
Abstract
Vertigo and dizziness can be related to migraine in various ways: causally, statistically or, quite frequently, just by chance. Migrainous vertigo (MV) is a vestibular syndrome caused by migraine and presents with attacks of spontaneous or positional vertigo lasting seconds to days and migrainous symptoms during the attack. MV is the most common cause of spontaneous recurrent vertigo and is presently not included in the International Headache Society classification of migraine. Benign paroxysmal positional vertigo (BPPV) and Ménière's disease (MD) are statistically related to migraine, but the possible pathogenetic links have not been established. Moreover, migraineurs suffer from motion sickness more often than controls. Persistent cerebellar symptoms may develop in the course of familial hemiplegic migraine. Dizziness may also be due to orthostatic hypotension, anxiety disorders or major depression which all have an increased prevalence in patients with migraine.
Introduction
Dizziness and vertigo rank amongst the most common complaints in the general population and are frequently reported by patients with migraine. In individual migraineurs, the critical question is whether the dizziness or vertigo is related to migraine or not.
This review will explore the association of migraine with: (i) vestibular vertigo, (ii) motion sickness, (iii) cerebellar symptoms and (iv) non-vestibular dizziness. We thereby distinguish between vertigo, which is a vestibular symptom and dizziness, which is not. Patients may report a variety of different sensations that need to be carefully inquired about: rotational vertigo or other illusory sensations of motion indicate vertigo, i.e. vestibular symptoms, while a sensation of lightheadedness, giddiness, unsteadiness, drowsiness or impending faint implies dizziness of non-vestibular origin. This distinction can be made in most cases. However, a residual grey area remains, either as a semantic problem or because mild vestibular dysfunction may present with dizziness rather than vertigo. Moreover, in the medical literature, a clear differentiation between vertigo and dizziness is sometimes not made. In the following, we will use quotation marks to denote an ambiguous use of the term dizziness.
Approximately 16% of the adult population are affected by migraine at some time in their lives (1) and the lifetime prevalence of ‘dizziness’ (comprising both vertigo and non-vestibular dizziness) has been found to be 23% in a large population-based survey (2). Thus, about 3–4% of the general population would be expected to have both migraine and ‘dizziness’ by pure coincidence. However, there is evidence that migraine and ‘dizziness’ actually concur much more often. In a recent study, the prevalence of migraine according to the criteria of the International Headache Society (HIS) (3) was 1.6 times higher in 200 dizziness clinic patients than in 200 age- and sex-matched controls from an orthopaedic clinic (38%vs 24%, P < 0.01) (4). In particular among patients with unclassified or idiopathic vertigo, the prevalence of migraine has been shown to be elevated (5–7). Conversely, 53 out of 200 unselected migraine patients reported vertigo, compared with nine out of 116 patients with tension headache (27%vs 8%, P = 0.01) (8). The association between migraine and vertigo was significant, both for vertigo with headache and for vertigo in the headache-free period. In another study, migraine patients reported about 2.5 times more vertigo and also about 2.5 times more dizzy spells during the headache-free phase than controls not suffering from headaches (9). In summary, the available data indicate a more-than-chance association of migraine with vertigo and dizziness.
Migraine and vertigo
Patients with both episodic vertigo and migraine have been reported from the early days of clinical neurology (10). However, systematic studies on the interrelations of migraine and vertigo have been undertaken in the last two decades only. Both from the clinical and from a research point of view, it is useful to assign the association of migraine with vertigo to one of three categories: (i) vertigo that is causally related to migraine –migrainous vertigo, (ii) vertigo syndromes that are not caused by migraine but show a statistical association with migraine, possibly as a result of an association of both conditions with a third factor, or (iii) vertigo that co-exists with migraine in the same patient just by coincidence.
Migrainous vertigo (MV)
In the last decades, a syndrome that causally links vertigo to migraine has started to take shape from published case series. Comprehensive clinical observations suggest that vertigo can be an independent migrainous symptom which usually does not correspond to an aura and which may dissociate from headaches.
An early manifestation of migrainous vertigo is benign paroxysmal vertigo of childhood which is characterized by brief attacks of vertigo or disequilibrium, anxiety and often nystagmus or vomiting that occur recurrently for months or years in otherwise healthy young children (11). Many of these children later develop migraine, often years after vertigo attacks have ceased (12). A family history of migraine in first-degree relatives is twofold increased compared with controls (13). In a population-based study, the prevalence of recurrent vertigo probably related to migraine was estimated at 2.8% in children between 6 and 12 years (13).
