
Abstract
Background:
Ankle-foot orthoses may be used in pre-ambulatory children with cerebral palsy; however, their effect on the acquisition of walking is unknown. This case report aims to evaluate the effect of an ankle-foot orthosis–footwear combination on the acquisition of walking in a single subject with cerebral palsy.
Case Description and Methods:
This study reports the orthotic management of a single child with spastic bilateral cerebral palsy over a 15-month period, during which time the ability to independently stand and walk was acquired. Custom rigid ankle-foot orthoses were prescribed. Gait speed and Edinburgh Visual Gait Score were assessed with and without the orthoses.
Findings and Outcomes:
The subject developed the ability to stand and walk using an ankle-foot orthosis–footwear combination with a walker frame, and to a limited extent without a walker frame. The subject remained unable to take independent steps unless wearing the ankle-foot orthosis–footwear combination. Clinically significant differences in gait speed and Edinburgh Visual Gait Score were observed.
Conclusion:
An ankle-foot orthosis–footwear combination may aid the development of independent walking in some children with cerebral palsy. Further research on the effects of orthoses on the acquisition of walking ability in children with cerebral palsy is needed.
Clinical relevance
Custom rigid ankle-foot orthoses combined with footwear may aid the development of independent standing and walking in some children with bilateral spastic cerebral palsy. This intervention may be considered in clinical practice and future research in this patient group.
Background
Ankle-foot orthoses (AFOs) can influence spatio-temporal gait characteristics, kinetics, kinematics, energy expenditure and gross motor function in cerebral palsy (CP). This is affected by clinical presentation and AFO design.1–5 The literature is limited in clinical applicability, however, as most studies do not describe the orthoses used.6,7 One approach to AFO design emphasises the importance of sagittal plane alignment of the shank within the ankle-foot orthosis–footwear combination (AFO-FC).8,9
A report from the International Society for Prosthetics and Orthotics includes ‘to provide a base of support’ and ‘to facilitate training in skills’ as aims of orthotic management in CP. 10 Use of AFOs to support the development of walking is in line with these aims. However, while the development of walking in children with CP has received some attention in the literature,11,12 the effect of orthoses on the acquisition of walking in children with CP is unknown. This case study aims to evaluate early intervention with AFOs in a subject with CP, before the onset of independent standing or walking.
Case description and methods
The CARE reporting guidelines were followed. 13 Written consent was obtained from the patient’s parent for publication of the information and images in this article. The subject was a female aged 1 year 5 months at the initial orthotic assessment (see Table 1). A diagnosis of CP was suspected and confirmed 3 months later. Her parent reported delayed motor skill development – crawling but unable to stand or step independently. The presentation was a bilateral spastic distribution. 14 Primarily, the lower limbs were affected, with the upper limbs mildly affected. Assisted stepping was initially a Melbourne type one pattern but changed to type two (see Figure 1(a) and (b)) and later type five (see Supplemental Appendix) over a period of 10 months. 15
Timeline of changes in presentation and orthotic treatment.
