
Abstract
Posttraumatic stress disorder is a heterogeneous disorder with disturbances in hyperarousal or avoidance behaviors and intrusive or reexperiencing thoughts. The uncinate fasciculus and cingulum bundle are white matter pathways implicated in stress and trauma pathophysiology, yet their structural integrity related to posttraumatic stress disorder symptom domains is yet to be understood. Forty-four trauma-exposed young adults underwent structural and diffusion-weighted magnetic resonance imaging. Stress and trauma exposure indices and severity of posttraumatic stress disorder symptoms were collected and used to predict current integrity of the uncinate fasciculus and cingulum bundle. Severity of reexperiencing posttraumatic stress disorder symptoms was significantly related to increased fractional anisotropy (r = .469 p < .001) and decreased mean diffusivity (r = −.373, p = .013) of the right posterior cingulum bundle. No other findings emerged with respect to stress exposure or of hyperarousal (p’s > 0.05) or avoidance (p’s > 0.2) posttraumatic stress disorder symptoms. The posterior cingulum connects medial temporal lobe structures with visual areas in the occipital lobe and has been implicated in visual memory and self-referential thought. Increased structural connectivity along this pathway may therefore explain the emergence of reexperiencing posttraumatic stress disorder symptoms. This along with the lack of results with respect to stress exposure suggests that structural aberrations in white matter pathways are more strongly linked with the actual experience of stress-related psychological symptoms than just exposure to stress.
Nearly 90% of people in the United States will experience a traumatic event in their lifetime. 1 Although most are resilient in the aftermath of trauma,2–6 a substantial minority go on to develop debilitating psychopathologies.7–10 In particular, stress and traumatic stress lead to increased risk of posttraumatic stress disorder (PTSD), a disorder characterized by symptoms of reexperiencing the event through intrusive thoughts, nightmares, flashbacks, avoidance of trauma-related stimuli, and symptoms of hyperarousal.11–13 Although cumulative stress and trauma exposure increase risk of psychopathology, 7 the brain changes that mediate this risk are not well understood.
Stress and traumatic stress can negatively impact the brain, for example, through the integrity of white matter tracts.11,14–16 White matter tracts are the myelinated axons of neurons that connect brain regions to coordinate the transfer of information throughout the brain. 17 Estimation of the integrity of white matter tracts can be done with diffusion tensor imaging (DTI), a noninvasive magnetic resonance imaging (MRI) technique that harnesses the diffusion properties of water through brain tissue. 18 Studies using DTI have shown that stress and trauma impact white matter integrity through activation of the hypothalamic–pituitary–adrenal (HPA) axis and the release of various stress hormones. 19 Excess exposure to stress hormones, particularly in critical windows of brain development, can impair maturation and integrity of white matter pathways 20 in circuits supporting memory formation and maintenance as well as emotion regulation, both processes implicated in PTSD.11,15,18,19,21 Therefore, it is important to understand how stress and trauma affect the structural integrity of the brain to understand how structural integrity may underlie altered cognitive and affective processing in PTSD.
One region that has been repeatedly implicated in stress-related psychopathology is the hippocampus as it is especially sensitive to activity of the HPA axis.11,14,19 Specifically, high levels of cortisol and other stress hormones are thought to lead to damage of the hippocampus. 11 Some researchers have found that smaller hippocampal volume confers greater risk of developing PTSD if individuals are exposed to trauma. 11 As the hippocampus is also important for the encoding and retrieval of memories, particularly emotional or stress-related memories,19,22–24 impaired retention of extinction learning which is consistently observed in PTSD implies hippocampal dysfunction.25,26 Although the effects of stress on the hippocampus are well-documented, the downstream or upstream effects of stress on adjacent white matter pathways that involve the hippocampus are less understood.19,27
The cingulum bundle is a white matter tract that projects from the cingulate gyrus to the hippocampus and medial temporal lobe cortices that allows for the communication of the limbic system to the cortex. 28 Integrity of the cingulum has been argued to play an important role in emotion regulation and has been hypothesized to contribute to the dysregulated emotions seen in PTSD.29,30 Decreased integrity of the cingulum has been reported in a variety of populations, including women with high exposure to trauma,31,32 Afghanistan and Iraq war veterans with PTSD, 29 adults with major depressive disorder, 14 adults with a history of childhood trauma, 33 and adolescents with a history of abuse. 34 This weaker connectivity in the cingulum has been shown to have functional consequences, including the insufficient top-down emotion appraisal and regulation characteristic of PTSD.15,29,31 Thus, repeated exposure to trauma and subsequent stress may be related to the microstructural degradation of the cingulum. 35
By contrast, other researchers have found increased integrity of the cingulum in individuals afflicted by various types of trauma, including an act of terrorism, 36 combat,30,37,38 severe mine accident survivors, 39 and in a mixed-trauma sample of PTSD patients, 40 and that greater cingulum integrity is related to greater symptom severity in these samples.30,37,38,40 Discrepancies in terms of whether trauma is related to decreased versus increased cingulum integrity may be related to the fact that PTSD is a heterogeneous disorder, and the presence of specific symptom clusters of PTSD may be directly related to cingulum integrity. Some researchers have found that increased structural connectivity of the cingulum is related specifically to intrusive reexperiencing symptoms, though some report increased 30 while others report decreased symptoms. 39 At this time, more research is needed to clarify direction of findings as it relates to the association between cingulum white matter integrity and PTSD symptoms.
