
Abstract
Introduction:
Narcolepsy is a chronic neurological sleep disorder, the diagnosis of which is based upon clinical evaluation and additional paraclinical assessments. Awareness of narcolepsy is low and screening tools needed. The Epworth Sleepiness Scale (ESS), the Ullanlinna Narcolepsy Scale (UNS), and more recently the Swiss Narcolepsy Scale (SNS) were used as screening tools for narcolepsy. The aims of the present study are (1) to assess the value of the SNS in a new series of patients with narcolepsy with cataplexy (NC), and (2) to compare its sensitivity and specificity with the ESS and UNS.
Patients and Methods:
We prospectively assessed by questionnaire patients with NC (n = 80, all with assessment of cerebrospinal fluid (CSF) hypocretin-1 levels) and patients with excessive daytime sleepiness (EDS) of other origin (n = 111) in Zurich and Leiden. Causes of EDS included idiopathic hypersomnia (n = 12), behaviorally induced sleep insufficiency syndrome (n = 32), restless legs syndrome (n = 7), sleep-disordered breathing (n = 22), and hypersomnia due to medical disorders (n = 9). Diagnoses were made according to the International Classification of Sleep Disorders (third edition). Cutoff values of UNS and SNS for diagnosis of narcolepsy were those suggested in the literature.
Results:
For the diagnosis of narcolepsy, the following sensitivities and specificities were found: SNS (89% and 88%), UNS (100% and 62%), and ESS (91% and 54%). For the diagnosis of narcolepsy with low or non-detectable CSF hypocretin-1, the sensitivities and specificities were: SNS (93% and 88%), UNS (100% and 62%), and ESS (93% and 54%).
Discussion:
In conclusion, the SNS is accurate and superior to the ESS and the UNS for the screening/diagnosis of NC and allows, in addition, the identification of hypocretin-1 deficient patients.
Background and aims
Narcolepsy with cataplexy (narcolepsy type 1; NC) is characterized by chronic excessive daytime sleepiness (EDS) with irresistible sleep attacks, sudden loss of muscle tone triggered by emotions (cataplexy), and disturbed nocturnal sleep. Commonly associated symptoms are hypnagogic or hypnopompic hallucinations and sleep paralysis, parasomnias, periodic limb movements in sleep, increased body weight, as well as cognitive and psychiatric disturbances. 1,2
The diagnosis of NC is primarily based on a detailed medical history. 3 Cataplexy is the pathognomonic symptom of the disorder. In addition, paraclinical assessment including sleep laboratory and laboratory analysis is executed: Low mean sleep latencies (<8 min) and the presence of ≥2 sleep onset REM periods on the multiple sleep latency test or in a polysomnography confirm the diagnosis. Additionally, the presence of human leucocyte antigen DQB1*0602 supports the diagnosis (detectable in 98% of narcoleptics, but also in 12–38% of non-narcoleptic Caucasian subjects). 4 The most sensitive (87%) and specific (99%) finding for NC is the finding of markedly decreased hypocretin-1 (orexin A) levels in the cerebrospinal fluid (CSF), which probably reflects a loss of hypocretin-producing neurons in the hypothalamus. 5 –7
Questionnaires can be helpful to screen/diagnose NC. The Ullannlinna Narcolepsy Scale (UNS) 8,9 is the most commonly used questionnaire. A score of ≥14 was suggested to have a high sensitivity (100%) and specificity (98.8%) for NC. 8 Although being highly sensitive, the specificity seems to be less pronounced, 10 which limits the usefulness of the scale for clinical purposes. Furthermore, the score consists of 11 questions, making it less practicable in the daily usage. The Epworth Sleepiness Scale (ESS) is also used to detect narcoleptic patients. 11,12 A score >10 was found to have a sensitivity and specificity of 93.5% and 100%, respectively, for the diagnosis of narcolepsy. 12
In a previous study, 10 we reported the accuracy of a new scale (the Swiss Narcolepsy Scale (SNS)) for the diagnosis of narcolepsy in 57 patients with narcolepsy when compared with 40 controls and 56 patients with EDS. This five-item scale was found to have high sensitivity (96%) and specificity (98%) for the diagnosis. However, the population of patients with narcolepsy was somewhat heterogenous (patients with typical and atypical cataplexy were included), and CSF hypocretin-1 levels were available only in a small portion of patients (n = 12).
