
Abstract
Background
Posttraumatic stress disorder is associated with impairments in sustained attention, a fundamental cognitive process important for a variety of social and occupational tasks. To date, however, the precise nature of these impairments and the posttraumatic stress disorder symptoms associated with them have not been well understood.
Methods
Using a well-characterized sample of returning United States military OEF/OIF/OND Veterans who varied in posttraumatic stress disorder symptoms, we employed a validated sustained attention paradigm designed to probe fluctuations across two attentional states characterized by prior research, including a peak state termed “in the zone” and a less efficient, more error-prone state termed “out of the zone.” Rewarded and nonrewarded conditions were employed to examine whether motivating strong task performance could ameliorate sustained attention deficits. Analyses examined associations between attentional state, availability of reward, and posttraumatic stress disorder symptoms.
Results
Results indicated that, consistent with prior findings, higher levels of posttraumatic stress disorder symptoms were broadly associated with impaired task performance. This impairment was driven largely by performance deficits during individuals' optimal (“in the zone”) attentional state, and follow-up analyses indicated that the performance deficit was primarily associated with anhedonia and emotional numbing symptoms. However, the deficit was partially ameliorated when better performance was rewarded.
Conclusion
Our results provide a more complex understanding of the sustained attention deficits associated with posttraumatic stress disorder and suggest that external incentives may help to enhance sustained attention performance for affected individuals.
Posttraumatic stress disorder (PTSD) is a chronic and debilitating psychiatric disorder that can emerge in the aftermath of exposure to traumatic events involving threatened or actual death, sexual violence, or serious injury. 1 Recent evidence suggests that impairments in attention play a central role in the clinical phenomenology of PTSD.2,3 In particular, PTSD symptoms are associated with deficits in sustained attention or the ability to maintain focused attention over prolonged periods of time.4–6 When performing tasks of sustained attention, those with elevated PTSD symptoms have shown reduced ability to resist internal 4 and external 5 distractors, screen out irrelevant information,7,8 and maintain attention to task-relevant stimuli.9–11 These impairments are particularly concerning given that sustained attention is a fundamental cognitive function that underlies many activities of daily life, from work/school activities 12 to driver safety 13 to effective social communication. 14 In addition, the ability to sustain attention may be conceptualized as a foundational neuropsychological skill, upon which a variety of higher level cognitive functions rely. 15 Finally, recent evidence suggests that attentional impairments may contribute to difficulty disengaging attention from trauma-related stimuli.2,16 In turn, this attentional bias is implicated in many of the most central symptoms to the PTSD diagnosis, identified in a recent network analysis, including intrusive thoughts and memories, persistent negative emotionality, and efforts to avoid trauma reminders. 17 Clearly, sustained attention impairments play an important role in PTSD symptoms.
Recent work also suggests that amelioration of attention-related impairments is associated with PTSD symptom reduction. One recent study employed a cognitive training program designed to reduce cognitive interference from distractors. 18 Compared with a group that did not receive the intervention, those who completed the intervention reported reductions in both interference control and PTSD reexperiencing symptoms. Similarly, two randomized controlled trials of Israeli and United States Veterans examined the effects of attention bias modification training, which aimed to shift attention away from threats, and attention control training, designed to train a balance of attention allocation between threat and neutral stimuli. 19 Both training programs reduced attention bias variability and PTSD symptoms, and an analysis combining data from the two programs found that change in attention bias variability partially mediated improvement in PTSD symptoms. These findings suggest that addressing attention-related impairment has the potential to reduce PTSD symptoms. To move toward this goal, however, a more nuanced understanding of the nature of sustained attention deficits in relation to PTSD symptoms is needed.
Recently, researchers have focused on intrinsic moment-to-moment fluctuations in sustained attention, rather than only examining overall performance during sustained attention tasks. 17 Specifically, our work and that of others20–22 have used fluctuations in response variability during sustained attention to operationalize these attentional dynamics, which has led to the observation that at least two attentional states exist that have differential behavioral and neural correlates. These include a stable, more efficient, and potentially less effortful state during which individuals are less prone to errors, termed “in the zone,” and a more variable, less efficient, error-prone, and potentially more effortful state termed “out of the zone.” 20 Operationalizing these states has allowed intraindividual fluctuations to be captured and modeled, whereas previous work had only averaged across time to characterize individual sustained attention ability. This study employed one of the primary tasks developed to parse these two states and aimed to examine the association between PTSD symptoms within and across each state to more precisely elucidate the degree to which PTSD symptoms are related to impairments in sustained attention.
