
Abstract
The term racial trauma is used to describe the cumulative distressing and traumatizing effects of racism in all of its forms, and it closely resembles the construct of posttraumatic stress disorder (PTSD). This investigation aims to increase our understanding of racial trauma by comparing the characteristics of those with a clinically-relevant diagnosis of racial trauma to those without, based on the findings of a clinical semi-structured interview and symptom checklist for assessing racial trauma, the University of Connecticut Racial Ethnic Stress and Trauma Survey (UnRESTS), administered to a diverse group of adults (N = 97). This paper extends prior work on racial trauma by examining the correlations between racial trauma and validated self-report measures of discriminatory distress, controlling for racialization. We examine the correlation between a clinically-relevant diagnosis of racial trauma and racial/ethnic identity. We also compare racism-related PTSD symptoms in those with and without racial trauma to inform clinical assessment. Finally, we examine the factor structure of racial trauma symptoms using the 24 items from the UnRESTS PTSD symptom checklist and compare these to current DSM-5 models. The structure of racial trauma symptoms differed from the DSM-5 4-factor model, as do other PTSD models in the research literature. Clinical and research implications are discussed.
Introduction
Defining Racial Trauma
Racism is a chronic stressor in the lives of people of color (POC) that can result in many adverse mental health outcomes. 1 Racial trauma has been defined as a psychological injury caused by mistreatment of a person due to their race, ethnicity, or skin color.2,3 It may take the form of a severe interpersonal stressor that endangers one's health or even one's life, or it may take the form of an institutional stressor that is motivated by racism and causes considerable continuous pain. Both of these forms have the potential to appear in a variety of ways. 4 Because of its chronic and accumulative nature, racial trauma eventually causes an individual's capacity for coping to become exhausted. 5 Those of any race, ethnicity, or people group can experience racial trauma since it is tied to their social identity. There are various manifestations of racial trauma, including experiencing police harassment (ie, when law enforcement officials harass, threaten, or physically assault a person because of their race or ethnicity), distressing medical experiences (ie, persistent fear for one's own or one's loved ones’ lives after experiencing medical mistreatment), community violence (ie, witnessing or experiencing violence or fear for one's own or one's family's safety), and workplace discrimination. 6
The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5 7 ) serves as the most authoritative guide to how we define posttraumatic stress disorder (PTSD) for mental health clinicians. Some experiences of racial trauma, such as being physically assaulted in the context of a hate crime, would qualify as trauma according to the DSM-5's initial PTSD criteria (Criterion A: “exposure to an actual or threatened death, serious injury, or sexual violence” 7 , p. 271). Other symptoms of racial trauma (eg, persistent exposure to racial microaggressions, vicarious trauma through graphic media coverage of police brutality) may not meet the aforementioned requirement, yet be experienced as traumatic. 8 In spite of this, such experiences have been included in our definition of racial trauma because previous research has shown that the prevalence and severity of PTSD symptoms do not vary as a function of whether the event met Criterion A,9,10 and such experiences are associated with symptoms above and beyond Criterion A events.11,12
Although PTSD, as described in the DSM-5, is caused by discrete events such as assault, combat, or natural disasters, research indicates that experiences of racism can have the same debilitating psychological effects on POC. As such, racial trauma can be defined as the cumulative experiences of racism throughout a person's lifetime that lead to severe mental and emotional injury. 13 Sufferers may exhibit symptoms of intrusion (eg, recurrent nightmares, upsetting thoughts), avoidance behaviors, negative changes in cognition and mood (eg, distorted blame, embarrassment, isolation, dysphoria), and alterations in arousal and reactivity (eg, self-destructive behaviors, hypervigilance, sleep issues 5 ).
How Similar is Racial Trauma to PTSD?
Carter et al 14 explored the links between symptoms of trauma and race-based traumatic stress to understand if and how reactions to negative race-based experiences are comparable to or different from symptoms associated with PTSD conceptualizations of trauma. They suggested that although the patterns of associations fluctuate slightly depending on stress level, race-based traumatic reactions and PTSD trauma symptoms are, in fact, relatively comparable to one another. They assessed their hypothesis, creating 2 groups of ‘stress’ and ‘no stress,’ based on the participants’ (n = 421) scores on the Race-Based Traumatic Stress Symptom Scale (RBTSSS 15 ). Accordingly, the ‘no stress’ group (n = 266) comprised people with no race-based traumatic stress elevations. Results of a canonical correlation analysis showed a strong relationship between race-based traumatic stress symptoms and PTSD conceptualizations of trauma (as measured by the Trauma Symptom Checklist-40 [TSC-40]).
