
Abstract
Background
Prior research has indicated that posttraumatic growth (PTG) often co-occurs with symptoms of posttraumatic stress disorder (PTSD). However, it is yet unclear what longitudinal patterns of posttraumatic symptom levels may predict the development of PTG.
Methods
World Trade Center (WTC) rescue and recovery workers (2038 police and 2103 non-traditional responders) were assessed an average of 3, 6, 8, and 12 years post-9/11/2001. Responders’ WTC-related PTSD symptoms were characterized by No/Low Symptom, Worsening/Subtly Worsening, Steeply Worsening (only for non-traditional responders), Improving, and Chronic trajectories. PTSD symptom trajectories were examined as predictors of PTG, which was assessed using total scores on the Posttraumatic Growth Inventory-Short Form.
Results
Across both occupational groups, being female, older, Hispanic, and experiencing more post-9/11 traumatic events were independently associated with self-reported PTG. Among police responders, a greater number of WTC exposures and supportive family members while working at the WTC site were linked to higher PTG. Among non-traditional responders, Black race/ethnicity, less education, fewer pre-9/11 traumatic events, and the presence of support while working at the WTC site were additionally linked to higher PTG. Only the moderate PTSD symptom trajectories (ie, worsening and improving) for police responders and all symptomatic trajectories for non-traditional responders were associated with higher levels of PTG.
Conclusions
Symptomatic 12-year trajectories of PTSD symptoms and certain sociodemographic characteristics, stressor exposures, and supportive resources were associated with PTG in traditional and non-traditional WTC responders. Results provide insight into subgroups of WTC responders who may benefit from PTG-promoting interventions, as well as potentially modifiable targets to help foster PTG in this population.
Introduction
Since being formulated two decades ago, the concept of posttraumatic growth (PTG) has expanded our understanding of what is considered a “typical” reaction following a potentially traumatic event. 1 PTG occurs when survivors of a traumatic event experience perceive personal benefits while attempting to cope with the trauma and its aftermath. 1 Manifestations of these posttraumatic benefits include greater appreciation for life, more meaningful interpersonal relationships, enhanced spiritual beliefs, a new-found purpose in life, and an increased sense of personal strength. 2 The experience of PTG has been replicated across cultures, developmental periods, and types of traumatic events. However, a consensus has not yet been reached regarding the relationship between PTG and distress following a traumatic event. The Tedeschi and Calhoun model of PTG proposes that if a traumatic experience is severe enough to shift an individual's worldview, it may be significant enough to shift their self-identity. 1 Therefore, exposure to traumatic events has the potential to generate simultaneously meaning-making cognitions, growth-oriented behaviors, and high levels of distress. 3 This study aims to understand the relationship between distress and self-reported growth by examining how posttraumatic stress disorder (PTSD) symptom trajectories across four time-points predict PTG in a sample of over 4000 World Trade Center (WTC) rescue and recovery workers followed prospectively for over a decade after the 9/11 WTC attacks.
The Relationship Between PTSD and PTG
While PTSD and PTG may appear diametrically opposed, research suggests that individuals can experience both simultaneously. 4 Extensive cross-sectional studies across diverse populations have found conflicting results regarding the nature of the relationship between these outcomes. Some suggest that PTSD is positively correlated with PTG (eg, Solomon and Dekel 5 ), while others have found no association 6 or even negative correlations (eg, Kimhi et al 7 ). Longitudinal analyses illustrate a dynamic relationship between these outcomes, with initial levels of higher PTG predicting lower levels of PTSD at succeeding time points and lower subsequent PTSD symptoms levels following new traumatic events.8–10 Other longitudinal studies have found a reciprocal relationship between PTG and symptoms of PTSD, indicating that PTG may not consistently act as a protective factor against the development of subsequent PTSD symptoms.11–13 As these mixed results suggest, the field currently lacks a cohesive model to encompass the concurrent nature of PTG and PTSD. These inconsistencies may result from differences in sampled populations (eg, military service members vs cancer survivors vs survivors of serious accidents), as well as variability in the associated types of traumatic events to which participants were exposed. Epidemiologic surveys indicate that the average duration of PTSD symptoms is approximately six years. 14 However, most prior longitudinal studies of PTG utilized measures of PTSD symptoms spanning a year or less, limiting our understanding of the influence of chronic PTSD symptom trajectories on the experience of PTG.
