
Abstract

Introduction
Cerebral palsy (CP) is an acquired, static neuromuscular disorder involving muscle spasticity, muscle tone, and/or postural abnormalities. Foot and ankle deformities in patients with CP are common. Problems can arise because of dynamic overactivity and muscle imbalances, often leading to issues with ambulation, orthotic, and shoe wear. 14 Current treatment methods involve both operative and nonoperative interventions depending on the extent of deformity and the circumstances of the case. These treatments are designed to improve range of motion, foot and ankle mechanics, gait, and quality of life. Although there are many studies in the literature evaluating foot and ankle deformities in CP patients, it is important to consolidate all of these studies to determine a suitable approach to diagnosing and managing foot and ankle deformities in pediatric CP patients. The purpose of this review is to cover normal gait mechanics and contrast these with pathologic changes seen in patients with CP. Additionally, the aim of this review is to also present a current model for clinical decision making regarding the management of foot and ankle pathology for patients with CP by evaluating the presentation and treatment options for these patients. This review will add to the current literature by providing additional information on how to appropriately use a pediatric CP patient’s clinical history, physical examination, radiographs, as well as other factors, to guide management strategies, which can include the various nonoperative or operative modalities also discussed in this review. Clinicians can use this review to determine the best course of action for their patients, with the overall goal to improve patient outcomes and quality of life.
Background
Normal gait is characterized by proper interaction between the ankle, foot, and the floor. From a biomechanical standpoint, ankle plantar flexion is usually associated with knee extension, as excessive plantar flexion forces the knee into recurvatum, whereas ankle dorsiflexion is associated with knee flexion and crouch gait. This relationship is known as the plantar flexion/knee extension couple and is thought of as the basis of normal gait. 14
In order to best understand foot and ankle function in normal gait, the lower extremities distal to the knees can be broken into 4 segments: the tibial (shank) segment, the hindfoot (talus, calcaneus), the midfoot (navicular, cuneiforms, cuboid), and the forefoot (metatarsals, phalanges).13,18 Similarly, the foot can be broken into 2 segments: lateral (calcaneus, cuboid, lesser toe metatarsals, phalanges) and medial (talus, navicular, cuneiforms, great toe metatarsal, and phalanges).13,18
In a normal gait cycle, function of the ankle and foot can be characterized using the concept of 3 ankle rockers (Figure 1).14,18,29 The function of the first rocker is to provide shock absorption during the loading response. The second rocker provides stability during the midstance, and the forefoot functions as a rigid lever during the terminal stance to prepare for toe-off (third rocker).
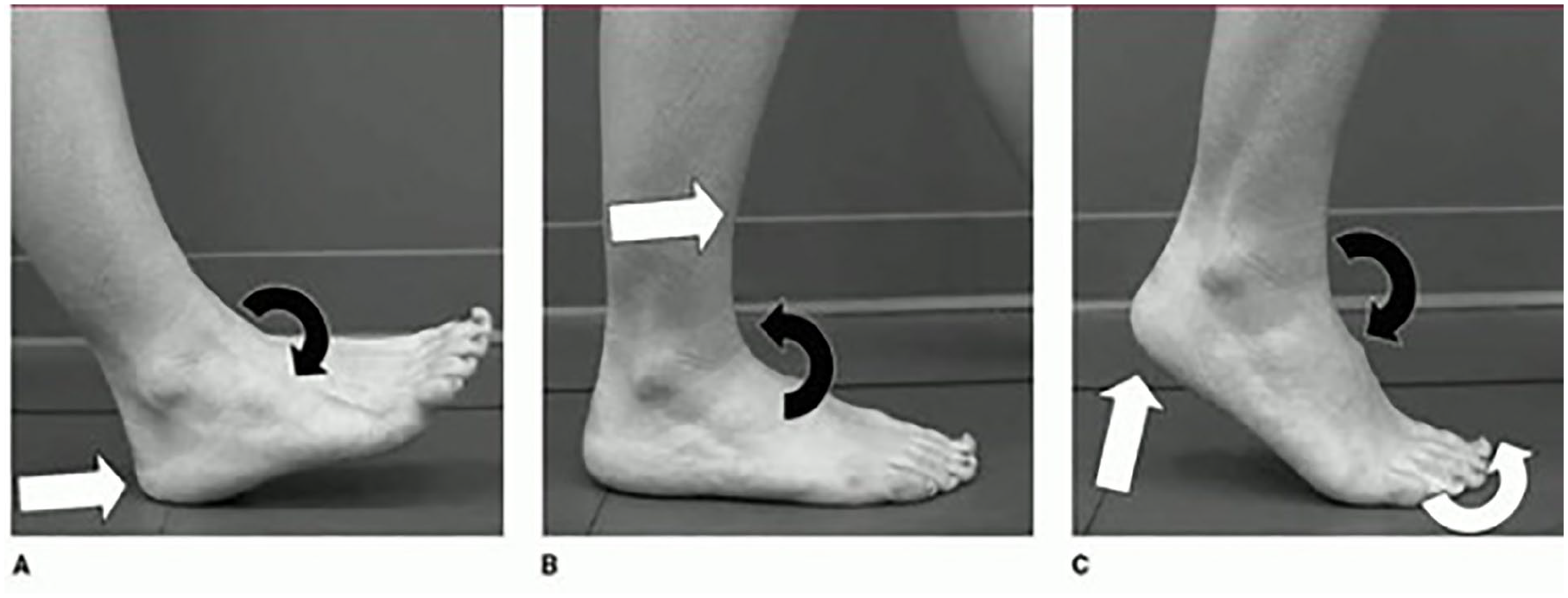
The 3 ankle rockers of normal gait. 2 (A) The first rocker occurs when the heel strikes the floor (white arrow) and is closely followed by tibiotalar plantarflexion (black arrow). (B) The second ankle rocker involves tibial advancement forward over the foot (white arrow) while the tibiotalar joint transitions from dorsiflexion to plantarflexion (black arrow). (C) The third rocker is characterized by a heel rise and forefoot dorsiflexion (white arrows) with concomitant ankle plantarflexion (black arrow). Reproduced with permission from Davids et al. 18
In the swing phase of the normal gait cycle, the foot and ankle are involved in the clearance and prepositioning for the subsequent stance phase.13,18 During the initial swing, the tibia (shank) segment is externally rotating, and the ankle is plantarflexing. During midswing, the tibia (shank) segment rotates internally, and the ankle dorsiflexes. The hindfoot goes into valgus (eversion) unlocking the proximal segment. 26 The terminal swing is characterized by further extension of the midswing movements followed by prepositioning of the foot and ankle to repeat the gait cycle. It is important to note that the tibial rotation during swing is a minor change compared with the complex rotation of the ankle.