According to the results, race-based encounters appeared to generate symptoms/injuries similar to those linked with PTSD, including dissociation, anxiety, and depression, as well as sleep disturbance and sexual dysfunctions. Furthermore, race-based traumatic reactions (as measured by the RBTSSS) such as low self-esteem, depression, and hypervigilance were most closely linked to PTSD trauma symptoms. The race-based traumatic reactions of intrusion, avoidance, physical symptoms, and anger were also linked to PTSD trauma symptoms, although the relationships were more moderate.
Further, Roberson and Carter 16 explored the link between race-based traumatic stress symptoms and traditional trauma symptoms in Black Americans. Using criterion-related profile analysis, Roberson and Carter were able to analyze the level and arrangement of race-based traumatic stress symptoms that predict trauma reactions in participants who report differing levels of race stress. Across all groups, the presence of race-based traumatic stress symptoms was a significant predictor of trauma. However, a difference was found between the No-Racial Stress and Racial Stress groups when it came to the symptom presentation that predicted trauma reactions. More specifically, in the Racial Stress group, depression, intrusion, anger, and low self-esteem were the primary drivers of the link between race-based traumatic stress symptoms and trauma reactions. Also noteworthy is the fact that hypervigilance was not linked to trauma reactions in people with racial stress. Roberson and Carter 16 concluded that distinct symptom presentations should be considered when measuring trauma caused by racial encounters.
The Posttraumatic Stress Disorder Checklist for DSM-5 (PCL-5 17 ) has items that mirror the PTSD symptoms listed in DSM-5. In investigating the latent factor structure of the PCL-5 (and by extension, the DSM-5 PTSD criteria), Gentese et al 18 found support for both a 5-factor model and the DSM-5 4-factor model. Zawadzki et al 19 used a similar scale called the Posttraumatic Diagnostic Scale for DSM-5 (PDS-5) and examined several models, based on DSM-IV, DSM-5, and other conceptualizations of PTSD. They found the best fit for a 6-factor model, which included reexperiencing, avoidance, anxious arousal, numbing, dysphoric arousal, and negative cognitions and mood.
In a similar study using the PCL-5, Grau et al 20 compared fit indices of the 4-factor PTSD model and found that a 7-factor model demonstrated the best fit. While the 4-factor model consists of Re-experiencing, Negative Alterations in Cognitions and Mood, Alterations in Arousal and Reactivity, and Avoidance, the 7-factor model consisted of the following factors: Re-experiencing, Negative Affect, Anxious Arousal, Dysphoric Arousal, Avoidance, Anhedonia, and Externalizing Behaviors. Notably, the 7-factor hybrid model was previously introduced as an alternative factor structure for the DSM-5's 4 factors as a better representation of the symptom clusters that comprise PTSD, and has been linked to increased ability to understand the relationship between PTSD symptom clusters and comorbid conditions, functional impairment, and quality of life, compared to the 4-factor model (Pietrzak et al, 2015). Additionally, the 7-factor hybrid model appears to better represent the heterogeneous nature of PTSD symptom presentation than the current 4-factor model. So, even the model of PTSD as advanced by the DSM-5 may be inadequate.
