
Abstract
Background:
Patients with neuromuscular diseases such as cerebral palsy (CP) are living longer because of advances in medicine, yielding a larger number of adult patients that could benefit from corrective surgery. However, some surgeons are hesitant to offer surgery to these patients because of concern for postoperative complications. A paucity of literature exists that describes complications in patients undergoing foot and ankle surgery for neuromuscular diseases. The primary study outcome was to identify the postoperative complication rates associated with foot and ankle surgery in adult patients with neuromuscular disease.
Methods:
The charts of patients with neuromuscular diseases who had foot and ankle surgery by the senior author at a single institution from March 2010 to March 2020 were reviewed. Patient charts were reviewed for demographic data, medical history and diagnoses, and surgical treatment information. Only patients’ index procedures with the senior author were evaluated for surgical data. Patient charts were assessed to determine the presence or absence of a postoperative complication following an index procedure.
Results:
In a cohort of 42 patients, females comprised 60% of the patient cohort. The average age was 35 (range, 20-69) years old. CP was the most common neuromuscular diagnosis at 52% (22 of 42) patients. Eighteen percent (11 of 60) of the index surgeries had 1 or more complication with a total of 13 complications. The overall wound complication rate was 10% (6 of 60), infection rate was 8% (5 of 60), and the nonunion rate following arthrodesis was 10% (2 of 21).
Conclusion:
We conclude that foot and ankle surgery in this complex population can be done safely, with postoperative complication rates similar to the average population. Although these patients may present with unique challenges, surgeons should not forgo surgery out of concern for postoperative complications.
Level of Evidence:
Level IV, retrospective cohort study at a single institution.
Introduction
Patients with neuromuscular diseases, such as cerebral palsy (CP), can be very limited in mobility. These mobility limitations can have long-lasting effects on lifestyle and well-being. In their review of adults with CP, Andersson and Mattsson 1 report that 35% of patients had decreased walking ability and 27% had never been able to walk. Eighty percent of these patients reported contractures, and 18% suffered from pain every day.
Adult patients with neuromuscular disease commonly experience limb deformities among other musculoskeletal pathologies. 7 Fabry et al 3 showed that conservative treatment with shoes, lifts, and bracing was not effective in correcting bony deformity. Patients with neuromuscular diseases such as CP are living longer because of advances in medicine. Increased life expectancy in this patient population combined with desire for improved function creates a large number of patients who may benefit from deformity correction.
To our knowledge, there is no literature that reports postoperative complications following foot and ankle surgery in the population of adults with neuromuscular disease. Some surgeons are hesitant to offer surgery to these patients because of concern for complications. This study seeks to provide more information regarding postoperative complications associated with foot and ankle surgery in adult patients with neuromuscular disease.
Methods
Following approval from the institutional review board, a retrospective chart review was conducted on patients with neuromuscular disease who underwent foot and ankle surgery by the senior author from March 2010 to March 2020. Fifty-two extremities in 42 patients were included in the final analysis. Inclusion criteria were the diagnosis of a neuromuscular condition leading to weakness, spasticity, or deformity of the foot or ankle; surgery performed to correct foot deformity; age >18 years at time of surgery, and a minimal follow-up of 6 months for arthrodesis procedures and 3 months for all other procedures. Exclusion criteria included the following: (1) patients with Charcot-Marie-Tooth (CMT) disease; (2) patients with inadequate follow-up; (3) patients with uncontrolled or complicated diabetes; and (4) patients on our institution’s research exclusion list.
The primary study outcome was to identify the overall complication rate associated with foot and ankle surgeries in adult patients with neuromuscular disease. Patient charts were reviewed for demographic data, medical history and diagnoses, and surgical treatment information. For the purpose of our study, we identified an index surgery as the first surgical intervention performed on a given extremity for a unique foot and ankle pathology. Only the index surgery was evaluated for complications. Subsequent surgeries such as irrigation and debridement, hardware removal, or revision surgery were not separately assessed for complications. Operative notes for index surgeries were then reviewed to classify the procedure type(s). Procedures were classified into categories of Achilles lengthening, other tendon lengthenings or tenotomies, tendon transfers, arthrodesis, osteotomy, lesser toe procedures, or other.
