
Abstract
We surveyed 1436 women aged 40–54 years in the community. Of these, 278 (19.4%) were diagnosed with migraine or probable migraine based on the International Classification of Headache Disorder criteria. The diagnoses of migrainous vertigo (MV) were modified from Neuhauser’s criteria. Of the 278 women, 238 (85.6%) underwent an interview and 72 (30.3%) of those with migraine or probable migraine had MV. The 1-year prevalence of MV among mid-life women was 5.0% (95% CI, 4.0–6.3%). The MV subjects had a higher proportion of aura (23.6% vs 9.6%; OR, 2.9), nausea (76.4% vs 55.8%; OR, 2.6) and photophobia (61.1% vs 41.7%; OR, 2.2) compared with the migraine subjects without MV. The migrainous subjects with and without MV had similar Short-Form 36 (SF-36) scores. Our study showed that MV was common in mid-life women. Their health-related quality of life was similar in migrainous subjects with MV and those without MV.
Introduction
Migraine is a common clinical syndrome that is characterised by episodic headaches with associated numerous other neurological symptoms, which include dizziness and vertigo (1). This association was first described as early as the 19th century (2). However, studies of the interrelationships between migraine and vertigo have been hindered by several factors (3). First, both vertigo and migraine may co-exist in the same individual by chance alone. Second, there are some variations in the clinical manifestations of migrainous vertigo (MV). Furthermore, patients with MV may have symptoms that overlap with other clinical entities, such as Meniere’s disease and benign paroxysmal positional vertigo (BPPV).
The prevalence of MV was high both in the dizziness clinic and in the migraine clinic, which a previous study reported as approximately 7% and 9%, respectively (4). In another study, migraine headache and vestibular vertigo concur in the general population at a rate that is approximately three times higher than would be expected by chance alone (5). A further study found a higher prevalence of vertigo in patients with migraine than in those with tension-type headaches (6). Increasingly, MV is becoming recognised as a frequent cause of vertigo.
The term, MV, was coined by Neuhauser et al., (4) who proposed operational diagnostic criteria. Although MV is not included in the International Classification of Headache Disorders, 2nd edition (ICHD-2) as a distinct entity, diagnostic criteria have recently been developed and modified to facilitate the identification of patients for whom vertigo is likely to be a symptom of migraine (7,8).
Previous studies have suggested a link between female sex hormones and migraine, which include the alterations in steroid hormone production that occur in women during the menopausal transition (9–11). Large-scale surveys have shown that the prevalence of migraine declines after menopause (12). Our previous study also supported the clinical impression that the prevalence of migraine increases before menopause and declines after spontaneous menopause (13). However, the inter-relationship between MV and the menopausal transition has not been investigated to date.
Therefore, in the current study, we sought to estimate the prevalence of MV in mid-life women during the menopausal transition in a community-based survey. Furthermore, we aimed to investigate the clinical characteristics of MV, the associated sociodemographic characteristics of affected individuals, and their health-related quality of life (HRQoL).
Methods
Subjects
The present neurotological survey is a cross-sectional study of the Kinmen Women-Health Investigation (KIWI) cohort study. The KIWI cohort is a community-based longitudinal study aimed at investigating changes in cognition, mental health and migraine in women during the menopausal transition (14). Detailed study design and methodology of KIWI have been published elsewhere (14). In brief, we put an advertisement regarding the study in a local newspaper. About 1 week after announcement, all eligible women were contacted by mail to maximise enrolment. The participants were encouraged to go to local health office for evaluation by study neurologists. The Institutional Review Board of Taipei Veterans General Hospital approved the protocol of this study.
Kinmen is an island located to the west of Taiwan. Most people living in Kinmen are Han Chinese and engage in farming activities or small businesses. The standard of living and life-style are comparable to those in a rural community of Taiwan. There are four townships in Kinmen, which all have a similar demographic composition. Based on logistic convenience, we chose Kin-Hu and Kin-Cheng, two of the four townships, for this study. According to the registration records and our household census, there were 1622 women aged 40–54 years who reside in the two target townships (15). Of these eligible women, 1436 participated in the survey and 278 of these (19.4%) were diagnosed with migraine or probable migraine by neurologists based on the ICHD-2 classification criteria (16).
Evaluation
Demographic data were collected with regards to the medical history, family history, menstrual and reproductive history, information on personal habits, headache characteristics and associated symptoms, and history of dizziness and vertigo from all participants through self-administered questionnaire in the presence of well-trained interviewers. They also completed the Hospital Anxiety and Depression Scale (HADS) (17,18) and the Medical Outcome Study (MOS) 36-Item Short-Form Health Survey (SF-36) (19–21).