Higher Prevalence of Certain PTSD Symptoms in POC
Assessing PTSD symptoms in populations experiencing chronic multilayered stress requires accurate and nuanced assessment. Mekawi et al 21 recognized this need in their publication examining the psychometric properties of the PCL-5 in a sample consisting of urban-dwelling, trauma-exposed Black American adults. Using Item Response Theory analysis to assess item difficulty and discrimination, the findings substantiate that PCL-5 items functioned considerably differently compared to samples from previous research. 21 For item discrimination categories meeting clinically significant levels, results indicated the most “difficult” items (strongest indicators of severity) were flashbacks, inability to experience positive emotions, nightmares, strong negative beliefs, exaggerated startle response, and irritability/anger. The “least difficult” (most common) items were diminished interest, hypervigilance, cued emotional distress, difficulty sleeping, detachment, and difficulty concentrating. 21 Possible explanations regarding the low levels of difficulty in hypervigilance, sleep difficulties, and avoidance may be attributed to Black Americans experiencing these symptoms as a result of contending with the day-to-day racism that occurs when living in a racialized society; along with the pressure on Black people to overcome racism vis a vis suppressing their emotions through adherence to the Strong Black Woman schema, the “cool pose,” or John Henryism.22–24 Further, internal avoidance of trauma may be attributed to the larger pattern of historical systemic racism in the United States. 21 Overall, results emphasized the importance of flashbacks, inability to experience positive emotions, and nightmares and de-emphasized the importance of hypervigilance and sleep difficulties when assessing for clinically significant symptoms of PTSD in Black Americans and further may inform culturally relevant treatment in Black Americans. 21
The Role of Ethnic and Racial Identity
A strong, positive ethnic identity has been found to protect POC from some of the mental health harms of racism. 25 Khaylis et al 26 investigated whether an individual's ethnic identity mediates the impact of racism on the severity of PTSD symptoms in the presence of race-related stress. Assessing race-related stress, ethnic identity, and PTSD symptoms through self-report measures and conducting a simultaneous multiple regression, they found that in reaction to perceived racism, ethnic identity moderated PTSD symptoms such that a stronger ethnic identity was associated with greater PTSD symptoms in the face of rising levels of race-related stress. In addition, race-related stress was found to be an independent predictor of PTSD symptoms.
Purpose
The purpose of this paper is to increase our understanding of racial trauma and confidence in our assessment tools through a psychometric examination based on the results of a semi-structured interview and symptom checklist for assessing racial trauma. The clinical interview used is the University of Connecticut Racial Ethnic Stress and Trauma Survey (UnRESTS 5 ), administered to a national sample of diverse adults. This paper extends prior work on racial trauma by examining the correlations between the presence of racial trauma, validated racial trauma measures, and strength of ethnic identity, controlling for racialization. Unlike most prior studies, we are also able to compare trauma symptoms between those with and without racial trauma because we conducted clinical interviews of all participants. Finally, we examine the factor structure of racial trauma symptoms using the 26 items from the UnRESTS and compare these to the DSM-5 model to determine if racial trauma meaningfully differs from PTSD.
Method
Participants
There were a total of 106 interviews conducted. Five were excluded due to being duplicates (participant did interview more than once—only one interview was included) and 3 were excluded due to data loss, leaving a total of 97 UnRESTS interviews for analysis.
Of these, 44.3% were female and 53.6% male. The participants ranged in age from 19 to 67 years old (M = 33.81). About 40.2% of the participants self-identified as Black (or African, African American, or Black Caribbean), 32% as Asian (East Asian, South Asian, Asian American), 16.5% as White (or European American), 4.1% as multiracial, and 3.1% as Native American, and 4.1% as Other races. Of these, 9.3% were non-White Hispanic and 4.1% identified as White and Hispanic. The vast majority of the participants identified as heterosexual (72.2%), 5.2% as gay/lesbian, and 6.2% as bisexual.
Measures
For a DSM-5 diagnosis of PTSD, the examinee must have:
at least 1 symptom in the Re-Experiencing category, at least 1 symptom in the Avoidance category, at least 2 symptoms in the Negative Changes in Cognition & Mood category (counting only one from #9 and only one from #10), at least 2 symptoms in the Physiological Arousal & Reactivity category, at least 1 symptom from the Distress & Interference category, and the Duration of Disturbance must be a YES answer (more than 2 months).
We used the participants’ responses from the final section of the UnRESTS to determine a racial trauma “diagnosis” based largely on DSM-5 criteria. If the respondent satisfied the criteria for at least 3 of the 4 PTSD symptom clusters (A-D), the disturbance persisted for more than a month (F), and clinical significance was evident, racial trauma was determined (G). (For more details on this process, see the RTS validation paper
27
).
Statistical Analysis
For correlational analyses, a racial trauma diagnosis based on the findings of the UnRESTS served as the dependent variable, whereas the other racial and psychopathology constructs (UnRESTS ethnic identity, RTS, TSDS scores) were the independent variables. A point-biserial partial correlation was used to determine the relationship between racial trauma, PTSD, ethnic identity, and discriminatory trauma symptoms among the participants. We conducted a Fisher r-to-z comparison for dependent samples to determine which measure was a better predictor of racial trauma. 30
Furthermore, a Chi-square test was conducted to identify the group differences in PTSD symptoms between participants with and without racial trauma. Finally, we conducted an exploratory factor analysis (EFA) using the 24 main items of the UnRESTS PTSD checklist to examine the factor structure of racial trauma, to ascertain if it was more like the DSM-5 4-factor model or different.15,20 All analyses were conducted using IBM SPSS Statistics (SPSS) v. 27.
