
Abstract
Background
Diabetes-related distress (DRD) is a common psychological issue of people living with diabetes. International guidelines advise to take DRD into consideration in diabetes care but evidence for Greece is scarce. In the present study we aimed to estimate the frequency of DRD as assessed by Diabetes Distress Scale (DDS) and to examine its connections with clinical and sociodemographic characteristics among patients with type 2 diabetes mellitus (T2D) in urban primary care (PC) in Greece.
Methods
This descriptive survey included adults with a diagnosis of T2D of at least six months under medication treatment attending a novel, public urban PC unit. Patients with other forms of diabetes, dementia, and psychosis were excluded. Patients were screened for DRD with DDS instrument and correlations were made between DRD and clinical and sociodemographic characteristics.
Results
In 135 eligible participants the frequency of moderate to high levels of DRD (DDS ≥ 2) was 24.4% and of high levels of DRD (DDS ≥ 3) was 7.4%. Emotional burden (EB) subscale was significantly correlated with younger age, insulin use, duration of insulin use, and the number of insulin injections per day. Longer diabetes duration showed significant correlation with DDS total, EB, and regimen distress. Participants with lower income, sedentary lifestyle, micro-vascular complications, more episodes of hypoglycaemia, and higher levels of glycated haemoglobin (HbA1c) experienced significantly higher distress.
Conclusion
DRD screening is important in urban PC and in more susceptible patients as those on more insulin injections per day, with longer diabetes duration, higher levels of HbA1c, lower income, sedentary lifestyle, and more episodes of hypoglycaemia.
Introduction
Through a life span with diabetes, patients and their families have to adopt or change a demanding set of self-care behaviors 1 , 2 in order to achieve and maintain optimal glycaemic outcomes [glycated haemoglobin (HbA1c) <7%]. 3 These include day-to-day taking of more or less complex drug regimens, including insulin and non-insulin injections, healthy diet, frequent exercise, capillary blood checking, blood draws, foot self-care, and appointments with healthcare providers. 1 These self-care requirements may be burdensome for patients and their families; at the same time living with the fear of both acute (e.g., hypoglycaemia, hyperglycaemia) and chronic (e.g., micro- and macro-vascular) complications generates considerable psychological stress. 4 This chronic stress may result in subclinical emotional distress, like diabetes-related distress, and clinically diagnosable disorders, like depression. 4
The term diabetes-related distress (DRD) was first proposed by Polonsky et al. 5 and refers to the significant negative emotional reaction to the diagnosis of diabetes, the threat of complications, the self-management demands, and the unsupportive interpersonal relationships, including the relationships with healthcare providers. 6 Most commonly used measures for DRD are brief, self-report surveys like the Problem Areas in Diabetes (PAID) scale 5 and the Diabetes Distress Scale (DDS). 7 Assessing for DRD is important because, for example in patients with type 2 diabetes mellitus (T2D) (which accounts for the 90-95% of the total), recent research indicates that elevated levels of DRD are associated with reduced diabetes self-care, 8 poor medication adherence, 9 presence of depressive symptoms 10 and worse glycaemic outcomes (HbA1c). 8 , 9 More importantly, patients with T2D and higher levels of DRD have increased risk of cardiovascular disease11–13 and lower quality of life. 14 , 15
DRD encompasses the worries, concerns, fears, and threats associated with living with a chronic and demanding disease like diabetes. 16 DRD is an expected response to living with diabetes, or the emotional side of it that does not necessarily imply psychopathology. 16 Although for long the emotional burden of diabetes was focused on depression, observational studies in T2D patients indicate that DRD is far more prevalent and persistent than depression 17 and more closely related to diabetes self-care 18 and HbA1c.17–19
DRD can be addressed as part of a comprehensive diabetes care within the diabetes treatment setting. 16 Nevertheless, the prevalence of DRD differs across treatment settings [i.e., primary care (PC) versus secondary/tertiary care or urban versus rural healthcare]. 15 , 16 , 20 Furthermore, the approach of healthcare providers in addressing diabetes psychological issues across the levels of care might vary, with PC providers ideally situated for conducting screening and apply interventions. 21 Especially in PC, since the number of patients who are treated for diabetes grows, complementary screening for DRD and depression with self-report questionnaires has been reported to be essential and effective in a structured disease management program. 22
Screening by itself is not an intervention, but can serve as a basis to initiate a collaborative problem-solving approach. 21 Even monitoring DRD has beneficial effects, 23 so it is important for healthcare providers to exhibit interest, understanding, and awareness on DRD, irrespectively of their background. 24 In Greece in particular, the need for evidence on DRD in the urban PC is important because diabetes care is mainly offered by private practices, diabetes-specific tertiary care (DSTC), and rural PC. 25
Despite the year-by-year increasing number of publications regarding DRD, 26 little has been shown in this scientific field in Greece, with one study validating PAID scale 27 and another one comparing rural PC with DSTC. 15
The aim of our study was to assess the levels of DRD using the DDS questionnaire in T2D patients presenting in Greek public urban PC and to examine associations between sociodemographic and clinical characteristics with DRD levels.