Another white matter tract that is implicated in the pathophysiology of PTSD is the uncinate fasciculus (UF), a tract which connects the temporal cortices involved in memory formation and the frontal cortices involved in emotion regulation.16,41,42 Decreased UF integrity has been linked to impaired extinction learning41,43,44 as well as misevaluation of social-emotional stimuli that may be linked to avoidance behaviors seen in PTSD.41,43,44 A review of the development of the UF indicates that early life abuse or stress may be associated with decreased structural integrity due to the sensitivity of limbic regions to stress hormones. 43 Decreased integrity of the UF has been reported in children with a history of maltreatment,33,45 police officers with PTSD, 44 and in mixed-trauma community samples.46,47 In addition, reduced UF integrity is predictive of psychological vulnerability to future stress or trauma. 45 Therefore, impaired structural integrity of the UF may be another potential indicator of stress history and PTSD symptom severity.
Although structural changes have been identified in various populations with adverse backgrounds of stress and trauma, very few of these studies have included samples with emerging adults.48,49 Longitudinal studies investigating developmental changes in major white matter pathways suggest that the cingulum and UF stop maturing around the mid-20 s, which means white matter in emerging adults may still be developing.20,50 Understanding how stress and trauma affect white matter pathways while they are still maturing may help inform the trajectory of mental health outcomes later in life. Moreover, very few studies have compared the effects of both stress exposure and severity of stress-related symptoms across the domains of reexperiencing, avoidance, and hyperarousal symptoms on white matter integrity.38,51 Therefore, one of the primary purposes of the current study is to investigate how stress exposure and symptoms of PTSD may impact the structural integrity of white matter pathways, particularly the cingulum bundle and the UF in emerging adults. Previous research has shown that the direction of integrity changes in the cingulum may explain different stress-related symptoms.15,29–31 Owing to this hetereogeneity of findings, we predicted that altered cingulum integrity would be associated with greater life stress and increased severity of PTSD symptoms. In addition, we also predicted that decreased integrity of the UF would be related to greater life stress as well as increased severity of PTSD symptoms.
Method
Participants
Sixty-seven trauma-exposed young adults (23 males and 44 females; Mage = 22.32, standard deviation (SD) = 3.75) originally participated in this study. Inclusion criteria included being right handed, over 18 years old, and reporting experience of at least one past trauma as measured by the Life Events Checklist (LEC). 52 Exclusion criteria included the presence of neurological disorders, mania, psychosis, history of head trauma, or any contraindications for a MR scan including metal in the body, pregnancy, or claustrophobia. To ensure normality, seven participants were excluded from analysis for outlying ( ± 2.5 SD) stress and PTSD symptom severity scores (n = 4 females, n = 1 male) and outlying diffusion measures (n = 2 females). In addition, due to the uneven distribution of males and females, and to account for potential gender49,53–55 and age differences20,54 that have been well documented in the white matter pathways of interest, the final sample included in analysis was matched in terms of gender and age distribution. In addition, the final sample was also matched on total PTSD severity scores from the PTSD Checklist Civilian (PCL-C). 56 The final sample thus had 44 participants (22 males and 22 females; Mage = 22.93, SD = 4.13). The study was approved by the University of Wisconsin—Milwaukee Institutional Review Board. According to the Declaration of Helsinki, participants provided written informed consent and were paid for their participation in the study.