In adults, the term benign recurrent vertigo has been used for a vestibular disorder that shows some features in common with migraine which include precipitation by alcohol, lack of sleep or emotional stress, female preponderance, an individual history or a positive family history of migraine (14, 15). Subsequently, various names have been introduced such as vertigo as a migraine equivalent (16), migraine-associated dizziness (17, 18), migraine-related vestibulopathy (19, 20), vestibular migraine (21), or migrainous vertigo (4). Case series, which have included up to 100 patients, have highlighted additional features that provide evidence for the migrainous origin of episodic vertigo even in the absence of headache: the concurrence of visual auras, photophobia and phonophobia, relief by sleep and effectiveness of anti-migraine therapy (4, 14–25, 27). It should be noted that most authors have conceptualized MV as a vestibular disorder, but some have included unspecific dizziness as well (17, 19, 25).
MV may occur at any age (17, 19, 21). It has a female preponderance with a reported female-to-male ratio between 1.5 and 5 and 1 (4, 19, 21, 25). In most patients, migraine begins earlier in life than MV (4, 21). Some patients have been free from migraine attacks for years when MV first manifests itself (21). MV seems to occur more often in patients with migraine without aura than in patients with migraine with aura (8, 18, 21, 25). Population-based prevalence studies are still lacking.
Clinical presentation of MV
Patients typically report spontaneous or positional vertigo. Some patients first experience spontaneous vertigo, which transforms into positional vertigo later in the attack (14, 15). Altogether, 40–70% of patients experience positional vertigo (but not benign paroxysmal positional vertigo) in the course of the disease (4, 8, 25). Head motion intolerance, i.e. episodic imbalance and illusory motion aggravated or provoked by head movements, is a frequent additional symptom suggesting a vestibular problem. Of note, migrainous vertigo and non-vestibular dizziness can co-exist in the same patient (17, 18, 25) but can be well differentiated in most cases. Nausea and imbalance are frequent but unspecific accompaniments of acute MV. Both duration and frequency of attacks can vary between patients and in individual patients over time. The duration of vertigo ranges from seconds to several hours and, sometimes, up to several days. For some patients, it may take several weeks to fully recover from an attack. The attacks may occur days, months or even years apart in an irregular fashion. Some patients experience clusters of short attacks of vertigo, lasting seconds to a few minutes. Such clusters can last for hours to days and patients may experience head motion intolerance between the short attacks. Overall, between 10 and 30% of patients have vertigo with the typical duration of a migraine aura, i.e. 5–60 min (4, 21). Attacks shorter than a migraine aura are not unusual and have been reported in 20–30% of patients while attacks lasting hours or days occur in 20–50% of patients (4, 17, 19, 21). MV often misses not only the duration criterion for an aura as defined by the IHS, but also the temporal relationship to migraine headaches: vertigo can precede headache as would be typical for an aura, may begin with headache or appear late in the headache phase. Many patients experience both attacks with and without headache (4, 17, 25). Quite frequently, patients have an attenuated headache with their vertigo as compared with their usual migraine (22, 25). In some patients, vertigo and headache never occur together (4, 17, 25). Absence or attenuation of migrainous headache during MV attacks may be due to an interaction of vestibular and trigeminal mechanisms as suggested by a study showing disappearance of headache or a decrease in headache intensity after caloric activation of the vestibular system during migraine attacks (26).
Along with the vertigo, patients may experience photophobia, phonophobia and visual or other auras. These phenomena are of diagnostic importance, as they may represent the only apparent connection of vertigo and migraine. They need to be specifically inquired about as patients often do not volunteer them.
Hearing loss and tinnitus are not prominent symptoms of MV but have been reported in individual patients with MV (19, 23, 25). Hearing loss is usually mild and transient, without progression in the course of the disorder. The frequency of cochlear symptoms and their temporal association with the vertiginous attacks has not been studied systematically. Cochlear symptoms have also been found in vertigo-free migraine patients (8).
In summary, the clinical presentation of MV is variable in many respects and the connection to migraine can be subtle. The repeated presence of migrainous symptoms along with the vertigo (migrainous headache, photophobia, phonophobia, auras) points to the correct diagnosis.