Three common ankle/foot segmental misalignment patterns occur in patients with CP: equinus, equinoplanovalgus, and equinocavovarus.14,27,36,39 These abnormalities often arise from a combination of muscle spasticity, disrupted motor control, overactive plantar flexor muscles, and/or ineffective dorsiflexor muscles. 18 Additional muscle imbalances may be present between the extrinsic muscles such as the posterior tibialis (PT), toe extensors and flexors, and the peroneus brevis and longus.
Equinus is common in children with CP and usually occurs in the setting of a spastic gastrocnemius but can also result from a tight gastrocsoleus complex. The spasticity of these muscle groups causes plantar flexion of the hindfoot by pulling the calcaneal tuberosity proximally. This subsequently limits dorsiflexion at the tibiotalar joint (Figure 2). Equinoplanovalgus is characterized by pronation deformities of the midfoot caused by imbalance between the PT and peroneus brevis (Figure 3). The lateral column of the foot is functionally and structurally shorter than the medial column resulting in an eversion of the foot and ankle. In this deformity pattern, there is often excessive plantar flexion of the hindfoot (equinus), and deformities such as hallux valgus may be present.14,19 Equinocavovarus is characterized by equinus deformity of the hindfoot coupled with supination deformities of the midfoot and forefoot (Figure 4). The lateral column of the foot is functionally and structurally longer than the medial column resulting in malalignment of the hindfoot, midfoot, and forefoot. More complex segmental malalignments may occur but are much less common.14,18,27,36,39


Plain radiographs of the foot in a child with equinoplanovalgus deformity. 8 (A) There is forefoot abduction, hindfoot pronation, and talonavicular uncoverage shown in the anteroposterior view. (B) Lateral view shows forefoot and midfoot pronation and hindfoot plantar flexion. Reproduced with permission from Davids et al. 19

Alterations in gait are common in all 3 deformities leading to altered function. Equinus is characterized by a spastic gastrocnemius or gastrocsoleus complex resulting in ankle plantar flexion throughout the stance phase. The stability in midstance (second rocker) is compromised because of excessive ankle plantar flexion. 3 To compensate for this, patients may flex their hips to a greater degree than normal. Observers may notice an exaggerated hip flexion in these patients. 34 In equinoplanovalgus segmental malalignment, the midtarsal joint is often significantly dorsiflexed, everted, and abducted throughout gait, and the tarso-metatarsal joint is plantarflexed and slightly adducted. 8 This results in no significant abduction of the forefoot compared to the hindfoot. The range of motion of the midtarsal joint is reduced because of the midtarsal joint having reached the largest possible dorsiflexion allowed by the constraints of skeletal and ligament structure. 8 Equinocavovarus affects foot stability and position in the stance phase, and the lever arm (third rocker) is minimally functional. 30 Additionally, the ability to generate tension is adversely affected because of the shortened length of the plantar flexor muscles.3,14 To compensate for the foot deformities, patients may have excessive pelvic rotation to aid in limb advancements. Other compensatory mechanisms found in these patients include knee hyperextension, increased pelvic lordosis, as well as others. 34 It is important for clinicians to not only focus on the foot and ankle deformity in these patients, but to also observe how these patients compensate for their deformity by performing a thorough gait analysis examining the whole body. Further, calluses may be present that may have arisen from abnormal weightbearing patterns, and there may be pain with weightbearing.