Patient charts were further reviewed to determine the presence or absence of a postoperative complication following index surgery. We defined a postoperative complication as the development of wound problems, infection, nonunion or delayed union, or medical complication. Wound problems were defined as delayed healing or dehiscence requiring additional treatment to obtain final healing. Medical complications included, but were not limited to, deep vein thrombosis, pulmonary embolism, and sepsis. Patients’ postoperative follow-up appointment notes, emergency department visit notes, and hospital admission notes were evaluated to assess for complications.
Results
The final patient cohort consisted of 42 patients (52 extremities). The cohort was 60% female (25 of 42 patients). The average age was 35 years (range, 20-69). CP was the most common neuromuscular diagnosis, accounting for 52% of the patients (22 of 42 patients). Patients were affected by conditions including CP, spina bifida, multiple sclerosis, Down syndrome, Rett syndrome, Hallervorden-Spatz syndrome, Apert syndrome, muscular dystrophy, leukodystrophy, cerebrovascular injury, spinal cord injury, traumatic brain injury, and transverse myelitis. Patient demographic information and neuromuscular diagnoses are summarized in Table 1.
Demographics (N = 42).

Abbreviation: CVA, cerebrovascular accident.
A total of 60 index surgeries were performed. The number of procedures performed during a patient’s index surgery ranged from 1 to 15, with an average of 3.3 procedures per index surgery. Achilles lengthening was the most common procedure performed, occurring in 45% (27 of 60) of index surgeries. Tendon transfers and arthrodesis were the next most common procedure types, occurring in 40% (24 of 60) and 35% (21 of 60) of index surgeries, respectively. Osteotomies were performed in 30% (18 of 60) of index surgeries, whereas tendon lengthening and tenotomies were performed in 23% (14 of 60) of index surgeries. Lesser toe procedures were performed in 13% (8 of 60) of index surgeries.
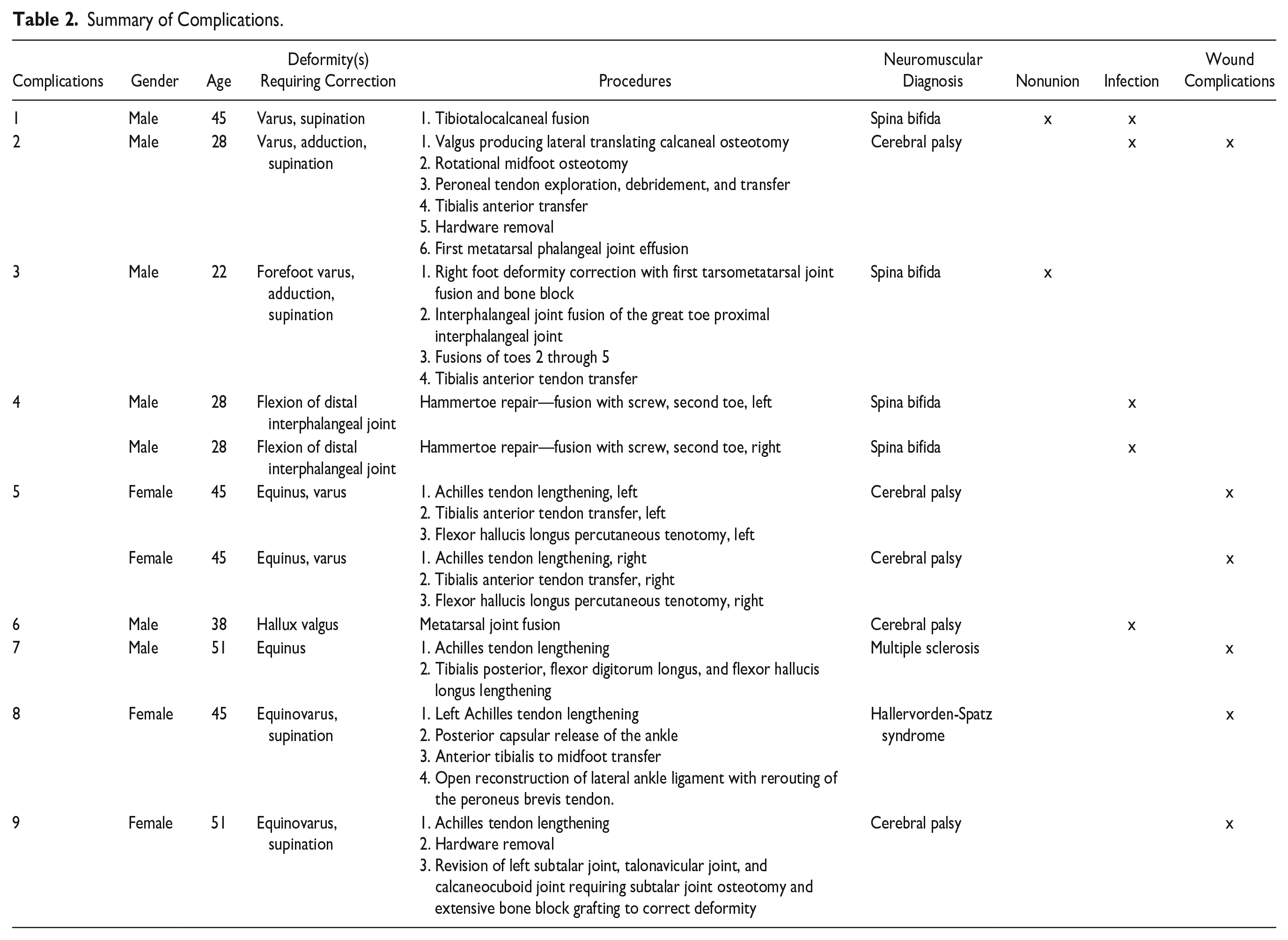