Diagnostic criteria of migrainous vertigo (MV)
The subjects who were diagnosed as migraine or probable migraine sufferers were invited to receive semi-structured interviews for MV by board-certified neurologists who were experienced in the study of headache and neurotological conditions. The diagnostic criteria of MV were modified from Neuhauser’s criteria (4); the diagnosis was made if:
The patient had experienced at least two attacks of episodic vertigo (spinning or rotational sensation) of at least moderate severity that interfered with the activities of daily living and were accompanied by migraine headache, photophobia, phonophobia or a migraine aura, such as scotoma or fortification spectrum visual phenomenon, sensory and speech symptoms. There was a current or previous history of migraine headaches. Other causes of vertigo, such as benign paroxysmal positional vertigo (BPPV) and Meniere’s disease, were excluded by appropriate investigations. Some points are used to differentiate MV from BPPV or Meniere’s disease. Compared with BPPV, migrainous positional vertigo is of shorter disease course, frequently recurrent, manifested early in life and accompanied with migrainous symptoms (22,23). In addition, hearing loss and tinnitus are often not prominent in MV patients. Hearing loss is usually mild and transient, without progression in the course of the disorder in MV in contrast to Meniere’s disease (23). The neurologists excluded the possibilities of BPPV or Meniere’s disease during the interview.
The four episodic vestibular symptoms, which include rotational vertigo, positional vertigo, other illusory self or object motion, and head motion intolerance (the sensation of imbalance or illusory self or object motion provoked by head motion) were queried during the interview. The typical migraine aura consists of visual and/or sensory and/or speech symptoms which fulfilled criteria B and C for one of the subforms of migraine with aura (1.2.1–1.2.6) proposed by the ICHD-2 (16).
We asked the subjects four questions about the relationship between vertigo/dizziness and headache attacks:
Did you experience vertigo during headache attacks? Did you experience vertigo during headache-free period? Did you experience dizziness during headache attacks? Did you experience dizziness during headache-free period?
Menopause-related symptom check-list
This was modified from the Kupperman index on the experience and frequency of symptoms in the previous two weeks (24). Two vasomotor symptoms, hot flushes and night sweating, were included.
Hospital Anxiety and Depression Scale (HADS)
All participants completed the Hospital Anxiety and Depression Scale (HADS) (17,18). The HADS is a self-completed questionnaire that was developed for the specific use in the hospital out-patient setting. Each subscale for anxiety or depression includes seven questions that are rated with a score of 0–3 depending on the severity of the problem described in each question. In this study we used a cut-off point of 7/8 in anxiety and depression scores as clinically significant cases (25).
Medical Outcome Study (MOS) 36-Item Short-Form Health Survey (SF-36)
The SF-36 is a 36-item, self-administered questionnaire. It is a generic instrument for the measurement of HRQoL over the previous 4 weeks. It has eight domains: physical functioning; role limitation due to physical problems; bodily pain; vitality; general health perceptions; social functioning; role limitation due to emotional problems; and mental health.
After summing the Likert-scale items in the SF-36, each scale was then standardised so that it ranged from 0 (the lowest level of functioning) to 100 (the highest level) (20). The translation of the Chinese version of the SF-36 was developed using a standard methodology that was followed by the International Quality of Life Assessment Project (21). Cronbach’s α-coefficient values for the Chinese version of SF-36 were all above the criteria of 0.7 (range, 0.72–0.90), as demonstrated in a previous study (21).
Statistical analysis
SPSS v17.0 for Windows (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The 1-year prevalence of MV is presented as the number of cases per 100 persons with 95% confidence intervals (CIs). We grouped the participants into three categories: those with MV, those with migraine without MV, and those without migraine (non-migraine). The initial descriptive analysis compared the demographic information, headache characteristics, HADS and SF-36 scores between the three groups using an analysis of variance (ANOVA) with the post hoc least significant difference (LSD) test or chi-squared test when appropriate. Odds ratios (ORs) with 95% CIs were calculated. All statistical tests were two-sided. For balancing the type I and type II errors in multiple comparisons, we defined a significant P-value as being less than 0.01.
Results
Demographic characteristics of study population
Among the 1436 women who participated the headache survey, 278 subjects were diagnosed with migraine (n = 237) or with probable migraine (n = 41). Of these subjects, 238 (85.6%) received an interview for MV and 72 (30.3%) of these had MV. Therefore, the 1-year prevalence of MV among mid-life women was 5.0% (95% CI, 4.0–6.3%). Twenty-six of the 720 pre-menopausal women had MV (3.6%; 95% CI, 2.5–5.2%); 26 of the 370 perimenopausal women had MV (7.0%; 95% CI, 4.8–10.1%); 11 of the 203 spontaneous menopause women had MV (5.4%; 95% CI, 3.1–9.4%) and 9 out of the 101 surgical menopausal women had MV (8.9%; 95% CI, 4.8–16.1%; chi-squared test, P = 0.028).
