
Abstract
Spontaneous intracranial hypotension (SIH) has gained more attention in the eyes of clinicians in the past years and is now recognized as an important cause of headaches. While usually self-limiting and benign, some patients suffer from debilitating symptoms that interfere significantly with their social and professional life. Thus, recognition and adequate treatment of SIH is of paramount importance. Recent refinements in imaging techniques combined with modern microneurosurgical techniques offer many diagnostic and therapeutic possibilities today. The aim of this review is to give the reader an updated review on the state-of-the art in the challenging diagnosis and treatment of SIH as well as an insight into recent developments of pathophysiological concepts and affiliations with other enigmatic diseases.
Keywords
Introduction
Spontaneous intracranial hypotension (SIH) is an increasingly recognized disease. While SIH was rarely diagnosed in the past, it is now acknowledged as an important cause of headaches. Spinal dural cerebrospinal fluid (CSF) leaks cause SIH. Aim of the current review is to give an overview over SIH with emphasis on recent developments in diagnostics and therapy.
The terminology is varied and many synonyms are in use (see Table 1). The term “spontaneous intracranial hypotension—SIH” is currently most convenient, although approximately 50% of patients do not present with “hypotension,” that is, low CSF pressure at lumbar puncture, at all.
Synonyms for spontaneous intracranial hypotension.

While SIH usually follows a self-limiting course of short duration and some patients experience only mild symptoms, others may present with persistent, incapacitating symptoms. The clinical hallmark is orthostatic headache, but the clinical picture can be diverse and it should be borne in mind that affected individuals with chronic disease can present with atypical symptoms. This renders the diagnosis challenging and not infrequently the patients end up on a diagnostic odyssey.
SIH should be suspected in all patients with orthostatic symptoms as well as in young and middle-aged patients with new-onset, daily persistent headaches. Typically, the symptoms occur immediately or within seconds to minutes of assuming an upright position and resolve within minutes after lying horizontally. 1 Nevertheless, a delayed response to postural change, after minutes or hours, may occur. SIH needs to be differentiated from the pathophysiologically similar postlumbar puncture headache as well as orthostatic headache due to postoperative CSF leaks or shunt overdrainage where there is an obvious trigger.
The estimated incidence is 5 per 100,000 inhabitants, 2 though the real figure might be significantly higher. Patients in their 40s and 50s are the most frequently affected, with females being twice as likely to be affected as males. 2 –4
The cause of the disease is a CSF leak, most commonly along the cervico-thoracic spine, with subsequent loss of CSF. 2,4,5 Usually, the leaks themselves do not provoke any local symptoms. It is the CSF leakage, the hypovolemia, and the resulting brain sagging that causes the clinical symptoms.
A third of all patients report a minor trigger, such as strenuous physical activity, positional change, lifting of a weight, coughing, sneezing, or chiropractic manipulation. 2,3,6,7 Very occasionally, according to the literature, patients display signs of connective tissue disorders, like joint hypermobility. 2,4,5,8
Schievink et al. 9 proposed a classification of spinal CSF leaks into four specific types: (1) longitudinal dural tears, (2) meningeal diverticula, (3) direct CSF-venous fistula, and (4) an indeterminate category, if no specific leak can be diagnosed.
In a study on 14 patients with refractory SIH, microsurgical examination revealed a CSF leak in all cases. 10 The majority were small longitudinal dural tears of 4–10 mm, either on the ventral dural aspect (ca. 76%) or at the axilla of the exiting nerve root (ca. 20%). For the ventral leaks, the predominant cause was a small extradural discogenic microspur. The lateral tears at the axilla were often accompanied by an outpouching of the arachnoid leading to or representing spinal meningeal diverticula. With this rigorous surgical workup, only a few cases (approximately 4%) showed abnormalities along the exiting nerve root, most often nude nerve roots or thin dural covering. Our current surgical series of >50 patients corroborates the earlier findings.
In clinical practice, patients with a short duration of symptoms (approximately 80%) need to be distinguished from chronic, persistent cases. In the latter, extensive diagnostic testing usually identifies one of two main types of CSF leaks (Figure 1)
10
: – leakage through a longitudinal tear in the ventral dura, most often caused by a calcified microspur, which penetrates the dura like a knife (80%); and – leakage through a longitudinal tear in the lateral dura, associated with a meningeal diverticulum in the region of the nerve root (20%).