Mean follow-up in the study was 20 months. Thirteen complications in 11 patients were noted, resulting in an 18% (11 of 60) complication rate of index surgeries. The overall wound complication rate was 10% (6 of 60); infection rate was 8% (5 of 60), and delayed union/nonunion rate following arthrodesis was 10% (2 of 21). No patients suffered serious medical complications, such as deep vein thrombosis, pulmonary embolism, or sepsis. A full breakdown of complications by patient, deformity, and corresponding procedure(s) can be found in Table 2.
Summary of Complications.
Discussion
Many neuromuscular diseases are associated with static or progressive foot and ankle deformity. Murphy 6 comments that although CP is neurologically nonprogressive, many secondary conditions may develop, including contractures, degenerative arthritis, and foot deformities. 12,13 Although these foot issues may be asymptomatic in teens, they can lead to limited mobility and weightbearing difficulties later in life.4,6,9 Flexible deformities can also become fixed as the soft tissues contract. 3
A study of 221 adults with CP found that 80% reported contractures and 77% reported problems with spasticity. 1 Another study of 72 adults with CP found that the effects of CP evolve into adulthood, with loss of ambulation and deterioration in walking distance. Among the 72% of the sample who had previously walked, 24% had stopped walking, mainly before the age of 40 years. 1 Even if restoration of ambulation is not possible, obtaining a functional position of the foot is still of great importance. The ability to safely stand and pivot, take short steps in and out of the bathroom, and reach for overhead objects all require a tolerant position of the foot. 7
Several studies have reported successful foot and ankle surgery in adults with CP. Triple arthrodesis combined with soft tissue release and osteotomy was shown in one study to achieve a functional weightbearing position of the foot throughout the adult years. 7 Another study evaluated triple arthrodesis in patients with rigid pes planus deformity. In this study, Horstmann et al 5 reported that resolution of deformity provided an adequate base for standing and improved ability to tolerate shoe wear and/or braces. These studies demonstrate that patients with neuromuscular disease can benefit from surgical treatment.
