
Abstract
Metabotropic glutamate receptor 5 (mGluR5) dysregulation has been implicated in the pathophysiology of many psychiatric disorders, as well as nicotine use and dependence. We used positron emission tomography with [18F]FPEB to measure mGluR5 availability in vivo in 6 groups: (1) nicotine users (NUs) without other psychiatric comorbidities (n = 23); (2) comparison controls (CCs) without nicotine use or psychiatric comorbidities (n = 38); (3) major depressive disorder subjects with concurrent nicotine use (MDD-NU; n = 19); (4) MDD subjects without concurrent nicotine use (MDD-CC; n = 20); (5) posttraumatic stress disorder subjects with concurrent nicotine use (PTSD-NU; n = 17); and (6) PTSD subjects without concurrent nicotine use (PTSD-CC; n = 16). The goal of the study was to test the hypothesis that mGluR5 availability in key corticolimbic regions of interest (ROIs) is different in NU with versus without comorbid psychiatric disorders (ROI: dorsolateral prefrontal cortex [dlPFC], orbitofrontal cortex [OFC], ventromedial prefrontal cortex [vmPFC], anterior cingulate cortex [ACC], amygdala, hippocampus). We found that NU had 11%–13% lower mGluR5 availability in OFC, vmPFC, dlPFC, and ACC as compared with CC, while PTSD-NU had 9%–11% higher mGluR5 availability in OFC, dlPFC, and ACC compared with PTSD. Furthermore, relationships between mGluR5 availability and psychiatric symptoms varied as a function of psychiatric diagnosis among NUs. NU showed a negative correlation between mGluR5 and smoking cravings and urges (r's = –0.58 to –0.70, p's = 0.011 – 0.047), while PTSD-NU had the reverse relationship (r's = 0.60–0.71, p's = 0.013–0.035 in ACC, vmPFC, and dlPFC). These findings have substantial implications for our understanding of glutamate homeostasis in psychiatric subgroups and for identifying key neural phenotypes among NU. mGluR5 is a potential treatment target for precision medicine in individuals with nicotine use.
Introduction
Nicotine is among the most widely consumed psychoactive drugs in the world, and nicotine addiction is among the most common and deleterious psychiatric conditions. While predominantly consumed via cigarette smoking, nicotine may also be vaped through electronic nicotine delivery systems or consumed via sublingual and oral routes (ie, smokeless tobacco or nicotine pouches). Despite substantial reductions in nicotine consumption over the past 50 years in the United States, cigarette smoking remains the leading cause of preventable death. 1 Present estimates suggest that 1.3 billion adults regularly utilize nicotine products, and up to 50% die as a result.2,3 According to the World Health Organization, there are over 8 million tobacco-related deaths each year, including deaths from second-hand exposure. Long-term quit rates are low, and treatments have limited effectiveness in promoting abstinence. 4 Moreover, nicotine use tends to be more highly concentrated among populations with low socioeconomic status and underlying psychiatric comorbidities such as major depressive disorder (MDD), posttraumatic stress disorder (PTSD), and others. 5 Nicotine use is associated with high rates of comorbidity and may indeed contribute to the onset and severity of other serious psychiatric conditions, including MDD, PTSD, and anxiety disorders.6–10 For example, individuals with a history of smoking in adolescence have up to a 4-fold increase in risk for developing MDD symptoms in adulthood.11,12 The complex interactive relationship between nicotine use and other psychiatric disorders has been extensively documented. 13 Thus, it follows that the development and optimization of treatments for nicotine addiction will require understanding the differential effects of nicotine use on the brain in individuals with underlying psychiatric disorders. Increasing knowledge in this area will ultimately lead to more personalized treatment approaches to addiction and other commonly comorbid psychiatric disorders.