Presentation
Clinical decision making for the management of foot and ankle problems in patients with CP can be challenging. Therefore, it is advised to use a multifactorial approach involving clinical history, physical examination, radiographic evaluation, and gait analysis. Once these aspects are accounted for, the deformity can be assessed, and a treatment plan can be made.
Clinical History
When treating children with CP, the patient’s clinical history is the most important guide in treatment. Ascertaining the patient’s ambulatory capacity, need for ambulatory assists, operative history, and functional independence frames the visit and allows the clinician to adequately evaluate and address the parent’s concerns.
Asking parents and patients how they describe their ability to walk gives the clinician insight into the patient’s comfort and tolerance for walking. Inquiring about stamina allows one a gross idea of how efficiently the patient ambulates. Parents may comment about tripping, or hearing the foot slap, or that the patient’s feet turn in, all of which begins to frame the clinical picture. As with any patient, if ambulatory tolerance is limited by pain, this should be explored. Gathering the classic descriptors of pain such as duration, location, radiation, and actions that either worsen or alleviate pain, can further inform the clinician as to areas of pathology in the foot and ankle.
For those patients who present having seen other providers, they may have ambulatory assist devices ranging from ankle-foot orthoses (AFOs) to walkers. It is important to understand how they rely on these devices. It is important to ask how often they use them and what happens to their gait if they do not use them. How long have they used them is useful information, especially for braces, because braces may be old and worn out, or simply ill fitting.
Gathering a good operative history is of the utmost importance as making decisions regarding tendon transfers and lengthening hinge on those structures being untouched. It is also useful to know which surgeries may have improved the patient and which may not have. It is further important to determine how independent the patient is at baseline. The needs of a community ambulator are very different from a child who relies on caregivers for help with activities of daily living. This frames the goals of treatment and ties together the rest of the history.
Standardized functional outcome measures are also important to assess in this patient population. There are currently several patient-reported outcomes (PROs) that are used for CP patients, including the Caregiver Priorities and Child Health Index of Life with Disabilities (CPCHILD), Functional Mobility Scale, and the Patient-Reported Outcomes Measurement Information System (PROMIS).9,22,28 Administering these tools in clinical practice can help a clinician understand a patient’s satisfaction and monitor their outcomes longitudinally.
Physical Examination
The physical examination should begin with a visual inspection of the patient standing with a focus on the alignment of the patient’s spine, hips, and lower extremities. Care should be taken to observe the hindfoot with the patient away from the clinician and note varus or valgus alignment. Any malalignments should be measured in degrees away from midline. For patients who require a walker or similar device, a visual inspection of the patient standing may proceed with caution. If the patient is unable to stand, then an assessment of the spine, hips, and lower extremities may be completed individually.