Foot and ankle surgery has also been found to be beneficial in spina bifida patients. Positioning of the foot in these patients can be challenging, and foot deformity can prevent successful shoe wear or foot positioning in a wheelchair. One study found surgical tenotomy to be more reliable for achieving lasting correction and preventing recurrence as compared to tendon transfer or lengthening. For bony deformities, osteotomies are the treatment of choice, as correction is achieved while preserving joint motion. 10 Another review of 84 adults with spina bifida found that surgical procedures aimed at maintaining a plantigrade foot were beneficial. 8
In our cohort of 46 patients, we noted an 18% (11 of 60) complication rate. This compares favorably with previous literature on elective foot and ankle surgery.
We found our wound complication rate to be similar to that of a general elective foot and ankle surgery population. In a study of 290 foot and ankle patients (295 elective surgeries), 16.9% had postoperative wound complications. 14 In our study, 10% (6 of 60) of index surgeries developed wound complications.
Our cohort’s nonunion rate was similar to that demonstrated in previous foot and ankle literature. One article cited nonunion rates at approximately 12% for foot and ankle arthrodesis. 11 In our study, a total of 21 index surgeries involved arthrodesis, and 10% (2 of 21) of those resulted in nonunion. However, our diagnosis of nonunion was based on radiographs and clinical examination. As some studies have used routine computed tomography scan to evaluate fusion rates, the current study may underrepresent some subclinical nonunions.
We did find that our infection rate was higher than that reported in the general foot and ankle surgery literature. One study of 631 patients undergoing foot and ankle surgery found the infection rates to be 2% to 3%. 2 In our study, 8% (5 of 60) of index surgeries were complicated by infection.
Interestingly, whereas spina bifida patients comprised only 10% of our patient cohort (4 of 42 patients) they accounted for 38% (5 of 13) of the overall complications. These patients accounted for 100% of the nonunions (2 of 2) and 60% (3 of 5) of the infections. Our findings are reflected in other orthopaedic surgery literature with higher rates of infection and nonunion found in spina bifida patients undergoing hip and spine surgery. 15
The study’s main strength is that it adds to a paucity of literature regarding outcomes of foot and ankle surgery in adults with neuromuscular disease. To our knowledge, there is no literature that reports postoperative complications following foot and ankle surgery in the population of adults with neuromuscular disease. Our findings can provide surgeons with more information regarding risks of surgery in this particular patient population and promote future discussion.
This study also has several limitations. The study is limited to 1 surgeon at 1 geographic location within a single hospital system, which may limit its applicability in different environments. The study also had a relatively short follow-up period. Although this should adequately demonstrate the majority of early complications, it is possible that a nonunion could go undetected until later in the postoperative course. We also define nonunion based on clinical examination and radiographs rather than standardized computed tomography scan, which could lead to an artificially low nonunion rate compared with other literature. Another limitation is we did not account for adverse effects on mobility as a result from surgery. Many of the patients had limited mobility at baseline; thus, measuring their changes in mobility would be challenging. Additionally, the patients have a wide range of diagnoses with a wide range of various surgeries. Finally, a comparison of our complication rates to the general patient population is difficult without a control group. Because many of these patients had complex deformities and the surgeries were often quite complicated with up to 15 procedures per surgery, we decided it would not be feasible to create a comparable control group.
Additional research is certainly warranted to further our understanding of foot and ankle surgeries in patients with neuromuscular disease. Future studies could include a larger patient series, longer follow-up, and use of patient-reported outcomes, radiographic evaluation, and degree of correction. A larger patient series may also benefit from further stratification based on primary neuromuscular diagnosis and/or particular surgical procedures.
Conclusion
With an overall complication rate of 18% (11 of 60), our study found that surgical intervention for deformity correction in patients with neuromuscular disease does not carry an increased risk of postoperative complications. Although these patients may present with unique challenges, surgeons should not forgo surgery for concern of increased risk for postoperative complications (with a possible exception to spina bifida patients). Further research is warranted to report outcome measures, better understand the risk for complications in this population, as well as stratify risk based on procedure type and specific neuromuscular disease.
Footnotes
Ethical Approval
Ethical approval for this study was obtained from HealthPartners Institute Institutional Review Board (ID 21-268).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. ICMJE forms for all authors are available online.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.