of positive STI tests during the COVID-19 pandemic and we expect to see more positive tests in the future, highlighting a need to increase screening in this population.5,28 Moreover, though PrEP, in combination with harm reduction interventions, is proven to be effective in decreasing transmission of HIV in patients who inject drugs, in our cohort, we found documentation of discussion of PrEP with few patients. 29
Similarly, very few of those eligible received a referral for HCV treatment. Current guidelines recommend offering treatment to all patients with chronic HCV and no contraindications exist for ongoing active substance use. 16 Recent advances in direct-acting antiviral medications for HCV treatment has meant simpler dosing regimens, fewer adverse effects, and higher treatment success, allowing more treatment management by PCPs compared to prior decades, which required specialist care. In addition, providing therapy to patients with SUD is a cost-effective strategy for reducing HCV burden. 30 Inpatient HCV treatment is currently being piloted at OHSU; however, success of the program is tightly linked to our ability to adequately screen our population. Therefore, screening and then initiating HCV therapy during the inpatient admission or establishing structured referral processes to an outpatient provider for treatment are crucial to ensuring access to care and reduction of transmission in the community.
Chlamydia and gonorrhea screening was performed infrequently in our population, especially among men, and was substantially lower than the proportion screened for syphilis. Given the limited bandwidth for detailed contact tracing by public health departments for these infections, less data are available on the burden of disease in those with SUD compared to HIV, HCV, and syphilis.4,6,7,12,13 Since the primary mode of transmission in these diseases is sexual, the stark contrast in testing proportions between syphilis, HIV, chlamydia, and gonorrhea, may indicate a cognitive dissonance and an important role for bundled testing or creating order-sets for screening. In addition, ID providers did not consistently recommend testing for chlamydia and gonorrhea, indicating a need for additional education on SUD and associated behaviors that put patients at risk. Studies have shown those with SUD engage in more sex without condoms, transactional sex and sex with partners who inject drugs.8,9,31 In a large national cross-sectional data set between 2011 and 2015, Brookmeyer et al. 6 identified both men and women who inject drugs to be more likely to have sex with a partner who also injects drugs, engage in transactional sex, and report two or more sexual partners in the last year compared to those who do not inject drugs. In addition, chlamydia or gonorrhea diagnoses in the last year, previous syphilis and herpes diagnoses were also more common in men and women who inject drugs compared to those who do not. 6
In addition, over half of our population experienced unstable housing and less than a quarter had a PCP, reflecting significant structural, social and economic barriers to accessing healthcare, including screening and preventive care. A survey performed among people who use drugs in Ottawa between March and December 2013 reported unstable housing in a similar proportion (60.6%) with younger age, not having a PCP, monthly income less than $499, incarceration in the last 12 months, no support from peer workers and non-public disability support payments as the primary income source associated with unstable housing. 20 Another large population-based study in the US identified a significant increase in unstable housing among youth who inject drugs, with increased risky injection behaviors and transactional sex among those with unstable housing. 18 In addition, unstable housing among Medicaid recipients was associated with increased chronic disease burden, increased frequency of hospitalization, emergency room use and overall expenditures 3.8 times higher than housed Medicaid recipients. 17 The significant barriers related to unstable housing negatively impact both access to care and risk for co-infections, making hospital admission an even more important opportunity to provide additional screening, preventive health services, and treatment.
Our study has limitations. We describe our experience at a single academic medical center where the majority of our population is white, significantly limiting generalizability and our ability to identify and describe disparities resulting from structural racism. Our study population included those admitted with a severe bacterial infection requiring two or more weeks of antibiotics, who had both ID and addiction medicine consults, which is a specific and small proportion of patients admitted with SUD. We suspect this group has a higher rate of co-infection screening compared to people with SUD who are not seen by ID and/or addiction medicine, as prevention and screening are often not the focus for inpatient providers while managing other acute illnesses. Due to the limited number of patients with certain exposures, we did not have adequate power to include all potential confounders in multivariable analysis. In addition, since our study is retrospective in nature, our data are restricted to what was documented in the chart, and it is possible that screening recommendations were made over the phone or PrEP was discussed with a patient but not documented. We expect this misclassification to be non-differential with regards to case–control status and would result in an underestimation of these variables in our population.
Our study has important implications for patient care, provider education, and future research. With limited funding to STI clinics and the impact of the COVID-19 pandemic on public health resources, hospital admissions can serve as an ideal moment and place to screen high-risk populations and initiate or refer for PrEP or HCV treatment. 28 A shift in the mentality of inpatient care needs to occur to include these screening and preventive measures, as only focusing on the acute issue results in a failure to provide holistic care to our community. Given our population had both addiction medicine and ID team consultations, this group, theoretically, should have the optimal screening recommendations during their admission, yet we still identified multiple missed opportunities.
Providing medications for opioid use disorder to patients with SUD while in the hospital is a reachable moment. 32 Similarly, screening for common co-infections while in the hospital and when access to care may otherwise be limited is critical. Screening and preventive services for disease can no longer be deferred to PCPs when many of the structural barriers associated with unstable housing have resulted in few patients with SUD having durable access to a PCP or any outpatient care in the setting of traditional public health systems being underfunded and overwhelmed. Efforts to improve inpatient provider education and awareness of stigma, structural determinants of health, addiction medicine and risks associated with co-infection acquisition should be implemented. With greater awareness and standardization of screening with bundles or order-sets, which have been recently implemented at our institution, we hope to normalize inpatient screening for co-infections. Normalization of screening then allows for appropriate treatment and education with less stigma and judgment. Furthermore, building effective processes and structure to allow these patients access to PrEP and HCV treatment in the inpatient setting with reliable transition to the outpatient setting is critical to reducing spread of these infections and lessening the public health burden. Future research should broaden the scope of patients studied to include any inpatient with SUD, evaluate provider biases and dynamics driving lack of screening recommendations, and assess implementation of PrEP reminders, screening order-sets, and referral pathways.
Our current screening for co-infections in patients with SUD during hospital admission is inadequate. Increased awareness can hopefully lead to more patients receiving treatment and prevention for co-infections and by doing so, lower the community spread and burden of multiple infections as an outcome of a hospitalization for a single one.