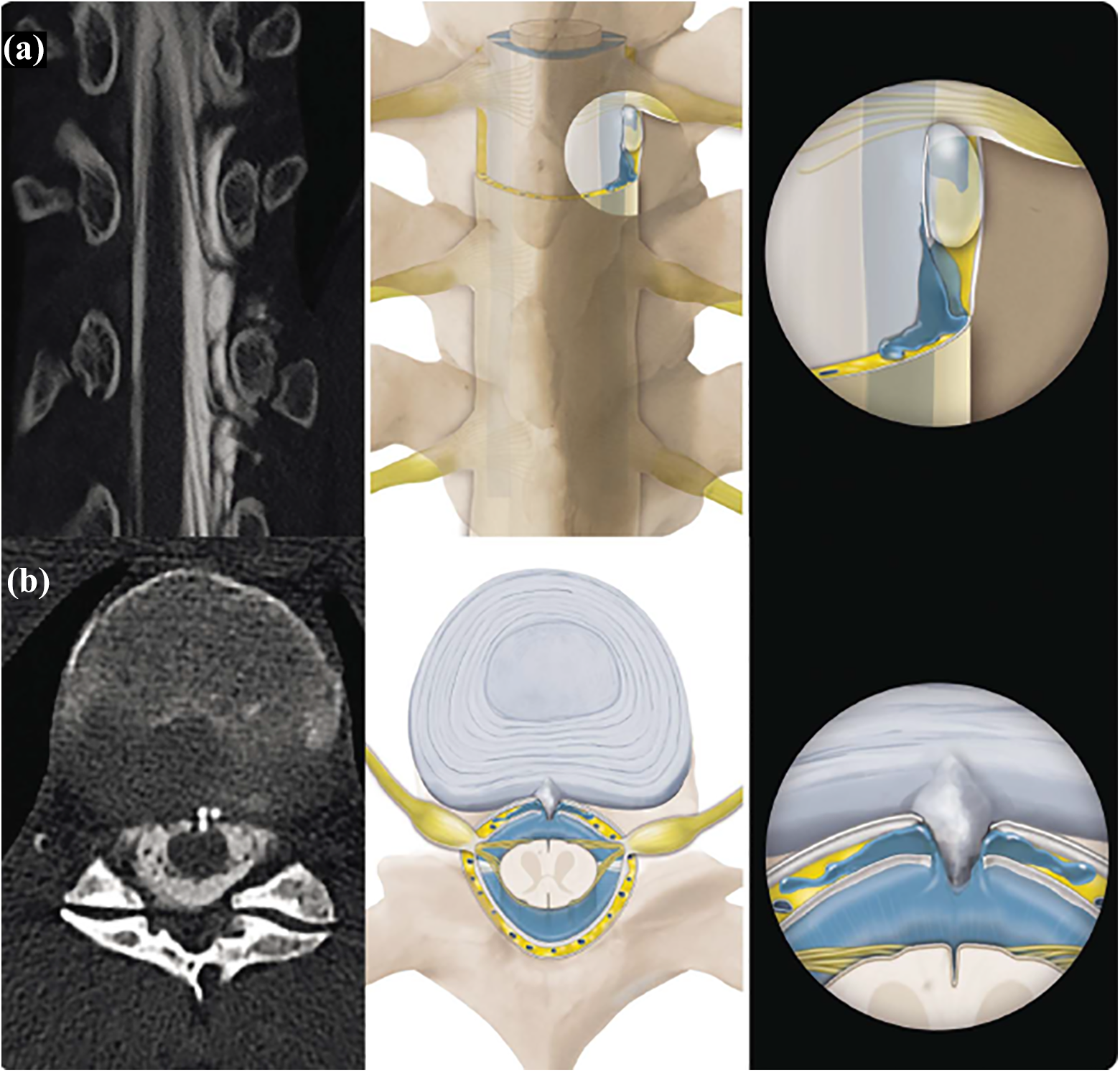
Pathology of spinal CSF leaks: computed tomography (CT)-myelography (left) and artist’s rendering (middle and right) of two frequent mechanisms in patients with intractable symptoms. (a) Spinal meningeal diverticulum according to dural tear and CSF leakage with an outpouching of the arachnoid in the region of a nerve root. (b) Microspur at the disc level penetrating the ventral dura like a knife and causing a longitudinal slit. CSF: cerebrospinal fluid; SIH: spontaneous intracranial hypotension.
Recent radiological and microsurgical investigations revealed that a calcified, degenerative bony microspur is often the culprit lesion in cases of intractable CSF leaks. 10 –12 Arising from the level of the intervertebrate disk space, these microspurs pierce the ventral dura and produce a slit-like defect a few millimeters in length. 10 These microspurs and the associated CSF leak have to be localized exactly, and then they are amenable to surgical treatment. These microspurs can also occur asymptomatically, that is, without an associated CSF leak. Multiple microspurs may be present in the same patient. For targeted treatment, it is therefore of the utmost importance to localize the exact anatomical site of the leak and not only the presence of a microspur.
Meningeal diverticula have been known for some time to be associated with spinal CSF leaks. However, in our own experience, these lesions are causal in only 20% of cases with proven CSF leaks. 9,10 The dura may be more prone to tearing in the region of the axilla of a nerve root, which leads to CSF leakage and subsequent prolapse of the arachnoid membrane. This can be recognized as meningeal diverticulum on imaging and is also amenable to surgical treatment. In other series, spinal diverticula are found more often (42% of cases). 9 However, it should be borne in mind that the mere presence of a spinal meningeal diverticulum is not per se identical with the diagnosis of a CSF leak. Greater insight is likely with further developments in imaging.