Result
Descriptive Statistics
Roughly one-third (33%) of those who took the UnRESTS were diagnosed with racial trauma (N = 32). Out of 38 Black Americans who were interviewed, 47.4% were diagnosed with racial trauma, for Asian Americans it was 22.6% out of 31, and for Hispanic Americans it was 50% out of 12.
The mean ethnic identity score on the UnRESTS was M = 8.51 (SD 2.44) for Black Americans, M = 6.52 (SD 2.98) for Asians Americans, and M = 7.77 (SD 2.09) for Hispanic Americans.
Each participant was asked to give an example of major discrimination they experienced, and they were able to give up to 2 examples. Among the 32 with a diagnosis of racial trauma, 96.9% gave 1 example and 71.9% gave 2 examples, for a total of 54 examples. Of these 54 examples, in 50% of cases the participant indicated that they feared for their “life, health, or safety.” Participants most frequently reported having a traumatic interaction with a “group of White peers or teachers” (26.9%), followed by “coworkers or bosses” (21.2%), “dating partners” (13.5%), “authority figures (eg, police, military, doctor)” (13.5%), an “stranger” (13.5%), “a store or restaurant” (7.7%), or a “friend” (5.6%). Further, respondents indicated that their traumatic experience(s) included threats (28.8%), stereotyping/xenophobia/othering (25.0%), attempting to make the person feel bad on purpose (eg, demeaning, bullying) (23.1%), being held to an unfair standard or unequal treatment (13.5%), and physical harm (eg, violence, arrest, spitting) (11.5%).
Correlates of Racial Trauma
There was a moderate, positive correlation between participants’ experience of racial trauma, as measured by RTS and racial trauma based on a clinical review of the UnRESTS which was statistically significant. Ethnic identity (as measured by the UnRESTS) was also found to be significantly positively correlated with racial trauma as measured by the RTS. These results are shown in Table 1.
Point-Biserial Partial Correlations Between Racial Trauma Diagnosis and Racial Variables, Controlling for White Race.

Abbreviations: UnRESTS, UConn Racial/Ethnic Stress & Trauma Survey; RTS, Racial Trauma Scale; MEIM-6, Multiethnic Identity Measure, 6 items.
*P < .05, **P < .01, ***P < .001, 2-tailed. N = 83.
A racial trauma diagnosis was significantly moderately correlated with the 2 self-report measures of discriminatory trauma symptoms, the RTS and TSDS. Using a Fisher r-to-z comparison to determine which measure was a better predictor of racial trauma, the difference was not significant (z = 0.132; p = .448).
PTSD and Racial Trauma
As outlined in Table 2, the Chi-square test showed that compared to people without racial trauma, for those with racial trauma, all the items of the PTSD symptoms were significantly greater, except for G5: “…negative physical reactions when reminded of racism-related experiences.” Additionally, those deemed to have clinically significant racial trauma largely met all criteria for PTSD, except for “Physiological Arousal & Reactivity,” where only 41% qualified for this PTSD criterion (two or more symptoms) based on the DSM-5, however, they were still significantly more likely to have these symptoms than those without racial trauma. Further, 28% had at least one dissociative symptom. Because of the large number of comparisons, we also applied a Bonferroni correction, and all the correlations were still significant, except for one item under Re-Experiencing (G3: Have you had the experience of feeling as if a past racism-related event was happening to you all over again…?).
PTSD Symptom Frequency for People With and Without Racial Trauma.

*P < .05, **P < .01, 2-tailed; n = 32 people diagnosed with racial trauma; n = 61 for people without racial trauma.
Factor Analytic Findings
An EFA was used to discover the underlying relationships between racial trauma symptoms on the UnRESTS. 31 We examined the factorability of the first 24 UnRESTS items, which are part of the DSM-5 symptom criteria for PTSD. Bartlett's test of sphericity was significant (χ2 (276) = 896.81, P < .001), and the Kaiser–Meyer–Olkin measure of sampling adequacy was 0.71, which was higher than the generally advised value of 0.6. Given these overall indicators, factor analysis was found to be appropriate for all 24 items.