With this study, we aimed (1) to assess the sensitivity and specificity of a German and a Dutch version of the SNS in a new and prospective series of patients with NC, in whom CSF hypocretin levels were available, (2) to compare its sensitivity and specificity with the UNS and the ESS, and (3) in the subgroup of CSF hypocretin-1 deficient patients with narcolepsy in particular.
Patients and methods
The study has been performed at the University Hospital of Zurich, Switzerland (German version of the SNS, UNS, and ESS), and at the Leiden University Medical Center, the Netherlands (Dutch version of the SNS).
Concerning ethical approval a further use of these data for this publication is permitted corresponding to article 34 of the Swiss law on human research.
We prospectively assessed consecutive adult patients with NC. The diagnosis of narcolepsy was made according to international criteria. 3 In all patients, CSF hypocretin-1 levels were available. In Zurich, we included 27 NC patients (mean age 36 ± 15 years, 8 men). The Leiden center contributed with 53 NC patients (mean age 42 ± 16 years, 28 men). Hypocretin-1 levels were measured in crude CSF with a radioimmuno assay as published before. 13 The cutoffs for low/absent levels of CSF hypocretin-1 were <320 pg/ml in Zurich and <110pg/ml in Leiden.
Results were compared to 111 non-narcoleptic patients presenting with the symptom of EDS and subsequently diagnosed with an EDS of another specific origin (mean age 47 ± 15 years, 68 men). The most common causes of EDS were idiopathic hypersomnia (n = 12), behaviorally induced sleep insufficiency syndrome (n = 32), restless legs syndrome (n = 7), sleep-disordered breathing (n = 22), and hypersomnia due to medical disorders (n = 9).
Questionnaires
All patients filled in the SNS. Patients from Zurich additionally filled in the UNS and the ESS. The questionnaires (used in the clinical evaluation in both centers) were given to the patients during clinical visits following a short instruction. The ESS has been validated in German before. 14
The SNS includes the following five items (see Table 1): (1) inability to fall asleep; (2) being unrefreshed in the morning; (3) taking a nap at noon; (4) knee buckling during cataplexy; and (5) sagging of the jaw during cataplexy. A calculated value of <0 (formula to calculate the score see Table 1) is indicating the presence of NC. The translation was done by narcolepsy specialists with a well-founded knowledge in the language-specific meaning of the individual questions.
The 5 questions forming the SNS (in the english translation, german original in brackets, with the corresponding values) and the calculation & evaluation.

Results
NC patients
Disease duration in NC patients was 1–54 years (mean 16.6 ± 12.9 years). Fifty-eight (64%) NC patients were treated at the time of the study—45 with stimulants, 33 with anticataplectic drugs, and 20 with both.
CSF hypocretin-1 was low or absent in 69 patients (86%) suffering from NC. In 11 patients (14%), normal values were found. An SNS score <0 was found in 71 NC patients (89%, mean value: −38, range −101 to 36). Of the nine false-negative patients, four had a normal CSF hypocretin-1 level. All nine patients had clear-cut cataplexy.
