
Abstract
Background:
Transcranial Doppler (TCD) is a well-established tool for cerebrovascular assessment. Estimating the flow velocity across the intracranial arteries helps to identify children with sickle cell anaemia who are at risk for stroke.
Objective:
Our aim is to correlate TCD findings with clinical condition in children with sickle cell disease (SCD) to determine the value of TCD assessment as a predictive tool for stroke in SCD and to identify any association of TCD findings with disease severity, transfusion therapy and treatment administered.
Methods:
Eighty-five paediatric SCD patients aged from 3 years to 18 years of both genders who were followed up at the Hematology Clinic of New Children’s Hospital at Cairo University were included in this cross-sectional observational study. All our participants underwent routine laboratory investigations and TCD assessments.
Results:
Oof the 85 patients, two patients (2.3%) died before completing the TCD study and eventually 83 patients were included in the analysis. Seventeen (20.5%) patients had abnormal TCD findings, seven (8.4%) patients showed high-risk findings and 10 (12.1%) patients had conditional flow pattern. Logistic linear regression analysis confirmed that annual frequency of blood transfusion and hydroxyurea (HU) dose were associated with a decreased risk of abnormal TCD findings.
Conclusion:
The current study demonstrates that our TCD data reproduce the findings of other studies and that it is very likely the results from large trials are applicable for Egyptian children. The annual frequency of blood transfusion and HU dose were associated with a decreased frequency of abnormal TCD findings.
Introduction
Sickle cell disease (SCD) is a generic term for a group of disorders that includes homozygous sickle cell anaemia, sickle cell haemoglobin C disease, sickle cell thalassaemia disease and other compound heterozygous conditions. They are all characterized by the presence of amutated β-globin gene, βS-globin and all-cause clinical disease. 1
Sickle cell anaemia is highly prevalent in sub-Saharan and equatorial Africa, with a lesser but significant prevalence in the Middle East, India and the Mediterranean region. The incidence of SCD in sub-Saharan African countries ranges from 1% to 2%, which translates to approximately 500,000 cases per year. 2
Stratification of stroke risk with transcranial Doppler (TCD) served as the basis for the development and testing of a therapeutic strategy using blood transfusion for the primary prevention of stroke in a randomized multicentre trial initiated in 1995 called the Stroke Prevention Trial in Sickle Cell Anemia (STOP). 3
Little is known about applicability of STOP criteria for management of SCD among Egyptians children which hampers preventive strategies against the disease.
The aim of the current study was to assess the role of TCD for predicting stroke in Egyptian children with SCD and to determine the correlation of the severity of TCD findings with different parameters such as disease severity, transfusion therapy and treatment administered.
Patient and methods Study Design Cross-sectional observational study
Study population
Our study involved 85 paediatric SCD patients who were followed up at the Hematology Clinic of New Children’s Hospital at Cairo University from 1 January 2016 until 1 January 2017. The patients ranged in age range from 2 years to18 years and were of both genders. None of our patients experienced a transitory ischaemic attack or a stroke during the study period.
We excluded patients with previous cerebrovascular accidents or any other neurological disorders (e.g. cerebral palsy) and patients with evidence of crises over the previous 4 weeks.
The study protocol was approved by the Research Committee of the Pediatric Department at Cairo University.
All patients had the following data collected: Clinical data: Full history-taking and a review of medical records were performed with a special emphasis on the patient’s age, duration of disease, frequency and severity of vaso-occlusive crises, disease-related complications and the duration and frequency of blood transfusion. A detailed history of the dose and duration of treatment were also recorded. Laboratory testing: Routine laboratory investigations included a complete blood count, reticulocyte count, haemoglobin electrophoresis, measurement of serum ferritin, liver and kidney function tests, measurement of serum lactate dehydrogenase and a coagulation profile. Vascular imaging: TCD was conducted at the Neurovascular Unit of the Neurology Department at Cairo University using DWL Multi-Dop T digital manufactured by Compumedics Germany GmbH.