Sustained attention has also been shown to fluctuate when manipulated by extrinsic motivators, such as reward, or performance-based reinforcements.23–25 As such, we examined the potential for strategic reinforcement to improve deficits in sustained attention associated with PTSD symptoms. Several recent studies of healthy participants found that rewarding performance in a sustained attention task improved overall performance and reduced reaction time variability.23–25 Using neuroimaging during sustained attention, the authors found that when performance was rewarded, participants proactively recruited and sustained task-positive neural activation. In turn, recruitment of these regions predicted improved performance, suggesting that this may be the mechanism by which external incentives enhanced performance. 2 Although these findings suggest that the availability of performance-based reinforcements can improve sustained attention and strategic allocation of neurocognitive resources, it is not yet clear whether this holds true for performance deficits associated with PTSD symptoms. A recent meta-analysis found that PTSD is characterized by deficits in multiple aspects of reward sensitivity, including “wanting” or incentive motivation, and called for increased attention to the role of reward in PTSD research. 26 In addition, manipulation of reward has been proposed as a therapeutic component of Attention Bias Modification Therapy, suggesting that reward may indeed reduce attention deficits associated with PTSD. To examine this potential further, this study compared rewarded and nonrewarded task conditions and the interactions between PTSD symptoms, attentional state, and reward condition on task performance.
In addition to more precisely investigating the nature of sustained attention deficits associated with PTSD symptoms, we examined which PTSD symptom clusters are most strongly associated with sustained attention deficits. PTSD is a highly heterogeneous disorder, encompassing a broad constellation of symptoms and a high degree of interindividual variability in symptom composition and severity. 27 As such, it is unlikely that sustained attention deficits stem broadly from the diagnosis, affecting all with the diagnosis equally regardless of symptom composition. More likely, the deficit stems from multiple clusters of symptoms, or subtypes that can be tied more directly to etiology, underlying biology, and tailored intervention strategies. For example, Bomyea et al. 18 found that cognitive training to reduce interference from distractors was associated with a reduction specifically in reexperiencing symptoms. Given these findings and the attention-interfering nature of PTSD intrusive symptoms (e.g., intrusive recollections, “flashbacks”), we hypothesized that these symptoms would be most strongly associated with task performance.
Finally, given that PTSD shares symptoms with other related conditions, we reran our primary analyses, substituting PTSD Checklist—Civilian Version (PCL-C) scores for those of the depression, anxiety, and stress subscales of the Depression, Anxiety, and Stress Scale (DASS) to evaluate the likelihood that our findings were the result of overlapping constructs. 28
Taken together, the present study had two primary aims. The first was to examine associations among PTSD symptom severity, availability of reward, and attentional state (in vs. out of zone) on performance during the gradual onset continuous performance (gradCPT) task.5,20 The second aim was to examine these same interactions in relation to each symptom cluster separately in follow-up analyses. In this way, our study aims to shed light on the precise nature of sustained attention deficits associated with PTSD, the symptom clusters most closely associated with these specific deficits and the potential role of reward in ameliorating these deficits.
Methods
Participants
Eighty participants were recruited sequentially from the Translational Research Center for Traumatic Brain Injury and Stress Disorders (TRACTS), a Rehabilitation Research and Development National Center for TBI Research at the Veterans Affairs Boston Healthcare System. All participants were Veterans who had deployed during Operations Enduring Freedom/Operation Iraqi Freedom/Operation New Dawn and were recruited for participation in the present study between October 5, 2015 and October 5, 2016. TRACTS exclusion criteria include (a) current diagnosis of schizophrenia spectrum or other psychotic disorders (not related to PTSD); (b) current active suicidal and/or homicidal ideation, intent, or plan requiring crisis intervention; (c) cognitive disorder due to general medical condition other than TBI; (d) history of neurological illness [other than traumatic brain injury (TBI)]; or (e) history of seizures. Additional details related to TRACTS protocol and methodology are reported elsewhere. 29 All research procedures were approved by the Institutional Review Board of Human Studies Research at the VA Boston Healthcare System.