Stress and Trauma Measures
Life stress and trauma were assessed using the LEC, 52 the Life Events Scale (LES), 57 and the Daily Hassles Scale (DHS). 58 LEC has good internal (Kappa = .61) and test–retest reliability (r = .82) 52 and assesses occurrence of major life events that a person has experienced firsthand, witnessed, or heard about happening to someone close to them (e.g. natural disaster, assault, combat, life-threatening illness, or injury). The LES assesses the occurrence and severity of major life events that have happened in the last 12 months (e.g. marriage, unwed pregnancy, death of parent, failure of a grade in school, and serious illness). The DHS has demonstrated good test–retest reliability (r = .79) 58 and assesses the degree to which an individual is bothered by daily pressures, or difficulties (e.g. financial security, preparing meals, not getting enough sleep, job dissatisfaction, and traffic).
Based on Vinkers et al., 59 in addition to examining these three self-report measures individually, a cumulative stress index (CSI) was calculated by z-transforming all three scales (LEC, LES, and DHS) and summing the three z scores. Although it is unlikely these stress measures should be weighted equally when computing the cumulative index, it would be difficult to determine appropriate weights of these various measures, and this method allows for at least a preliminary investigation of an index of cumulative stress.
PTSD symptoms were assessed using the PCL-C. 56 The PCL-C is a 17-item self-report measure that assesses each of the symptom domains of PTSD including reexperiencing, avoidance, and arousal symptoms. Participants rate their degree on a scale of 1 to 5 (1 = not at all, 5 = extremely) for which they have been bothered by a given problem. Example items include “repeated, disturbing dreams of a stressful experience”, “having physical reactions (e.g., heart pounding, trouble breathing, sweating) when something reminded you of a stressful experience,” and “being ‘super-alert’ or watchful or on guard.” Responses can be summed to attain a total PTSD symptom severity score or can be summed by symptom domain.
MRI Acquisition
MRI was collected on a 3 T short bore GE Signa Excite system. High-resolution spoiled gradient recalled anatomical images were acquired in a sagittal orientation (repetition time (TR) = 8.2 ms; echo time (TE) = 3.2 ms; field of view (FOV) = 24 cm; flip angle = 12°; voxel size = 1 × 0.9375 × 0.9375 mm). Diffusion-weighted images were collected using an echoplanar pulse sequence with 70 contiguous 2-mm-thick axial slices and 38 noncollinear diffusion gradients (TR = 10 s; TE = 77.99 ms; b value = 800 s/mm2; FOV = 25.6 cm; flip angle = 90°; voxel size = 2 × 2 × 2 mm).