Clinical and neurotologic findings in patients with MV
The general neurologic and otologic examination and tests in the symptom-free period are unremarkable in most cases (17, 24). About 10–20% of MV patients have unilateral hypoexcitability to caloric stimulation and about 10% have directional preponderance of nystagmus responses (17, 21). Such findings, however, are not specific for MV, as they can be found also in migraine patients without vestibular symptoms (28) and in many other vestibular syndromes. Neuro-ophthalmological evaluation may reveal mild central oculomotor deficits in the absence of other brainstem or cerebellar signs (21).
A neurotologic study of 15 patients during the acute phase of MV showed imbalance in all patients but one, a peripheral type of spontaneous nystagmus in three, a central type of spontaneous nystagmus in four and a central positional nystagmus in four patients. A unilateral deficit of the horizontal vestibulo-ocular reflex was observed in three patients and saccadic pursuit in two (29). Overall, findings during acute MV pointed to central vestibular dysfunction in eight patients (53%), to peripheral vestibular dysfunction in three patients (20%), and were inconclusive with regard to the involved structures in four patients (27%).
Diagnostic criteria of MV
Like migraine itself, MV cannot be diagnosed by specific biological markers but only on the basis of history. To date, there are no internationally approved criteria for the diagnosis of MV. A recent proposal from our group uses operational clinical criteria modelled on the IHS classification of headaches (4). Operational diagnostic criteria, however, are a trade-off between sensitivity and specificity. Therefore, two separate diagnostic categories appear to be useful: definite and probable migrainous vertigo (Table 1). A diagnostic interview applying these criteria has been proposed recently (30).
Diagnostic criteria for definite migrainous vertigo
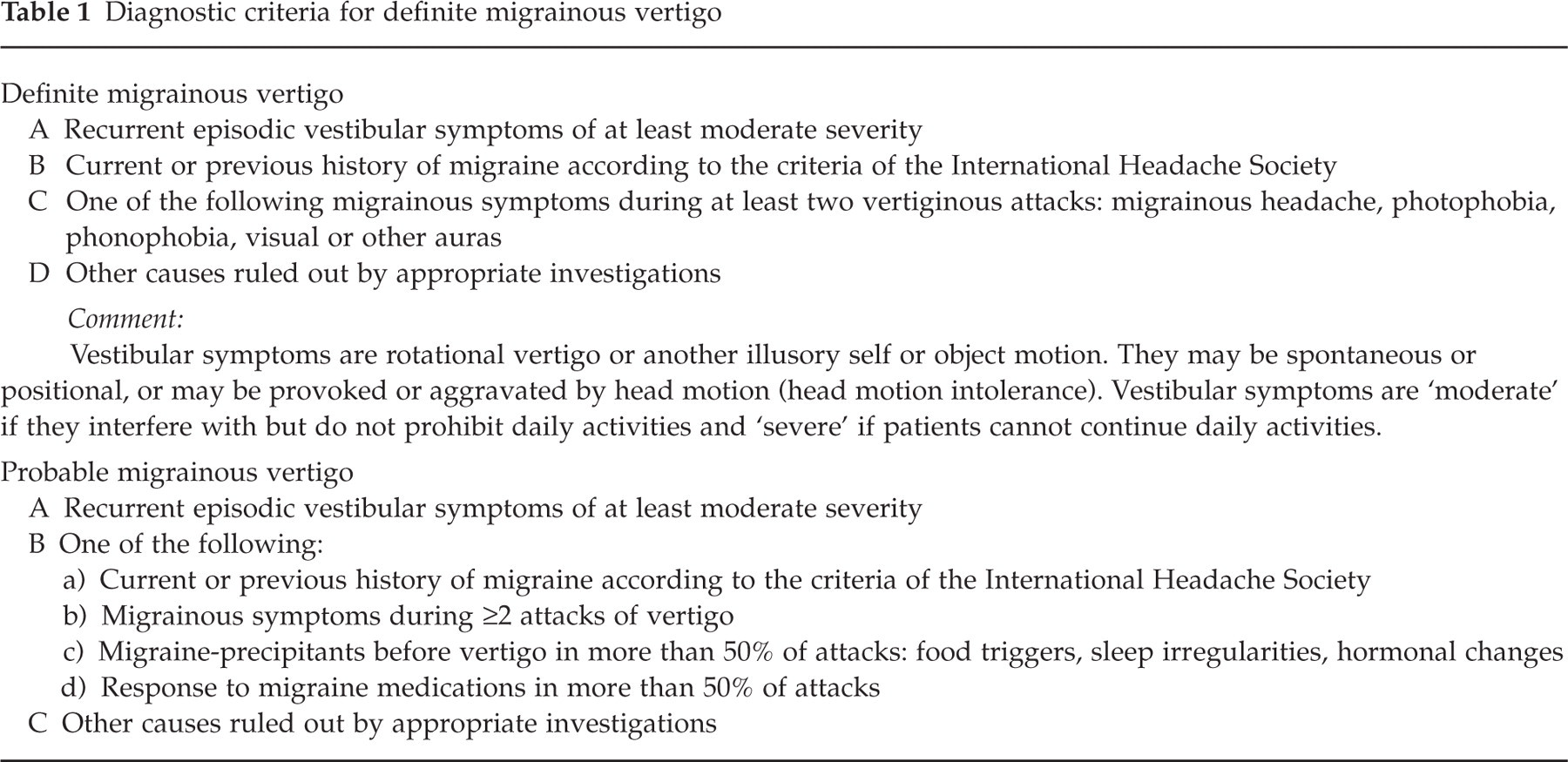
The criteria for definite MV are stricter than the inclusion criteria of most MV case series published so far. The prevalence of definite migrainous vertigo according to these criteria was 7% in a group of 200 consecutive dizziness clinic patients and 9% in a group of 200 migraine clinic patients (4). The clinical features of MV in 33 patients from our dizziness clinic fulfilling the criteria for definite MV are summarized in Table 2.
Clinical features of definite migrainous vertigo in 33 patients
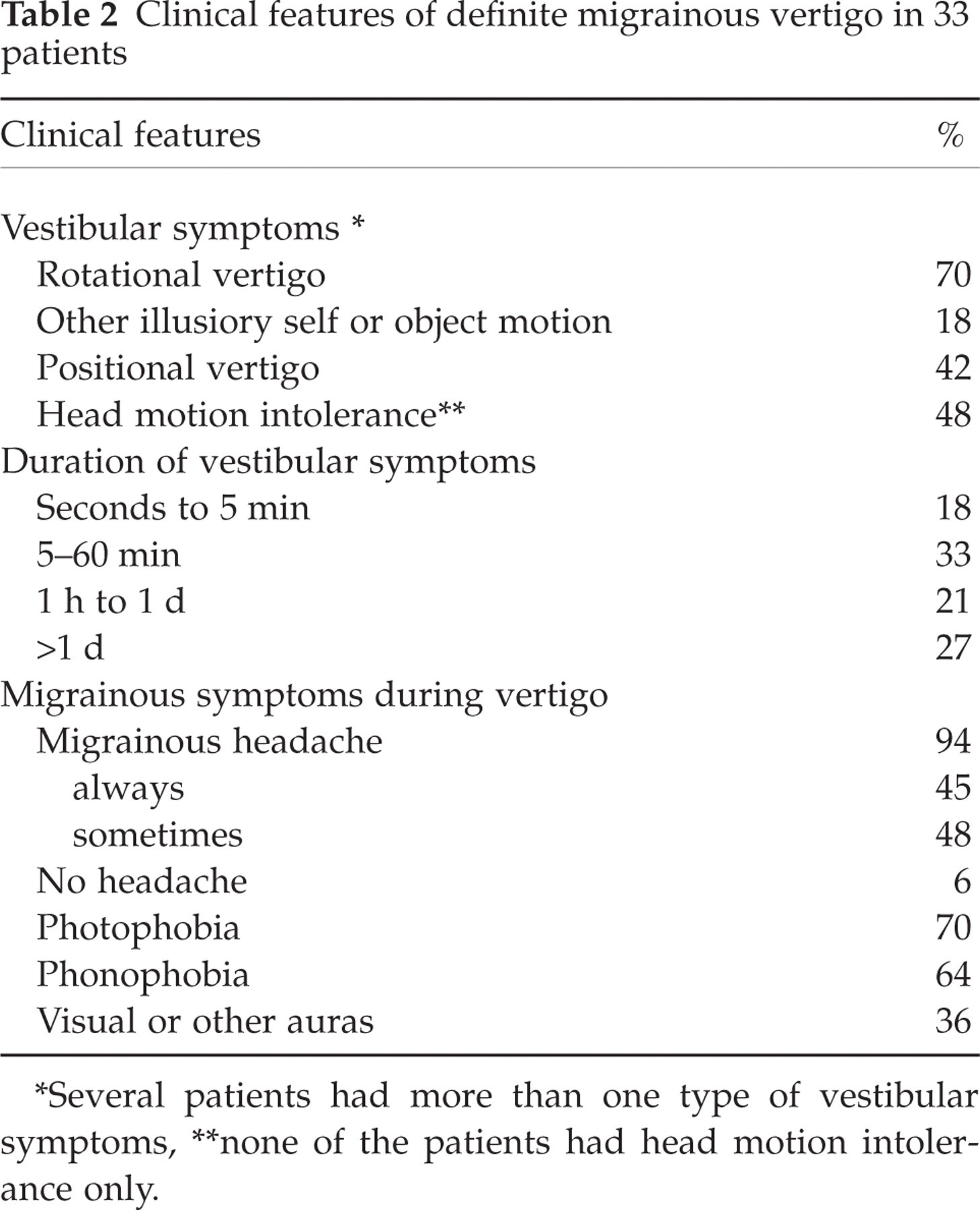
∗Several patients had more than one type of vestibular symptoms
∗∗none of the patients had head motion intolerance only.