Nicotine binds to acetylcholine receptors (nAChR) throughout the body. In the brain, nicotine binding to nAChR leads to the release of multiple neurotransmitters including dopamine, glutamate, and gamma-aminobutyric acid.14,15 The effects of nicotine on dopamine neurotransmission have been investigated extensively.16,17 However, more recent research has highlighted the role of glutamate in nicotine use. 18 Glutamate is the primary excitatory neurotransmitter in the central nervous system 19 involved in critical cognitive processes including regulation of mood, 20 learning, 21 memory, 22 and sleep. 23 Dysregulation of glutamate transmission is implicated in modulating drug dependence, craving, and perpetuation of drug addiction.24–27
The metabotropic glutamate receptor 5 (mGluR5) has been specifically implicated in the pathophysiology of nicotine addiction, as it regulates glutamate neurotransmission and is widely distributed throughout the central nervous system, particularly in prefrontal and limbic areas relevant to drug use and addiction. 28 This receptor has been implicated in psychopathologies that often co-occur with nicotine addiction,29–33 and clinically relevant endophenotypes such as executive function impairment, 34 mood disorders, 35 and impulsivity. 36 Importantly, a growing body of evidence implicates mGluR5 in the pathophysiology of addiction,18,37,38 including nicotine.18,39–41 For example, preclinical studies suggest that mGluR5 regulates the reinforcing effects of nicotine by modulating dopamine release in the nucleus accumbens,42,43 and subcutaneous administration of nicotine results in reduced mGluR5 expression.44,45 Moreover, negative allosteric modulation of mGluR5 in rats has been shown to result in reduced nicotine self-administration, 46 and reduced responsiveness to nicotine. 47
Studies have examined mGluR5 availability in nicotine users (NUs) and some psychiatric disorders separately, but the interactions between the two conditions have not been fully characterized. A study by Akkus et al 25 and colleagues found 20% lower mGluR5 availability in otherwise healthy smokers relative to nonsmokers. Other studies did not show between-group differences in otherwise healthy smokers versus nonsmokers. 20 Studies in individuals with MDD have shown mixed results, with some indicating lower mGluR5 availability and others showing no differences. These discrepancies may be due in part to methodological differences (radiotracer, outcome measure selected, etc).20,48,49 Conversely, our studies in individuals with PTSD have shown higher mGluR5 availability compared with controls or individuals with MDD.32,33
Positron emission tomography (PET) with the radioligand [18F]FPEB, which binds specifically to mGluR5,50,51 provides a highly reliable, noninvasive technique to measure mGluR5 availability in vivo in people who use nicotine and have mental health disorders. Here, we utilized [18F]FPEB PET imaging to determine differences in mGluR5 availability in key neural regions of interest (ROIs) relevant to the pathophysiology of nicotine addiction 52 (dorsolateral prefrontal cortex [dlPFC], orbitofrontal cortex [OFC], ventromedial prefrontal cortex [vmPFC], anterior cingulate cortex [ACC], and amygdala, hippocampus) among NUs who had comorbid internalizing psychiatric disorders (major depressive disorder subjects with concurrent nicotine use [MDD-NU], posttraumatic stress disorder subjects with concurrent nicotine use [PTSD-NU]) compared with those who do not (NU). We hypothesized that mGluR5 availability would be different when comparing NUs with and without these disorders. We further hypothesized that mGluR5 availability among NUs would be differentially associated with relevant indicators of clinical severity (eg, measures of nicotine desire, craving, and depression) across groups (eg, NU, MDD-NU, and PTSD-NU).
Materials and Methods
Participants
Study participants were recruited from the local community. Six groups were recruited and participated in PET scanning with [18F]FPEB (Table 1): (1) healthy comparison controls (CCs) without past or present nicotine use; (2) NUs without psychiatric comorbidity; (3) individuals with MDD; (4) MDD plus nicotine use (MDD-NU); (5) posttraumatic stress disorder (PTSD); (6) individuals with PTSD plus nicotine use (PTSD-NU). The CC and NU groups were unmedicated and had no current or prior history of psychiatric illness. Participants in nonnicotine groups used nicotine products <40 times in their lifetimes. Participants ranged in age from 19 to 71 years. All participants completed physical, psychiatric, and neurological examinations at an initial screening visit to establish diagnoses and rule out any major medical or neurological illnesses. The screening included electrocardiography, complete blood counts, serum chemistries, thyroid function test, liver function test, urinalysis and urine toxicology screening, and plasma pregnancy tests (for women). Psychiatric diagnoses were confirmed using the Structured Clinical Interview for DSM-5. 53 Depressive symptoms were further assessed using the Montgomery-Åsberg Depression Rating Scale (MADRS) 54 and Beck Depression Inventory (BDI) II. 55 For NUs, the Questionnaire of Smoking Urges (QSU) was used to assess nicotine craving. The QSU is an effective measure of the desire and intention to smoke (ie, rewarding factors), as well as relief from withdrawal symptoms, 56 with higher scores on the QSU indicating stronger craving and a higher likelihood of short-term smoking. The Fagerström Test for Nicotine Dependence (FTND) was used to measure the degree of physical dependence on nicotine use. 57 Of note, data from 65 out of 73 non-nicotine using participants, and 50 out of 59 NU participants have been analyzed and published previously.20,32,33
Study participants*.