Next, the patient should lay supine. A measurement of each of the patient’s lower extremities from the superior aspect of the iliac crest to the distal aspect of the fibula should be recorded in order to determine if there is any leg-length discrepancy. Next, the plantar aspect of the feet should be examined for calluses that may have arisen from limited range of motion or from abnormal walking/weightbearing patterns. Additionally, a manual examination consisting of active and passive range of motion of the patient’s lower extremities, including the hip, knee, ankle, and subtalar joints should be performed. Specifically, for the ankle, the Silfverskiold test should be used to differentiate gastrocnemius vs soleus contracture. Selective motor control and flexibility should also be analyzed and noted. Additionally, spasticity measures should be performed in these patients, possibly using the Tardieu Scale or the Ashworth Scale. 2 Measuring torsional alignment may be further considered. Chen described using the transmalleolar axis or the thigh-foot angle, as well as imaging options, such as ultrasonography, magnetic resonance imaging (MRI), or computed tomography (CT). 10 Furthermore, muscle strength testing, such as maximum voluntary isometric contractions of ankle dorsiflexion, is a very important component of the physical examination.
Once the manual examination has been completed, an observational gait analysis should be performed. The patient should be barefoot and wearing shorts so the knee and lower thigh can be better visualized. The patient should walk approximately 20 feet away and toward the observer with observation occurring from multiple viewpoints including the coronal and sagittal planes. Documented observations should include the foot position at initial contact (ie, toe strike, heel strike, flat foot), foot alignment (varus/valgus in the transverse and sagittal planes), lower extremity alignment (varus/valgus), and foot clearance during the swing phase. Examining limb alignment in the sagittal plane is also important during gait observations to look for crouch.
Radiographic Evaluation
Weightbearing radiographs of the foot and ankle facilitate clinical decision making for the management of foot and ankle deformities in patients with CP. Nonweightbearing images do not aid in the evaluation and should not be used.
There are 3 standardized radiographic views that should always be obtained (AP ankle, AP foot, lateral foot). When interpreting, one must determine the alignment of the foot and ankle. This can be accomplished by dividing the foot into 3 segments (hindfoot, midfoot, forefoot), and 2 columns (lateral, medial).
A comprehensive technique of radiographic segmental analysis of the foot and ankle has been developed by Davids et al. 15 Ten radiographic measurements from a cohort of 60 normal feet in children aged 5-17 years were used to determine the alignment of the various segments of the foot and ankle (Table 1). 15 This analysis technique can facilitate proper course of action and treatment. For instance, pes equinoplanovalgus in children with CP would be characterized by hindfoot equinus and valgus, midfoot pronation, forefoot pronation, and a short lateral column based on these radiographic measurements. 15 This would allow surgeons to predict that operatively correcting the hindfoot and midfoot deformities will unmask a forefoot supination deformity. 15 Therefore, using these 10 radiographic measurements can be used to describe malalignment patterns and assist in clinical decision making.
Mean Values, SDs, and Ranges for the 10 Radiographic Parameters. 12

Abbreviation: AP, Anteroposterior.
Source: Reproduced with permission from Davids et al. 15
Levels of Deformity
There are 3 levels of foot and ankle deformities in patients with CP and are often progressive with growth and development.14,19 Level 1 is classified as a dynamic soft tissue imbalance without skeletal malalignment or abnormality. Level 2 deformities involve fixed or myostatic soft tissue imbalances with associated skeletal segmental malalignments or abnormalities. Level 3 deformities are characterized with the same soft tissue imbalances as seen in level 2, but also involve structural skeletal deformities. Recognizing and understanding the level of deformity will guide the clinical decision-making process and guide the course of treatment.
Treatment
The principal goals of treatment are to optimize the segmental alignment of the foot and ankle, to maximize shock absorption function during loading response phase, and to restore the rigid lever arm available to the ankle plantar flexor muscles in the midstance and terminal stance phases of the gait cycle. 15 Improved segmental alignment also facilitates the application of foot and ankle orthotics, which can benefit function in both the stance and swing phases of the gait cycle. 17 Management of foot and ankle deformities in children with CP may include nonoperative and operative modalities.
Nonoperative Modalities
In mild cases of CP, nonoperative modalities provide an opportunity to improve gait and prevent the worsening of musculoskeletal deformities. Serial casting has long been considered a viable option. AFOs are also commonly used in patients with mild CP for a variety of pathologies (Table 2). In order to assess and provide proper care, the orthosis design, material of construction, and cost must be considered.
Properties and Performance Characteristics of Ankle Foot Orthoses. 2
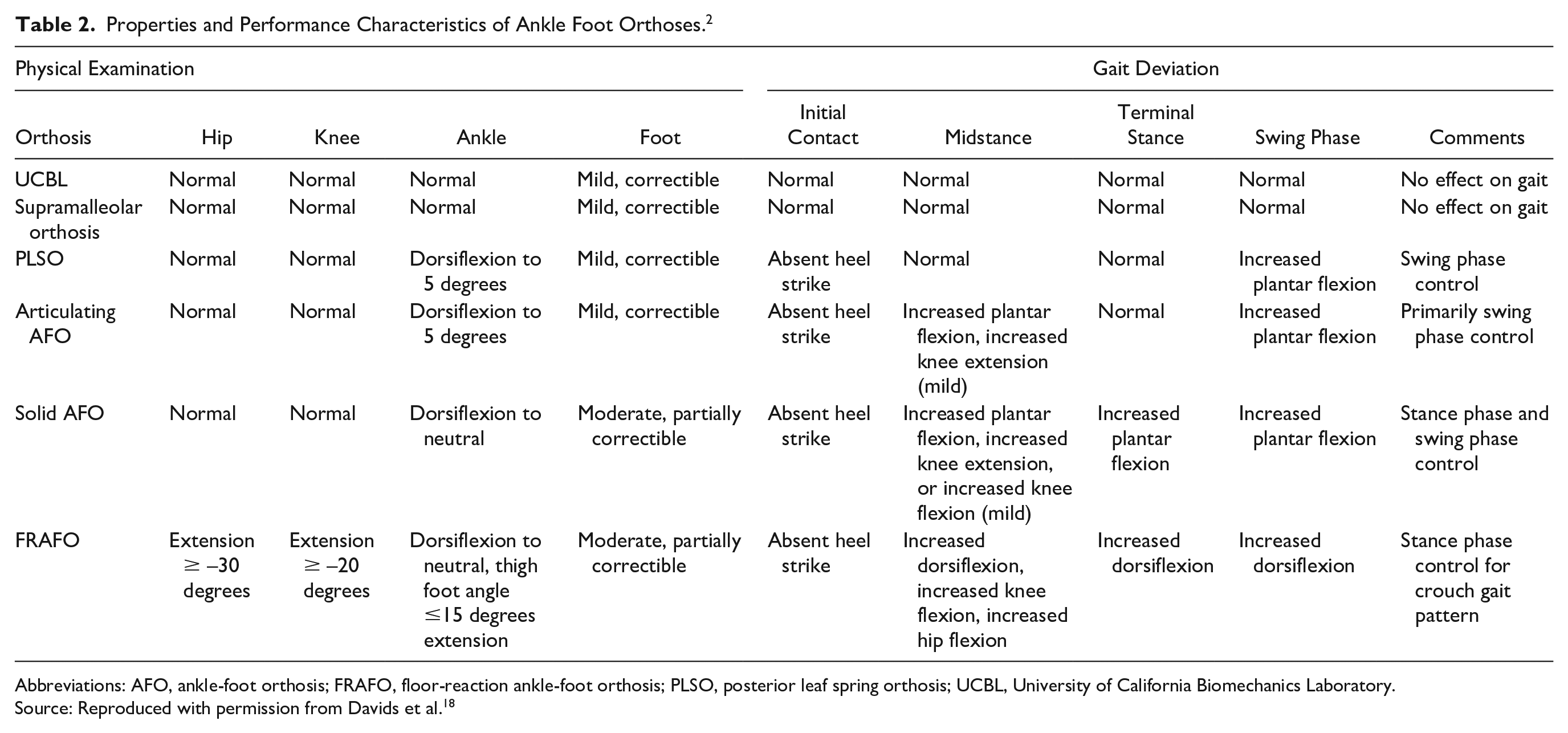
Abbreviations: AFO, ankle-foot orthosis; FRAFO, floor-reaction ankle-foot orthosis; PLSO, posterior leaf spring orthosis; UCBL, University of California Biomechanics Laboratory.