Migrainous vertigo and the IHS classification of migraine
Vertigo is not included in the IHS classification as a migrainous symptom in adults except in the framework of basilar migraine (3), which involves vertigo in more than 60% of the patients (31). As an aura symptom of basilar migraine, vertigo should last between 5 and 60 min and should be followed by migrainous headache. In addition, in order to fulfil the IHS criteria for basilar migraine, a second aura symptom from the posterior circulation should be reported (e.g. dysarthria, double vision or bilateral paresthesias). In fact, less than 10% of MV patients in published case series fulfil the criteria for basilar migraine (4, 19, 21, 25), which makes basilar migraine an inappropriate category for these patients. As a consequence, most patients with MV cannot be classified with the current IHS criteria.
Differential diagnosis of MV
Differential diagnosis of MV should be guided by distinction of vestibular symptoms and non-vestibular dizziness and should consider the common causes of recurrent vertigo (Table 3). Of note, among 75 patients with migraine presenting to a neurological dizziness clinic, MV was only the third most common diagnosis after benign positional vertigo and psychiatric dizziness (e.g. due to panic disorder or depression) (4). MV of recent onset may be difficult to differentiate from early Ménière's disease, where cochlear symptoms may be lacking.
Recurrent vertigo in patients with migraine: differential diagnoses for migrainous vertigo

Pathophysiology of MV
The pathophysiology of MV is unclear. Spreading depression may play a role (17) when cortical areas are involved that process vestibular information. Several neurotransmitters which are involved in the pathogenesis of migraine (calcitonin-gene related peptide, serotonin, noradrenaline, dopamine), are also known to modulate the activity of vestibular neurones and could contribute to the pathogenesis of MV (17, 19, 25, 32). Recently, a synopsis of potential pathophysiological links between migrainous and vestibular mechanisms has been presented (30). Such interactions may involve the vestibular nuclei, the trigeminal system and thalamocortical pathways.
In the last decade, genetic defects of ion channels have been identified as the cause of various paroxysmal neurologic disorders. The finding of an abnormal voltage-gated calcium-channel gene in familial hemiplegic migraine (FHM) and episodic ataxia type 2 (EA-2) (33) – both of which can have vertigo and migraine headache as prominent symptoms – has prompted the search for a susceptibility gene for MV in the same region. So far, however, no such genetic defect could be identified (27, 34). In summary, none of the potential pathophysiological mechanisms for MV has been experimentally investigated. Therefore, they are all still highly speculative.
Treatment of MV
In many patients, MV attacks are severe, long and frequent enough to warrant acute or prophylactic treatment. However, evidence for effective treatment is scarce.
A few case reports suggest that medication used for migraine prophylaxis may be effective: propranolol (35), metoprolol (21), pizotifen (22), or flunarizine (21). Acetazolamide, which is not normally used for migraine prophylaxis (36), has also been applied successfully. A recent retrospective study reported a prophylactic effect of a stepwise treatment consisting of avoidance of food triggers, low-dose tricyclic antidepressants and a beta-blocker in more than 50% of patients (18). However, these findings are difficult to interpret in the absence of a control group and a well-documented pre-treatment period, as both frequency and duration of attacks vary considerably in the natural course of the disorder (17).