Clinical Assessment
Demographics
Participant characteristics (N = 80).

Note: Three participants did not complete the DASS, leaving a sample of n = 77 for that scale; n = 80 for all other measures and demographic characteristics. PCL-C: PTSD Checklist—Civilian Version; DASS: Depression, Anxiety, and Stress Scale—21-item version.
PTSD Symptoms
Participants self-reported symptoms of PTSD over the past month using the PCL-C. 30 The PCL-C is a 17-item self-report rating scale designed to probe each of the 17 Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM-IV) 31 symptoms of PTSD related to any potentially traumatic event. The PCL-C assesses symptom clusters B (intrusions, nightmares, flashbacks, emotional, and physical reactivity), C (avoidance of thoughts/feelings, avoidance of places/activities, amnesia, loss of interest, social detachment, psychological numbing, and foreshortened future), and D (difficulty sleeping, irritability/anger outbursts, difficulty concentrating, hypervigilance, and exaggerated startle). Items are rated on a Likert-type scale ranging from 1 (not at all) to 5 (extremely). Total scores range from 17 to 85, with higher scores indicating higher levels of PTSD symptoms. Psychometric testing of the PCL has demonstrated that the measure is both valid and reliable. 32
Depression, Anxiety, and Stress
Participants reported these symptoms using the short form of the DASS. 28 The DASS is a 21-item measure that includes three 7-item subscales which capture depression (e.g., “I couldn't seem to experience any positive feeling at all”), anxiety (e.g., “I felt I was close to panic”), and stress (e.g., “I found it hard to wind down”) symptoms. Each item describes a relevant symptom, and participants are asked to rate the extent to which they have experienced the symptom on a 0 (Did not apply to me at all) to 3 (Applied to me very much, or most of the time) scale. Respondents are asked to report on their experiences of these symptoms in the past week. Total scores range from 0 to 63, with higher scores indicating more severe symptoms. Research has demonstrated that the DASS-21 distinguishes well between depression, physiological arousal, and stress symptoms. 33 In addition, the DASS-21 has demonstrated adequate reliability and validity across clinical and community samples.33,34
Sustained Attention Paradigm
Sustained attention was probed using the gradual onset Continuous Performance Task (gradCPT; see Figure 1 for task schematic).
20
In the gradCPT task, participants are presented with a series of gray-scale images, each of which is either a city scene (90%) or a mountain scene (10%). The images transition gradually from one to the next with no interstimulus interval. Participants respond to the city images by pressing the space bar and withhold response to the mountain images. The images transition every ∼800 ms, requiring participants to quickly identify the scene and make or withhold their response accordingly. The gradCPT task is well suited to capture sustained attention due to the gradual transitions between images; these gradual transitions avoid the abrupt stimulus onsets which serve to recapture attention with each transition in other continuous performance tasks (e.g., the sustained attention to response task
35
).
gradCPT Task Schematic. Participants are presented with a series of gray-scale images, each of which is either a city scene (90%) or a mountain scene (10%). Participants are asked to respond to the city images by pressing the space bar and make no response to the mountain images. Images transition gradually from one to the next every 800 ms with no interstimulus interval, requiring participants to quickly identify the scene and make or withhold their response accordingly.
Participants completed a total of eight 1-minute task “blocks,” comprised of four fixed-order blocks that were each presented with and without available rewards, such that there were 4 minutes of each reward condition. Order of blocks was randomized while maintaining alternation of rewarded and unrewarded blocks. Availability of rewards for performance was signaled by the color bordering the scenes (green vs. blue). 24 Prior to the task, participants were told that a performance-based reward would be calculated for each of the four rewarded blocks; plus or minus $0.01 for correct and incorrect presses to cities, respectively, and plus or minus $0.10 for correct and incorrect nonpresses to mountains, respectively. Participants were advised that the minimum bonus award was $0.00, the maximum award was approximately $8.00, and that the task was coded so that simply pressing or failing to press to 100% of the trials would lead to a bonus of $0.00. After these instructions were given and understood, a 30-s practice was completed, and a hypothetical bonus amount was displayed on screen at its conclusion. At the end of the experimental task, all participants received $8.00 as their performance bonus.