Methods
Study Design, Setting, and Participants
This descriptive survey took place in a Local Health Team (Τ.ΟΜ.Υ.) unit of a city with population of 23.000. This unit belongs to the recently established public urban PC in Greece (funded by the Greek State and the European Union) 28 and it has a certified specific interest in the care of people with diabetes. The data was collected during August 2019-March 2020. The participants were adult ambulatory outpatients with a diagnosis of T2D for at least six months under current medication treatment registered in our unit and presenting in the study setting for any medical reason referring to diabetes. Further inclusion criteria were the following: able to understand Greek, able to complete questionnaires, and willing to participate in the study. None of the participants belonged to an ethnic minority or had any diabetic foot complication at the present examination or in the past. Patients with type 1 diabetes mellitus (T1D), latent autoimmune diabetes in adults, gestational diabetes, dementia, and psychosis were excluded.
Data Collection
Persons willing and eligible to participate were recruited by the first researcher, a PC family physician, and were asked a series of questions regarding their background data (i.e., age, marital status, years of education, employment, monthly income, smoking status, physical activity level). Other background data i.e., family history of T2D in first degree relatives, medical history, medication treatment (including the use of antidepressants and benzodiazepines even intermittently during the last month) and the number of episodes of any level of hypoglycaemia during the last six months were also recorded. Finally, data derived from the clinical examination i.e., blood-pressure, Body Mass Index (BMI) [weight (Kg)/height (m2)], waist circumference and laboratory results [i.e., HbA1c, lipid profile, creatinine, uric acid, and, when available, urine albumin creatinine ratio (ACR)] were gathered. Acceptable laboratory results were those obtained during the previous six months. The calculated low-density lipoprotein cholesterol via the Friedewald formula was not used if triglyceride values were higher than 400 mg/dL. 29 BMI categories were defined according to the World Health Organisation 29 and the threshold for an abnormal waist circumference was set at ≥102 cm for men and ≥88 cm for women. 29
The comorbidities that were recorded included: hypertension (known history or use of any antihypertensive medication), dyslipidaemia, 30 heart failure, and atrial fibrillation. Coronary artery disease, carotid artery disease (as assessed by duplex ultrasound or revascularisation), stroke or transient ischaemic attack, and lower extremity artery disease (as assessed by duplex ultrasound, or revascularisation, or self-reported intermittent claudication) were considered as macro-vascular complications. The micro-vascular complications recorded involved: known retinopathy, nephropathy (estimated glomerular filtration rate <60 ml/min/1,73m2 or ACR >30 mg/g at two visits ninety days apart), 30 and self-reported peripheral neuropathy. We qualitatively tried to approximate diabetic peripheral neuropathy with the positive answer in the question: “do you feel numbness, tingling, burning, sharp pain on feet or hands especially at night that bothers you”?
A second researcher, an appropriately trained healthcare visitor, assisted the participants answering the DDS questionnaire (dictating the questions while the participants were reading them) and collected the data about DRD blindly of the first researcher.