Source: Reproduced with permission from Davids et al. 18
There are 6 common orthotic designs: foot orthosis, supramalleolar orthosis, posterior leaf spring orthosis, articulating ankle-foot orthosis, floor-reaction ankle-foot orthosis, and solid ankle-foot orthosis. 18 A thorough physical examination will facilitate selection of the optimal ankle-foot orthosis. Table 2 provides context on which AFO to select based on various parameters including foot and ankle segmental alignment as well as gait deviation. 18
Selecting the optimal AFO requires an understanding of the biomechanics of a normal gait as well as the functional deficits to be addressed by the orthosis. Specifically, the capabilities and limitations of each orthosis should be considered. AFO use in growing children often require new orthoses every 12-18 months. 18
In addition to bracing, dynamic soft tissue imbalances may be treated pharmacologically. Botulinum toxin is a neurotoxin that prevents acetylcholine release at the neuromuscular junction causing flaccid paralysis of the targeted muscle. The primary focus of this approach is to improve muscle tone and spasticity. Multiple RCTs have shown an injection of botulinum toxin A (12 U/kg) into the gastrocnemius muscles in patients with spastic diplegia and hemiplegia yielded significant decreases in viscoelastic aspects of spasticity and increases in dorsiflexion range as early as 8 weeks postinjection.6,7,24,31 Further, Dursun et al 20 demonstrated that combining intermittent serial casting with botulinum toxin injections may provide additional benefits for CP patients. It is important to be aware of the indications of botulinum toxin for pediatric CP patients. Younger children are of lower weight and thus require a limitation of the doses and the choice of muscles to be treated. Also, its use requires specific training and the support of a multidisciplinary team. 23
Administration of intrathecal baclofen and selective dorsal rhizotomy are neurosurgical approaches for the treatment of dynamic soft tissue imbalances in mild cases of CP. Baclofen acts on the central nervous system as a γ-aminobutyric acid B (GABAB) agonist and is used to treat muscle spasticity. 32 Multiple randomized controlled trials (RCTs) have shown that administration of intrathecal baclofen in spastic diplegia patients decreased muscle spasticity in the lower extremities after a single injection.1,21,25 The use of baclofen is limited because of its side effect profile, including sedation, muscle weakness, fatigue, dizziness, and ataxia. 11 Baclofen should also be used with caution in patients with seizure disorders as it can provoke seizures in these patients. Baclofen must also be weaned gradually to avoid a withdrawal syndrome. 11 Selective dorsal rhizotomy is a surgery involving the sectioning of lumbar and sacral nerve roots with the goal of reducing excessive alpha motor neuron activity and spasticity in patients with CP.35,40,42 Early detection and administration of the aforementioned options will improve outcomes and reduce the chances of requiring orthopedic surgery.
Operative Treatment Goals
When nonoperative modalities are not indicated or have been exhausted, operative intervention may be warranted. The goal of operative treatment is to correct bony deformities of the foot and ankle in order to improve the biomechanics of the lower extremity. By doing so, the surgeon aims to make gait more efficient and less painful.
The operative techniques are designed to improve foot shape and reduce pain. Specifically, the aim is to improve stability and function of the foot during the swing phase and improve loadbearing and accepting capabilities. From a pain standpoint, it is important to note that foot and ankle deformities in children with CP are better tolerated than in adults. As these patients age and increase in body weight, there is a greater magnitude of abnormal loading, which results in premature degenerative changes of the joints.14,19 Thus, it is presumed that operative treatment of foot and ankle deformities in children with CP will improve loading patterns and thereby reduce long-term degenerative arthritis in early adulthood.
Operative Techniques
As previously stated, there are 3 common ankle/foot segmental misalignment patterns as seen in patients with CP (equinus, equinoplanovalgus, and equinocavovarus). The operative treatment techniques for each of these misalignment patterns based on the level of deformity are discussed below.
Equinus
Patients with spastic equinus deformities often have overactive plantar flexor muscles causing a shift of the loadbearing point from the hindfoot to the forefoot. Although level 1 deformities primarily involve overactivity of these muscles, level 2 deformities involve muscle tightness and/or structural skeletal deformities. Operative intervention begins with level 2 deformities.
The goal of operative treatment in patients with equinus deformities is to achieve greater dorsiflexion when the knee is extended. This can be accomplished via lengthening of the gastrocnemius and/or soleus muscles. 39 In order to determine which muscle(s) require lengthening, assessment of ankle dorsiflexion range of motion using the Silfverskiold test, which assesses ankle motion with the knee flexed and extended, will guide the choice. Limited ankle range of motion with the knee extended that improves with knee flexion suggests gastrocnemius muscle involvement (+ Silfverskiold test). Limited range of motion with both a flexed and extended knee suggests gastrocnemius and soleus muscle involvement.14,19
Fractional lengthening of the gastrocnemius alone typically allows 5 degrees of improved dorsiflexion when the knee is extended.14,19 This procedure is best performed proximally at the level of the muscle belly. When both muscles, the gastrocnemius and soleus, are involved and 15 degrees or less of correction is required, selective fractional lengthening at the midcalf is considered best practice.14,19 When both muscles are involved but greater than 15 degrees of correction is required, nonselective lengthening distally at the tendo-Achilles level is necessary.14,19 It is important to note that muscle weakness postoperatively can occur.