Overall performance accuracy, or sensitivity to discriminating cities and mountains, operationalized here as d′, was computed using a signal detection approach to hits (correct omissions to mountains) and false alarms (incorrect omissions to cities). 36 This accuracy measure is thought to best reflect sustained attention ability and was the focus of the current study. 36 We used standard procedures to correct for cases in which hit rates were 100% or false alarm rates were 0%, with one-half error deducted or added on the basis of the number of target or nontarget trials presented, respectively. No participants had 0% false alarm rate (no omission errors) for “Go” trials (city scenes). Only five participants (6.25%) had 100% hit rate (no commission errors) for “No Go” trials (mountain scenes).
In-the-zone and out-of-the-zone periods were calculated based on the within-subject variance time course (VTC) of each trial, or the absolute deviation of the trial's RT from the mean run reaction time (RT). A smoothed VTC was calculated to integrate information from the surrounding 20 trials (∼16 s), via a weighted average, using a Gaussian kernel of nine trials (∼7 s). Performance was then divided into low- or high-variability epochs (i.e., in the zone and out of the zone), based on a median split on the smoothed VTC for each run. Importantly, in- and out of the zone epochs were calculated within subjects using a median split approach conducted on each individual participant's data. In this way, each participant's states were defined relative to his or her own performance and were in/out of the zone 50% of the time, reflecting the participant's best and worst periods of RT stability. This is consistent with our previous definition of these states.20,36,40 In- and out-of-the-zone epochs were calculated for each reward condition separately. Additional details on the calculation of zones can be found in previous publications. 24
Analysis Strategy
Analyses were conducted using a linear mixed effects (LME) model strategy with R software (v. 3.3.1; lme4 package) to examine main effects (Model 1) and interactions (Model 2) between PTSD symptoms (i.e., total PCL score, entered as a continuous variable), attentional state (in vs. out of zone; see Esterman et al.20,24 for performance-based calculation of attentional states), and availability of reward (reward, no reward) on overall task performance (d′). Follow-up analyses were conducted using an identical strategy, replacing total PCL scores with scores calculated within symptom clusters using corresponding items of the PCL (reexperiencing, avoidance/numbing, hyper-arousal). Finally, control analyses were conducted also using the identical linear mixed model, replacing PCL scores with each of the three subscales of the DASS (Depression, Anxiety, and Stress).
Results
Participant characteristics are summarized in Table 1.
Aim 1: PTSD Symptoms, Attention, and Reward
Model 1
In our initial model, we included only main effects of reward, zone, and PCL scores. The main effect of reward was significant, t(79) = 6.06, p<.001, reflecting improved task performance in the reward compared with the no-reward condition. The main effect of zone was also significant, t(79) = 13.20, p<.001, reflecting improved task performance during in-the-zone state compared with out-of-the-zone state. A significant main effect of PTSD symptoms also emerged, t(78) = 2.06, p = .04, reflecting improved task performance with fewer PTSD symptoms.
Model 2: Interactions With PTSD Symptoms
In this model, all interaction terms were included. A significant Zone × PTSD symptoms interaction emerged, t(101.25) = 2.15, p = .03, reflecting a stronger association between PTSD symptoms and poor performance in in-the-zone state compared with out-of-the-zone state. In other words, PTSD symptoms appeared to have a more deleterious effect on in-the-zone compared with out-of-the-zone performance. The Reward × PTSD symptoms interaction was not significant, t(101.46) = 1.57, p = .12.