EDS patients without narcolepsy
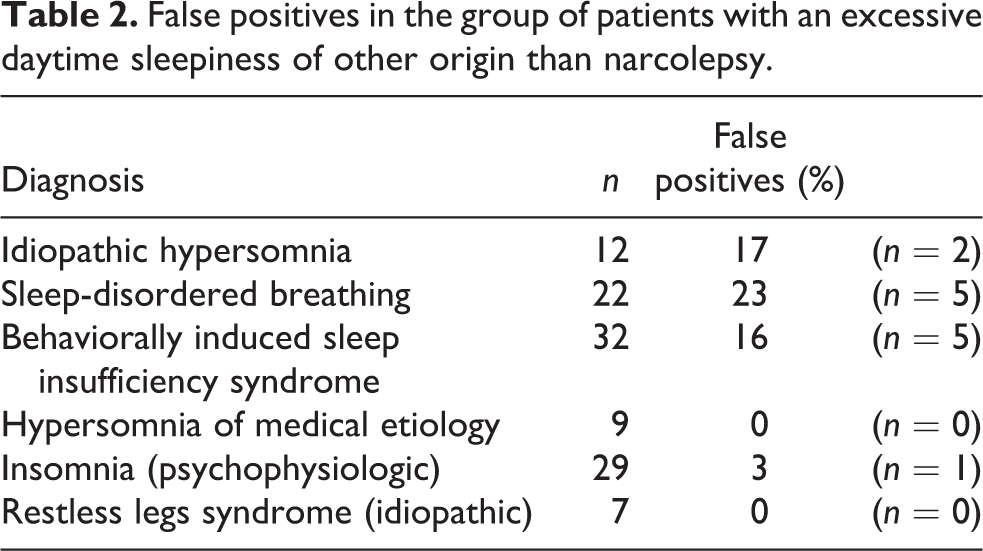
The mean value of the SNS in EDS patients without narcolepsy was 23 (−46 to 66). Cataplexy-like symptoms were not reported in these patients. False-positive results (SNS score <0) occurred in 13 patients, with the highest ratio in patients with sleep-disordered breathing and behaviorally induced sleep insufficiency syndrome (see Table 2). In the subgroups of patients with restless legs syndrome and patients with hypersomnia of medical etiology, no false positives were observed.
False positives in the group of patients with an excessive daytime sleepiness of other origin than narcolepsy.
Sensitivities and specificities of the SNS, the ESS, and the UNS
For the diagnosis of NC, the SNS (score <0) had a sensitivity of 89%, a specificity of 88%, and an accuracy of 89% (see Table 3, first column and Figure 1).
Sensitivities | Specificities | Accuracy of the Swiss Narcolepsy Scale (in all NC and in the subgroup of patients with low or absent CSF hypocretin-1).
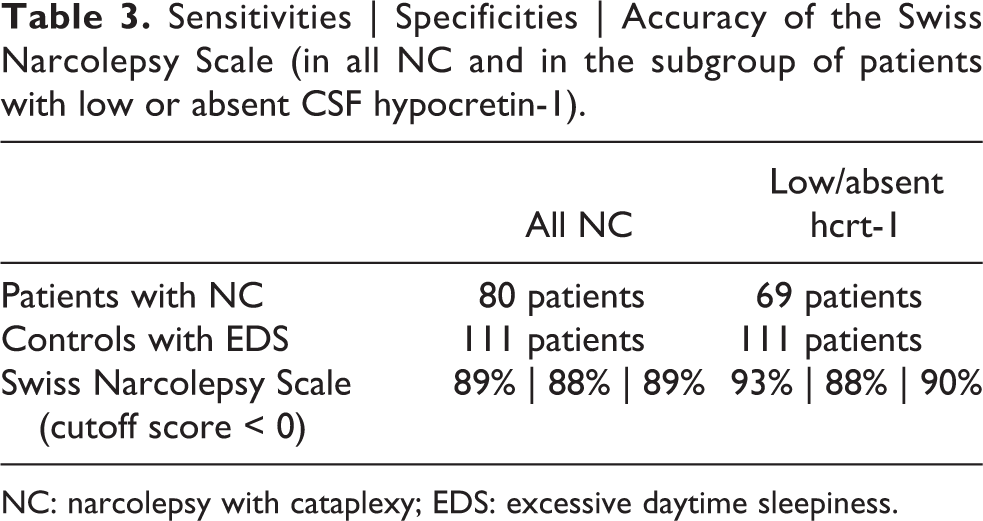
NC: narcolepsy with cataplexy; EDS: excessive daytime sleepiness.