Comparison of demographics, blood pressure, past medical history, menopausal status, menopausal symptoms and hospital anxiety and depression scores (HADS) among the participants

Significant P-values in bold.
a P < 0.01 compared with migraine without MV; b P < 0.01 compared with MV.
MV, migrainous vertigo.
Headache characteristics and vestibular symptoms
Headache characteristics and vestibular symptoms in migrainous subjects with or without migrainous vertigo (MV)
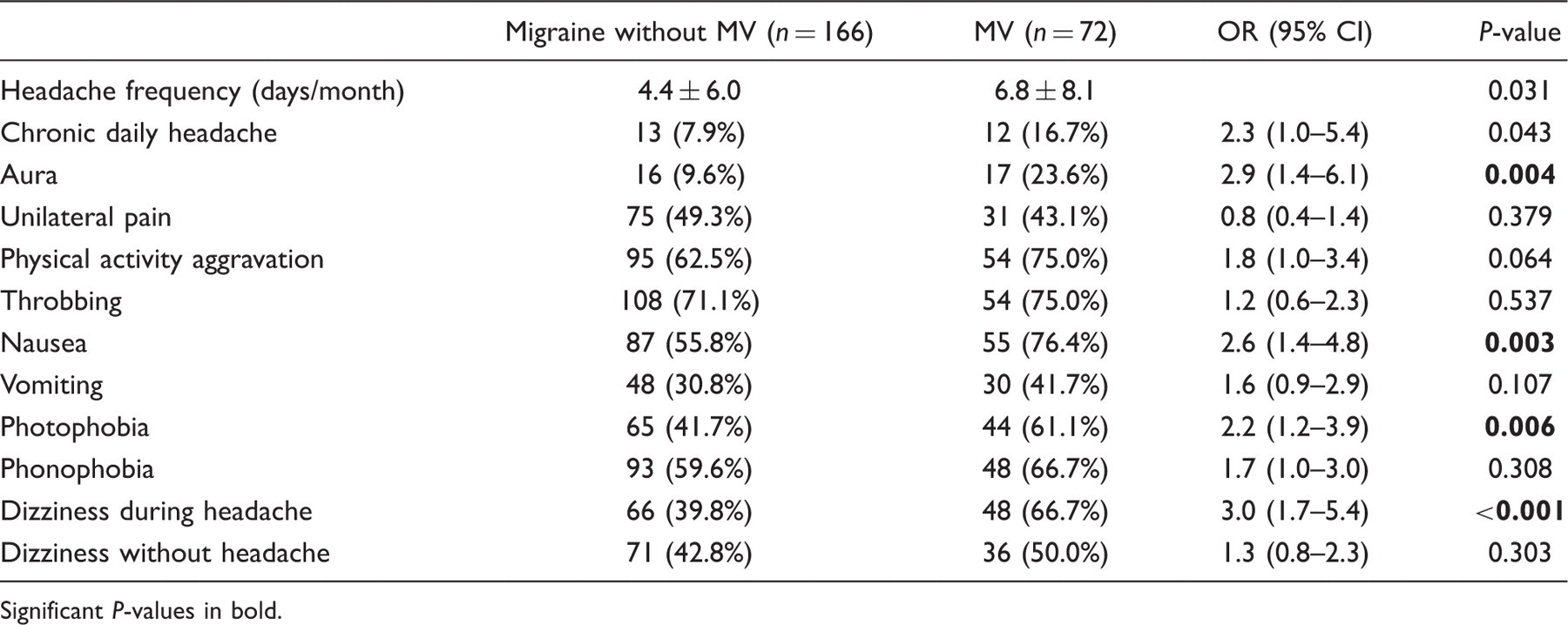
Significant P-values in bold.
As expected, dizziness was associated more frequently with headache attacks in subjects with migraine with MV than in those without MV. Nevertheless, the rate of occurrence of dizziness did not differ outside headache attacks between subjects with migraine with MV and those without MV.
Rotational vertigo was the most common type of vertigo in subjects with MV (n = 64; 88.9%), followed by illusion of motion (n = 9; 12.5%). Only six subjects (8.3%) had positional vertigo and three subjects (4.2%) had intolerance to vestibular head motion. In the MV subjects, 32 (45.7%) had photophobia during vertigo attacks; 38 (52.8%) had phonophobia and one perceived an aura.