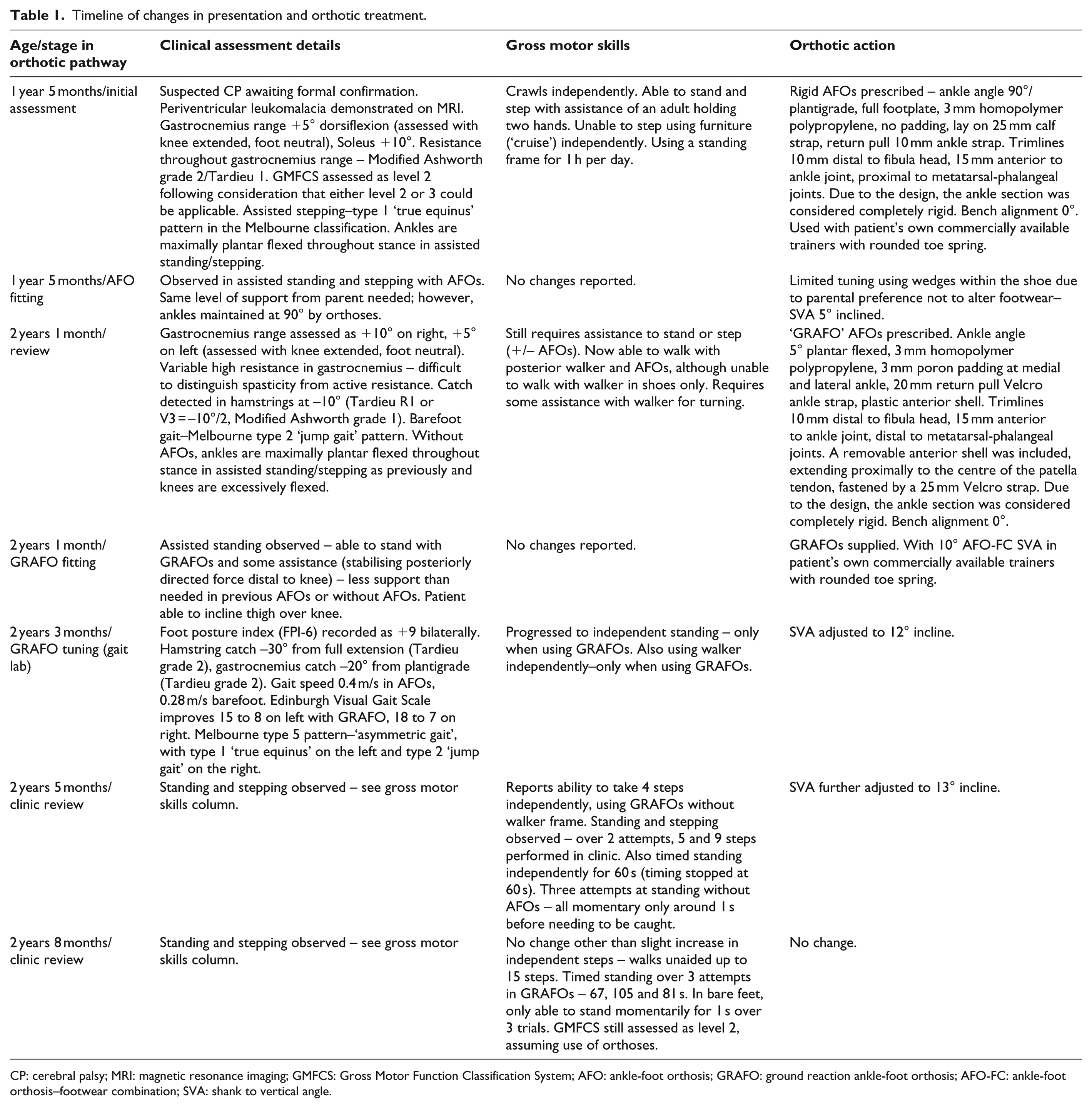
CP: cerebral palsy; MRI: magnetic resonance imaging; GMFCS: Gross Motor Function Classification System; AFO: ankle-foot orthosis; GRAFO: ground reaction ankle-foot orthosis; AFO-FC: ankle-foot orthosis–footwear combination; SVA: shank to vertical angle.