Current research indicates that psychological distress following trauma may be necessary to initiate the cognitive processes that may help facilitate PTG.2, 3 Although limited by insufficient evidence from longitudinal studies to date, the current model posits that for PTG to develop, a traumatic event must be severe enough to challenge one's worldview and self-conception and cause subsequent rumination. 15 The rumination occurs to resolve the cognitive dissonance between pre- and post-trauma outlooks. These include intrusive ruminations as a component of PTSD and deliberate or meaning-making cognitions about the trauma leading to PTG. 15 Current literature points to a curvilinear relationship or inverted U-curve model, with moderate PTSD symptoms being a stronger predictor of PTG than low or severe PTSD symptoms.16–21 Prior work indicates that those who have never developed psychopathology or distress following trauma may not be cognitively prompted to engage in meaning-making or reframing that can lead to growth. Additionally, those who experience very severe intrusive cognitions about the trauma may be too distressed to engage in the deliberate reframing necessary to grow one's identity or representation of the trauma.22,23 In a sample of US veterans who have PTSD, veterans who endorsed PTG reported better mental functioning and general health than those who did not endorse PTG, supporting the potential clinical utility of PTG. 17
PTG in Populations Exposed to the 9/11 Attacks on the World Trade Center
Several cross-sectional studies have examined the relationship between PTG and PTSD in populations exposed to the WTC attacks. In a representative sample of 1004 adults from across the United States six weeks after September 11th, 2001, PTG following the attacks was positively correlated with psychological distress, including PTSD symptoms, and higher levels of exposure to the 9/11 attacks. However, PTG was also associated with greater adaptive coping strategies and higher functioning. 24 This association again emphasizes the possibility of experiencing simultaneous growth and distress. In an international sample of 1505 adults assessed an average of nine weeks after 9/11, initial levels of PTG were associated with higher levels of trauma-related symptoms. Six and a half months after 9/11, a follow-up assessment established that those who reported decreased trauma symptoms had higher levels of PTG. 16 A curvilinear relationship was observed within this sample nine weeks after 9/11, as those who reported intermediate levels of trauma symptoms also developed the highest amount of growth. First responders are particularly vulnerable to developing PTSD because of their likelihood of exposure to multiple traumatic experiences. Prior work has shown in at least two samples of police officers that higher PTSD symptoms were related to higher levels of PTG.3, 25 To our knowledge, no other studies have yet examined PTG in a population of WTC rescue and recovery workers, nor have they examined the relationship between PTSD and PTG using a longitudinal approach for the length of time or with a sample size larger than ours.
The Present Study
We aimed to determine how differing PTSD symptom trajectories predict PTG for both non-traditional (eg, construction workers) and police WTC responders. These occupational groups were assessed separately due to significant differences in pre-disaster training and demographic variables, and because the latent growth mixture modeling-derived PTSD symptom trajectories differed by occupational group. 26 While previous longitudinal work has focused on the association between PTSD symptoms and PTG within shorter timespans of one to two years, this study aims to advance the field's understanding of the relationship between PTG and PTSD symptom trajectories, which were assessed across four time-points over an average of twelve years following a shared traumatic event experienced by the entire sample. This study also provides a unique contribution to the literature by examining the relationship between PTSD symptom trajectories and PTG in a sample of participants who were all exposed to the same index traumatic event, which may help to explain some of the mixed results in prior studies of PTSD and PTG. The present study was conducted with two primary aims: (1) to determine the level of self-reported growth in each of the occupational groups and the relationship between growth and PTSD risk and protective factors, and (2) to examine whether longitudinal PTSD symptom trajectories predict growth, controlling for additional risk and protective factors. Based on the curvilinear model of the relationship between PTSD and PTG,16–18 we hypothesized that responders with moderate symptom trajectories (ie, Worsening and Improving trajectories) would report higher PTG levels, and that responders with severe symptom trajectories (ie, Steeply Worsening and Chronic trajectories) would report lower PTG levels relative to WTC responders with a No/Low-PTSD symptom trajectory.