*Values are reported as mean (standard deviation) except where noted.
Abbreviations: PTSD-CC, person with PTSD who does not use nicotine; PTSD-NU, person with PTSD who currently uses nicotine; MDD-CC, person with MDD who does not use nicotine; MDD-NU, person with MDD who currently uses nicotine; CC, healthy person who does not use nicotine; NU, person without a known psychiatric diagnosis who currently uses nicotine; BDI, Beck Depression Inventory; MADRS, Montgomery-Åsberg Depression Rating Scale; FTND, Fagerström Test for Nicotine Dependence; QSU, Questionnaire of Smoking Urges; THC, tetrahydrocannabinol.
**Values are reported as mean (range).
Exclusion criteria for both MDD and PTSD groups were active suicidal ideation; mild-to-severe substance use disorder (past 6 months), or moderate-to-severe substance use disorder (past 12 months moderate, lifetime for severe) except for nicotine; positive urine toxicology or pregnancy tests at screening or before any scan; history of loss of consciousness for more than 5 min; and contraindications to magnetic resonance imaging (MRI) scans. Individuals in the MDD group could not meet the criteria for a current or historical diagnosis of PTSD. CC and NU individuals could not meet current or lifetime criteria for any DSM-5 psychiatric diagnosis except for nicotine use disorders or have a first-degree relative who met such criteria. Individuals who tested positive for substance use (including tetrahydrocannabinol [THC]) on urine toxicology screen on either scan or screen day were excluded from participation. The study was approved by the Yale University Human Investigation Committee and the Radioactive Drug Research Committee. All participants provided written informed consent.
MRI and PET Procedures
T1-weighted MRI scans were acquired for all participants on a 3T scanner (Trio, Siemens Medical Systems). This was done both to evaluate potential structural abnormalities and to facilitate co-registration with PET data. The radiotracer [18F]FPEB was synthesized onsite at the Yale PET Center (as described previously). 58 Among people who used nicotine, the timing of use was standardized to 1.5 h prior to PET scanning. High molar activity [18F]FPEB (32.19–186.85 MBq) was injected intravenously using a bolus plus infusion (B/I) paradigm with a KBol = 190 over 120 min.58,59 There were no significant differences in the injected dose or mass between groups (see Table 1). Emission data were acquired with a high-resolution research tomograph (HRRT; Siemens/CTI) during the established equilibrium period of 90–120 min after the start of injection.58,59 Head motion was tracked using the Polaris Vicra optical tracking system (Vicra, NDI System Waterloo). A 6-min transmission scan was obtained for attenuation correction. Dynamic scan data were reconstructed with corrections for attenuation, normalization, randoms, scatter, dead time, and motion using the ordered-subset expectation maximization-based MOLAR algorithm. 60 The HRRT has an intrinsic spatial resolution of ∼2.5 mm full width at half maximum. Venous sampling was conducted throughout scanning to measure the metabolite-corrected venous input function. This procedure has been validated by our research team in previous studies.20,58
Statistical Analysis
Statistical analyses were completed using SPSS Statistics v26 (IBM Corp.). Independent-samples t-tests and one-way analysis of variance (ANOVA) were used to assess differences between demographic and clinical characteristics across groups. Percent differences were computed to quantify the magnitude differences in mGluR5 availability across groups. Group differences in the relationship between psychiatric diagnostic status, NU, and mGluR5 availability were assessed using a multivariate ANOVA (MANOVA), with a diagnostic group, NU status, and the interaction of group × NU status entered as the independent variables, with mGluR5 availability in ROIs as dependent variables. Tukey's honest significant difference (HSD) posthoc comparison domain scores were performed to evaluate region-specific differences. Statistical significance for all domain scores was determined using the Benjamini-Hochberg procedure. 61 A priori power analyses confirmed a minimum of 80% power to conduct all planned analyses.