Treatment of acute MV with acute migraine medication can be attempted with ergotamine (21), sumatriptan (37, 38) and vestibular suppressants such as promethazine, dimenhydrinate and meclizine (37). A pilot randomised placebo-controlled trial of oral zolmitriptan for acute MV according to the above criteria showed inconclusive results due to low power (39). Multicentre trials with triptans administered subcutaneously or nasally for fast relief of migrainous vertigo are clearly needed.
Migraine and Ménière's disease
An association between Ménière's disease (MD) and migraine has been considered already by Prosper Ménière in 1861 (40). Sporadic accounts of headaches as an additional symptom in typical Ménière attacks have provided further reason to suspect a link between MD and migraine (41, 42). Subsequent studies of the prevalence of migraine in MD produced conflicting results (43, 44,) but a recent controlled study has provided well-documented evidence for such an association (45). The study compared 78 patients with idiopathic unilateral or bilateral MD according to the criteria of the American Academy of Otolaryngology (AAO) (46) with age- and sex-matched controls. The prevalence of migraine according to the IHS criteria was almost twice as high in the MD group than in the control group (56%vs 25%, P < 0.001). Furthermore, 35 (45%) of the patients with MD always experienced at least one migrainous symptom (migrainous headache, photophobia, aura symptoms) along with their MD attacks. Twenty-eight (36%) of MD patients had IHS migraine and always experienced at least one migrainous symptom (migrainous headache, photophobia, aura symptoms) along with their MD attacks (Table 4, A. Radtke, personal communication). The study illustrates that there are migraine patients with recurrent vertigo for whom it is not possible to differentiate with certainty whether they have migrainous vertigo or MD. The two conditions may share pathophysiological mechanisms such as neurotransmitter imbalances or ion-channel-dysfunction that lead to a spectrum of migrainous, vertiginous and cochlear symptoms. Of note, this diagnostic ambiguity between migrainous vertigo and MD will only rarely occur in unselected patients with migraine and vertigo, considering the rarity of MD compared with migrainous vertigo. As a rule of thumb, hearing loss is an occasional, mild and non-progressive feature in MV, while it is a regular accompaniment of MD progressing to severe hearing loss within a few years.
Migrainous symptoms during Ménière attacks in 44 patients with MD and IHS-migraine (%)

Migraine and benign paroxysmal positional vertigo
Benign paroxysmal positional vertigo (BPPV) is the most common cause of recurrent vestibular symptoms both in unselected patients (21, 47) and in migraineurs (4) presenting at a dizziness clinic. The diagnosis of BPPV is straightforward. Patients give a very typical account of recurrent short (10–20 s, maximum 1 min) attacks of rotational vertigo, which are provoked by certain changes in head position, like turning over in bed, lying down or sitting up, looking up or bending down. A positive positional test as described by Dix and Hallpike with a typical torsional nystagmus beating towards the undermost ear – frequently with an upbeating vertical component – confirms the diagnosis (48). Patients can be treated effectively with the Epley or Semont canalith repositioning manoeuvre (49–51). When the nystagmus is atypical, variants such as horizontal canal BPPV and central positional nystagmus should be considered.
Although clinically two separate entities, there is evidence for a link between migraine and BPPV. Migraine has been found to be three times more common in patients with idiopathic BPPV than in patients with BPPV secondary to trauma or surgical procedures (52). Moreover, migraine was two times more common in patients with idiopathic BPPV than in age and sex-matched controls (53). Genetic factors and vascular damage to the labyrinth have been discussed as pathogenetic mechanisms linking the two conditions (52).
Vertigo as a symptom of migrainous infarction
Migraine is associated with an incresed risk for stroke (54). Migrainous infarctions are rare and occur predominatly in the territory of the posterior cerebral artery (55, 56). Vertigo accompanied by other brainstem symptoms has been reported in individual patients with migrainous stroke (7, 57).
Migraine and motion sickness
Motion sickness occurs more frequently in patients with migraine (30 to 50%) than in controls with tension headache or in headache-free controls (about 20%) (8, 9). The association is more pronounced in children (58) and in migraine with aura (9). Findings from a study in crew members of a yacht race suggest an influence of the menstrual cycle on the occurrence of both motion sickness and headache (59). Migraineurs also report more ‘visual vertigo’ while looking at spinning objects (9). Headache, scalp tenderness and photophobia could be provoked by optokinetic stimulation in a recent study. Migraineurs were more nauseated and had longer-lasting headache and photophobia than controls (60). In an individual patient, it may be difficult to differentiate between episodic motion sickness and attacks of MV induced by motion stimuli. This should be decided by taking into account the type and duration of symptoms. Nausea and dizziness improving after cessation of the motion stimulus point to a diagnosis of motion sickness, while rotational or positional vertigo persisting after the motion stimulus has disappeared, suggest MV.