Materials and Methods
Participants
All participants were recruited from the WTC Health Program (WTC-HP). The WTC-HP, a regional clinical consortium of five medical institutions located throughout the greater New York City (NYC) area, was established by the Centers of Disease Control and Prevention in 2002 to provide health monitoring and treatment specifically to WTC responders. For the present study, participants were sampled from the cohort of 10 835 WTC responders who had attended at least three WTC-HP periodic health monitoring visits across the five consortium clinics over eight years following 9/11/01 (see Pietrzak et al 27 for details). Sixty one percent of these responders had consented to be contacted for future studies and were invited to complete a web-based survey between June 2012 and December 2014 regardless of their previously reported symptom levels. Participants who did not have access to the internet were given the option of completing a paper-and-pencil version via mail. In total, 4487 (67.6%) of these WTC responders participated in the survey and were eligible for this analytic sample (3461 [77.1%] participated online, and 1026 [22.9%] completed the paper-and-pencil version; 4261 [95.0%] in English and 226 [5.0%] in Spanish). Two hundred and sixty-five participants were excluded from this analytical sample because of incomplete survey responses, resulting in an N of 4222 in the analytic sample. Survey completers included 2038 police and 2184 non-traditional responders (see Feder et al 26 for details). The investigation was carried out under the latest version of the Declaration of Helsinki. The Mount Sinai Institutional Review Board reviewed and approved the study design. Informed consent was completed before participating in the online and paper-and-pencil survey versions.
Procedures
In 2014, Pietrzak et al first reported WTC-related PTSD symptom trajectories in WTC responders who were WTC-HP members. 27 The PTSD trajectories examined in our current sample were identified during a previous analysis completed by our team. 26 In that analysis, longitudinal WTC-related PTSD symptoms were characterized by four trajectories in police responders, including No/Low-Symptom (76.1%), Worsening (12.1%), Improving (7.5%), and Chronic (4.4%) trajectories. As described in Feder et al, 26 1.3% of the Worsening group screened positive for probable PTSD (cutoff PCL-S ≥ 44) at T1 and 62.4% screened positive at T4. At T1, 52.9% of the Improving group screened positive for probable PTSD and only 15% screened positive at T4, and 74% of the Chronic group screened positive at all four time points. Five trajectories were identified for non-traditional responders, including No/Low-Symptom (55.5%), Subtly Worsening (19.3%), Chronic (10.8%), Improving (8.5%), and Steeply Worsening (5.9%) trajectories. Again, as described in Feder et al, 26 14.3% of the Subtly Worsening group screened positive for probable PTSD (cutoff PCL-S ≥ 44) at T1 and 61.3% screened positive at T4. In contrast, 30.1% of the Steeply Worsening group screened positive at T1 and 92.8% screened positive at T4. At T1, 79.8% of the Improving group screened positive and only 14.8% screened positive at T4, and 91.8% of the Chronic group screened positive at all four time points. These subjects were assessed over four time-points, an average of 3 (T1), 6 (T2), 8 (T3), and 12 (T4) years post-9/11/2001. For this cohort, the first three time-points comprise WTC-HP health monitoring visits conducted a median of 2.8, 5.7, and 7.8 years post-9/11/2001. The fourth time-point (T4) consisted of the web-based survey, administered a median of 12.2 years post-9/11/2001.