Results
To include as much of the available sample as appropriate, we did not employ a group matching procedure. Instead, demographic differences as a function of diagnostic status and nicotine use were evaluated, with variables that were observed to differ between groups adjusted for in analyses. One-way ANOVA and chi-square analyses indicated that groups (including CC and NU subgroups) did not differ significantly with respect to age, race, weight, depressive symptom severity (for the clinical groups), [18F]FPEB dosage, or other potentially relevant variables (ie, weight, intelligent quotient, and years of education; Table 1). The exception was sex, which did differ significantly across groups (Table 1). Bivariate correlations between the primary dependent variables (mGluR5 availability in the 5 study ROIs) and demographic variables were examined to evaluate their potential to confound analyses. No significant correlations were observed, and as such, no demographic variables were adjusted for in primary analyses. However, given observed group differences in sex, analyses were repeated after adjusting for sex to examine any potential effect on observed results.
mGluR5, NU, and Psychiatric Diagnosis
We conducted a MANOVA to evaluate differences in mGluR5 availability as a function of psychiatric status and their interaction. There was a significant interaction of diagnosis × NU (F12, 238 = 1.892, p = .036), indicating that the relationship between mGluR5 availability and NU differed significantly across diagnostic groups. Specifically, posthoc Tukey's HSD tests suggested the diagnosis × NU interaction effect was significant in the OFC (p = .049; did not survive correction for multiple comparisons), ACC (p = .042), and marginally significant in the dlPFC (p = .070). In participants without other psychiatric diagnoses (NU), mGluR5 availability was 11%–13% lower in the OFC, vmPFC, dlPFC, and ACC as compared with CC. In participants with PTSD, mGluR5 availability was 9%–11% higher in OFC, dlPFC, and ACC among PTSD-NU as compared with PTSD alone. Figure 1 provides a visual display of the interaction of diagnosis and NU, with each group depicted separately (PTSD and PTSD-NU in blue, MDD and MDD-NU in red, and CC and NU in green).