A significant three-way (Reward × Zone × PTSD symptoms) interaction also emerged, t(78) = 2.04, p = .04. To interpret this interaction, follow-up analyses were conducted to examine Reward × PTSD symptoms interaction within each zone separately. During in-the-zone attentional state, a significant Reward × PTSD symptoms interaction emerged, F(1,78) = 4.27, p = .04. This interaction reflected a weaker negative association between PTSD symptoms and performance in the reward compared with the nonreward condition. Importantly, this finding suggests that reward may ameliorate or reduce the burden of PTSD symptoms on in-the-zone performance (see Figure 2(a); median split of PCL for illustrative purposes). During performance that was out of the zone, the Reward × PTSD symptoms interaction was not significant, F(1,78) = 0.39, p = .54, suggesting that in this attentional state, the relationship between PTSD symptoms and performance was similar with and without reward (see Figure 2b).
Effects of PTSD symptoms, attentional state (zone), and reward on gradCPT task performance. (a) During in-the-zone task performance, the negative association between PTSD symptoms and task performance was reduced when task performance was rewarded (significant Reward × PTSD symptoms interaction in the zone epochs, p < 0.05). (b) This effect was not observed during out of the zone epochs, during which the relationship between PTSD symptoms and performance was similar across reward conditions (interaction not significant, p > 0.5). Note that PCL-C scores were split into high and low groups using a median split approach for clarity of visual presentation (low group M = 31.75, SD = 7.63; high group M = 58.73, SD = 10.16), though scores were entered into the LME analysis as a continuous variable. Error bars reflect the standard error of the mean.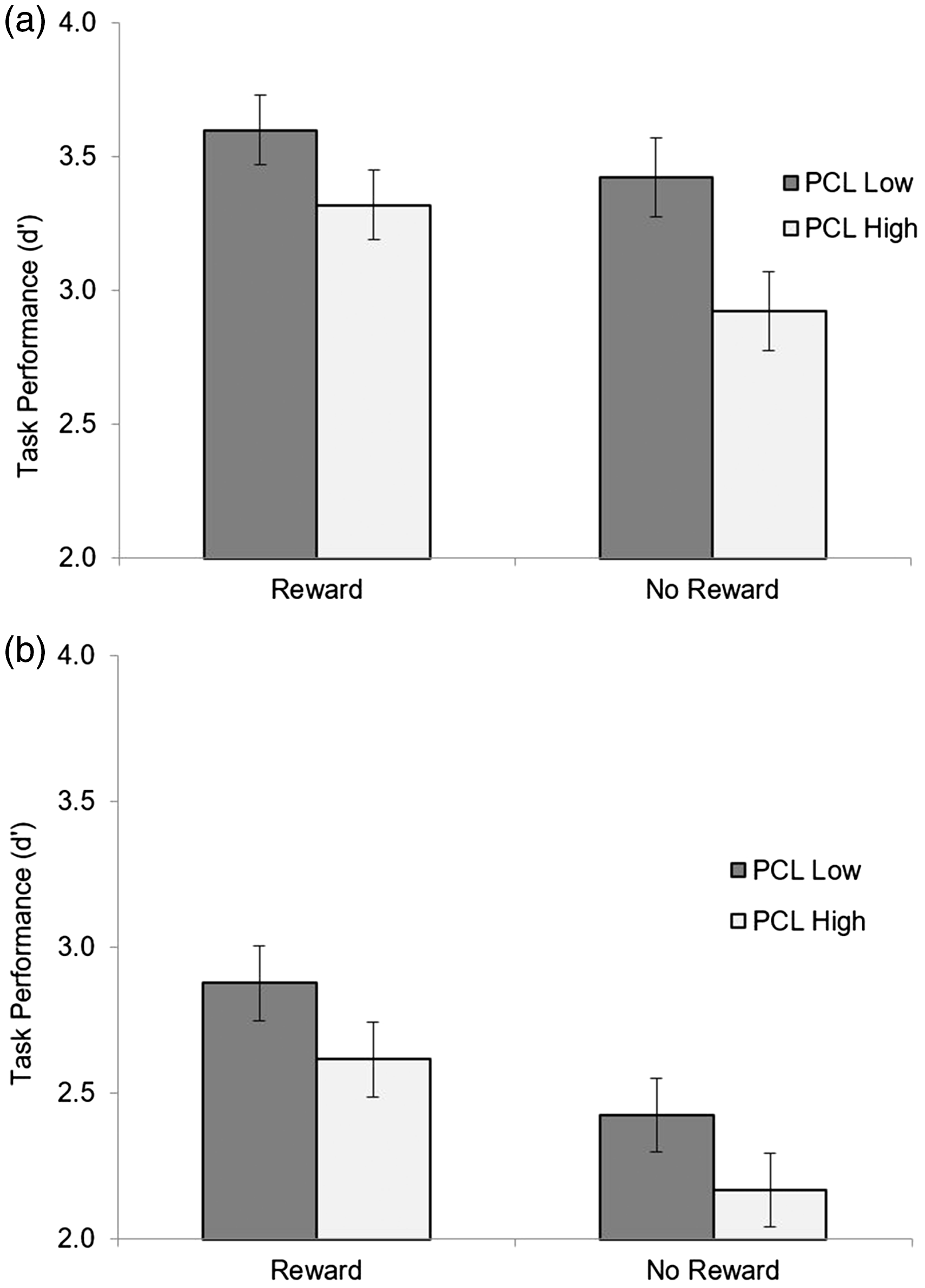
To further determine the robustness of these results, we conducted a similar analysis using an analysis of covariance model rather than an LME model (Supplementary Analysis No. 1). Furthermore, we considered dichotomous rather than continuous PCL measures (Supplementary Analysis No. 2), as well as adding TBI status as an additional predictor (Supplementary Analysis No. 3). Overall, these alternative models replicated the above pattern of results.
Aim 2: Parsing Results by PTSD Symptom Clusters
To examine the degree to which specific PTSD symptom cluster(s) may be primarily associated with gradCPT performance, we conducted the same linear mixed model described previously (Model 2), separately for each of the three DSM-IV PTSD symptom clusters, including (1) reexperiencing (Cluster B), (2) avoidance and numbing (Cluster C), and (3) hyperarousal (Cluster D).