Instrument
The DDS was chosen because it has been never studied again in a Greek PC setting. The DDS consists of 17 items with four subscales according to the four broad domains that define DRD: emotional burden (EB) (5 items), physician related distress (PD) (4 items), regimen related distress (RD) (5 items), and interpersonal distress (ID) (3 items). 7 Answers to each item are based on a 6-point Likert scale, rated from 1 (“not a problem”) to 6 (“a very serious problem”) for the last month. The total mean item score is calculated by summing up the answers to all items and dividing by 17. The mean score of each subscale is calculated by summing up the answers to all the items in that subscale, and dividing by the particular number of items. A score of <2.0 is considered as “little or no distress”, 2.0–2.9 as “moderate distress” and ≥3.0 as “high distress.” 31 The “clinically meaningful” level for DRD is set at ≥2.0. 31
DDS was already available in Greek in the official website 32 of the original author although evidence for the validity of the Greek version is lacking. The permission of the original author 7 was obtained.
Ethical Considerations
The Declaration of Helsinki 33 ethical principles for research involving humans were applied throughout the study. The research protocol was approved by the Scientific Council of the 5th Regional Health Authority of Thessaly and Sterea (Central Greece), in which the study setting belongs (21.1.2020/89337). All potential participants were informed about the study’s purpose, the voluntary nature of their participation, and the right to withdraw at any time. All participants signed an informed consent. The data was coded and only the researchers had access to them.
Statistical Analysis
Categorical variables are expressed as numbers and percentages, and continuous variables are expressed as means with standard deviations. Non-parametric tests were used, as the data did not follow the normal distribution. The Spearman’s rank correlation coefficient was used to test the correlations between continuous variables, e.g., DDS levels (total scale and subscales), HbA1c values, age, and duration of diabetes. A moderate-strong positive/negative relationship would be considered the one with r ≥0.50 to 0.70 or ≤−0.50 to −0.70 respectively. The relationships between dichotomous variables (e.g., gender, smoking habit, insulin use) and categorical variables (e.g., income, physical activity levels) with continuous variables were tested with Mann-Whitney U tests and Kruskall-Wallis tests respectively. Statistical analysis was performed with SPSS 21.0 (IBM Corporation 2012, SPSS Statistics for Windows, Version 21.0. IBM Corp, Armonk, NY) and p-values < 0.05 were considered significant. Cronbach's alpha was found to be good for DDS (0.80).
Results
From the 161 persons firstly designed to participate one refused, and two were excluded due to either severe illness or to the development of dementia. Until the termination of the study we did not have sufficient data for 23 persons which were ruled out of the analysis. Our final sample consisted of 135 eligible T2D patients. The mean age of the participants was 68.8 years (SD 8.86, range 43-88). Patients were taking up to four different diabetes medications. The maximum number of insulin injections per day was 4. Patients had up to five diabetes-related complications. More than one out of five patients (22.9%) had at least one macro-vascular complication. Participants’ background data and clinical parameters are presented in Tables 1 and 2.
Participants’ background characteristics (n = 135).
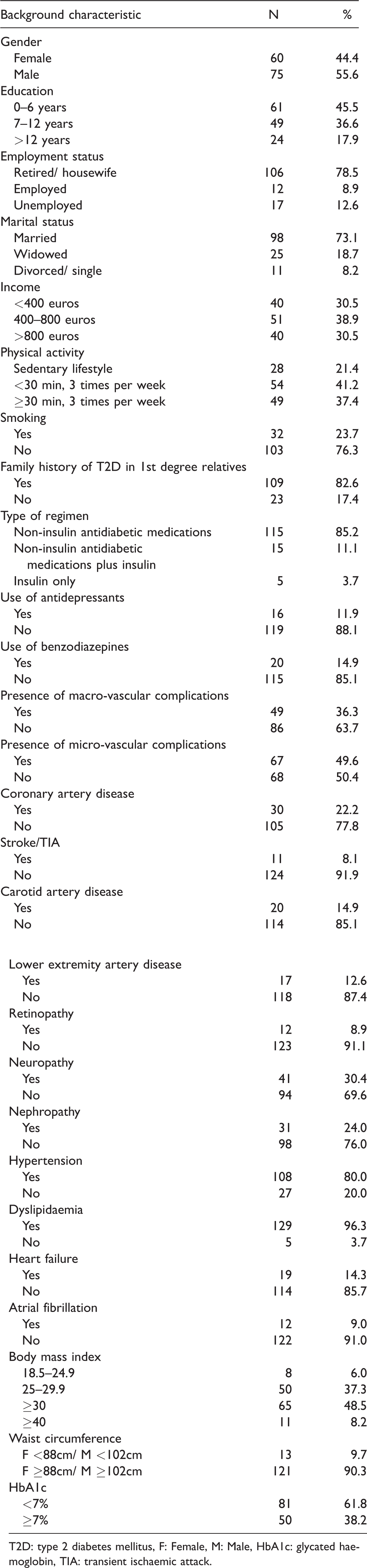
T2D: type 2 diabetes mellitus, F: Female, M: Male, HbA1c: glycated haemoglobin, TIA: transient ischaemic attack.