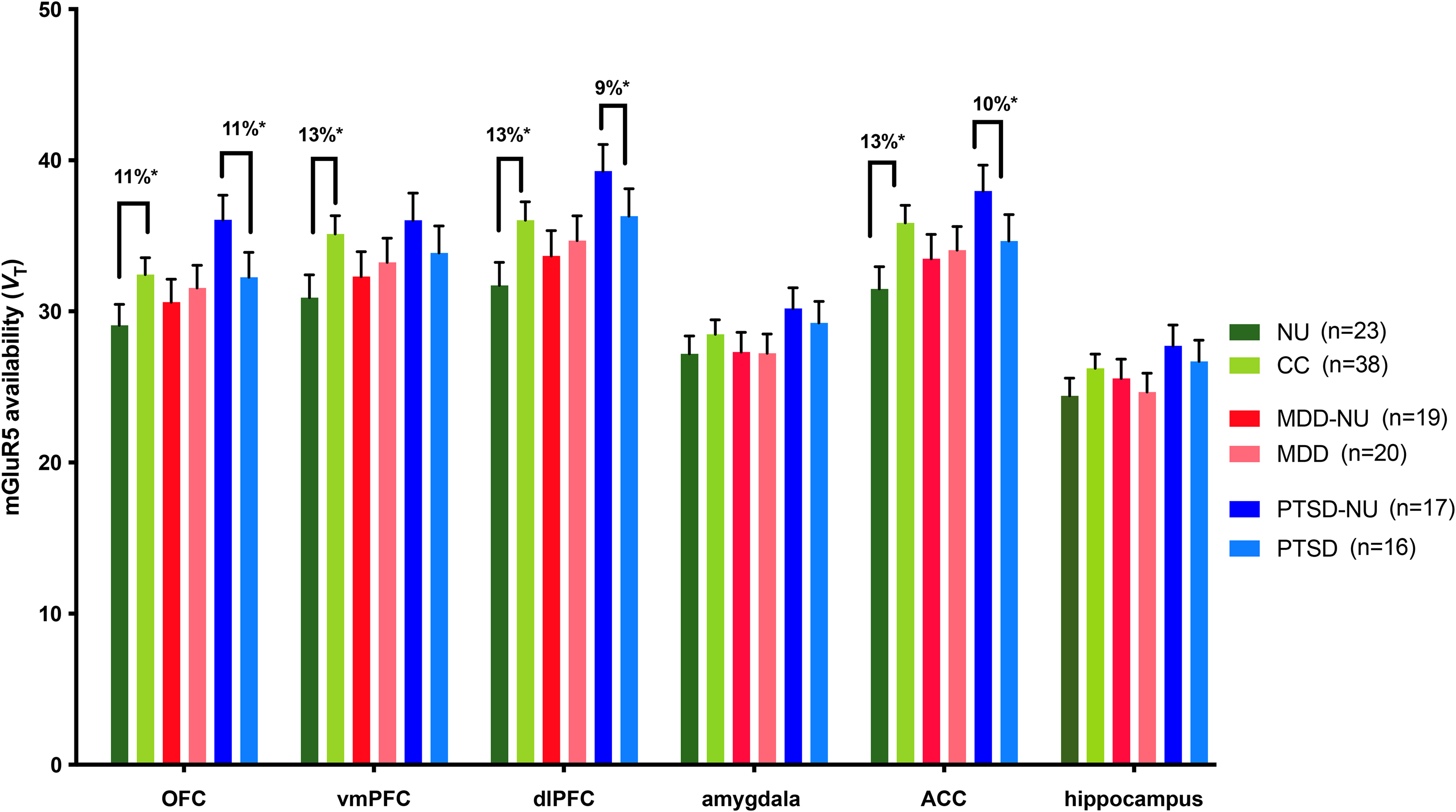
mGluR5 availability in the 5 study ROIs broken down by NUs and CC within study groups: NUs without psychiatric comorbidity, MDD, and PTSD. The data are displayed as the mean ± SEM. Percent differences are displayed above the brackets to illustrate the magnitude of significant findings.
Secondary Analyses
Secondary analyses were conducted to examine the relationships between mGluR5 availability, nicotine use, mood symptoms, and cognitive functioning both within and across psychiatric diagnostic groups and nicotine-use status. No relationships were observed between mGluR5 availability and cognitive functioning within or across diagnostic groups. With respect to mood, we observed significant negative relationships between mGluR5 availability and scan-day MADRS score in MDD-NU only (r’s = -0.58 to -0.70, p’s = 0.011-0.047 in OFC, ACC, vmPFC, amygdala, and dlPFC). No other significant relationships between mGluR5 availability and mood symptoms were observed within or across groups. With respect to nicotine use, the QSU Brief desire and relief subscale scores were differentially related to mGluR5 availability in NU and PTSD-NU. Specifically, in NU, QSU relief (r’s = -0.58 to -0.70, p’s = 0.011-0.047 in ACC, vmPFC, amygdala, and dlPFC) and desire (r = −0.60, p = .04 in vmPFC) subscale scores were negatively correlated with mGluR5 availability (Figure 2, Panels C and D). Further, total years smoked was positively correlated with mGluR5 availability in NU (amygdala r = 0.53, p = .029; hippocampus r = 0.51, p = .035) and negatively correlated with years of smoking in MDD-NU (vmPFC r = −0.58, p = .036). By contrast, in PTSD-NU, QSU relief (r’s = 0.60-0.71 p's = .013–.035 in ACC, vmPFC, and dlPFC) and desire (r = 0.61, p = .023 in OFC) subscale scores were positively correlated with mGluR5 availability (Figure 2, Panels A and B). No significant associations with years of smoking or other nicotine use-related variables were observed in other groups.

Exemplar correlations between ACC mGluR5 availability and QSU brief and relief subscale scores in PTSD NU (displayed in blue) and NU (displayed in gray).