For reexperiencing symptoms, the main effect on task performance was marginally significant, t(78) = 1.97, p = 0.05. A significant Zone × Reexperiencing symptoms interaction emerged, t(100.3) = −2.00, p = .048, reflecting a stronger association between reexperiencing symptoms and poor performance during in-the-zone compared with out-of-the-zone periods. Neither the Reward × Reexperiencing symptoms, t(101.2) = 1.27, p = .21, nor the three-way Reward × Zone × Reexperiencing symptoms interaction, t(78) = 1.56, p = .12, was significant. Taken together, these results suggest that although PTSD reexperiencing symptoms only marginally predicted task performance overall, these symptoms were more negatively associated with in-the-zone performance compared with out-of-the-zone performance. However, unlike the findings for overall PTSD symptoms, the reward condition was not associated with a reduction in the strength of the relationship between reexperiencing and in-the-zone task performance.
PTSD avoidance and numbing symptoms did have a main effect on task performance, t(78) = 2.07, p = 0.04, with higher levels of symptoms associated with poorer performance. The Zone × Avoidance and Numbing symptoms interaction was significant, t(101.7) = 2.32, p = .02. Consistent with the findings observed for all PTSD symptoms, this interaction reflected a stronger negative association between avoidance and numbing symptoms and performance during in-the-zone compared with out-of-the-zone periods. The Reward × Avoidance and Numbing symptoms interaction was not significant, t(101.6) = 1.72, p = .09, suggesting that the availability of reward may not have influenced the relationship between avoidance and numbing symptoms and task performance. The three-way Reward × Zone × Avoidance and Numbing symptoms interaction was significant, t(78) = 2.34, p = .02. To interpret this interaction, we conducted follow-up analyses to examine Reward × PTSD symptoms interaction separately within each zone. Within the in-the-zone attentional state, there was a significant Reward × Avoidance and Numbing symptoms interaction, F(1,78) = 6.39, p = .01, reflecting a significant positive association between avoidance and numbing symptoms and task performance in the reward compared with the no-reward condition. Consistent with the pattern of findings observed for PTSD symptoms overall, this suggests that the negative association between avoidance and numbing symptoms and in-the-zone performance may be reduced when performance is incentivized by an external reward. Also, consistent with the pattern of findings for PTSD overall, the Reward × Avoidance and Numbing symptoms interaction was not significant for out-of-the-zone performance, F(1,78) = 0.32, p = .58. Taken together, these findings suggest that avoidance and numbing symptoms were most impairing in-the-zone, but that reward also had the most ameliorative effect on performance in this attentional state, particularly for the individuals with higher levels of symptoms. These findings are also consistent with the pattern of results observed using the full PCL scores and suggest that the avoidance and numbing symptom cluster may be driving much of this pattern.