Image Analysis
Sample characteristics of trauma-exposed individuals (LEC > 0).
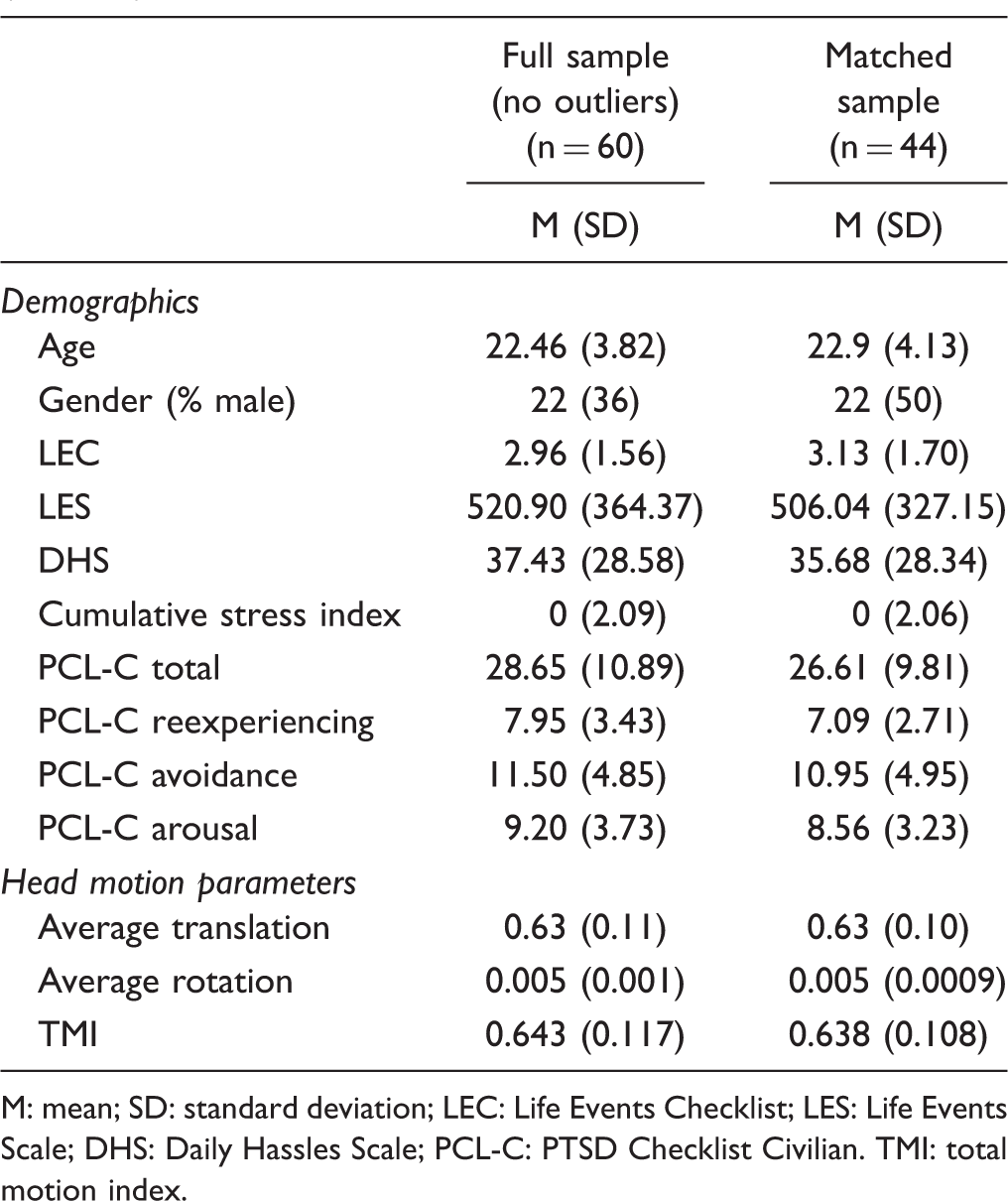
M: mean; SD: standard deviation; LEC: Life Events Checklist; LES: Life Events Scale; DHS: Daily Hassles Scale; PCL-C: PTSD Checklist Civilian. TMI: total motion index.
Next, FMRIB Software Library's (FSL’s) bedpost was used to fit the ball-and-stick model of diffusion at every voxel. Two anisotropic compartments were fit at every voxel to account for crossing fibers. We then used TRACULA to conduct global probabilistic tractography to reconstruct white matter pathways. This reconstruction references an atlas of manually segmented white matter pathways of 33 healthy individuals. TRACULA segments the cingulum into anterior and posterior components. The anterior cingulum spans the cingulate gyrus from the anterior cingulate cortex until reaching the turning point of the cingulum bundle at the posterior cingulate cortex (PCC). The posterior cingulum runs the rest of the cingulum bundle from the posterior cingulate gyrus to the entorhinal and parahippocampal cortices. Fractional anisotropy (FA) and mean diffusivity (MD) values were extracted for the UF, and anterior cingulum (CCG, cingulum cingulate gyrus) and posterior cingulum (CAB, cingulum angular bundle) (See Figure 1 for pathways from a representative subject). FA is a measure of the degree of anisotropic diffusion and estimates the overall coherence of tissue such that higher values indicate greater white matter integrity. MD approximates the overall rate of diffusion with higher values indicating poorer white matter integrity. FA and MD values were weighted on a voxel-wise basis according to the probability of each voxel being in the tract and then averaged over all voxels in that tract.
White matter pathways of interest rendered by TRACULA for a representative subject.
Results
To better characterize this study’s sample, demographic, stress, and PTSD symptom measures for the full sample (n = 60 excluding outliers) and matched sample (n = 44) are reported in Table 1. All subsequent results reported utilize the matched sample (n = 44).
White matter tract characteristics (n = 44).