Equinoplanovalgus
Patients with spastic equinoplanovalgus often have overactive plantar flexor muscles (similar to equinus) as well as overactive evertor muscles. Level 1 deformities involve dynamic or myostatic overactivity of these muscles, whereas level 2 deformities are characterized by muscle tightness. Level 3 deformities involve skeletal misalignments, which result in an eversion of the foot and ankle. Deformities such as hallux valgus may be present (discussed later). Operative intervention begins with level 2 deformities.
For patients with a level 2 equinoplanovalgus deformity, operative treatment of the overactive plantar flexor muscles is treated as described above in patients with equinus deformities. Additionally, a transfer of the peroneus brevis muscle to the peroneus longus muscle will address evertor muscle tightness. At the time of surgery, it is vital to determine that normal segmental alignment has been restored.14,19
Level 3 equinoplanovalgus deformities require soft tissue and skeletal segmental realignment. Soft tissue imbalances are managed as described above. Skeletal segmental realignment is addressed via lateral column lengthening at the calcaneocuboid (CC) joint, neck of the calcaneus, or body of the cuboid.14,19 The procedure involves lengthening of the lateral segments of the foot approximately 1 to 2.5 cm via placement of a tricortical iliac crest allograft. Over time, because of ligamentotaxis, there is progressive stretching of the lateral soft tissue.14,19 If the graft size is greater than 1.5 cm, internal fixation should be used in order to minimize graft collapse during healing and to promote mobilization.14,19 Lateral column lengthening through the neck of the calcaneus may provide a more durable correction than calcaneocuboid joint fusion. 12 However, there is a limit under which this operation can be safely performed: <35 degrees of talocalcaneal angle, <25 degrees of talo–first metatarsal angle, and >5 degrees of calcaneal pitch on weightbearing radiographs. 43 Subtalar motion is often preserved, and patients often see a resolution of the issues related to the deformity while avoiding the need for an arthrodesis and the complications associated with it. 27
After lateral column lengthening is performed in a level 3 equinoplanovalgus deformity, proper alignment of the medial column should be assessed. If the medial column is hypermobile in the sagittal plane, or if there is a residual varus deformity of the forefoot, then a plantar flexion osteotomy is made in base of the great toe metatarsal or the medial cuneiform.14,19 If there is an incomplete correction resulting in a forefoot abduction deformity, then a talonavicular arthrodesis should be performed.14,44 If the lateral column lengthening fails to correct the equinoplanovalgus deformity, then an arthrodesis of the talonavicular, CC, and subtalar joints should be performed to achieve optimal alignment.14,44 Even in significant equinoplanovalgus deformities with cerebral palsy, this is not often required.
Equinocavovarus
Patients with spastic equinocavovarus often have overactive plantar flexor muscles (similar to equinus) as well as overactive invertor muscles leading to adduction of the forefoot. Level 1 deformities involve dynamic or myostatic overactivity of these muscles, whereas level 2 deformities are characterized by muscle tightness. Level 3 deformities involve skeletal misalignments, which result in an inversion of the foot and ankle. Operative intervention begins with level 2 deformities.
For patients with a level 2 varus deformity, operative treatment of the overactive plantar flexor muscles is treated via split transfer of the tibialis anterior or tibialis posterior muscles depending on contributions of these muscles during the stance and swing phases of the gait.14,37 Physical examination findings and dynamic electromyography are used to determine the relative contributions of these muscles.14,19,33 In patients that have plantar flexion muscle power greater than their dorsiflexion counterpart, split anterior tibial tendon transfer and fractional lengthening of the posterior tibial tendon is recommended over split posterior tibial tendon transfer. 4 Additionally, fractional lengthening of the ankle plantar flexor muscle group, tibialis posterior muscle, abductor hallucis, plantar fascia and short intrinsic muscle of the foot, flexor hallucis, and digitorum longus muscles may be required for correction of soft tissue contractures (Figure 5).14,19 As stated previously, it is vital to determine that normal segmental alignment has been restored via intraoperative stress radiographs.14,19 Failure to restore proper segmental alignment could result in a level 3 varus deformity.