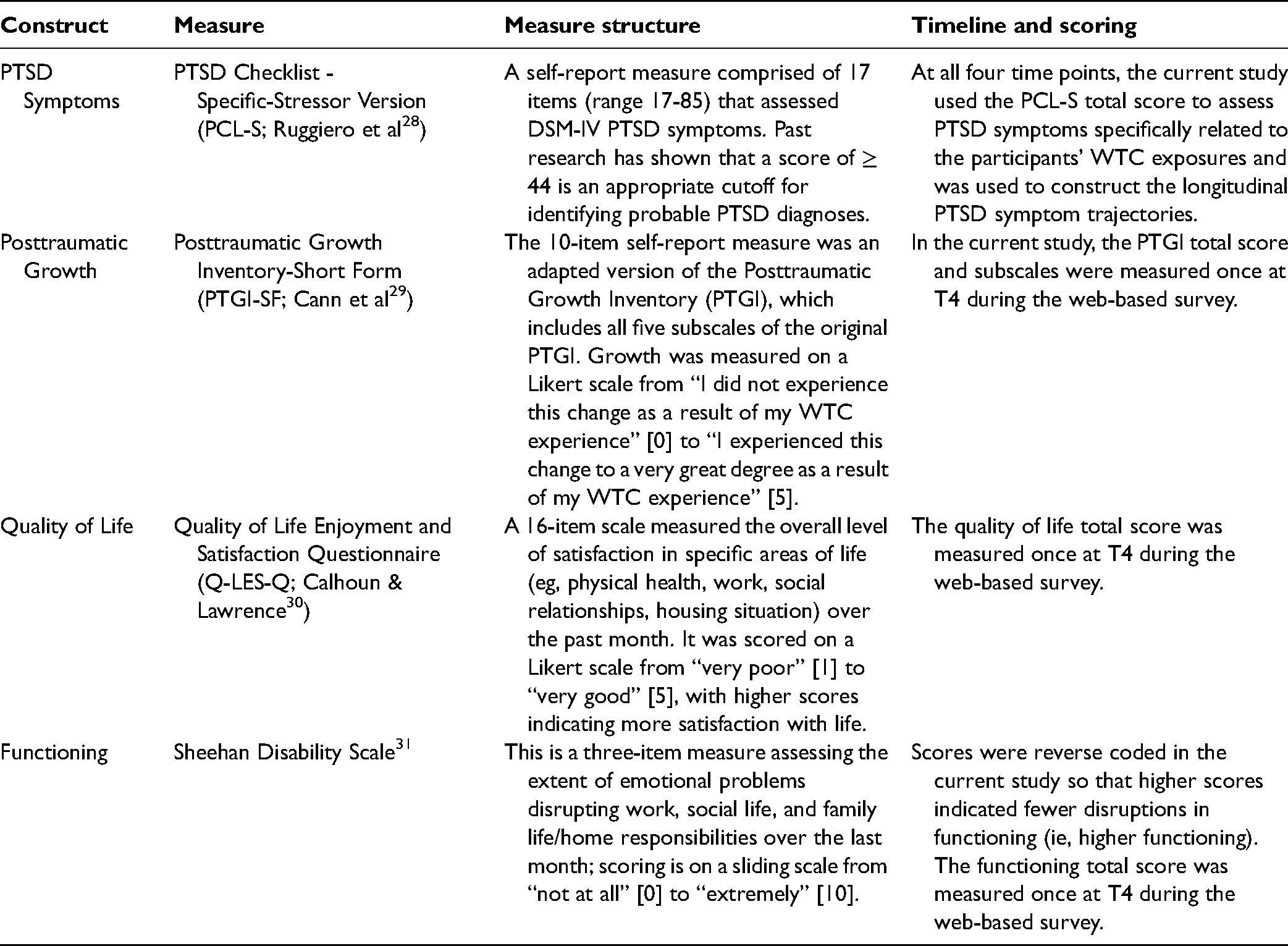
Demographic characteristics and several PTSD risk and protective factors were assessed during the first health monitoring visit at the WTC-HP (T1). Levels of PTG, functioning, quality of life, and other potential risk factors were additionally assessed in the web-based survey (T4; Timeline of data collection procedures can be found in Supplemental Figure 1). The information regarding all measures utilized to assess core constructs is presented on Table 1.