M: mean; SD: standard deviation; FA: fractional anisotropy; MD: mean diffusivity; UF: uncinate fasciculus; CCG: cingulum cingulate gyrus (anterior cingulum); CAB: cingulum angular bundle (posterior cingulum).
Tract Integrity and Stress Exposure
To examine the relationship between white matter integrity and stress, FA and MD measures were extracted in each hemisphere for the UF, anterior (CCG) and posterior cingulum (CAB). LEC, LES, and DHS were z transformed and summed to generate a CSI. DTI measures of each tract in each hemisphere were entered as predictors in separate linear regressions with each of the stress exposure measures as outcome variables. Results showed no significant associations with the UF and any of the stress measures (all p’s > .06). In addition, there were no significant associations between stress measures and either the anterior (CCG) (all p’s > .13) or posterior cingulum (CAB) (all p’s > .20).
Tract Integrity and PTSD Symptom Severity
To examine the relationship between white matter integrity and PTSD symptom severity, again FA and MD measures in each hemisphere for the UF, anterior (CCG) and posterior (CAB) cingulum, were entered into four separate linear regressions predicting total PCL-C symptom severity, reexperiencing, avoidance, and hyperarousal symptoms. Severity of reexperiencing symptoms was positively correlated with FA in the right posterior cingulum (r = .469, p < .001). Although it did not survive the Holm–Bonferroni correction, reexperiencing symptoms were also negatively correlated with MD (r = −.373, p = .013) of the right posterior cingulum bundle (CAB) (Figure 2). These results suggest that greater integrity of the right posterior cingulum bundle (CAB) is related to greater reexperiencing symptoms. PCL-C total and subscale scores were not associated with FA or MD values in the anterior cingulum (all p’s > .15) or UF (all p’s > .11).
Greater integrity of the right posterior cingulum is related to reexperiencing symptoms. FA: fractional anisotropy; MD: mean diffusivity.
Discussion
The current study used DTI measures of FA and MD to investigate how stress exposure and PTSD symptoms predicted alterations in the integrity of key white matter tracts, the cingulum bundle and the UF, in an emerging adult sample. We expected that stress exposure and PTSD symptoms would be related to altered cingulum integrity and decreased integrity in the UF and found partial support for our hypotheses. Lifetime stress exposure was not related to UF or cingulum bundle integrity; however, there was evidence that reexperiencing symptoms of PTSD were related to cingulum, but not UF, integrity. Therefore, greater structural connectivity of this pathway may be a biomarker for increased reexperiencing symptoms.
In accordance with our findings, others have also found that increased cingulum integrity is related to PTSD symptom severity.30,36 Montag et al. 49 also found a positive correlation between posterior cingulum (CAB) integrity and trait anxiety in healthy adults. Together these results indicate that internalizing symptoms whether in PTSD or anxiety may be related to increased cingulum integrity.
Reexperiencing symptoms in PTSD are intrusive memories of a traumatic event. 13 These intrusive memories are largely involuntary and may manifest as flashbacks or nightmares involving vivid imagery or other strong sensory elements. 24 The increased integrity of the posterior cingulum we observed may explain reexperiencing symptoms due to its connectivity between the hippocampus and PCC. 28 As stated previously, the hippocampus is involved in the encoding and retrieval of memories particularly stress-related memories.19,22–24 Involuntary retrieval of memories involves the hippocampus along with the structures associated with the original perception of the event; however, all in the absence of prefrontal cortex recruitment.23,62,63 The absence of prefrontal activation suggests the lack of top-down control in the involuntary memory retrieval process. 63 Therefore, involuntary retrieval of salient memories, in this case, intrusive memories from a stressful or traumatic event, are mediated by hippocampal processes. In addition, the PCC, a key structure in the default mode network, has been implicated in internally focused thought. 64 Functional connectivity studies have shown that the PCC plays an important role in directing attention internally and retrieving episodic and semantic memories.64,65 Due to its structural and functional connections, the PCC is sometimes viewed as a “hub” for which information from the cortex and subcortical structures can be integrated. 65 Thus, hyperconnectivity of the posterior cingulum (CAB) from the hippocampus to the PCC could be reflective of greater internally directed attention and memory retrieval 66 which may lead to the increase in reexperiencing symptoms in PTSD.