Correction of level 2 equinocavovarus deformity. 8 (A) Markings designate 3 incision points to lengthen the appropriate soft tissue structures. (B) A plantar incision is made releasing the plantar fascia and intrinsic muscles of the foot. (C) A distal medial incision is made, and fractional lengthening of the abductor hallucis muscle is performed. (D) A medial calf incision is made, and fractional lengthening of the gastrocsoleus muscle group is performed. (E) Fractional lengthening of the tibialis posterior muscle is performed through the medial calf incision. Reproduced with permission from Davids et al. 19
Level 3 varus deformities require soft tissue and skeletal segmental realignment. Soft tissue imbalances are managed as described above. Skeletal realignments in level 3 varus deformities may require a combination of operative procedures. Proper alignment of the foot and ankle can be achieved by performing multiple sequential osteotomies. Hindfoot varus malalignment may be corrected by calcaneal closed wedge or laterally based closing wedge osteotomies.14,19,38 Midfoot supination deformities may be corrected by cuboid closed wedge osteotomy or lateral column shortening through the cuboid.14,19,38 Forefoot pronation may be corrected by dorsiflexion osteotomy of the medial column or first metatarsal dorsal wedge osteotomy; the first metatarsal dorsal wedge is a closing wedge.14,19,38 Forefoot supination deformity may be corrected by plantar flexion osteotomy of the medial column.14,19
Arthrodesis of the foot and ankle is reserved as a last case option for patients with level 3 varus deformities as these procedures will permanently impact a patient’s ability to properly ambulate. In extreme midfoot cavus deformities, a double arthrodesis of the CC and talonavicular joints may be required. 41 Additionally, a triple arthrodesis of the CC, talonavicular, and subtalar joints may be required.14,19,41
Hallux valgus
Hallux valgus deformities may arise in patients with spastic equinoplanovalgus cerebral palsy. Patients with level 1 and 2 hallux valgus deformities often do not require operative intervention. The preferred treatment for level 3 hallux valgus deformities in patients with spastic CP is great toe MTP arthrodesis.5,16 Significant improvement in the hallux valgus, intermetatarsal, and lateral metatarsophalangeal angles were achieved and maintained after MTP arthrodesis.5,16 Additionally, multiple trials show an increase in functional outcome, improved cosmesis, orthotic use, and reduced pain postoperative treatment.5,16 The management of hallux valgus deformity in patients with spastic CP may be performed in conjunction with other segmental realignment surgeries. 5
Summary
Foot and ankle deformities in patients with CP often arise from a combination of muscle spasticity, disrupted motor control, overactive plantar flexor muscles, and/or ineffective dorsiflexor muscles. The 3 most common foot segmental malalignments in children with CP are equinus, equinoplanovalgus, and equinocavovarus. Clinical decision making is guided by clinical history, physical examination, radiographic evaluation, and gait analysis. Nonoperative modalities for level 1 deformities include utilization of ankle-foot orthotics, pharmacologic approaches such as botulin toxin, and neurosurgical approaches such as dorsal rhizotomy. Operative modalities are used in level 2 and 3 deformities and include muscle tendon unit lengthening or transfer, and skeletal osteotomies or arthrodesis. The goal of these treatments is to improve range of motion, muscle activity, foot and ankle function, and quality of life. The main limitation of this review is that it focuses mainly on 3 common foot malalignments in pediatric CP patients and not on other foot deformities. Future studies should evaluate the diagnosis and management of other foot misalignments in pediatric CP patients, such as planovalgus feet. Nevertheless, this review will add to the current literature by providing additional information on how to appropriately assess a pediatric CP patient and the different treatment options for a clinician to consider. Clinicians can use this review to determine the best course of action for their patients, with the ultimate goal of improving the outcomes and satisfaction of pediatric CP patients.
Supplemental Material
sj-pdf-1-fao-10.1177_24730114221091800 – Supplemental material for Topical Review: Approach to Diagnosis and Management of the Pediatric Foot and Ankle in Cerebral Palsy Patients
Supplemental material, sj-pdf-1-fao-10.1177_24730114221091800 for Topical Review: Approach to Diagnosis and Management of the Pediatric Foot and Ankle in Cerebral Palsy Patients by Sean A. Tabaie, Anthony J. Videckis, Theodore Quan and Evan D. Sheppard in Foot & Ankle Orthopaedics
Footnotes
Ethics Approval
Ethical approval was not sought for the present study because this study is a review article without any patient information and institutional review board approval is not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.