Assessment measures utilized in the protocol.
Data Analysis
Longitudinal trajectories of WTC-related PTSD symptoms among police and non-traditional responders across the four time-points were identified using latent growth mixture modeling (LGMM) of total PCL-S scores (full-information maximum-likelihood estimation in Mplus version 7.3). Before analyses, multiple imputation by chained equations was used to impute missing values for the dependent and independent variables. Further details about the derivation of these trajectories can be found in Feder et al. 26
Covariates were determined based on prior research on factors associated with resilience or PTSD following the WTC attacks. In studies of WTC attack-exposed samples, predictors included demographic characteristics, WTC exposure type and severity, history of other lifetime trauma exposures and stressful live events, co-morbid medical conditions, and the availability of social support.32–35 In an overlapping sample of 10 835 WTC rescue and recovery workers, our team determined that symptomatic trajectories of PTSD were associated with a prior psychiatric history, Hispanic ethnicity, the severity of WTC exposure, and a higher number of WTC-related medical conditions. 27 Greater education and greater family and work support while working on the WTC effort were protective factors against symptomatic trajectories. These factors were self-reported at either T1 or T4 and included as covariates in all our analyses.
STATA, version 13.1, was used to perform the analyses. Police and non-traditional responders differed in pre-disaster training and several study variables, including age and sex (as described in Pietrzak et al 27 and Feder et al 26 ); therefore, all analyses were stratified by occupational group (police vs non-traditional responders). For Aim 1, bivariate Pearson correlations were performed to determine whether PTG was associated with potential protective and risk factors for PTSD within each occupational group and are displayed in Table 2. For Aim 2, hierarchical linear regressions were completed to determine whether PTSD symptom trajectories predicted PTG with the Posttraumatic Growth Inventory-Short Form (PTGI-SF) total score as the outcome variable. As described in Table 3, the hierarchical models included demographic variables from T1 in Step 1, pre-9/11 variables in Step 2, peri-9/11 variables in Step 3, post-9/11 variables in Step 4, and finally trajectories of PTSD symptoms in Step 5, with the No/Low-Symptom trajectory as the reference category. While only the results from Step 5 are displayed in Table 3, Table S2 in the Supplemental Materials displays the full results of each step in the hierarchical models.
Means, standard deviations, and correlations.

Note: Posttraumatic Growth Inventory-Short Form total score is the dependent variable; SDS = Sheehan Disability Scale; Quality of Life = Quality of Life Enjoyment and Satisfaction Questionnaire total score. *P < .05; **P < .01.
Hierarchical linear regressions for trajectories of PTSD symptoms and posttraumatic growth.

Note: Unstandardized coefficients are presented with standard errors in parentheses; Posttraumatic Growth Inventory-Short Form total score is the dependent variable. *P < .05; **P < .01.
To evaluate if PTG is associated with functional measures, a secondary aim was included in a supplemental analysis to examine whether PTG total and subscale scores were cross-sectionally associated with higher functioning and higher quality of life in each occupational group after adjusting for PTSD symptom trajectories. Two hierarchical linear regressions were conducted within each occupational group to predict functioning and quality of life total scores. All variables from the five Steps in the Aim 2 model were included, with the addition of PTGI-SF total score as Step 6 of the model. These two models were then re-specified by replacing the PTGI-SF total score with the five PTGI-SF subscales. 17 All five subscales were entered simultaneously in these models to evaluate how they may relate to functioning and quality of life scores.