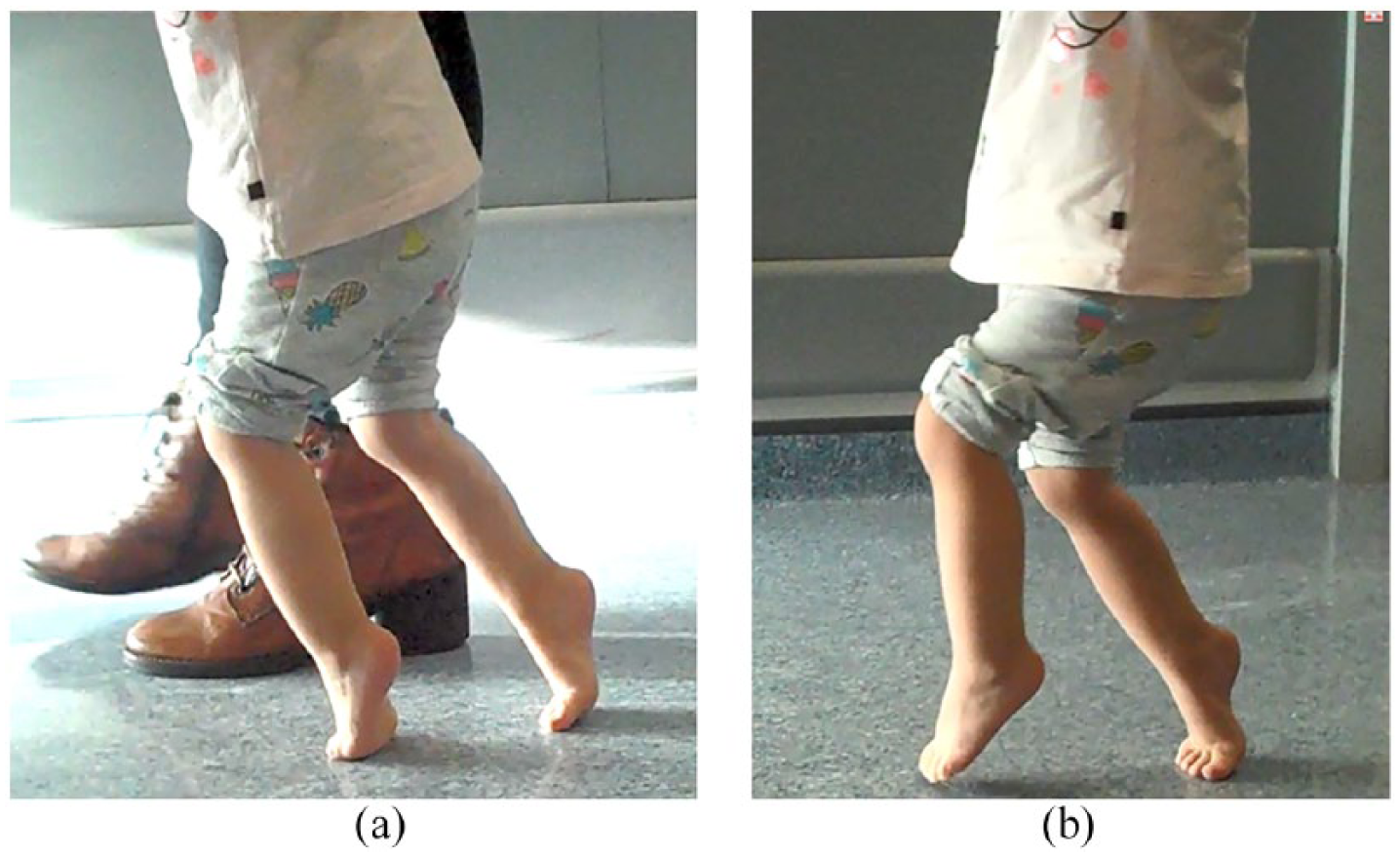
Assisted stepping in barefoot at age 2 years 1 month, displaying (a) excess knee flexion and (b) ankle plantar flexion through gait.
Assessment tools used included the Tardieu and Modified Ashworth Scales (muscle tone) 16 and the Gross Motor Function Classification System (GMFCS) (mobility level). 17 Gait speed and Edinburgh Visual Gait Score (EVGS) 18 were assessed with and without orthoses at one time point, 10 months following initial prescription of the AFOs. The EVGS uses 17 observations from gait to give a score between 0 and 34 for each limb, with higher scores indicating greater impairment. Gait speed and EVGS were assessed from video over 3 m with a 2-m run up in barefoot (holding parent’s hands) and in AFOs (with posterior walker frame). Order of testing was AFOs first, then barefoot. Timing was completed with a stopwatch by the orthotist, and an average was taken from two runs. EVGS was also scored by the orthotist. Testing was conducted at the beginning of the day.