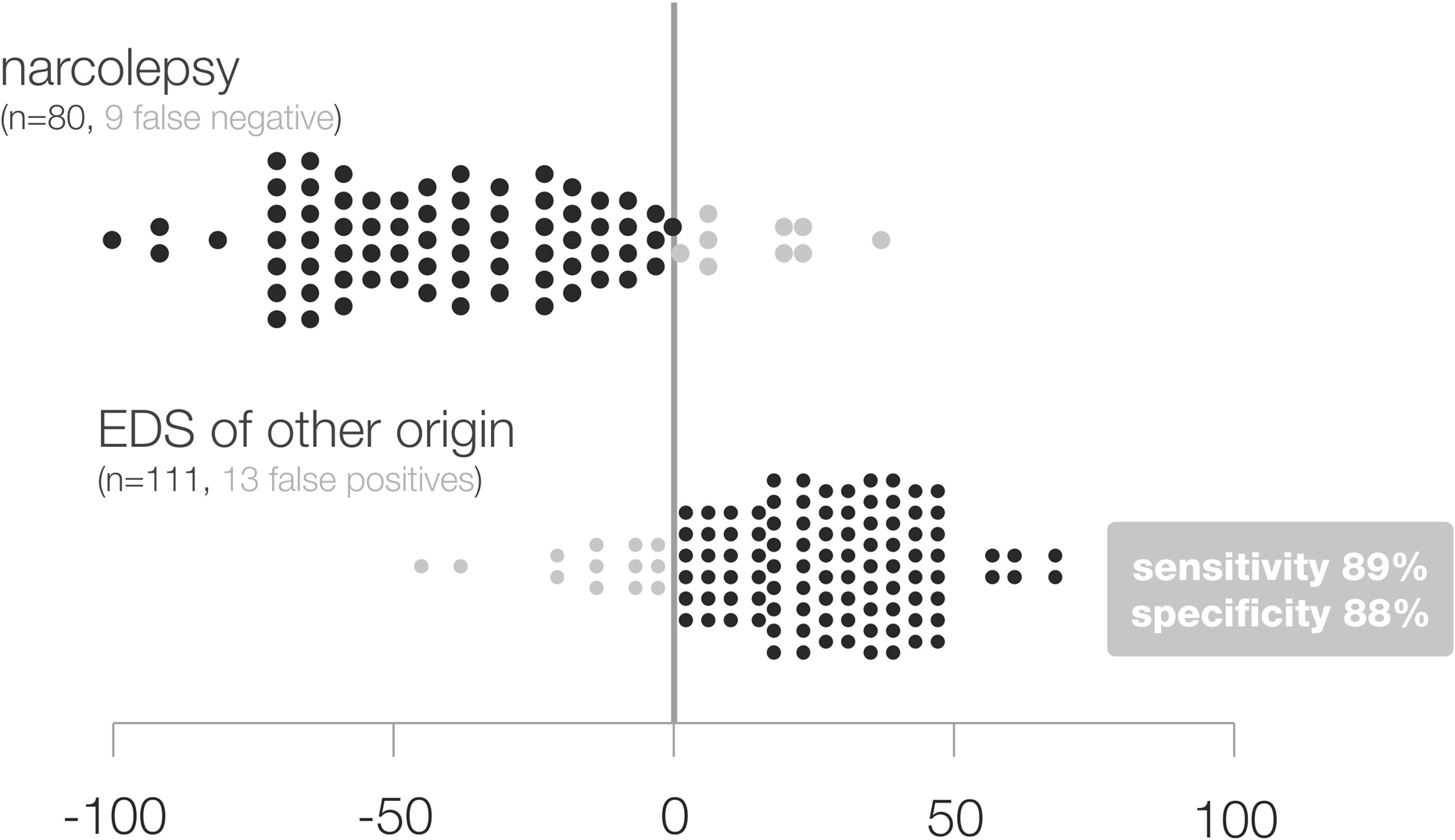
Density graphs of the SNS in patients with narcolepsy and patients with EDS of other origin. SNS: Swiss Narcolepsy Scale; EDS: excessive daytime sleepiness.