Results
Demographic and Psychosocial Variables
Bivariate correlations with PTGI-SF total scores are presented in Table 2, along with means and standard deviations for demographics and pre-/peri-/post-9/11 variables. Police responders had an average PTGI-SF total score of 20.42 (SD = 13.85), and non-traditional responders had an average PTGI-SF total score of 23.53 (SD = 13.49). Among police responders, PTG was positively associated with all pre-/peri-/ post-9/11 variables except the number of traumatic events before 9/11. Among non-traditional responders, PTG was positively related to the number of life stressors before 9/11, work support while working at the WTC site, and all post-9/11 variables. Also, non-traditional responders with fewer traumatic events before 9/11 had higher PTG. Age, gender, race/ethnicity, education, income, and marital status were all significantly correlated with PTG for at least one occupational group, supporting their inclusion as control variables in the subsequent analyses.
Supplemental analyses of cross-sectional association between the five PTG dimensions, indicated that only more openness to new possibilities was associated with higher functioning for both occupational groups in the fully adjusted model. Additionally, greater openness to new possibilities and a greater sense of relatedness to others were associated with higher quality of life scores among non-traditional responders (Supplemental Table S1). Higher spiritual change was associated with lower functioning scores in both occupational groups, as well as lower quality of life scores in non-traditional responders; and higher appreciation of life was also linked to lower functioning and quality of life scores in police responders, in the fully adjusted model.
Trajectories of PTSD and Risk Factors Predicting Posttraumatic Growth
Table 3 shows the results of the hierarchical linear regressions. For both occupational groups, being female and in a racial or ethnic minority group was associated with higher PTG. A higher number of pre-9/11 life stressors and of WTC-related exposures, and more sources of family support were significantly associated with higher levels of PTG for police responders. Higher work-related support was associated with higher PTG only for non-traditional responders, even after PTSD symptom trajectories were accounted for. A higher number of traumatic events since 9/11 was significantly associated with higher PTG for both occupational groups, after adjusting for PTSD symptom trajectories.
Relative to police responders with No/Low-Symptom PTSD symptom trajectories, responders with worsening trajectories had 3.7 points greater PTGI-SF total score, and responders with improving trajectories had 2.6 points greater PTGI-SF total score after adjusting for all covariates. Also, compared to non-traditional responders with No/Low-Symptom trajectories, responders with Subtly Worsening, Steeply Worsening, Chronic, or Improving trajectories of PTSD symptoms had 3.3 to 5.4 points greater PTGI-SF score, after adjusting for covariates. As seen in Figure 1, police responders with Worsening and Improving trajectories and non-traditional responders with Chronic and Improving trajectories had the greatest levels of growth. Significant mean differences in PTGI-SF scores were between the No/Low-Symptom trajectory and the symptomatic trajectories for both occupational groups, but no other differences were found between the remaining symptomatic groups according to the pairwise comparisons (as seen in Figure 1).

Average PTGI-SF total score across longitudinal trajectories of PTSD by occupational group. The results of pairwise comparisons from the regression model in Table 3 are displayed. PTGI-SF = posttraumatic growth inventory-short form total score; *P < .05; **P < .01.
Discussion
In this study, we aimed to determine the level of self-reported growth in each of the occupational groups and understand the relationship between growth and potential risk and protective factors against PTSD, and examine whether longitudinal PTSD symptom trajectories predict PTG. Our results indicate that across both occupational groups, female gender, older age, and Hispanic ethnicity (and black racial identity for non-traditional responders) were associated with higher PTG, even when accounting for PTSD symptom trajectories. In prior work, older age and female gender have been identified as predictors in PTG development, particularly in those with more severe PTSD.36, 37 Many of these factors were also previously found to predict more severe PTSD symptoms or reduced likelihood of resilience following 9/11 in the NYC community and WTC responders.27, 32–34 Collectively, these findings highlight the importance of considering these risk factors as part of psychoeducational and preventive interventions for first responders.