The main effect of Hyperarousal symptoms on task performance was not significant, t(78) = 1.66, p = 0.10. Neither the Zone × Hyperarousal symptoms, t(101) = 1.57, p = .12, nor the Reward × Hyperarousal symptoms interaction [t(101.2) = 1.30, p = .20] were significant. The three-way interaction (Reward × Zone × Hyperarousal symptoms) was not significant, t(101.2) = 1.3, p = .20. These findings suggest that hyperarousal symptoms alone did not play a significant role in performance on the gradCPT task, that the relationship between hyperarousal and task performance does not vary across attentional states, and that availability of reward is not associated with significant alternation of this pattern.
Control Analyses: Depression, Anxiety, and Stress
In our sample, scores on all three DASS subscales ranged from Normal to Extremely Severe (Depression range: 0–38, Anxiety range: 0–30, and Stress range: 0–30). Mean scores for the depression and anxiety subscales fell in the mild range, while the mean score for the stress subscale fell in the moderate range. Mean scores for all three subscales are reported in Table 1. We conducted three additional LME models examining associations between task performance and Depression, Anxiety, and Stress as measured by the three subscales of the DASS. No main effects of or interactions with DASS Depression (ps > 0.5), DASS Anxiety (ps > 0.6), or DASS Stress (ps > 0.2) were significant.
Discussion
Our findings suggest that PTSD symptoms, particularly avoidance/numbing and reexperiencing symptoms, are associated with sustained attention impairments that are strongest when participants are in-the-zone. However, incentivizing performance with reward improves in-the-zone performance, partially ameliorating the deficit associated with PTSD symptom severity. This finding sheds new light on the nature of attention deficits associated with PTSD symptoms and provides a novel and precise target for the development of interventions.
Our results replicate prior findings demonstrating an association between trauma-related symptoms and performance in a sustained attention task. 4 DeGutis et al. utilized the gradCPT task and focused on one specific aspect of sustained attention, inhibitory control (i.e., commission errors). Findings indicated impaired inhibitory control as demonstrated by commission errors on the gradCPT and a task assessing distractor suppression5,37 but no associations between PTSD symptoms and a variety of other measures of executive functioning. These results are also consistent with those from prior work using other measures of sustained attention and inhibitory control among individuals with PTSD symptoms.5–7,9
Our findings also suggest that the sustained attention impairment associated with PTSD symptoms is most pronounced during the optimal attentional state (i.e., in-the-zone) and in the absence of external reward. This attentional state is associated with neural activity in the default mode network and has been conceptualized as a more automatic or more efficient state that is associated with successful task performance. 20 This finding of impairment specifically in the optimal performance state dovetails with previous findings that PTSD symptoms are associated with reduced processing speed and decrements in or misallocation of cognitive resources.6,38,39 It may be that in lower motivation contexts, individuals with greater PTSD symptoms are not able to effectively utilize cognitive resources that would allow for efficient and accurate sustained attention performance. This finding also raises the question of whether, to achieve adequate performance on tasks requiring sustained attention, those with PTSD symptoms may spend more time in the higher effort, less efficient state, thereby depleting cognitive resources more quickly.
Alternatively, this finding may be related to difficulties regulating regions of the default mode network, areas engaged more strongly during in-the-zone performance,5,21,23,25,40 consistent with recent neuroimaging work.40,41 These recent studies have found that those with PTSD demonstrate less flexibility in shifting between default mode and executive control networks with increasing cognitive demand. In particular, Aupperle et al.41 found that during cognitive tasks with relatively low cognitive demand, those with PTSD demonstrated limited ability to disengage default mode regions. Consistent with this finding, those with higher levels of PTSD symptoms may have struggled to maximize the stability and efficiency of their in-the-zone, lower cognitively demanding periods due to limited capacity to flexibly recruit and disengage regions of the default mode network as needed.
