
Abstract
A 62-year-old female with a history of stroke due to cerebral arteriosclerosis suffered from recurrent fainting (<10s) provoked by rapid head movements up to four times per month for at least two years. There was no evidence of new strokes in repeated MRI and no high-grade vertebral artery stenosis on catheter angiography. Electroencephalography and cardiovascular workup were normal. Because fainting was head-position triggered, carotid massage was performed, demonstrating transient sinus arrest and carotid sinus syndrome (CSS) was diagnosed. After pacemaker implantation, episodes disappeared. Based on this case we discuss the diagnostic approach and also potential pitfalls and limitations of CSS.
Case description
A 62-year old female podiatrist with a history of stroke due to left-sided internal carotid artery stenosis at age 59 years suffered from short (lasting seconds), recurrent episodes with dizziness and sudden loss of consciousness up to four times a month for a period of at least 2 years. Events were provoked by rapid head movements, for example, during walking, but also at rest. Typically, fainting occurred when she worked overhead with her arms elevated and the head reclined. For example, hanging up the laundry or taking things down from shelves triggered the spells. Fall-related injuries such as deep lacerations at the head and the arms were linked to these transient losses of consciousness. Further consequences included social withdrawal, avoidance behavior, and the development of depressive symptoms.
In repeated brain magnetic resonance imaging scans, there was no evidence of recent cerebrovascular ischemia. Electroencephalographys and cardiovascular workup including electrocardiography (ECG) monitoring over 7 days, however, without recording a fainting spell, were normal. Although initially postulated based on magnetic resonance angiography and duplex, high-grade stenoses of the vertebral arteries bilaterally were not confirmed by catheter angiography (Figure 1(a) and (b)) and on the internal carotid arteries no significant (i.e. ≥50%) stenoses were noted either. Finally, right-sided carotid sinus massage was performed in supine position demonstrating transient sinus arrest for about 5 s (Figure 1c), and a cardioinhibitory carotid sinus syndrome (CSS) 1 was diagnosed. There was no clinical evidence for cerebral ischemia provoked by the carotid massage. After pacemaker implantation (DDD type, i.e. with dual chamber pacing and sensing, both triggered and inhibited mode), 2 no further episodes occurred (11 months follow-up).
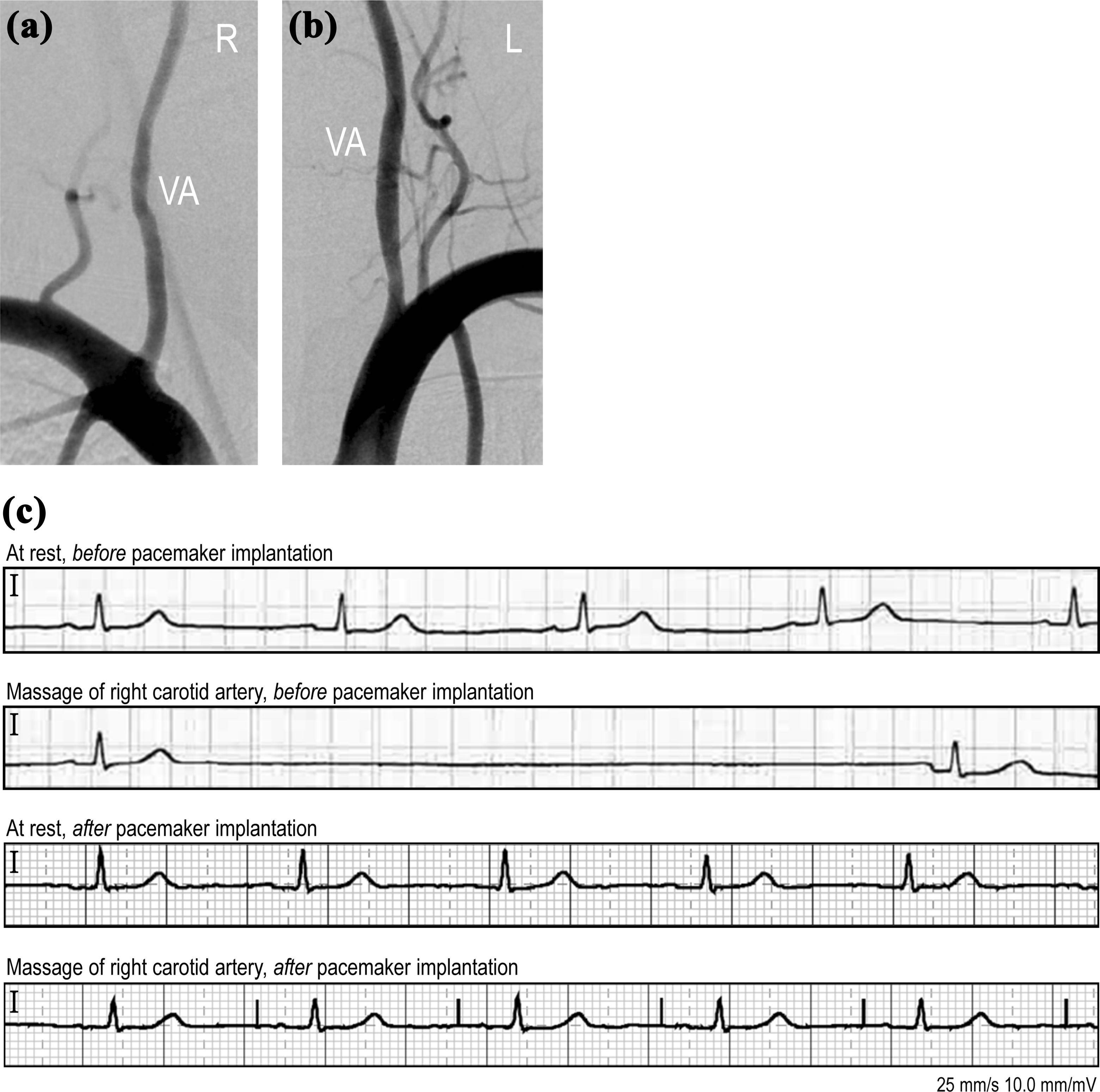
(a, b) Catheter angiography demonstrated minor stenosis (<30%) only of left VA and was otherwise normal. (c) ECGs before and after pacemaker implantation. Before treatment, carotid sinus massage triggered asystolia. After implantation, a pacemaker-triggered heartbeat was seen during carotid sinus massage. VA: vertebral artery.