Health-related quality of life
Scores obtained on the SF-36 in migrainous subjects without migrainous vertigo (MV) and in subjects with MV

Discussion
This community-based study found a high prevalence of MV in mid-life women. Compared with migraine subjects without MV, MV subjects were more likely to have aura, nausea and photophobia during attacks of headache. The negative impact on the HRQoL of these subjects was similar between migraine subjects with and without MV.
The community-based study found a high 1-year prevalence of MV (5.0%) among mid-life women. A German population-based survey found that the life-time prevalence of MV was 3.2%, and the 12-month prevalence was 0.89% (5). The difference between this and the present study might be explained by the different target populations that were examined; mid-life women during menopausal transition were interviewed in our study in comparison with a more general population that was included in the German study.
Several studies have documented higher proportions of migraine with aura (MA) in MV patients (4,5,26–31). Vertigo may be part of the aura, and 10–30% of patients have vertigo during the typical migraine aura (5,26–28). However, most attacks of vertigo do not fulfil the criteria for migraine aura. In fact, the vertigo experienced in patients with MV does not follow the temporal relationship seen in migraine attacks based on the ICHD-2 aura criteria. Overall, our results were compatible with the results from these reports. However, as we did not measure the duration of vertigo attacks specifically, as well as the temporal relationship with headache, it is unclear whether some of our MV subjects might fulfil the criteria of migraine aura or not.
In the current study, we found no significant association between systolic blood pressure, diastolic blood pressure, BMI, hypertension or diabetes in MV subjects, migraine subjects without MV and non-migraine subjects. A previous report found a significant association of MV with coronary heart disease (5). In addition, low blood pressure or hypotension has been linked to MV patients (31). The discrepancy between our results and these studies needs further investigation. In addition, our study did not show an association between therapies with female sex hormones or menopausal status between subjects with migraine and headache-free controls. However, higher frequencies of vasomotor symptoms (hot flushes or night sweating) were noted in the migrainous subjects, which was in accordance with our previous findings (13). Nevertheless, the menopausal symptoms did not predict the prevalence of migraine during the menopausal transition in the multivariate analysis but the menopausal status and the presence of premenstrual syndrome did (13). Whether these symptoms were related to hormonal changes or not remains to be elucidated.
Patients with migraine, whether with MV or not, had significantly higher scores for both anxiety and the total HADS score than was found in subjects without migraine. This finding is most likely to reflect the common association of migraine with anxiety disorder rather than MV itself. On the contrary, there was no evidence of an association of MV with depression, which was similar to a previous finding (5). Some prior studies have shown an association between vestibular vertigo and depression (32–34). However, these studies did not exclude the confounding effect of migraine.
As expected, MV subjects had more dizziness or vertigo during headache attacks. Nevertheless, there was no difference in the prevalence of dizziness outside headache attacks between subjects with migraine with MV and without MV. A prior study showed migraine patients had more non-vestibular causes of dizziness compared with controls (35). In addition, co-morbid psychiatric disorders, such as depression, panic attacks and anxiety disorders, may contribute, in part, to the frequent episodes of dizziness in patients with migraine (36,37). As stated above, there was a higher anxiety score in our patients with migraine, so it is possible that our migraine subjects either with or without MV had a higher proportion of non-vestibular dizziness outside of the attacks of headache.
A previous study pointed out that MV is not only a frequent disorder but also has a tremendous impact on the personal and social level (5). This study found a substantially lower level of HRQoL in their small sample of MV patients, as compared to a representative general population. However, that study did not evaluate the effect of migraine per se on the HRQoL. In the present study, we demonstrated that MV patients had a similar level of HRQoL when compared to subjects with migraine without MV, as evaluated by the SF-36. Previously, we have documented that migraine patients had significantly lower levels of HRQoL compared to age-matched controls (38). Overall, our study suggested that it is the occurrence of migraine itself that exerts the negative impact on the generic HRQoL in MV subjects. However, because disease-specific HRQoL questionnaire, such as the Dizziness Handicap Inventory (DHI) (39), was not applied in our study, it remains unclear whether MV patients have a lower HRQoL due to vestibular symptoms.
Study limitations
The strengths of the current study included the community-based interview by experienced, board-certified neurologists and the use of explicit diagnostic criteria for MV. Nevertheless, our study does have some limitations. The prevalence of MV may have been underestimated in our study due to recall bias. Subjects might have forgotten mild migrainous symptoms, such as nausea, photo- and phonophobia, or even moderate headache during the vertiginous attacks. Furthermore, our target population included mid-life women exclusively, and so it is premature to extrapolate our conclusions to men or other age groups in the general population.
Footnotes
Acknowledgements
This study was supported, in part, by a grant from the National Science Council (NSC-93-2314-B-075-085) and Taipei Veterans General Hospital (V99C1-047).