Nevertheless, the exact localization of the CSF leak before any surgical treatment is undertaken is of paramount importance. To further complicate the scenario, a meningeal diverticulum sometimes follows the course of a nerve root, 9,13 and although no extrathecal CSF is evident in such cases, patients can improve with targeted therapy (see below).
It is important to reiterate here that both microspurs and meningeal diverticula can be present in healthy individuals without any symptoms and therefore cannot be equated with the diagnosis of SIH. 14 Even in patients with a proven spinal CSF leak, a microspur is not necessarily the culprit lesion—verification by dynamic imaging is essential (see below).
Interestingly, dural defects at the skull base with subsequent oto- or rhinoliquorrhea are not associated with orthostatic headache and need to be clearly distinguished from SIH. However, unlike with spinal CSF leaks, there is a risk of meningitis associated with skull base defects. 15
Pathophysiology
Under physiological conditions, the buoyancy force reduces the brain’s weight of 1500 g to an effective mass of 50 g in CSF. 16 The remaining weight is borne by pain-sensitive structures such as the meninges, the cerebral and cerebellar veins, and some cranial nerves. 17 In the case of CSF hypovolemia, the brain sags in a caudal direction and imposes traction on those pain-sensitive structures. The displacement along the direction of the gravitational force explains the orthostatic nature of the complaints. 4,17 Similar symptoms can be induced by iatrogenic removal of CSF. Traction on the cranial nerves provokes accompanying symptoms like double vision (abducens nerve), hypesthesia (trigeminal nerve) and vestibulo-cochlear symptoms (vestibulo-cochlear nerve). Auditory and vestibular symptoms arise from pressure changes in the perilymph. 17 Strain on the cerebral bridging veins can lead them to rupture, with consequent subdural bleeding and hematoma formation (Figure 2). 18

T1-weighted contrast-enhanced magnetic resonance imaging (MRI) of a 34-year-old SIH patient with bilateral chronic subdural hematomas (arrow outlines). Chronic subdural hematomas in young patients, particularly if bilateral, should always prompt a search for a spinal CSF leak. Note also the dural enhancement as a typical sign of SIH (arrows). CSF: cerebrospinal fluid; SIH: spontaneous intracranial hypotension.
Symptomatology
Orthostatic headache is the hallmark symptom of SIH. 2 Early in the course of the disease, the headache is typically severe and bilateral, similar to postpuncture headache. Usually, the complaint sets in a few seconds to minutes after assuming the upright position.
Low flow leaks might become symptomatic only after several hours in the upright position, and some patients experience the so-called second half of the day headache. 19,20 When lying down, the symptoms improve quickly, usually within 15–30 min. However, some residual symptoms may persist even when lying flat. 4,14,20 The headache can be diffuse or have a more localized—frontal, temporal, or occipital—character. 4,14
Concomitant symptoms are frequently present and include nausea, vomiting, neck pain, vertigo, visual disturbances, tinnitus, and a sensation of pressure in the inner ear. 2,8,18,21 Some patients have no headache at all but only complain of cochlear-vestibular symptoms. 8 Occasionally, patients report double vision, facial hyposensibility, galactorrhoea, cognitive decline, or upper extremity paresthesia. 2,5,8 Rare cases of transtentorial and transforaminal herniation accompanied by a decline of vigilance, coma, or vascular infarcts have been described. 2,22 –24
Eye movement disorders are the most frequent finding during clinical examination. Most cases concern the abducens nerve, less frequently the oculomotor nerve. 25,26
With increasing duration of the disease, the orthostatic nature of the symptoms may wane; this makes the diagnosis much more challenging and it is often missed. 8,18,20,27 Some patients suffer from chronic daily headaches or headaches during the second half of the day. 8,27 In rare cases, symptoms are not aggravated and may not even worsen in the upright position, are only intermittently present, and are related to exercise or might even present as a thunderclap headache. 4,8,21 In clinical practice, it is essential to recognize the dynamic nature of the complaint characterized by an increasingly vague and nonspecific character with increasing duration of the disease.
SIH is an important cause of chronic subdural hematomas in young and middle-aged patients (<60 years). A spinal CSF leak can be demonstrated in one quarter of these patients, particularly in those who have bilateral hematomas, several relapses, and no history of trauma 28 (see Figure 2).
Traction on cerebellar veins through downward displacement of the cerebellum might lead to chronic microhemorrhages with subsequent superficial siderosis of the central nervous system (see below). Typically, the affected patients present with sensorineural hearing deficits and cerebellar ataxia.
Diagnostic workup
In typical cases with new onset, violent headaches that occur within seconds or minutes of assuming an upright position, the diagnosis is straightforward. But in order not to miss the diagnosis in patients complaining of chronic headaches without the typical postural dependence, one should always enquire about the exact course of the symptoms. In particular, an orthostatic component early in the course of the disease can give an important hint. An initially orthostatic headache can become chronic and acquire a less typical, persistent, intermittent, or even paradoxical (aggravated in the horizontal position) character. The temporal relation with positional changes, a trigger, previous lumbar puncture, and concomitant symptoms should be elicited. Interestingly, even after several years, many patients are able to recall the exact day and situation when the complaint began.
The International Classification of Headache Disorders (ICHD-3) diagnostic criteria for SIH are listed in Table 2. In principle, two criteria need to be fulfilled to make the diagnosis 1 :
Diagnostic criteria.


Typical signs of SIH on axial MRI: T1w contrast-enhanced sequences (left) display a strong dural enhancement (arrows). T2w images (right) show narrow bilateral subdural hygromas over the convexity. Note also the convex bulging of the superior sagittal sinus on both sequences (arrow outlines). SIH: spontaneous intracranial hypotension.

Sagital T1w contrast-enhanced MRI of the same patient before (left) and after (right) surgical closure of a spinal CSF leak. Note the flattening of the pons, obliteration of the perichiasmatic and prepontine cisterne, prominent pituitary, and collapsed lateral ventricle on the left image (arrows). CSF: cerebrospinal fluid.
A lumbar puncture is not required to make the diagnosis. 1 The opening pressure is neither sensitive nor specific. 29,30 In our own series, lumbar opening pressure was normal in more than 50% of patients with a confirmed spinal CSF leak. However, lumbar infusion testing has been shown to be superior to simple lumbar puncture. Using this technique, the parameters of CSF dynamics are assessed in detail by infusing sterile fluid intrathecally, while continuously measuring the pressure. 29
The first diagnostic step in suspected SIH is usually a cranial MRI, where more than 80% of patients display typical signs, and other forms of structural headache disorders can therefore be excluded. 2,4
The most important sign on cranial MRI is a diffuse dural enhancement and subdural hygromas (see Figure 3). 2,18 Other typical signs are listed in Table 3 and illustrated in Figure 4. 8,14 A spinal MRI might display extrathecal fluid and thereby make the diagnosis, too. Nevertheless, a spinal MRI usually does not show the exact segmental location of the leak.
Imaging signs on cranial MRI.

As an emerging technique, transorbital optic nerve sheath ultrasound offers a noninvasive screening tool and an easily repeatable follow-up examination after treatment. 31 The optic nerve sheath diameter, in particular the change measurable between the supine and the upright position, allows conclusions to be drawn about the filling pressure of the CSF space.
After the diagnosis has made according to ICHD-3, conservative therapy and epidural blood patching are indicated. Patients presenting with intractable symptoms should be investigated for the exact site of leakage (see Figure 5). This step is challenging and necessitates a dedicated neuroradiological team with the relevant expertise.
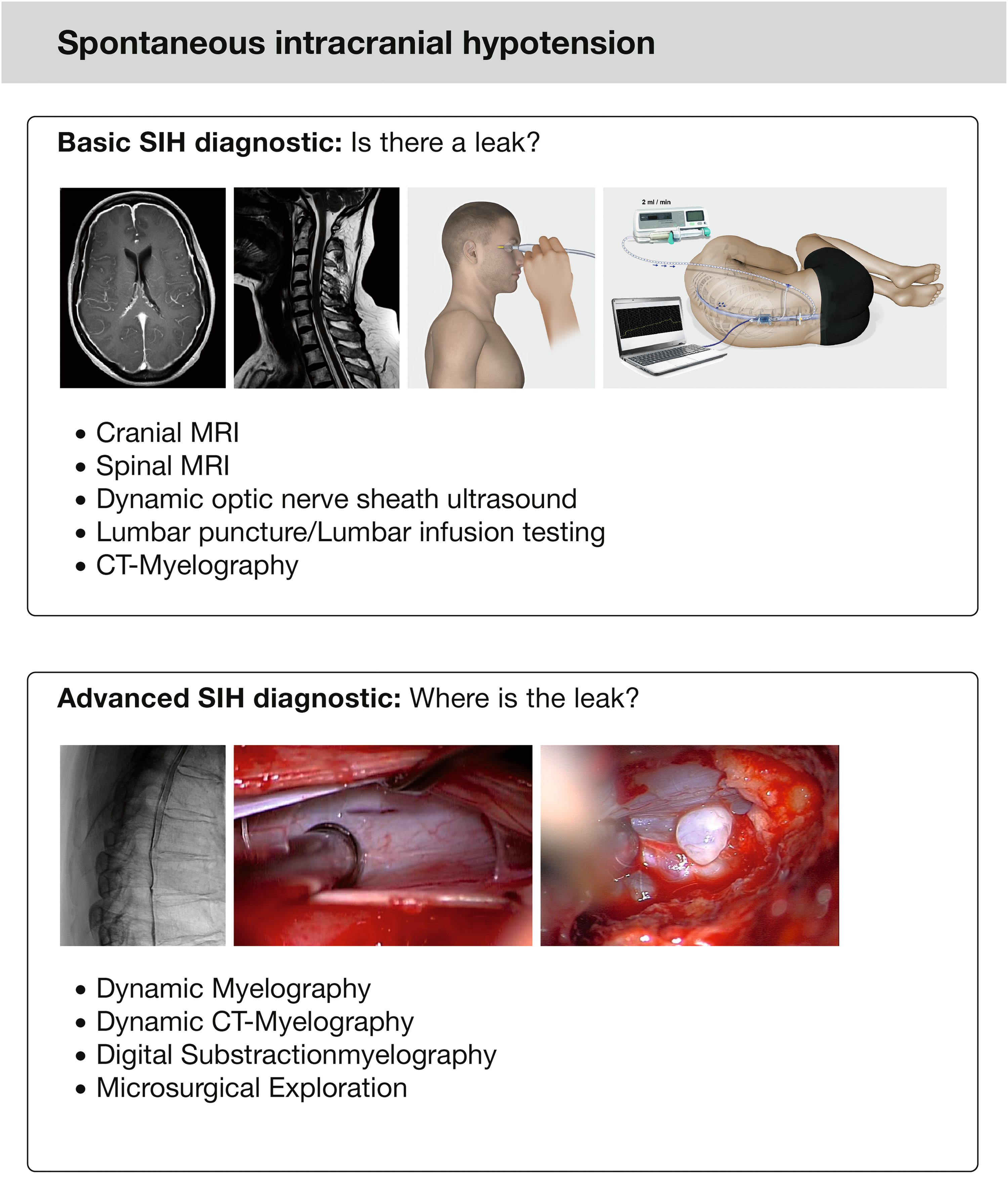
The diagnostic workup of SIH can be thought of a two-step process. While the first step aims at proving the presence of CSF leakage, the second step aims at precisely localizing the site of leakage and is a prerequisite for surgical treatment. CSF: cerebrospinal fluid; SIH: spontaneous intracranial hypotension.
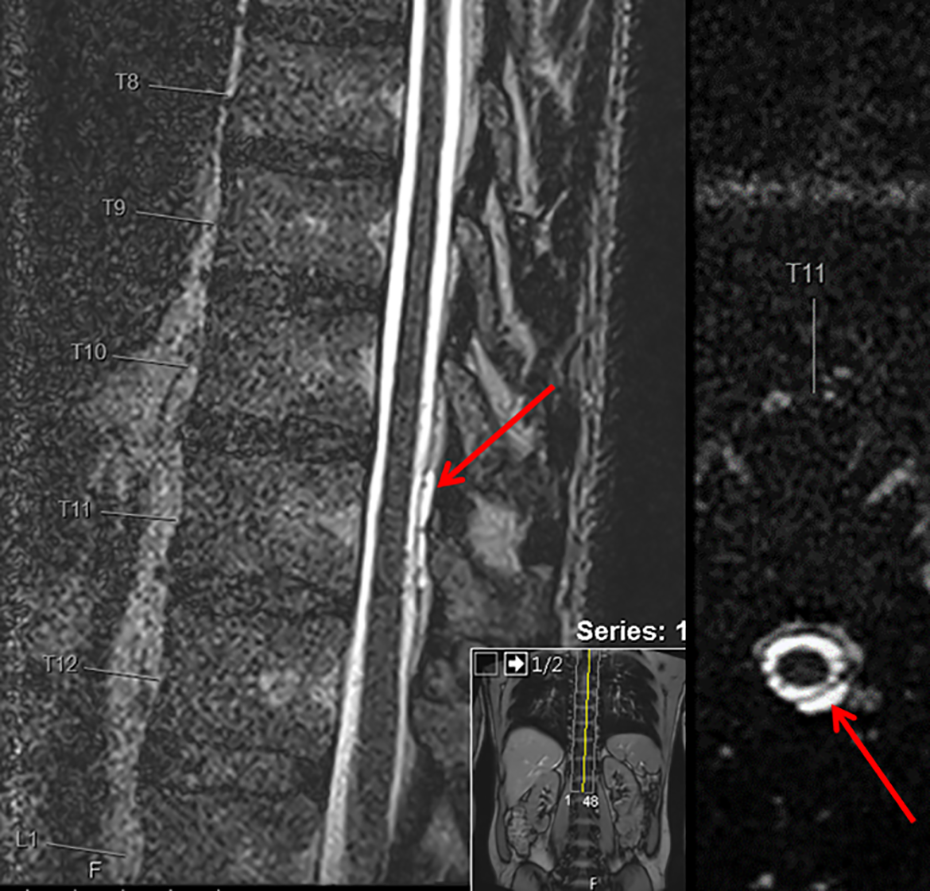
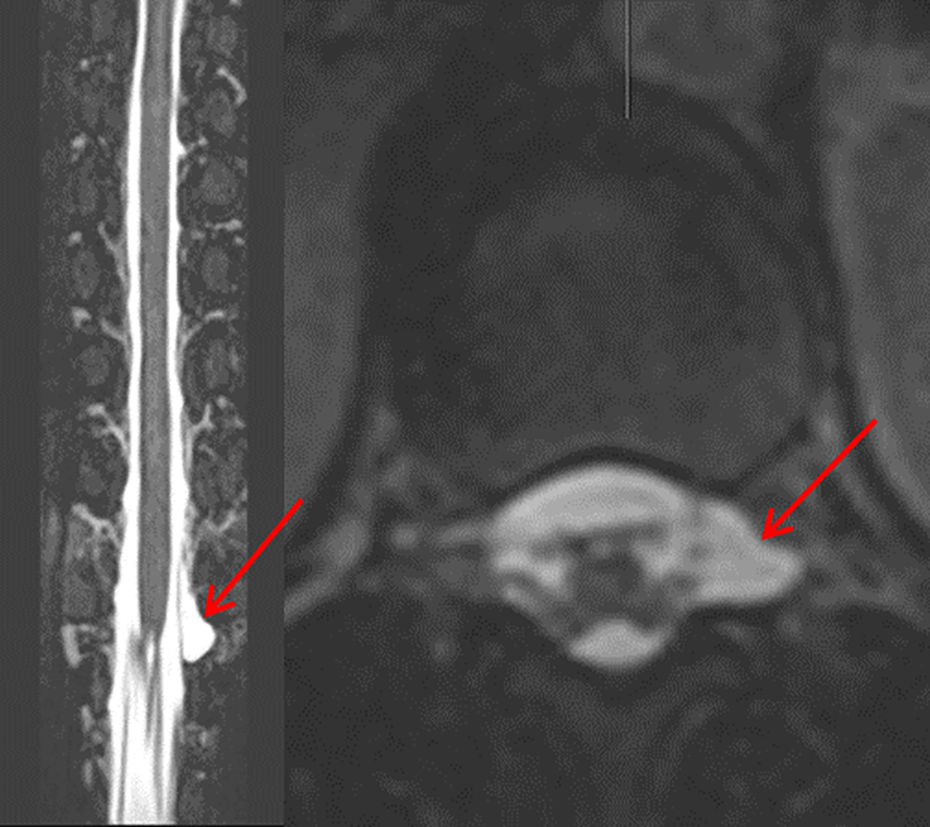
Spinal MRI with heavily T2-weighted sequences and fat suppression typically display extrathecal fluid extending over multiple levels. 2,8 Furthermore, meningeal diverticula can frequently be visualized, although their pathological significance is not entirely clear (see Figures 6 and 7). One study demonstrated a trend toward a larger proportion of patients with SIH harboring such diverticula compared with a healthy population, but the difference did not reach statistical significance. 13 Large and irregular-shaped meningeal diverticula are suspicious and can be associated with a CSF leak. 8 However, in 44% of healthy volunteers in the aforementioned study, spinal meningeal diverticula were also found. 13 Currently, only a dynamic study with intrathecal contrast application (see below) is able to verify a CSF leak in the region of a diverticulum. Intrathecal injection of Gadolinium for MR-myelography is considered an “off-label” use and in our experience offers little diagnostic advantage.