Descriptive results of participants’ clinical parameters.
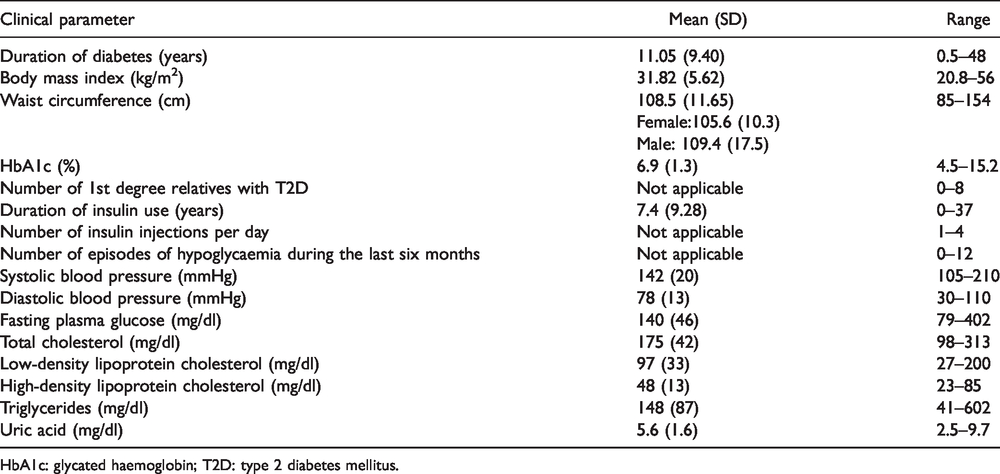
HbA1c: glycated haemoglobin; T2D: type 2 diabetes mellitus.
Participants had mean scores lower than 2.0 in all DDS subscales and in the total scale. The frequency of moderate to high levels of DRD was 24.4% (7.4% of high levels); 35.8% of the sample experienced moderate to high levels in RD, followed by 32.1% in EB, 20.9% in ID, and 10.5% in PD (Table 3).
Results in Diabetes Distress Scale.

Gender, marital status and employment status (all categories), smoking habit, family history of first degree family members with T2D, number of first degree family members with T2D, type of regimen and antidepressant or benzodiazepine use did not have an effect on total DDS levels. Age was correlated to higher levels of EB (r = −0.203, p = 0.019), the number of years of education to ID (r = −0.171, p = 0.049), and the duration of diabetes to the total DDS score (r = 0.239, p = 0.005), to the EB (r = 0.227, p = 0.008), and to the RD (r = 0.255, p = 0.003). Clinical and laboratory parameters such as BMI, waist circumference, blood pressure values, fasting plasma glucose, uric acid, and lipid levels were not correlated to DDS (total and subscales). Insulin use was correlated with EB (p = 0.002). The number of insulin injections per day (r = 0.202, p = 0.019) and the number of years of insulin use (r = 0.171, p = 0.048) were correlated to the EB. Participants with lower income (p = 0. 048) and those with sedentary lifestyle (p = 0.017) experienced higher levels of distress compared to people with higher income or any level of physical activity respectively. Patients with micro-vascular complications had higher scores in DDS total scale (p < 0.001), in EB subscale (p < 0.001), and in RD (p = 0.004). