
Abstract
Background: Children with cerebral palsy (CP) often demonstrate postural control difficulties. Orthotic management may assist in improving postural control in these children.
Objective: The purpose of this investigation was to examine the influence of floor reaction ankle foot orthosis (FRAFO) on postural flexion called the crouch position in children with CP.
Study Design: Quasi-experimental.
Methods: Eight children with spastic diplegic CP and eight matched typically developing children participated in this study. Postural control of children with CP was assessed in a static standing position on a force platform with/without a FRAFO. The parameters used were centre of pressure (CoP) measures, calculated from force platform signals including the standard deviation (SD) of excursion; phase plate portrait and SD of velocity in anteroposterior (AP) and mediolateral (ML) directions.
Results: The maximum knee extension was statistically significant in children with CP when barefoot compared to wearing braced footwear (p < 0.05, t = 10.01). AP and ML displacement, AP velocity and AP phase plate portrait of CoP were not statistically significant between children with CP with/without a FRAFO (p < 0.05).
Conclusion: FRAFO can improve the alignment of the knee, but may not be helpful in improving postural control in children with CP in a short time period.
This article will provide objective evidence about the effect of FRAFO on the postural control in children with CP. Therapists can use FRAFO to effectively decrease the knee joint angle in the sagittal plane in children with spastic CP, but cannot use it to improve the postural control.
Introduction
Postural control refers to an ability to control the body’s centre of mass (CoM) over the base of support (BoS).1–3 Children with cerebral palsy (CP) demonstrate poor postural control resulting in poor walking ability and reaching.1,3–7 Crouch position is a very common example of poor postural control in children with CP. This position refers to increased knee and hip flexion and ankle dorsiflexion 8 and is due to insufficient plantar flexion/knee extension.8–10 The crouch position may result in decreased postural control and increased muscle weakness in children with CP.4,11
Various interventions, such as orthotic management, surgery and physical training, are employed to overcome the crouch position in these children.2–4,6,12 A floor reaction ankle foot orthosis (FRAFO) increases external knee extension by altering the ground reaction force (GRF) in sagittal plane.8,10 It can also limit the ankle dorsiflexion.9,10 Few studies have examined the benefits of ankle foot orthoses (AFOs) for improving the postural control in children with CP. Furthermore, there is limited detailed evidence that evaluates the effect of AFOs in children with CP. 13 Rha et al. examined the effect of a hinged AFO on balance control in these children and concluded that it may improve their postural control. 3 Burtner et al. demonstrated that AFOs may be useful in improving balance. However, they were not successful in balancing muscle use in children with CP, who use an excessive degree of antagonist co-activation. 12 Rogozinski et al. examined the efficacy of a FRAFO in children with CP and found improved knee extension in the sagittal plane. 9 Lucareli et al. showed that a FRAFO can effectively improve the knee and ankle extension in children with spastic CP in the stance phase. 10 In another study on children with CP, Westberry et al. demonstrated that AFOs were not useful for improving the static foot malalignment. 14 To conclude, a FRAFO may be effective in reducing or eliminating the crouch position. However, there seems to be no evidence to demonstrate the influence of the FRAFO on postural control in these children. Therefore, the purpose of this study was to determine the effect of the FRAFO for children with CP on postural control during biomechanical realignment in a static standing position.
Methods
Subjects
Eight children with spastic diplegic CP (six females, two males; mean±SD age, height and weight: 8.12±2.41 years, 1.21±0.10 m, 21.87±5.93 kg respectively) and eight typically developing (TD) children (six females, two males; mean±SD age, height and weight: 8.37±2.13 years, 1.27±0.17 m, 25.25±4.16 kg, respectively) were recruited for this study. The children with CP demonstrated the crouch position during static standing, had no history of orthopaedic surgery in the past 1.5 years, and scored level 1 or 2 on the Gross Motor Function Classification System (GMFCS).3,15,16 The GMFCS was used to evaluate the severity of impairment. Level 1 represents mild restriction in mobility and level 5 indicates no independent mobility. 16 The spasticity of the triceps surae, hamstring and quadriceps muscles was examined using the Modified Ashworth Scale.17–19 Children with a Modified Ashworth score of 1 and 1+ were recruited for this study. Children were excluded if they had any fixed flexion contractures in their hip or knee joints, and any history of disease in the vestibular system affecting balance or a head injury.1,3,9 The TD children were screened and matched with children with CP based on their gender, age and weight. Children with a history of head injury, neurological, musculoskeletal and vestibular dysfunction were excluded from the study. 1 An orthopaedic surgeon examined all the children prior to participation in the study. The Human Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences approved the study protocol and the parents of the participating children provided their informed consent.
Data collection
Children in this study were selected from Valiasr Rehabilitation Center (VRC). VRC is a non-profit large rehabilitation centre with two branches in the north and south of Tehran providing services for children with physical dysfunction. A judgement sampling method from a convenient sample was used to recruit children in this quasi-experimental trial. Data were collected using a demographic questionnaire, clinical observation and examination of the subjects, an electrogoniometer and a force platform. Children with CP were asked to use a FRAFO for four weeks. The FRAFOs in this study were custom moulded made of 3-mm thickness polypropylene using a negative cast technique.3,12 The proximal part of the brace extended to just below the fibular head and its footplate extended to the tips of the toes. 3 Gradual adjustment to alternator ankle hinges was used to reduce the crouch position over a four-week period (Figure 1). Each child was seen four times during the first month to apply a gradual decrease in the orthotic ankle joint angle (at least five degrees a week). This procedure assisted adjustment to the new joint position and also prevented possible backward falls. Parents were advised to control the hind foot and knee positions while their children were wearing the FRAFO. The tests of this study were performed when the orthotic ankle hinge was in a neutral position (i.e. the leg perpendicular to the plantar plane of the foot 9 ).
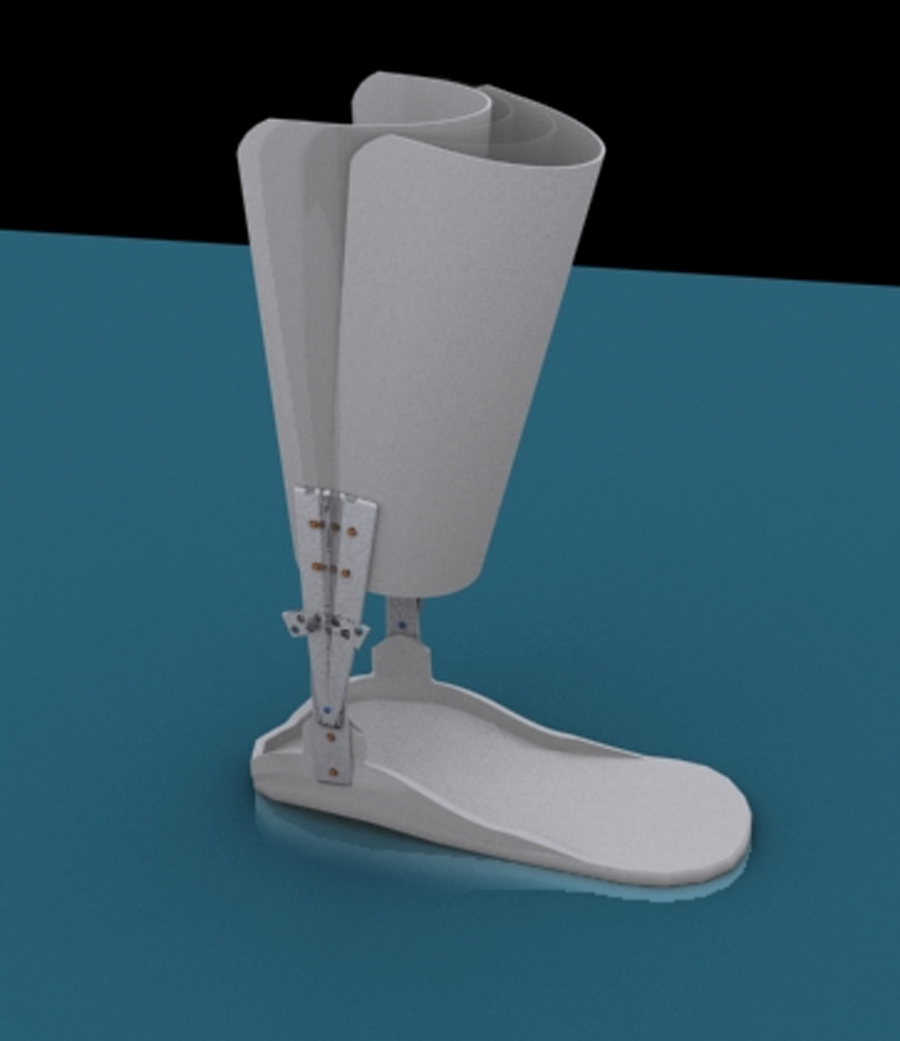
Adjustable floor reaction ankle foot orthosis.
The CoP was collected at the sampling frequency of 100 Hz using a strain gauge Kistler 9286BA force platform, Kistler 9865 amplifier and Kistler 5691A Data Logger (100 Hz, Switzerland). Data were stored for analysis on a Pentium-based PC. Force plate signals were exported to EXCEL for calculation of CoP parameters by formulae. 20 Standard deviation (SD) of velocity and displacement of CoP was measured in anteroposterior (AP) and mediolateral (ML) directions along the X-axis and Y-axis. Calculation using the formulae was also completed for a phase plane portrait. The phase plane portrait captured both static and dynamic aspects of postural control, but the SD of velocity and displacement provided insight only into the dynamic aspects of postural control.21,22 Environmental conditions, such as noise, temperature and humidity, were relatively similar between the tests.
An electrogoniometer was used to measure the knee joint angle with/without the FRAFO. Knee joint angle was measured prior to, and four weeks after, the orthotic intervention. The force plate signals were recorded after wearing the FRAFO for four weeks.
Each child was instructed to stand in a comfortable position with their arms hanging at their sides. Data were collected for 20 seconds.1,3,23 A two-minute seated period for relaxation was provided after each test.1,3,23 Children with CP were asked to stand with and without the FRAFO while assessing the CoP parameters. All children (both groups) were exposed to three trials during the study. Overall the, CP group was exposed to six trials within two experimental circumstances (with/without FRAFO) and the TD group three trials. The first sequence was three trials of ‘barefoot-FRAFO’ and the second one was three trials of ‘FRAFO-barefoot’ which were randomly assigned to the participants for COP signals collection to minimize the so-called ‘carry-over’ effects. This could have reduced the possible effect of first test condition on the following test results.
Statistical analysis
Prior to analysis, the CoP parameters (AP, ML), were calculated from displacement data measured by the force platform. Force plate signals were filtered with a low pass filter with a cut-off frequency of 5.0 Hz. 1
Relative and absolute reliability for each parameter were assessed using an interclass correlation coefficient (ICC) and standard error of measurement (SEM) (Table 1). Munro’s classification for reliability coefficients were used to describe the degree of reliability. 24 The Kolmogrov-Smirnov (K-S) test was applied to determine if the sample represented a normal distribution. The mean difference of each parameter was calculated between the CP group with a FRAFO and the TD group (CP with FRAFO-TD). The same process was repeated for all the recorded parameters of the CP group without FRAFO and TD group (CP without FRAFO-TD). Then a paired t-test was used to compare the mean of the new calculated parameters. Also, a paired t-test was used for comparing the mean of the knee joint angle data in CP group with and without a FRAFO. To determine the changes independent t-tests were used comparing the CP group (for both with/without FRAFO) and TD children (Table 2). For all tests, the p value < 0.05 was considered statistically significant. The results were analyzed using SPSS version 16.0 (SPSS Inc., Chicago, IL, USA).
Reliability analysis of parameters in deferent conditions.