Discussion
Summary of Main Study Finding
The key finding of this study was that mGluR5 availability in 4 corticolimbic ROIs (OFC, vmPFC, dlPFC, and ACC) varied as a function of MDD/PTSD among people who use nicotine. Specifically, NUs who did not have a diagnosis of MDD/PTSD had lower mGluR5 availability compared with CC, while the PTSD-NU group had higher mGluR5 availability compared with PTSD alone. This finding has substantial implications for our understanding of glutamate neurotransmission in various psychiatric subgroups and for identifying key neural phenotypes among NUs.
Our finding of lower mGluR5 availability among otherwise healthy NU compared with nonpsychiatric controls is consistent with prior literature.25,39 Using the radiotracer [11C]ABP688, Akkus et al 25 found that the global mGluR5 distribution volume ratio was 20.6% lower in the gray matter among cigarette smokers relative to nonsmokers. They similarly noted that former smokers who had quit smoking for a longer period of time had higher mGluR5 availability compared with more recent former smokers. This suggests that mGluR5 may normalize after a prolonged period of smoking abstinence. Overall, the collective findings of past studies coupled with the results of the current study suggest that long-term nicotine consumption via smoking may reduce mGluR5 availability, possibly through excessive glutamate release and subsequent receptor downregulation or other unknown mechanisms. This hypothesis requires more rigorous study for confirmation. However, given the cross-sectional nature of the evidence, an alternative explanation is that lower mGluR5 availability may predispose an individual to nicotine use. Nicotine has complex neuropsychiatric effects involving multiple neurotransmitter systems (ie, glutamate, dopamine, norepinephrine, serotonin, etc), 14 so the precise mechanism and clinical significance of mGluR5 downregulation in the setting of nicotine use remains unclear.
The effects of nicotine use on mGluR5 in psychiatric populations have not been previously reported. Here we show that PTSD-NU exhibits higher mGluR5 availability as compared with PTSD alone, but no difference between MDD-NU and MDD alone. Prior work in nonsmokers with PTSD found that mGluR5 availability was 20% higher as compared with healthy controls. 33 Furthermore, abnormal elevation of mGluR5 was associated with greater avoidance symptoms, suggesting a relevant clinical correlate. mGluR5 may be involved in trauma-related memories in PTSD. 28 In some preclinical models, mGluR5 antagonism blocks fear conditioning, and in higher doses might act as an anxiolytic.62,63
Stress and abnormal activation of the hypothalamic-pituitary axis (HPA) are common pathways by which the psychopathology of PTSD and nicotine addiction may intersect. 9 It has previously been proposed that upregulated mGluR5 may be related to abnormal glucocorticoid signaling in PTSD. 33 Similarly, nicotine use is also known to activate HPA and alter levels of cortisol, catecholamines, and adrenocortical tropic hormone.64,65 PTSD is associated with excessive sympathetic nervous system activity, clinically manifesting as hypervigilance and sensitivity to specific stimuli that trigger memories of traumatic events. 66 Depending on the dose, nicotine may further aggravate sympathetic symptoms or lead to anxiolysis. Prior preclinical studies have shown that nicotine may interfere with fear extinction (an important part of PTSD). 67 These effects may explain the observation of higher mGluR5 availability in smoking associated with PTSD.
Importantly, in addition to overall differences in mGluR5 availability in NU and PTSD as a function of nicotine use, we observed that associations between mGluR5 and relevant clinical symptoms varied in these groups. Specifically, NU without other psychiatric disorders showed a negative correlation between mGluR5 availability and smoking cravings and urges, while NU with PTSD had the reverse relationship. The negative relationship between mGluR5 availability and cravings/urges in NU without other psychiatric disorders suggests that changes in mGluR5 may impact immediate smoking cravings. The directionality of this relationship is unclear, though it may indicate that the high desire to smoke represents a mechanism to restore mGluR5 availability to more normal physiologic levels, given that mGluR5 is lower among NU. Alternatively, lower mGluR5 levels may be the consequence of higher nicotine dependence and more intense use. The large absolute differences in within-subject QSU scores in the PTSD group may reflect subject heterogeneity, the timing of smoking, or other unmeasurable factors related to PTSD. Given the outlier in the data, future work is needed to confirm these findings and assess clinical implications.