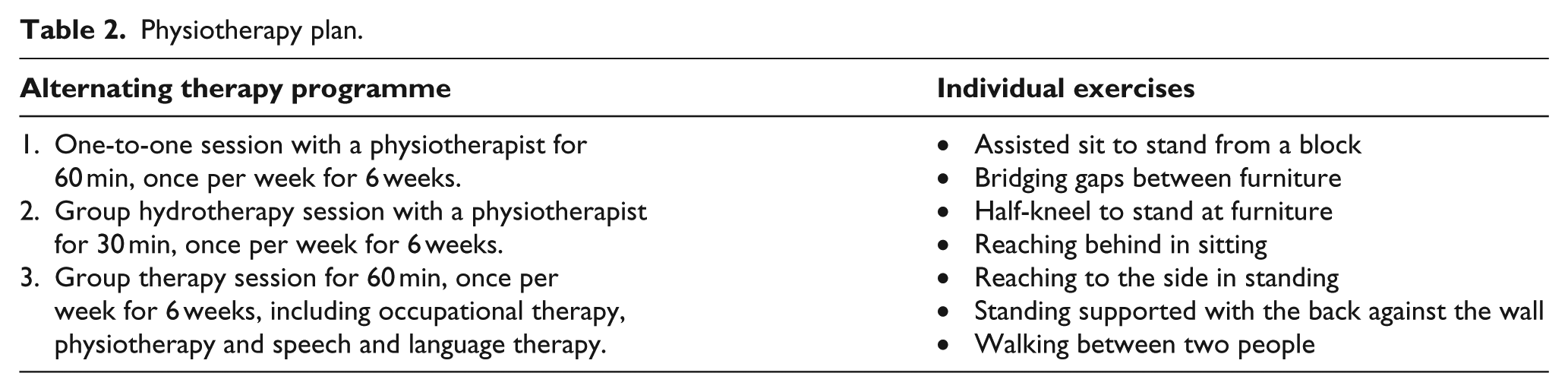
Full details on the custom AFO design are given in Table 1, described with reference to a published guideline. 7 Physiotherapy input is summarised in Table 2. During therapy, orthoses were worn for half of the time. At age 1 year 5 months, rigid AFOs were prescribed to aid assisted standing and stepping. The metatarsal-phalangeal joints (MPJs) were flexible. The mechanical goal was to prevent ankle plantar flexion during swing and stance phase. The ankle was aligned in 90° (plantigrade) in the AFO. Some tuning was undertaken with the AFOs, resulting in a slightly suboptimal shank to vertical angle (SVA) of the AFO-FC of 5° incline due to a limit in how much wedging could be added inside the shoe and parental preference not to have the footwear adapted at this stage. An SVA of 10°–12° incline or higher is more typically used. 19
Physiotherapy plan.
At age 2 years 1 month, the orthosis was changed to include an anterior shell and fixed MPJs. This design is frequently described as a ‘ground reaction ankle-foot orthosis’ (GRAFO). The mechanical goals were to prevent ankle plantar flexion during swing and stance, prevent excess knee flexion during stance and increase peak hip extension in stance. The ankle was aligned in 5° of plantar flexion in the orthosis due to increasing calf muscle tone, with bench alignment of the AFO of 0°. It was assumed that placing the ankle into plantigrade in the presence of increasing muscle tone may cause discomfort and possibly reduced knee extension due to the effect of stretching gastrocnemius, which also crosses the knee. An SVA of 10° was selected as 10°–12° SVA is recommended for excessive incline without knee/ankle stiffness. 19 Tuning was initially completed by measuring the SVA in standing, and then by observing the SVA at midstance using slow motion video without a ground reaction force overlay. This approach is in line with work that suggests that the SVA in standing and at midstance during gait are equivalent. 20 By the time video was used to assist tuning (age 2 years 3 months), a mixed gait pattern was present (Melbourne type five – see Table 1 and Supplemental Appendix). At this point, the SVA was adjusted to 12° incline. The subject’s own footwear was used – a trainer with a sole featuring a rounded toe spring, without custom adaptations. This was because the parent preferred not to modify the footwear, and it was concluded that the AFO-FC functioned well without modification. Use of the AFOs was reported as 5 h per day.