Others have found results contradictory to ours when investigating the relationship between symptom severity of PTSD and tract integrity in adults. For example, Zhang et al. 39 found that increased FA and thus increased integrity of the posterior cingulum was related to decreased reexperiencing symptoms in a sample of adult males in their 30 s with PTSD. Similarly, increased cingulum FA was shown to relate to decreased reexperiencing symptoms in samples of adult females in their 30 s and 40 s with PTSD.31,32 This indicates that structural changes in the brain may be differentially affected for adults versus emerging adults due to different neurodevelopmental stages of brain maturation. As white matter architecture is still maturing in emerging adults,20,50 symptoms from stress or trauma exposure may alter structural integrity of the cingulum, resulting in hyper connectivity of this pathway in those who have PTSD symptoms. However, in adults, the maturation process has largely ceased, and cingulum integrity slowly degrades over time.20,50 Thus, symptoms from stress and trauma experiences may only be reflected through increased degradation of this tract in more mature samples. This differential pattern in the way stressful experiences may be integrated into cingulum integrity could explain the discrepancies in white matter integrity findings in the literature.
Interestingly in our sample, stress exposure measures did not correlate with integrity of the cingulum. This suggests that stress or trauma exposure alone may not be sufficient to contribute to structural brain changes, but that such changes are more strongly linked with the actual experience of stress-related psychological symptoms, although this finding warrants replication. The CSI created for this study was created by combining multiple existing measures as a way to examine white matter integrity in relation to cumulative stress. Although this index did not yield any significant results, it would be useful for the field to develop a validated measure of composite stress, including both major stressors and smaller hassles, to assess this and other relationships. Although others have established the effects of stress exposure on brain structure in depression14,19,45,67 and anxiety,45,68 no one, to our knowledge, has investigated correlations of stress and trauma exposure effects alone on brain structure within the context of PTSD.
We did not find any significant differences in UF integrity related to stress exposure or PTSD symptoms. This result is inconsistent with the literature as stress and trauma have been shown to have negative effects on UF integrity,33,43 increasing an individual’s risk for development of psychopathology symptoms. 45 Fani et al. 32 and Averill et al. 38 also reported a null relationship with UF integrity and PTSD symptoms, arguing that the UF may not be contributing to PTSD symptoms. Although impaired integrity of the UF has been implicated in extinction learning, a common model of PTSD symptomology,41,43,44 it is possible that the UF does not directly contribute to stress-related psychopathology. As stated before, given the current study’s sample, the discrepancy in UF integrity findings may be a result of differential effects of stress at this unique neurodevelopmental stage compared to adulthood. Alternatively, the discrepancy in UF integrity findings may be a result of methodological differences in MRI acquisition and analysis.
There were a few limitations in the current study. First, our sample of emerging adults, though all exposed to trauma, did not necessarily meet criteria for PTSD diagnosis. A score of 30 on the PCL-C has been shown to be a significant clinical cutoff for diagnosis of PTSD. 69 Our sample had a mean PCL-C score of 27.32 indicating a subthreshold sample, so interpretation of findings with regard to PTSD diagnosis should be done with caution. In addition, this study was not a prospective one, so we cannot interpret the direct outcomes of brain changes and how they vary with symptoms, nor can we establish whether brain changes precede stress-related symptoms or vice versa.
Results of the current study indicate the importance of understanding how stress and its related symptoms correspond to the structural organization of the brain in emerging trauma-exposed adults. First, identification of neural markers of stress exposure as well as specific symptoms of PTSD, such as reexperiencing symptoms, could lead to more precise interventions and treatments in trauma-exposed populations. Second, discrepancies between findings reported here and prior papers underscore the necessity of examining the relationship between stress, symptoms, and white matter integrity across the lifespan. Therefore, future research should use a longitudinal experimental design to better characterize how structural changes over time relate to changes in symptoms.
Supplemental Material
Supplemental material for Structural Connectivity of the Posterior Cingulum Is Related to Reexperiencing Symptoms in Posttraumatic Stress Disorder
Supplemental material for Structural Connectivity of the Posterior Cingulum Is Related to Reexperiencing Symptoms in Posttraumatic Stress Disorder by Carissa N. Weis, Emily L. Belleau, Walker S. Pedersen, Tara A. Miskovich and Christine L. Larson in Chronic Stress
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NIH grant K01 MH086809 (PI: Larson).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.