It is notable that PTSD-NU differed from NU without psychiatric disorders regarding the relationship between smoking cravings and mGluR5. The relationship between nicotine use and PTSD is well-established and has been previously described in a systematic review. 9 The review found that smoking rates were disproportionately high among both clinical and nonclinical populations with PTSD, ranging from 34% to 86% (well above the US national average of about 15%). The odds ratio for cigarette addiction among people with PTSD ranges between 2.04 and 4.52. The relationship may be bidirectional (ie, smoking addiction is also a risk factor for the development of PTSD). PTSD smokers have been found to have lower quit rates as compared with non-PTSD smokers, though some trials have shown comparable quit rates. Our previous work has shown that higher mGluR5 availability in PTSD is associated with worse clinical presentation, including heightened symptoms of avoidance 33 and suicidal ideation. 32 Additional work is needed to determine whether nicotine use has a direct effect on mGluR5 availability in PTSD and what impact this has on clinical symptoms.
Of note, multiple studies have demonstrated a similarly robust relationship between nicotine use and MDD, showing that nicotine dependence predicts depressive symptom experience and intensity,68,69 and that nicotine dependence is associated with slower rates of recovery in MDD. 70 Consistent with this finding, mood symptoms significantly correlated with lower mGluR5 availability in MDD-NU, but not MDD individuals. Interestingly, no overall differences in mGluR5 availability were observed in MDD as a function of nicotine use, and no relationship was observed with cravings. MGluR5 availability may have a greater impact on different components of MDD (ie, anxiety) rather than the depressed mood itself. This lack of relationship may also be due to the heterogeneous nature of MDD, making it more difficult to detect statistically significant differences. Collectively, the findings indicate that nicotine use may modulate the relationship between mGluR5 availability and mood.
Limitations
This study has some limitations. First, the cross-sectional nature of the study design precludes a determination of causality between nicotine use, PTSD, and mGluR5 availability. This was a secondary analysis of previously acquired data. Consequently, the analyses are exploratory and should be interpreted with caution. Second, circadian factors can affect mGluR5 availability.71,72 While subjects were scanned at similar times of day, we could not control for individual differences in circadian biology. Third, the modest sample size may have limited our ability to detect small differences between groups that are in fact present. However, our sample size is relatively large compared with other PET studies involving human participants. Finally, there is no neural region entirely devoid of mGluR5.73,74 Consequently, the primary outcome measure of VT, used here, includes specific and nonspecific binding. Fourth, though the results were statistically significant, the observed differences in VT are similar to [18F] FPEB test–retest values for the ROIs, 58 indicating some findings may be related to test variability.
Conclusions
In summary, this study was the first to explore the differential relationships between mGluR5 availability, mood symptoms, and smoking cravings among NUs with different psychiatric diagnoses. We found that NUs who did not carry another psychiatric diagnosis had lower mGluR5 availability compared with non-NU controls, while NUs with PTSD had higher mGluR5 availability. Furthermore, the relationships between mGluR5 availability and psychiatric symptoms varied as a function of psychiatric diagnosis among NUs. NUs without other psychiatric disorders showed a negative correlation between mGluR5 and smoking cravings and urges, while NUs with PTSD had the reverse relationship. These data suggest that mGluR5 is an important molecular target in mood disorders that is implicated differentially depending on nicotine use.
Footnotes
Acknowledgments
We thank the staff of the Yale PET Center for their assistance, and our participants for their time and effort.
Author Contributions
S.R.B. contributed to data analysis, drafting, and editing of manuscript writing. M.T.D. contributed to data collection, data analysis and interpretation, drafting, and editing of the manuscript. I.E. led data collection and study design and contributed to manuscript drafting and editing. All authors were involved in manuscript drafting and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Drug Abuse (grant no. K23DA045957 to S.R.B.), National Institute of Mental Health [K01MH092681 (I.E.), R01MH104459 and R01MH116657 (I.E.), K08 MH117351-01 (to M.T.D.), T32MH014276-47 (to R.H.A.)], Dana Foundation (to I.E.), Nancy Taylor Foundation (to I.E.), VA National Center for PTSD (to I.E. and R.H.P.), and National Institute on Alcohol Abuse and Alcoholism [K01 AA024788 (to A.T.H.)].