When examining pre-/peri-/post-9/11 variables, the only independent factor associated with PTG for both occupational groups was a higher number of post-9/11 traumatic events. For police responders, a greater number of pre-9/11 stressors and greater familial support were associated with PTG. For non-traditional responders, greater occupational support was associated with PTG. These factors’ association with PTG align with the theory that greater psychological distress, including PTSD symptoms, and greater social support are independent predictors of PTG.2, 10, 38 Wei et al 4 showed that the strongest modifying factors in the relationship between PTSD and PTG are the level and type of trauma exposure, which align with our finding that higher WTC-related exposure severity was associated with PTG for police responders, even after controlling for PTSD symptom trajectories. 4 Notably, for non-traditional responders, above-high-school education and more pre-9/11 traumatic events were associated with lower levels of growth. Psychological distress is theorized to be a key factor in the development of PTG. 3 However, higher education and other lifetime traumas may be associated with more severe PTSD symptom trajectories, increasing distress levels and making it harder to generate meaning-making cognitions, thus decreasing the likelihood of developing PTG. In support of this conceptualization, higher education and a history of prior trauma predicted reduced resilience to PTSD symptoms post-9/11 in the NYC community study mentioned above. 32 Future work should probe the role of these potential growth-impeding factors if they are replicated in other samples.
The current findings suggest that symptomatic trajectories of PTSD across an average of 12 years post-9/11 predicted greater PTG in comparison to the No/Low Symptom trajectory, except for the chronic symptom trajectory for police responders. Our pairwise analyses of the PTSD symptom trajectories supported our hypothesis that the No/Low-Symptom trajectories would predict the lowest levels of growth. The curvilinear model of the relationship between PTSD and PTG posits that moderate, but not extreme or low, levels of trauma-related distress would result in PTG.16–18 In support of this model, the moderate symptom trajectories (ie, Worsening and Improving) were associated with higher levels of PTG across both occupational groups compared to the No/Low-Symptom trajectory. Our hypothesis was further supported for police responders, as the more severe Chronic symptom trajectory had comparable levels of PTG to the No/Low-Symptom trajectory. Counter to our hypothesis, the severe symptom trajectories (ie, Steeply Worsening and Chronic) for non-traditional responders had significantly higher levels of PTG compared to the No/Low-Symptom trajectory. However, our results did indicate that the magnitude of the difference in PTG level, when compared to the No/Low-Symptom trajectory, was smaller for the more severe trajectories (3.305 to 4.480 PTGI-SF points higher) than the moderate trajectories (5.055 to 5.438 PTGI-SF points higher), indicating that an inverted U-shape may best represent the relationship between PTSD and PTG in both occupational groups.
When examining the positive functional implications of overall PTG levels, our findings suggest that greater levels of growth were cross-sectionally associated with higher quality of life in non-traditional responders. However, our results indicate a mixed relationship between the dimensions of PTG and functioning and quality of life. Greater openness to new possibilities in life was the only dimension of PTG to be associated with higher functioning across both occupational groups. Greater openness to new possibilities in life and a stronger sense of relatedness to others was associated with higher quality of life in non-traditional responders. However, spiritual changes were associated with lower functioning across both occupational groups. One possible interpretation is that individuals with lower quality of life are often more likely to turn to religion/spirituality to cope and pursue finding meaning and thus might report experiencing more spiritual changes.26, 39 The significant relationship between overall PTG and quality of life in non-traditional responders should encourage future studies to explore psychotherapy focused on personal growth,30, 40–42 as well as incorporating strategies to help bolster PTG into interventions for rescue and recovery workers. 43
There were several notable strengths to this study. Among longitudinal studies predicting PTG, this study examined the prediction of PTG from PTSD symptom trajectories with a substantial sample size, across the greatest number of time points and for one of the longest assessment periods (approximately 12 years) of any study on the topic. Even though first responders are at higher risk of exposure to traumatic events through their occupation, there is a lack of research on PTSD symptom trajectories and PTG in this population. We examined this relationship in a diverse sample of responders engaged in WTC rescue, recovery, and clean-up efforts – including police and non-traditional responders – who were all exposed to the same primary traumatic event (the 9/11 WTC terrorist attacks).