CSS is a frequent cause of transient loss of consciousness affecting primarily subjects above the age of 50 years, with prevalence rates as high as 22–68% of all patients with unexplained syncope being reported. 1,3 Associated factors include hypertension, general atherosclerosis and coronary heart disease, 4 tight collars, neck tumors, and neck surgery/irradiation may trigger the reflex. 3 Neurodegenerative processes in the medulla oblongata and impaired function of the baroreceptors in the internal carotid arteries were postulated to be involved in its pathophysiology. 1 However, the specific mechanisms leading to hypersensitivity of the carotid sinus reflex are still largely unknown. 5 Two different types of carotid sinus syndrome can be distinguished. In the first type, called cardioinhibitory CSS ventricular asystole for more than 3 s reproducing the spontaneous symptoms is seen. In the second type, referred to as vasodepressor CSS, the blood pressure drops more than 50 mmHg while ventricular asystole is either absent or lasting less than 3 s. 6 In some cases, both asystole lasting more than 3 s and a drop in blood pressure of more than 50 mmHg can be observed; this condition has been termed mixed CSS. 6 Noteworthy, neurologic and cardiovascular complications seem to be rare after carotid sinus massage and therapeutic consequences may be significant. 1 According to a recent review, neurologic complications due to cerebral embolism occur at a rate of approximately 1 in 1000 patients, being transient in most cases. 7 Nonetheless, persistent deficits may result in major disability 8 or even death 9 in selected cases. Contraindications for carotid sinus massage include recent (i.e., within the last three months) transient ischemic attacks, strokes, and myocardial infarctions. 6 Carotid bruits are also considered a contraindication, except carotid Doppler excludes significant stenosis. 6 Overall, in elderly patients with unexplained syncope—especially if triggered by certain head positions—monitored carotid sinus massage should be performed by the specialist and only after contraindications have been excluded.
Footnotes
Authors’ contributions
BZ: acquisition and interpretation of the data, drafting the manuscript. JS: acquisition of data, revising the manuscript. ML: interpretation of the data, revising the manuscript. AAT: interpretation of the data, revising the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Steffel has received consultant and/or speaker fees from Amgen, Astra-Zeneca, Atricure, Bayer, Biosense Webster, Biotronik, Boehringer-Ingelheim, Boston Scientific, Bristol-Myers Squibb, Cook Medical, Daiichi Sankyo, Medtronic, Novartis, Pfizer, Sanofi-Aventis, Sorin, St. Jude Medical/Abbott, and Zoll. Her reports ownership of CorXL. Dr Steffel has received grant support through his institution from Bayer Healthcare, Biosense Webster, Biotronik, Boston Scientific, Daiichi Sankyo, Medtronic, and St. Jude Medical/Abbott. Dr. Zörner, Prof. Linnebank and Dr. Tarnutzer do not report any conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.