In our study, transtemporal and transforaminal windows were used, and the highest time-averaged maximum mean velocity of the middle cerebral artery, distal internal carotid artery, anterior cerebral artery, bifurcation and posterior cerebral artery were recorded using the values from the STOP trial as references (a velocity ≥200 cm/s was classified as high risk, between 199 cm/s and 170 cm/s as conditional and ≤170 cm/s as normal). 3
Statistical analysis
Eighty-five patients were included in the statistical analysis and two patients were excluded due to missing data. Precoded data were entered on the computer using the Microsoft Office Excel software program (2013) for Windows and SPSS version 16 from IBM was used to analyse the data. Qualitative data are summarized using numbers and percentages. Quantitative data are summarized using suitable measures of central tendency and dispersions according to the distribution of the data. Stepwise logistic regression analysis was performed to detect significant predictors of abnormal TCD findings in the study population. The value of p ≤ 0.05 was considered statistically significant.
Results
The study included 85 patients with SCD. Two patients (2.3%) died before completing the TCD study. One patient (SS) died because of a severe sequestration crisis after hospitalization in the intensive care unit. The cause of death of the other patient (Sβ) was not available in our data. Ultimately, only 83 patients were included in the analysis. Ten (11.7%) cases had hepatitis C virus (HCV+ve), five (3.5%) cases suffered from chronic cholecystitis, four (4.7%) cases had history of osteomyelitis, three (3.5%) cases suffered of pulmonary hypertension, one (1.1%) case had chronic urinary tract infection and one (1.1%) case suffered from chronic liver cell failure. Vaso-occlusive pain crisis which is defined as the occurrence of pain in the extremities, back, abdomen, chest or head that lasts two or more hours and cannot be explained except by the presence of SCD was reported in 17 (20%) cases.
The baseline and demographic characteristics of the study population are presented in Table 1.
Baseline demographic, clinical, and normal and abnormal TCD data of all study participants (n = 83).

VOC: vaso-occlusive crisis; HU: hydroxyurea.
a‘Severe’ VOCs were defined as patient-reported emergency department visits or hospitalizations for pain treatment.
b p ≤ 0.05: statistically significant.
Sixty-six (79.5%) patients in the study group had normal TCD findings compared to 10 (12.1%) patients who had conditional TCD findings and 7 (8.4%) patients had high-risk findings (Figure 1).

Distribution of TCD findings among study population (n = 83). TCD: transcranial Doppler.
The mean annual frequency of transfusions for patients with normal TCD findings was 2.86 ± 3.24 times/year compared to 1.06 ± 1.81 times/year in those with abnormal TCD findings with a significant p value of 0.004.
The mean hydroxyurea (HU) dose for patients with normal TCD findings was 19.64 mg/kg compared to 12.86 mg/kg for patients with abnormal TCD findings with a significant p value <0.001.
The stepwise logistic regression model showed that both the frequency of blood transfusion and the HU dose were independent predictors of abnormal TCD findings with p values of 0.024 and 0.002, respectively (Table 2 and Figure 2).
Logistic regression analysis for risk factors of abnormal TCD.
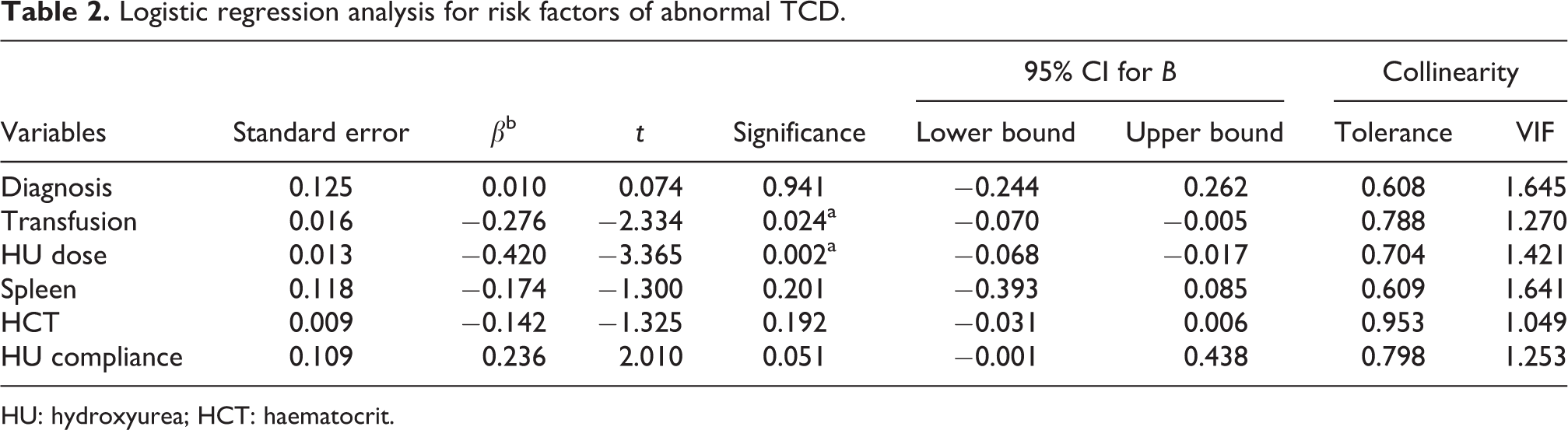
HU: hydroxyurea; HCT: haematocrit.