Finally, our findings suggest that providing an incentive for improved performance partially ameliorates the deficit in in-the-zone sustained attention associated with PTSD symptoms. This was especially true for attention deficits related to reexperiencing and avoidance/numbing symptoms. This suggests that incentive motivation may influence the degree of and potentially account for some aspects of these attentional deficits. If this is the case, attention training programs incorporating rewards could be particularly effective for those with PTSD symptoms. To test this, future studies may wish to examine incentive-based manipulations as adjuncts to existing attention training protocols. 4 Given recent evidence for the role of attention impairments in the maintenance of PTSD over time, 2 such interventions may not only improve attention but could potentially have additional downstream therapeutic effects. For example, improving sustained attention among those with PTSD may also reduce hypervigilance by allowing individuals to more easily disengage attention from trauma-related stimuli.
The out-of-the-zone attentional state was found to be less sensitive to PTSD symptoms and less modulated by the presence of reward. This finding is consistent with the interpretation that PTSD is characterized primarily by deficits in “peak performance” on sustained attention tasks. It also may be that these less efficient, suboptimal attentional states are more ubiquitous and/or have multiple contributors unrelated to PTSD.
Taken together, the results of this investigation suggest that sustained attention deficits associated with PTSD most strongly stem from impairments in attaining the optimal, stable, and high-performance state (in-the-zone), and that this deficit may be partially ameliorated by incorporating incentives for high performance. Future research may wish to build on this finding in several ways. First, replication in a larger sample size and in a non-Veteran sample with PTSD symptoms would be helpful to ensure that these findings generalize to the broader population of individuals with PTSD symptoms. Second, given the specific deficit associated with in-the-zone performance, it may be important to identify or develop attentional training programs that specifically target improvements in this attentional state for individuals with PTSD. Finally, future research should test the use of incentives to enhance outcomes in such training protocols and examine to what extent any such benefits persist over time.
Our results should be interpreted in light of several caveats. First, the present study was predominantly comprised of relatively young male Veterans. As such, the extent to which the findings would generalize to all adults with PTSD symptoms is unclear. In addition, participants in this study did not undergo neuroimaging while performing this task, and as such the correspondence between attentional states and their previously identified neural underpinnings 20 cannot be verified; however, a recent fMRI study of sustained attention in this same Veteran population largely replicates findings in civilian studies. 40 Third, findings within symptom clusters should be interpreted with caution given the exploratory nature of these analyses. Future research would benefit from larger sample sizes and careful correction for multiple comparisons. Fourth, it will be important for future research to determine the replicability of these results given the marginal nature of the effects. Finally, PTSD symptoms were assessed using the DSM-IV version of the PCL. Although research has demonstrated that most individuals who meet criteria for DSM-IV PTSD also meet criteria for PTSD as defined by DSM-5, 42 it cannot be determined with certainty that the findings described herein would replicate using DSM-5 PTSD diagnostic criteria. Nonetheless, this investigation contributes to our understanding of sustained attention deficits associated with PTSD and the potential for reward to ameliorate them.
Supplemental Material
Supplemental material for Reward Ameliorates Posttraumatic Stress Disorder-Related Impairment in Sustained Attention
Supplemental Material for Reward Ameliorates Posttraumatic Stress Disorder-Related Impairment in Sustained Attention by Sunny J. Dutra, Brian P. Marx, Regina McGlinchey, Joseph DeGutis and Michael Esterman in Chronic Stress
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the US Department of Veterans Affairs through the Translational Research Center for TBI and Stress Disorders (B9254-C), a VA Rehabilitation Research & Development Traumatic Brain Injury National Research Center, and Merit Review Award and Career Development Award from the Department of Veterans Affairs Clinical Sciences Research and Development Service (I01CX001653; IK2CX000706-01A2) to M. S. E. A National Institute of Mental Health postdoctoral training grant (5T32MH01983618) supported the fellowship of S. D.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.