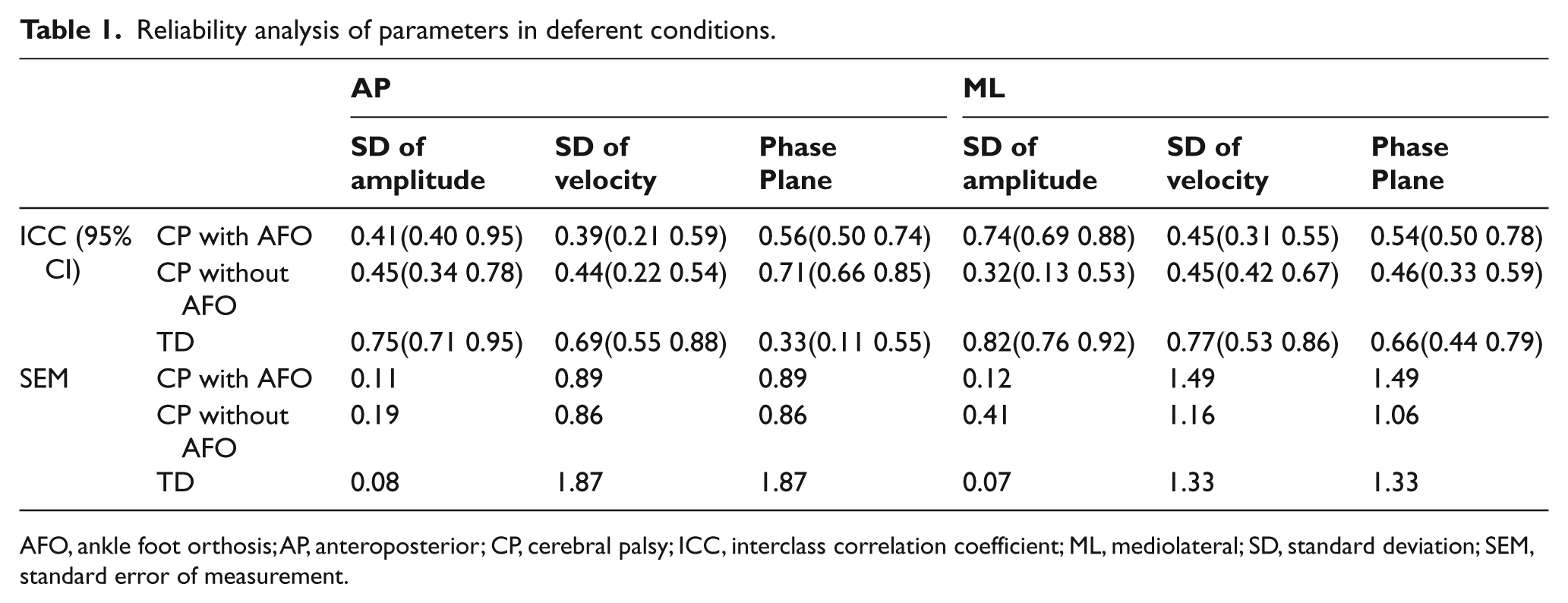
AFO, ankle foot orthosis; AP, anteroposterior; CP, cerebral palsy; ICC, interclass correlation coefficient; ML, mediolateral; SD, standard deviation; SEM, standard error of measurement.
Descriptive data for centre of pressure (CoP) measures in different conditions of postural control.