Sagittal (left) and axial (right) native T2w spinal MRI displaying an extrathecal collection of CSF (arrows). CSF: cerebrospinal fluid.
Coronal (left) and axial (right) T2w spinal MRI demonstrating a suspected meningeal diverticulum in the region of the left T12 nerve root (arrows).
The gold standard for proving a spinal CSF leak remains CT-myelography. It provides a good spatial resolution and an excellent visualization of bony microspurs (see Figure 8), although the exact site of leakage usually remains concealed. For visualization of the exact site of leakage, dynamic contrast examinations are used: dynamic myelography, dynamic CT-myelography, and digital subtraction myelography.

Left: Dynamic myelography with ventral contrast leakage at the Th6/7 level (arrow). Right: CT-myelography reveals a bony microspur causing a CSF leak (arrow). CSF: cerebrospinal fluid.
Dynamic myelography and digital subtraction myelography offer better temporal resolution and thereby allow the exact level of leakage to be localized. The examiner can track the spread of contrast agent inside the spinal canal and finally the leak into the epidural space under fluoroscopy and during positional changes (see Figure 7). With digital subtraction myelography, one is able to detect direct CSF-venous fistulas. 32
To date, no evidence is available regarding the superiority of one dynamic examination over another. However, all of them are associated with a significant exposure to radiation and some of them even necessitate general anesthesia. Therefore, they are applied only in the presurgical evaluation of therapy-refractory patients with intractable symptoms.
Some authors mention radionucleide cisternography, 3,18,33 but this exam does not allow exact localization of the leak and, in our opinion, provides no additional information.