A solution based on eigenvalues greater than one led to an 8-factor solution, with one factor having only one item. The insufficient number of primary loadings and difficulty of interpreting the 8-factor and subsequent factors in the initial analysis reporting led to examining solutions for 4, 5, 6, and 7 factors individually, using a Varimax rotation of the factor loading matrix. The 4-factor solution did not resemble the DSM-5 categories, included several cross-loadings, and had one item that failed to load at all (G3: flashbacks). The 6-factor solution, which explained 58.1% of the variance, was preferred because of its previous theoretical support and examining the scree plot. A Varimax rotation provided the best-defined factor structure. All items in this analysis had primary loadings over our cutoff of 0.45. No item had a cross-loading above 0.2 except for G5 “… negative physical reactions when reminded of racism-related experiences.” However, one loading was above the cutoff of 0.45, and the other was below it.
Table 3 provides the factor loading matrix for the 6-factor solution. Factor 1 comprised 7 items, that explained 14.15% of the variance, described as “Negative Feelings About Others.” Factor 2 comprised 5 items that explained 12.05% of the variance, described as “Disconnected.” Factor 3 comprised 4 items that explained 9.10% of the variance, described as “Self Loathing.” Factor 4 comprised 3 items that explained 8.36% of the variance, described as “Restless.” Factor 5 comprised 3 items that explained 7.92% of the variance, described as “Recollections are Distressing.” Factor 6 comprised 2 items that explained 6.52% of the variance, described as “Flashbacks.” This factor was also notably negatively correlated with being unable to remember important parts of the trauma (G8). The items associated with each factor can be seen in Table 3 in boldface.
Factor Loadings for Varimax Rotated 6-Factor Solution for 24 UnRESTS Items.

Extraction method: principal component analysis. Rotation method: Varimax with Kaiser normalization.
We examined the strength of the relationship between the factors and the total score. The correlations between factors ranged from 0.131 to 0.545, as shown in Table 4. These were also correlated to a total score, calculated by summing each factor, divided by its number of items. Each factor was highly correlated to the total.
Bivariate Correlations Between Factors.
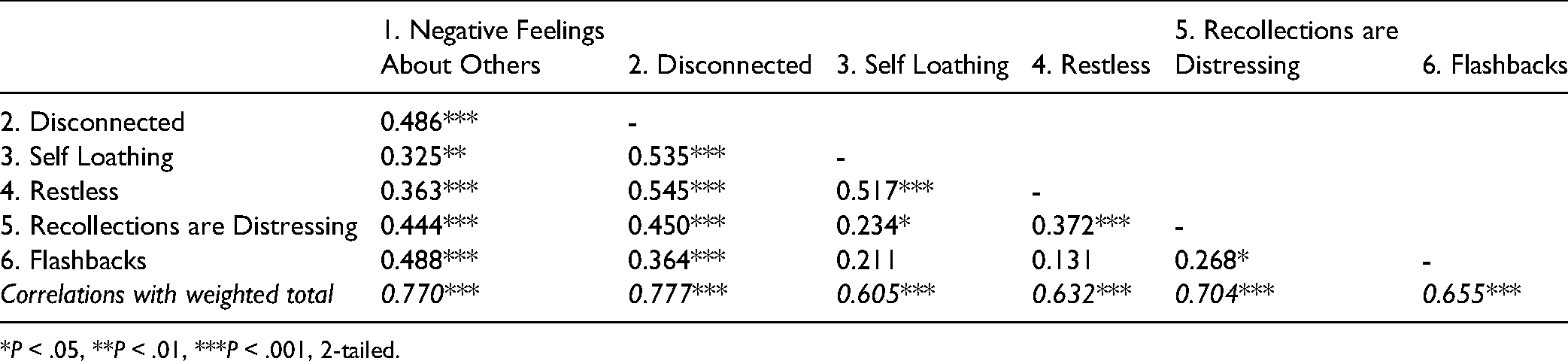
*P < .05, **P < .01, ***P < .001, 2-tailed.
Discussion
Racial Trauma by Ethnoracial Group
Using data from the UnRESTS, a clinical semi-structured interview and symptom checklist for assessing racial trauma, this study aimed to deepen our understanding of racial trauma by comparing the characteristics of those with a clinically-relevant diagnosis of racial trauma to those without. According to our results, approximately 32% of people who participated in the UnRESTS were found to have a history of racial trauma, with POC 10 times more likely to be diagnosed with racial trauma than Whites. We also observed diversity among various racial groups in terms of racial trauma diagnosis, with Black people being more likely to receive a racial trauma diagnosis than other racial/ethnic groups.