In the Zurich population (see Table 4), the UNS (score ≥14) had a sensitivity for narcolepsy of 100% and a specificity of 62% (accuracy 70%). The ESS (score ≥14) had a sensitivity of 91% and a specificity of 54% (accuracy 61%). To establish the best cutoff point for the ESS, we calculated the sensitivities and specificities with various cutoffs, finally applying the one (≥14) with the best combination of sensitivity and specificity.
Sensitivities | Specificities | Accuracy of the Swiss Narcolepsy Scale, the Ullanlinna Narcolepsy Scale, and the Epworth Sleepiness Scale in the Zurich population alone.

NC: narcolepsy with cataplexy; EDS: excessive daytime sleepiness.
For the diagnosis of narcolepsy with non-detectable CSF hypocretin-1, the sensitivity and specificity of the SNS rose to 93% (5 false negatives) and 88%, and the accuracy to 90% (see Table 3, second column and Figure 2).

Density graphs of the SNS in patients with narcolepsy having low/absent hrct-1 and patients with EDS of other origin. SNS: Swiss Narcolepsy Scale; EDS: excessive daytime sleepiness.
Discussion
Diagnosis of narcolepsy can be challenging. Lack of recognition of narcolepsy symptoms and difficulties in differential diagnosis often result in a delayed diagnosis of more than 5 years after symptom onset. 15 Simple screening/diagnostic tools for narcolepsy have been suggested including the UNS and more recently the SNS. The ESS is unspecific for narcolepsy, but frequently used to evaluate the severity of the excessive sleepiness in various disorders, including in patients with NC.
Our study now confirms the validity of the SNS as a highly specific screening tool for NC, particularly for hypocretin-deficient patients. Further, we show superiority of specificity of SNS against UNS and ESS (88% vs. 54% and 62%). Though the UNS and the ESS have a slightly higher sensitivity in our population, the comparatively low specificities limit their use by including too many false positives.
Not all of our patients with narcolepsy and cataplexy were hypocretin-1 deficient. The portion of these is in concordance with previous studies. 16,17
Key points in the differential diagnosis of narcolepsy are the occurrence of cataplexy (narcolepsy type 1 vs. other EDS disorders) and awakening/performance after sleep (narcolepsy vs. hypersomnia). The high specificity of the SNS is mainly due to the composition of the questionnaire with inclusion of questions on cataplexy and awakening. In cataplexy, the occurrence of muscle weakness in the face or neck is suggested to be more specific than in the knees (limbs), but knee cataplexy is described more frequently. 18 In our scale, both aspects are addressed, with emphasis on facial cataplexy. Nevertheless, cataplexy mimics or cataplexy-like symptoms (in non-narcoleptic patients with daytime sleepiness more prevalent 10 ) might be a confounding factor and could therefore lead to a false-positive result. If the higher frequency of false positives in sleep-disordered breathing (compared to idiopathic hypersomnia and behaviorally induced sleep insufficiency syndrome; see Table 2) is of any significance seems to be doubtful (small sample size of the individual control groups could overstate the difference). In our knowledge, there are no reports in the literature of a higher frequency of cataplexy-like symptoms especially in sleep-disordered breathing.
An additional practical advantage of our score is that it consists of a small number of questions (5 vs. 11 (UNS) or 10 (ESS)) and can be filled out within a few minutes by the patient.
Our score obviously may be helpful to screen patients with EDS, seeking for medical advice, for further testing for the diagnosis of narcolepsy. It obviously does not substitute a detailed diagnostic evaluation, which always includes a detailed face-to-face interview at first and whenever necessary specific ancillary tests.
The SNS is a reliable, simple, and quick tool in screening and will help to diagnose NC (narcolepsy type 1).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.