Postural tachycardia syndrome (POTS) is an important differential diagnosis in patients being examined for SIH. Usually, it manifests with orthostatic vertigo, coat-hanger neck pain, concentration difficulties, nausea, and presyncope, but some patients complain of orthostatic headache as the sole manifestation. 34 Female patients in their 30s and 40s are primarily affected. Diagnosis can be made by a tilt table examination demonstrating a rise in heart rate when in the upright position of 30 bpm or up to a frequency of more than 120 bpm. 35 In fact, clinical symptoms and results of autonomic testing might even overlap in SIH and POTS. 36
Therapy
Conservative therapy consists of bedrest, hydration, and liberal caffeine intake (e.g. 2 × 200 mg). If symptoms persist, a lumbar epidural blood patch (EBP) is the cornerstone of treatment. Thereby, 15–50 cc of autologous blood are injected into the lumbar epidural space. This should be followed by 12–24 h of bedrest in a horizontal or Trendelenburg position. 2,18 The injected blood has been shown to disseminate over several spinal levels, sometimes up to the cervical spine. 37 The success rate of an EBP is in the range of 58–77% and it can easily be repeated several times. 2,5,18,38,39 Many patients benefit from repeated blood patches, which sometimes have a cumulative effect. 8 Usually, the effect of an EBP begins immediately after the intervention.
As a pragmatic approach, and depending on the severity of the symptoms, at least one to three EBP should be applied in patients with persistent symptoms before further diagnostic testing to localize the precise site of leakage. 21,39,40
There is disagreement as to determine whether a CT-guided targeted blood patch to the site of leakage is more effective than a “blind” lumbar EBP. Although some authors favor a targeted EBP, 41 –47 based on our own experience with patients, we refrain from targeted EBP to the cervico-thoracic region due to the greater risk of neurological injuries in the absence of any additional benefit over a standardized EBP to the level L3/4.
Alternative treatment strategies encompass the injection of fibrin glue at the site of leakage or wearing an abdominal binder. In emergency situations, with impaired consciousness and impeding herniation, immediate supine or Trendelenburg positioning and an intrathecal infusion with sterile Ringer’s solution or normal saline solution are indicated. 18,22,48
Microsurgical treatment
Symptoms persist in 10–30% of patients despite repeated EBPs. 10,39,42,46 At this point, a second diagnostic step, namely localizing the precise level of leakage by the above-mentioned dynamic techniques, is indicated. If the leak is clearly visualized, the patient can benefit from targeted, causative surgical therapy. The microneurosurgical closure of a spinal CSF leak is technically demanding but is feasible via a dorsal approach (see Figure 9). 49 The typically longitudinal dural tear with a length of 4–10 mm can usually be directly sutured. Formerly, adjuvant techniques like epidural packing, wrapping of a nerve root, or dural augmentation were often used. 4,33,50 Lateral meningeal diverticula can be ligated or closed with an aneurysm clip. 4,51

Left: Microsurgical appearance of a meningeal diverticulum. Right: Visualization of a ventral, longitudinal dural tear (arrow) on transdural dorsal approach.
Patients with a spinal CSF leak and chronic subdural hematomas represent a particular population needing a distinct approach to management. Simple trepanation and drainage of chronic subdural hematomas in this situation is potentially dangerous and can precipitate downward herniation with serious consequences. 22,24,52 Furthermore, relapse is highly likely if there is ongoing CSF loss through a spinal leak. 22,28,53 The spinal CSF leak should ideally be treated before or at worst shortly after the drainage of a subdural hematoma. 2,54 On the other hand, it may be hazardous to postpone evacuation of a subdural hematoma due to the suspicion of a spinal CSF leak. Surgery for space-occupying hematomas must not be delayed, but care should be taken not to remove additional excessive CSF with subdural or subgaleal suction devices. To avoid these pitfalls, one needs to be aware of them and adapt the treatment strategy to the individual.
Prognosis
SIH is a benign disease in most cases, but rare complications with subdural bleeding and subsequent coma can lead to life-threatening situations. The disease is often self-limiting or the patient recovers under conservative treatment. 8 Most patients can be successfully treated with an EBP. Surgical treatment is indicated only in one out of five patients with persisting symptoms.
If the site of leakage is precisely localized and treated, the results of microsurgery are very good and the orthostatic symptoms resolve completely in over 90% of cases. After successful surgical closure of a CSF leak, relapses are rare. 10
Closure of the CSF leak in a timely manner seems to be an important prognostic factor, because, in our experience, restoration to the original condition is more difficult with increasing duration of disease. If the diagnosis of SIH is missed, the symptoms can become chronic and change in character after several weeks. Because of the vague and nonspecific nature of symptoms at this stage, the cause of the complaint can be missed.
The changing nature of the complaints when a CSF leak remains untreated is a well described phenomenon and some authors use the term post-SIH headache to describe them. Typically, these symptoms are no longer orthostatic but are often intermittent and associated with mood changes and sleep disturbances. 2 The putative underlying pathophysiology changes over time and the reason why, in some instances, residual symptoms may persist even after successful closure of the spinal CSF leak has yet to be elucidated.