This is in line with the research that demonstrates differential levels of trauma exposure depending on racial group. For example, Lee et al 32 evaluation of the prevalence of discrimination experiences among various racial groups in the United States showed that when compared to White Americans, members of all racial marginalized groups (Black, Hispanic, and Asian) reported experiencing a higher level of racial discrimination, with Blacks reporting the highest level of all the groups that were examined. Likewise, using a nationally representative sample, Chou et al 33 found that African Americans were more likely to report experiencing racial discrimination than Asian or Hispanic Americans, who did not differ substantially from one another. This is also corroborated with Carter et al’s 14 finding, indicating that persecution based on racial characteristics is a rare cause of traumatic stress among White people. Such findings suggest considerable distress and impairment in POC due to racism.
Racial Trauma and Ethnic Identity
Correlation analysis revealed a moderately positive relationship between racial trauma and ethnic identity, suggesting that people with stronger racial identities are also more vulnerable to experiencing traumatic experiences associated with racism. It seems that higher levels of racial identity are associated with both lower levels of risk for developing psychopathology as a result of racism, 25 and at the same time, an increased likelihood of encountering racial discrimination. One possible explanation is that those who are more prone to being racially stereotyped (because of their appearance) need a more robust sense of racial identity in order to face racism. Ethnic identity development, that is, developing a sense of belonging to one's culture, is thus vital for POC, especially Black individuals.
UnRESTS Interview Compared to Racial Trauma Self-Report Measures
We also found a positive link between racial trauma diagnosis and discriminatory trauma symptoms, as measured by RTS and TSDS. This suggests that in alignment with our expectations, POC's likelihood of being diagnosed with racial trauma using the UnRESTS interview increased in proportion to the number of anxiety-related racial trauma symptoms they reported experiencing. Results highlight the value of the UnRESTS in elucidating the lived realities of those impacted by racism, and the fact that exposure to traumatic discriminatory events can have a compounding traumatic effect on POC. 5 While the RTS may be a superior tool for assessing racial trauma in general, the TSDS may be more beneficial to be used with those with intersectional identities.
Differences Between Those With and Without Racial Trauma
Our findings revealed clear and consistent differences in symptom items between people with, and without racial trauma. In particular, people who had suffered racial trauma also showed significantly higher scores on almost all PTSD symptoms than those who had not. The largest divide between the 2 groups was with regard to whether or not the difficulties they faced because of racism were upsetting to them (G23; 81.3% of people with racial trauma compared to 11.8% of people without racial trauma responded yes). In contrast, the smallest difference between those with and without racial trauma was detected in terms of “taking more risks or doing things that may harm self or others (eg, reckless driving, taking drugs, having unprotected sex),” which did not reach statistical significance and was infrequently endorsed (3.1% of people with racial trauma, compared to 1.5% of people without racial trauma). Notably, such externalizing behaviors were also found to be infrequently endorsed by those with PTSD in the Grau et al’s 20 study. In addition, trying to avoid reminders of racism-related experiences (G7a) and ongoing negative feelings such as fear, horror, anger, guilt, or shame due to racism-related experiences (G11) seemed to be the strongest predictors of clinically-significant racial trauma.
These findings are in line with the literature suggesting that racial trauma may manifest with symptoms that are distinct from those often associated with PTSD. For example, Roberson and Carter 16 found that the relationship between race-based traumatic stress symptoms and trauma reactions was predominantly driven by depression (corresponding to items G12 and G14), intrusion (corresponding to items G1, G3, G4, G6), anger (corresponding to items G15, G17), and low self-esteem (corresponding to items G9a, G10a) in those with racial stress.