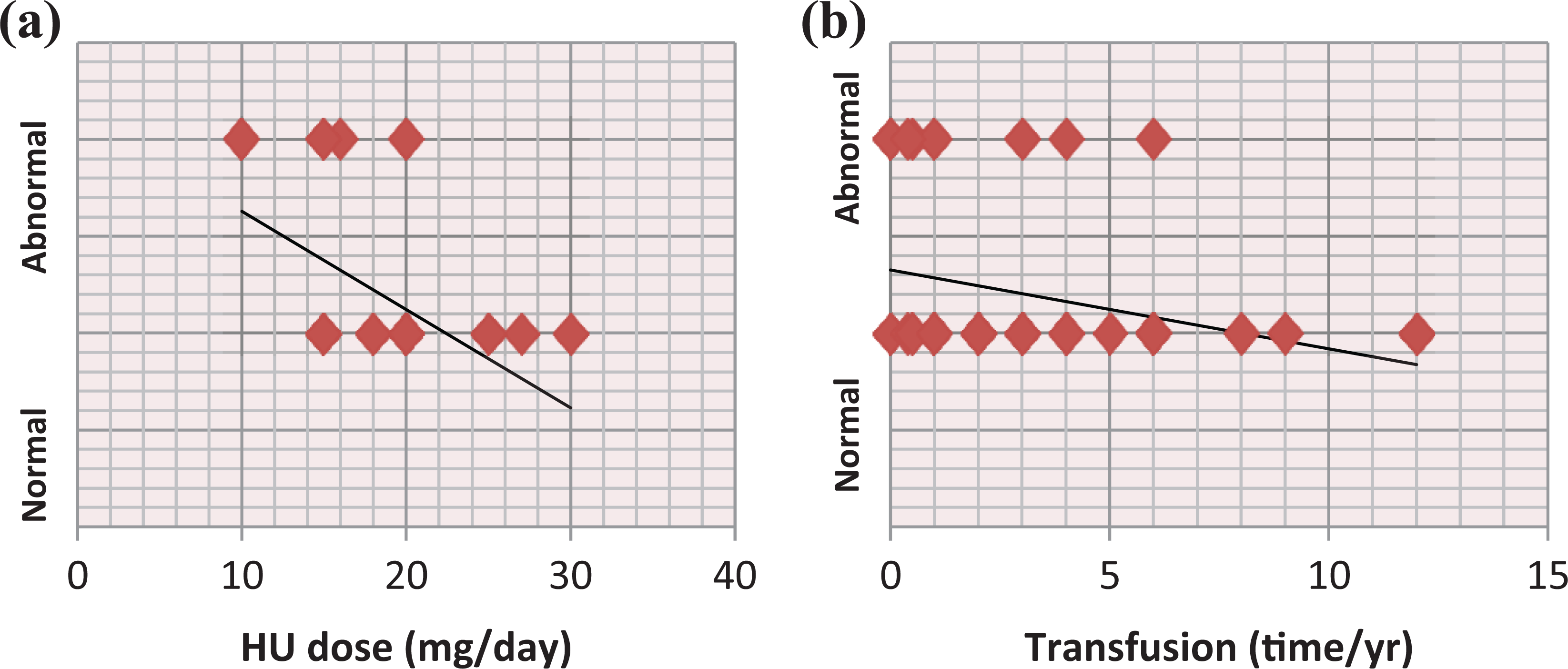
(a) Linear regression correlation of HU dose and (b) frequency of blood transfusion with TCD findings. HU: hydroxyurea; TCD: transcranial Doppler.