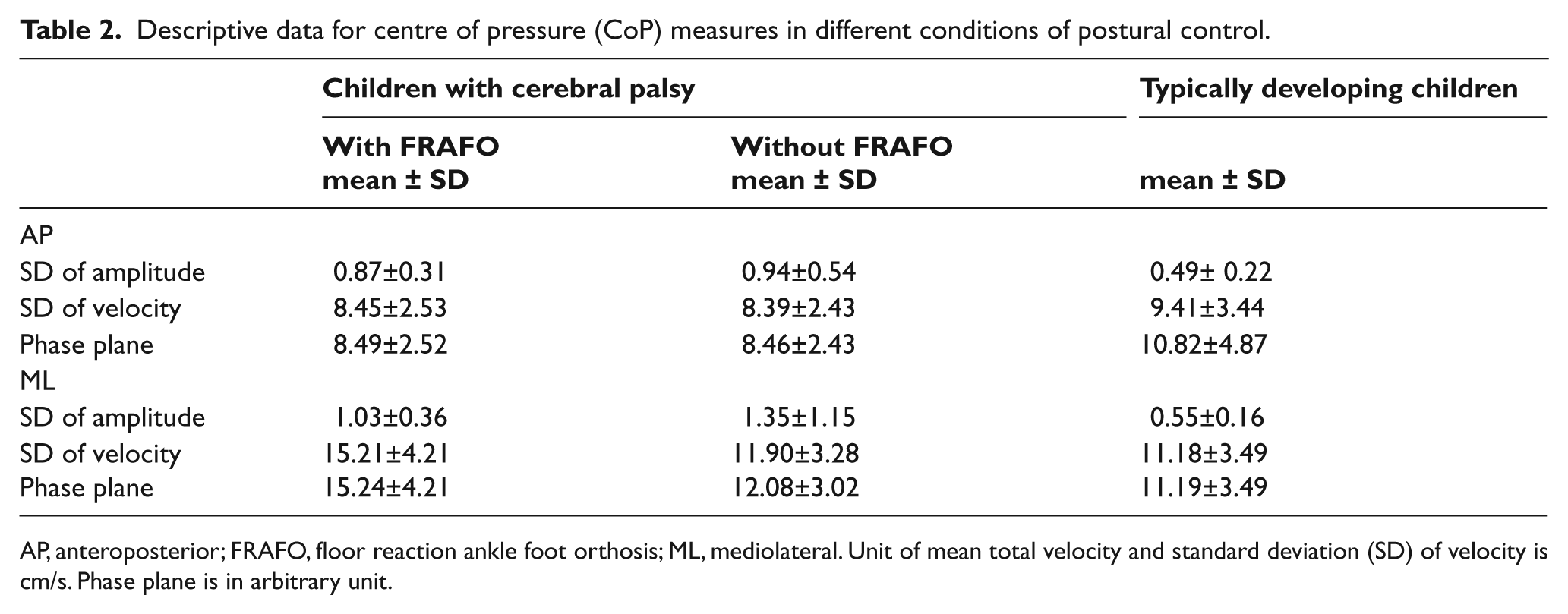
AP, anteroposterior; FRAFO, floor reaction ankle foot orthosis; ML, mediolateral. Unit of mean total velocity and standard deviation (SD) of velocity is cm/s. Phase plane is in arbitrary unit.
Results
There was no statistically significant difference for age (p = 0.76) and weight (p = 0.58) between the two groups. Descriptive statistics of the CoP parameters for CP and TD groups are displayed in Table 2. In comparison to the TD children, children with spastic CP in both circumstances (with/without FRAFO) showed lower values for SD in velocity and phase plane portrait in the AP direction. These parameters were higher in children with CP when barefoot compared to wearing braced footwear.
Summery of t-test to determine the changes of the mean difference between cerebral palsy (CP) with floor reaction ankle foot orthosis-typically developing (FRAFO-TD) group and CP without FRAFO-TD group. Data comparisons in CP group with/without AFO-TD children.