A notable limitation of this study is the use of a self-report measure to assess PTSD symptom severity as opposed to a clinician-administered diagnostic interview. One of the main limitations of this study is that PTG was measured only at the end of the 12-year follow-up period rather than shortly after 9/11 and throughout the follow-up period and, therefore, causal claims cannot be made about the effect of PTSD symptom trajectories on the development of PTG. As a result of this study design, any possible bidirectional relationships between PTSD symptom presentation and PTG could not be evaluated. 44 Further, potentially informative baseline (eg, religiosity/spirituality) and time-varying variables (eg, stressors, mental health treatment engagement) were not assessed during repeated assessments. Further research employing panel designs and incrementally informative predictors of PTG is needed to provide a more comprehensive understanding of factors associated with the development and maintenance of PTG in WTC responders and other trauma-exposed populations.
Prior work has primarily focused on cross-sectional or short-term (one to two-year) assessments of changes in PTSD symptom severity and PTG. Our work expands the literature by examining the prediction of PTG levels from longitudinal PTSD trajectories across four time points over an average of twelve years. The current study demonstrated that moderate PTSD symptom levels (ie, Worsening and Improving trajectories) were associated with relatively greater levels of growth after trauma and that greater growth may promote greater quality of life, independent of PTSD symptom severity. Our results suggest that growth-focused interventions may help improve the quality of life for rescue and recovery workers experiencing PTSD symptoms by specifically promoting openness to new possibilities and deeper connections to others after experiencing a traumatic event. Our study supports the conceptualization of PTG as concurrent with prolonged experiences of PTSD. It suggests that PTG may represent a “silver lining” that may help enhance quality of life for those who face posttraumatic distress. Further research is needed to evaluate longitudinal interrelationships between PTSD and PTG; biopsychosocial mechanisms linking PTSD symptoms to PTG; and the direct and interactive effects of PTG in promoting functioning and quality of life in WTC responders and other trauma-affected populations.
Supplemental Material
sj-docx-1-css-10.1177_24705470221122898 - Supplemental material for Longitudinal Trajectories of PTSD Symptoms Predict Levels of Posttraumatic Growth in World Trade Center Responders
Supplemental material, sj-docx-1-css-10.1177_24705470221122898 for Longitudinal Trajectories of PTSD Symptoms Predict Levels of Posttraumatic Growth in World Trade Center Responders by Marin M. Kautz, Abigail Collins, Clyde B. Schechter, Ryan Salim, Janice Rodriguez, Ritika Singh, Christopher R. Dasaro, Andrew C. Todd, Michael Crane, Jacqueline M. Moline, Iris G. Udasin, Denise J. Harrison, Benjamin J. Luft, Steven M. Southwick, Robert H. Pietrzak and Adriana Feder in Chronic Stress
Footnotes
Acknowledgments
We would like to acknowledge the faculty and staff of the World Trade Center Health Program; the labor, community, and volunteer organization stakeholders; and the WTC rescue and recovery workers, who gave of themselves so readily in response to the WTC attacks and to whom the WTC Programs are dedicated. Data were also provided by the WTC Health Program General Responder Data Center at Mount Sinai (CDC/NIOSH contract # 200-2017-93325). This study would not have been possible without the dedication and contributions of Steven M. Southwick, MD, who inspired our research to promote resilience and well-being in WTC responders and other trauma survivors. We dedicate this study to his memory.
Declaration of Conflicting Interests
Dr Feder is named co-inventor on an issued patent in the US and several issued patents outside the US, filed by the Icahn School of Medicine at Mount Sinai (ISMMS) for the use of ketamine as therapy for PTSD. This intellectual property has not been licensed.
Funding
This research was supported by the CDC/National Institute for Occupational Safety and Health (NIOSH) (A.F., R.H.P., and S.M.S., research contract # 200-2011-41919). Marin Kautz was supported by National Science Foundation Graduate Research Fellowship 1650457. Any opinions, findings, conclusions, or recommendations expressed in this article are those of the author(s). They do not necessarily reflect the views of the CDC/ NIOSH or the National Science Foundation.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.