Although dissociative symptoms are not necessary for a diagnosis of PTSD, we found that over a quarter of those with racial trauma had at least one symptom of dissociation related to experiences of racism, and such symptoms were very infrequent among those without racial trauma. Our results are in accordance with Polanco-Roman et al, 34 who found a positive association between racial discrimination and dissociative symptoms. Such findings suggest that POC may be more susceptible to dissociative symptoms due to their experiences of racial discrimination. In one PTSD study, dissociative symptoms emerged as the strongest correlate of functional impairment, and as such should be a focus of concern in clients. 35
Accordingly, our findings highlight the need for a more thorough understanding of racial trauma symptoms. As a result, practitioners must recognize that trauma presentation may differ in experiences of racial discrimination among POC. It is important to highlight that while some symptoms may be more indicative of challenges faced by POC in general (eg, G9c, G6), others may be more helpful in the identification of those who have undergone racial trauma (eg, G18, G13). Notably, as with any syndrome, items associated with distress and interference are the most critical (G23, G24).
Factor Analytic Findings
The factor analysis showed robust results, yielding a 6-factor solution that accounted for 58.09% of the total variance. The 6 factors were described as “Negative Feelings About Others,” “Disconnected,” “Self Loathing,” “Restless,” “Recollections are Distressing,” and “Flashbacks.”
According to our 6-factor model, we found that having negative feelings about others to be the strongest predictor of racial trauma, followed by feeling disconnected, restless, and having negative feelings about self. Comparable findings were reported by Carter et al 14 who found that trauma symptoms were most strongly linked to factors termed Hypervigilance (corresponding to factor 4, Restless), Physical Symptoms (corresponding to factor 4, Restless), Low Self-Esteem (corresponding to factor 3, Self Loathing), and Depression (corresponding to factor 2, Disconnected).
Moreover, in line with our expectation, our results from the factor analysis did not correspond to the DSM-5's 4-factor model for PTSD, not unlike the findings of previous studies such as Grau et al. 20 Our model was similar to the 7-factor structure of the RBTSSS, with the exception of a factor representing physical symptoms. 15 A possible interpretation of the discrepancy between the DSM-5's model for PTSD and our 6-factor model is that racial trauma differs fundamentally from PTSD, or it could be that the DSM-5's conceptualization of PTSD is inaccurate. Our 6-factor model, in comparison to the DSM-5's 4-factor model, allows for higher symptom cluster specificity, which may improve our understanding of racial trauma symptoms and facilitate the examination of the effect of individual factor elevations on treatment outcomes.
Limitations and Future Directions
One of the limitations of the present study was the relatively small sample size for the EFA. Additionally, the sample's racial representation was dominated by Black and Asian Americans, whereas the sample of Hispanic Americans, Asian Americans, Native Americans, and multiracial people was limited, reducing the findings’ generalizability to these racial groups. Furthermore, this investigation has been centered on experiences of POC versus White people. Because people of different races and ethnicities may face varied racial discrimination, it is important for future research to isolate the perspectives of specific racial/ethnic groups to gain a more nuanced understanding of the diversity of people's exposure to racism. Moreover, to completely comprehend the suffering experienced due to racism, future studies should account for intersecting identities such as gender, religion, and sexual orientation. Finally, future research should more closely investigate the distinctive aspects of racial trauma relative to PTSD, as well as how they may impact wellbeing of POC.
Conclusion
Self-report measures of racial trauma (RTS and the TSDS) are highly correlated to a diagnosis of racial trauma, but will not capture all sufferers, underscoring the importance of the UnRESTS. This study builds on previous racial trauma research by comparing the experiences of respondents regarding their relationships with racial constructs such as racial/ethnic identity across groups. In addition, we compared the racism-related PTSD symptoms of individuals with and without racial trauma and found that nearly all items discriminated between groups. Lastly, we evaluated the factor structure of racial trauma symptoms using 24 items from the UnRESTS PTSD symptom checklist and found important differences from the DSM-5 model. These findings add evidence to the growing literature suggesting a distinction between racial trauma and the DSM-5's conceptualization of trauma. The findings may also aid clinicians in gaining a deeper understanding of racial trauma symptomology and in developing more effective strategies for assessment and treatment of this syndrome, 36 which in turn will help reduce the public health burden of discrimination.
Footnotes
Acknowledgments
The authors thank Muna Osman, PhD, for assistance with statistical analyses.
Author Contributions
MTW conceptualized the paper, collected the data, and drafted the manuscript. MZ did the statistical analysis and also drafted the manuscript. Both authors edited the final document.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was undertaken, in part, thanks to funding from the Canada Research Chairs Program, Canadian Institutes of Health Research (CIHR) grant number 950-232127 (PI M. Williams) and the SSHRC Canada Graduate Scholarship-Masters (CGS-M; PI: M. Zare).