Discussion
The results of this study showed that 17 (20.5%) of the 83 included patients had abnormal TCD findings; seven (8.4%) had high-risk findings and 10 (12.1%) had conditional findings. Our data are almost consistent with those of the STOP trial, which was a randomized multicentre controlled trial involving 2324 children aged 2 years to 16 years who were screened with TCD in which the percentage of patients with high-risk findings was 9.7% and that of patients with conditional findings was 17.6%. 3,4
Our results are also in accordance with those of another cohort study from England 5 involving 124 children older than 3 years that revealed that seven patients (6%) had high-risk findings and 11 (9%) had conditional findings.
However, studies have shown a much lower incidence of abnormal findings among Brazilians (8–9% conditional and 0–1% high-risk findings) 6,7 and Africans who live in Italy (0% high-risk and 25% conditional findings). 8 However, the sample size in the last study (n = 12) was a major limitation.
In contrast, the incidence of abnormal findings was much higher in Nigerian children with SCD aged 3–18 years (n = 48), with a conditional rate as high as 31.5% and a high-risk percentage of 7.6%, which increased in the follow-up study after 3 months to 15%. 9 These findings may be explained by severe African genotype of SCD.
In the current study, comparing the mean number of transfusions per year among patients with normal TCD findings to that among patients with abnormal TCD findings (conditional and high-risk findings) showed a significant difference with a p value of 0.004. We concluded that the higher the rate of blood transfusion is, the lower the incidence of abnormal TCD findings is and, consequently, the lower the rate of stroke. This significant and strong positive correlation indicates the importance of blood transfusions in maintaining cerebral blood flow and preventing stroke in children with SCD. This result is in agreement with those of previous reports and studies. 3,10 Both previous studies demonstrated that blood transfusion greatly lowers the risk of stroke by 70% by reducing levels of sickle haemoglobin (HbS) to below 30%. Moreover, an extended trial (STOP II) concluded that discontinuation of transfusion for the prevention of stroke in children with SCD resulted in a high rate of reversion to abnormal blood flow velocities on Doppler studies and a high rate of stroke.
It is important to note that correlation of TCD findings with either disease severity by clinical means or HbS percentage at the time of the study did not appear to have any effect on TCD results. This highlights the need for screening all patients using TCD aiming for 1ry prevention of stroke, irrespective of clinical severity or HbS% levels.
Furthermore, correlation of TCD findings with haematological parameters (total leucocyte count, Hb and platelet) showed statically insignificant effect on TCD result. These findings were in contrast to another studies which demonstrated negative correlation between Hb and HCT levels and abnormalities in TCD studies. 11
Another important finding from the current study is that the dose of HU had a significant impact on the TCD results, as patients who received higher doses of HU had a decreased risk of developing abnormal TCD results. Our study also highlighted the importance of compliance to treatment, as only 8.8% of patients with good compliance showed abnormal TCD findings compared to 41.2% of those with poor compliance, and these results were statistically significant.
These findings corroborate those of a study from another group that found that HU therapy decreased TCD flow velocities in children with SCD. 12,13
Furthermore, logistic linear regression analysis showed that blood transfusion and HU dose were associated with a decreased risk of abnormal TCD results. This finding confirms the protective effects of transfusion and HU against the development of abnormal TCD velocities and stroke in children with SCD. This finding corroborates well with high-quality Cochrane Reviews for the use of red blood cell (RBC) transfusions in preventing stroke in children and adolescents at high risk of stroke (abnormal TCDs or silent cerebral infarct (SCI) and evidence that it may decrease the risk of SCI in children with abnormal TCD velocities). In addition, RBC transfusions may reduce the risk of acute chest syndrome and painful crisis in this population. 14,15
Our study is limited by lack of data on cerebral imaging (magnetic resonance imaging or computed tomography) which therefore cannot be correlated with TCD results.
Conclusion
The current study reproduced TCD findings of other studies and showed that the annual frequency of blood transfusion and HU dose were associated with a decreased frequency of abnormal TCD findings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.