Migraine and cerebellar symptoms
Cerebellar dysfunction causes imbalance which patients may experience as dizziness. Some families with familial hemiplegic migraine (FHM), a rare subtype of migraine, develop progressive cerebellar ataxia and nystagmus (61). Interestingly, mutations in the CACNA1A gene coding for the α1A subunit of a neuronal Ca2+ channel, which is heavily expressed in the cerebellum, have been identified not only in FHM but also in episodic ataxia type 2 (EA-2) and spinocerebellar ataxia type 6. EA-2 is characterized by short bouts of cerebellar ataxia, often with vertigo, and interictal nystagmus. Approximately half of the patients with EA-2 have migraine (62). Both FHM and EA-2 are associated with typical symptoms of basilar migraine (62, 63).
In more common types of migraine, cerebellar symptoms are not usually present, but subclinical hypermetria and other subtle subclinical cerebellar signs in patients with migraine with or without aura have been reported recently (64). The authors suggested dysfunctional Ca2+ channels as a possible cause. This hypothesis relies on findings of an involvement of the CACNA1A gene region in some families with non-hemiplegic migraine with and without aura (65). Another possible link between migraine and cerebellar dysfunction is the mild oculomotor deficits of cerebellar origin observed in patients with migrainous vertigo (21).
Migraine and non-vestibular dizziness
Migraine patients report not only more vertigo but also significantly more dizzy spells than controls (32%vs 13%) (9). These can usually be attributed to non-vestibular causes. However, mild vestibular dysfunction may also present with dizziness rather than vertigo.
Migraine, orthostatic hypotension and syncope
Among 500 unselected migraineurs, syncope during migraine attacks has been reported in 5% (66). Orthostatic symptoms have been found to be more frequent in students with frequent headaches than in controls with rare or no headaches (67) and also more common in patients with migraine than in controls (68%vs 8%) (68). Orthostatic hypotension can be induced by small doses of dopamine agonists such as bromocriptine and piribedil and counteracted by dopamine antagonist domperidone in migraineurs, but not in controls, suggesting hypersensitivity to dopaminergic stimulation as the underlying mechanism (69, 70).
Migraine and dizziness due to a comorbid psychiatric disorder
The interrelations of migraine, dizziness and certain psychiatric disorders are intricate. There are bi-directional associations of migraine with both major depression and panic disorder, with migraine being a risk factor for first-onset major depression and panic disorder and vice versa (71, 72). Dizziness is the second most common symptom of panic attacks after palpitations (73) and can be a symptom of major depression as well. To complicate things further, patients with panic and anxiety have an incresed rate of vestibular test abnormalities (74), which may reflect an elevated risk of patients with vestibular disorders to develop an anxiety disorder (75). Likewise, anxiety or panic disorder was reported by 14 out of 100 patients with migrainous vertigo (19).
Dizziness due to anti-migraine medication
Dizziness is listed as a side-effect of many medications, some of which are used in the treatment of migraine. Therefore, it is useful to elicit a detailed drug history and ascertain the onset of dizziness in relation to changes in medication. Beta-blockers and calcium-channel blockers, like most anti-hypertensive agents, can cause orthostatic hypotension, particularly at the beginning of treatment. Long-term treatment with beta-blockers can also cause lightheadedness and fatigue. Antidepressants, particularly tricyclic antidepressants, which are used in the prophylactic therapy of migraine, can cause sleepiness, blurred vision, lightheadedness and postural hypotension.
Conclusions
The associations of vertigo and dizziness with migraine are complex and can be subdivided into causal, statistical and coincidental relationships. There is emerging clinical evidence that recurrent vertigo is often causally related to migraine and that MV can be diagnosed by operational diagnostic criteria. The syndrome of MV deserves further research activity as it is common and clinically relevant. In addition, it may help to clarify the pathomechanisms of migraine itself. However, the current IHS classification of migraine does not reflect vertigo as a symptom of migraine and may thus hinder the recognition of MV. We would therefore advocate the inclusion of MV in a future revision of the IHS classification of migraine.