Findings and outcomes
A timeline illustrates patient presentation and clinical assessments over time (see Table 1).
Gross motor skills
There were no changes in mobility reported or observed in clinic following prescription of AFOs at age 1 year 5 months. At 2 months following the provision of the new AFOs (2 years 3 months), changes in motor skills had occurred with the subject progressing to independent standing and walking using a walker frame; however, these activities required the AFOs. At 4 months following provision of the AFOs (2 years 5 months), the subject could take some steps without a walker frame. Nine consecutive steps were observed in clinic. The subject could stand for more than 60 s without support other than the AFOs – over three attempts, the mean time was 84 s. Without AFOs, standing balance could only be maintained momentarily, for a mean of 1 s over three attempts (see Table 1).
Gait speed and EVGS
At review 2 months following fitting of AFOs (2 years 3 months), gait speed was 0.28 m/s barefoot (holding parent’s hands) and 0.40 m/s in AFOs (with posterior walker frame). Using the EVGS (see Supplemental Appendix), the left side was rated as 15 points barefoot and 8 points in orthoses. The right side was rated as 18 points barefoot and 7 points in orthoses.
Patient perspective
In line with the recommendations,
13
the patient’s parent was asked to give their perspective. An excerpt of the feedback is presented: The splints work. Without them she can stand up on tiptoe next to a table, but with the splints she can take steps – up to 10 steps when she has motivation to get something – she can walk […] She will bring me the shoes and splints and tell me ‘I want to walk’.
Discussion
This case study reports on a child who was unable to stand or walk independently prior to use of AFOs and, despite therapy with and without orthoses, remained unable to walk without AFOs. Use of orthoses may have expedited the onset of independent gait; however, the influence of factors such as natural development and physical therapy were not controlled for, which is a confounding factor.
Clinically significant cross-sectional differences in gait speed and EVGS were also observed. Gait speed with AFOs increased by 0.12 m/s (42.9%). Minimal clinically important difference (MCID) for gait speed has been reported as between 6.8% (medium) and 10.9% (large) in GMFCS level 2. 21 EVGS scores improved by 7 points on the left and 11 points on the right, both exceeding the reported MCID of 2.4. 22 These results may over-estimate the effects of the AFOs, however, by comparing barefoot gait with gait in shoes and orthoses. In addition, in one condition, support was provided by the parent, while in the second condition, support was provided by a frame which is a further confounder. However, the subject was unable to walk with the frame in shoes only which precluded testing this.
The AFO prescribed was intended to be in line with thinking outlined by Meadows, 8 Owen9,19 and Eddison 23 which emphasises the importance of shank alignment and tuning or optimisation of the orthotic prescription. The authors believe that the child in this case study represents an example of the success that can be achieved in some cases when using optimised rigid AFOs. However, given that the footwear was not altered or optimised, the AFOs were not considered tuned according to the full process described by Owen.9,19
Conclusion
Early use of AFOs may have expedited the onset of independent walking in a pre-ambulatory child with CP. Clinically significant cross-sectional differences in gait speed and quality were also achieved with the AFOs. Limitations of the study design have been discussed; further research on the effects of orthoses on the acquisition of walking ability in children with CP is needed.
Supplemental Material
Appendix_-_Gait_lab_images_final – Supplemental material for Improved motor function in a pre-ambulatory child with spastic bilateral cerebral palsy, using a custom rigid ankle-foot orthosis–footwear combination: A case report
Supplemental material, Appendix_-_Gait_lab_images_final for Improved motor function in a pre-ambulatory child with spastic bilateral cerebral palsy, using a custom rigid ankle-foot orthosis–footwear combination: A case report by Joshua Young and Sally Jackson in Prosthetics and Orthotics International
Footnotes
Acknowledgements
The authors would like to thank the subject’s parents for their engagement and permission to publish the information in this article. We would also like to acknowledge Queen Mary’s Hospital orthotic service and gait laboratory for their assistance, and Laura Underhill for her comments on the manuscript.
Author contributions
J.Y. conceived the study, and drafted and revised the manuscript. Both authors were involved in data collection, and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.