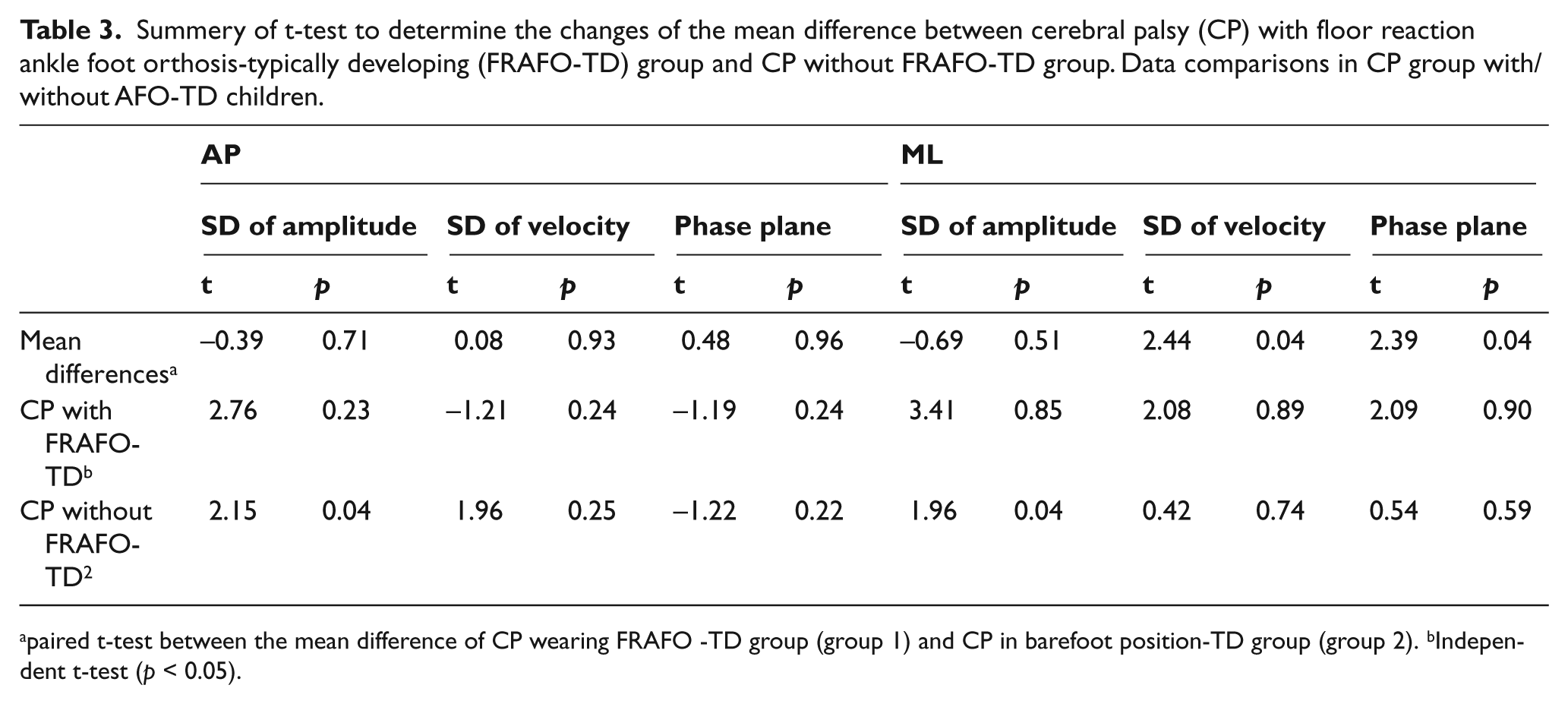
paired t-test between the mean difference of CP wearing FRAFO -TD group (group 1) and CP in barefoot position-TD group (group 2). bIndependent t-test (p < 0.05).
The normal distribution of data was tested using a K-S test. The results demonstrated that the data were normally distributed (p < 0.05). Using a paired t-test revealed that the SD of velocity in the ML direction (p < 0.05, t = 2.44) and also, the phase plane portrait in ML direction (p < 0.05, t = 2.39) were statistically significant in children with CP when barefoot compared to a braced position (p < 0.05). However, there were no significant differences in all postural control parameters with the exception of the two previously mentioned ones (p < 0.05). The knee joint angle in the CP group with/without FRAFO were statistically significant (p < 0.05, t = 10.01). There were significant differences in all parameters between children with CP when braced and the control group (p < 0.05) (Table 3).