Importantly, an exacerbation or a change of character of the headache should prompt an investigation to exclude a chronic subdural hematoma or cerebral venous thrombosis, particularly where there is sudden loss of the orthostatic component or impaired consciousness. 2,55 Cerebral venous thrombosis as a complication of SIH occurs in 2% of patients. 56
Emerging issues
Superficial siderosis of the central nervous system is a progressive, irreversible disease caused through sequestration of hem iron from chronic microbleeding (see Figure 10). 57 –60 The hallmark symptoms are progressive cerebellar ataxia and a sensorineural hearing deficit. 50 –61 While etiologically there is often a history of trauma, tumor, arteriovenous malformation, or brachial plexus injury, the cause of around a third of cases remains unclear. 58 A spinal CSF leak has been reported to be present in up to half of those cases. 59,60,62 –65 A proposed mechanism is the caudal displacement of the cerebellum with subsequent venous tearing and microhemorrhage. 63 Because of the progressive nature of the disease, a spinal CSF leak should be actively sought and surgically closed if present. 57,59 –61
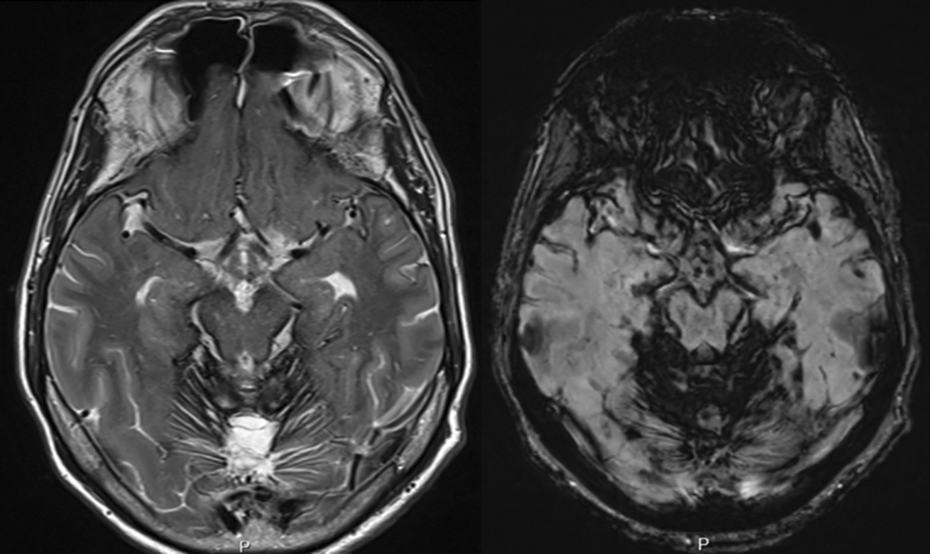
Axial MRI showing superficial siderosis of the central nervous system: T2w images (left) demonstrate a pathognomonic hypointensity around the cerebellum, particularly the cerebellar vermis, the quadrigeminal plate, and the brainstem. On susceptibility weighted imaging (SWI) sequences, the iron deposits are visible as dark spots on the cerebellum.
Recently, a link between SIH and idiopathic thoracic spinal cord herniation was proposed, as many cases of cord herniation occur at the level of the disk space with osteophytes and extrathecal CSF present. 66 –69 Idiopathic spinal cord herniation most frequently presents with Brown-Séquard syndrome or progressive myelopathy. 67,70 Usually at the thoracic level, where the natural kyphosis brings the spinal cord into the close vicinity of the ventral dura and the vertebral body, a degenerative microspur may provoke a ventral dural defect, which is subsequently tamponaded by the herniating spinal cord. 67 While most of the patients affected do not suffer from headache, cases of progressive development of myelopathy after resolution of orthostatic headache have been reported and support that theory. 66 Surgical treatment strategies are similar to those for dural defects in patients with SIH and involve reduction of the hernia and primary or patch repair of the defect. 67,68,70
Conclusion
Orthostatic headache is the hallmark symptom of SIH. Principally, SIH is a spinal disease caused by a spinal CSF leak. While usually a benign self-limiting disease of short duration, life-threatening complications can occasionally occur.
The first diagnostic step is a cranial MRI. Lumbar puncture is not a prerequisite for the diagnosis of SIH. The cornerstone of treatment is a lumbar EBP. It can be applied repeatedly and does not necessitate the exact localization of the site of leakage. Twenty percent of patients do not respond to conservative treatment and EBP. At this point, further diagnostic systematic testing to localize the exact site of leakage is indicated.
A bony microspur penetrating the ventral dura can be found in 80% of patients with intractable symptoms. Originating from the disk level, the microspur slits the dura like a knife and causes a persistent CSF leak. Cases refractory to conservative therapy can be cured by microsurgical treatment.
Many new findings and concepts in this still young field of research are emerging as a result of the vigorous efforts of several groups worldwide. Some of them are speculative and all of them will have to be proven. However, various interesting developments that will alter daily clinical practice can be expected in the near future. Diagnosis will most likely be facilitated by new MRI sequences. By getting to grips with CSF dynamics, our pathophysiological understanding of this disease is growing. Nevertheless, many unresolved issues remain in this sometimes debilitating disease and patient care still needs to be optimized.
Footnotes
Acknowledgment
The authors would like to thank Susan Kaplan for editing the manuscript and Anja Giger for designing the figures.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.