Discussion
The findings of this study indicated that a FRAFO can decrease the knee flexion angle in children with CP in the sagittal plane in a static standing position. Rogozinski et al. and Lucareli et al. reported similar results.9,10 The crouch position in children with CP results from a plantar flexion/knee extension imbalance. This may be a result of lower limb biarticular muscle spasticity and monoarticular muscles lengthening.8–10 GRF at crouch position is behind the knee axis, while muscles are not strong enough to correct plantar flexion/knee extension imbalance in these children.8,10 The FRAFO applies GRF directly into the anterior compartment of the knee joint and increases extension.8,9 Therefore, it can improve the knee joint angle in the sagittal plane improving knee extension.
The results of this study also revealed no statistically significant change in the excursion of postural sway in both directions and AP sway velocity in children with CP with/without the FRAFO. The results support the Rha et al. study which showed that there is no significant effect from a hinged AFO for improving the standing postural control of children with CP. 3 The findings of this study also concur with the observations of Burtner et al. who suggested that AFOs did not alter the preferred pattern for balance control in children with CP. 12 Leg and foot segmental malalignment in children with CP move the line of action of GRF lateral to the centre of the knee joint and can change the moment arm of the GRF about the knee axis. 9 AFOs neither improve the static foot malalignment (to correct the line of GRF in ML plane) and nor organize muscle use.12,14 These are the two main disruptions to postural control.4,6 However, it appears that a FRAFO (one type of solid AFOs) failed to improve the two main areas of deficits in postural control. Therefore, it was not able to improve the postural control of children with CP.
Another finding of this study revealed a significant increase in ML postural sway velocity in children with CP when wearing FRAFO. For children with CP, hip and body transverse rotation strategies are important for maintaining postural control. 1 For these children, ankle movement including plantar/dorsiflexion or inversion/eversion contributes less to maintaining the postural control, especially in the ML direction. 1 A FRAFO provides a neutral position for the ankle joint, but eliminates or minimizes the ankle and subtalar motion.9,10 Therefore, using a FRAFO for children with CP may eliminate the compensatory ankle strategy for reducing the speed of CoP excursion in ML direction. Increased ML postural sway velocity in children with CP wearing a FRAFO may positively affect postural control by eliminating the ankle strategy in a solidly braced position.
The results of this study indicated that the mean values of phase plane portrait in ML direction were statistically significant in children with CP using a FRAFO in comparison to no-brace, but were not significant in an AP direction. Increasing the value of the phase plane portrait in the ML direction in this group may be affected by enhancing ML postural sway velocity in comparison to the no-brace position (as mentioned previously, the phase plane portrait was achieved by calculating two parameters including CoP displacement and postural sway velocity 20 ). There seems to be no studies indicating the effects of AFOs (especially FRAFO) on phase plane portrait in children with CP. The report by Woolacott et al. showed that the crouched position may decrease the ability of children with CP to recover postural control. 4 According to their results, using a FRAFO to minimize the crouch position may improve postural control. However, significant improvement of ankle and knee movement in children wearing a FRAFO with CP did not further improve postural control improvement. Although, using a FRAFO may reduce the crouch position, it is not completely effective in improving the postural control of children with CP in a static standing position. This is probably due to the reduction in the compensatory ankle movement.
A potential limitation of this study is the small sample size in most parameters except for the excursion of CoP in both the AP and ML directions. Therefore, future research would be beneficial with a larger sample size.
Conclusion
This study demonstrates the effect of a FRAFO in decreasing the knee flexion angle in the sagittal plane. Thus, it might be expected that the FRAFO can biomechanically improve the crouch position. In contrast, this orthosis neither reduced the CoP excursion of postural sway, nor the AP sway velocity. Furthermore, it did increase the ML postural sway velocity. However, the FRAFO failed to improve the mean values of the phase plane portrait. In summary, this orthosis could be considered as contraindicated for children with CP who have significantly poor postural control, especially in the ML direction. The functional benefit of a FRAFO may be due to its ability to reduce the crouch position in children with CP, despite it being unable to improve postural control in a static standing position.
Footnotes
Acknowledgements
We would like to thank Dr Farhad Tabatabaii, Dr Ali Hossieni, Dr Mohammad R Safari and Dr Bijhan Forough for their valuable comments throughout this study.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.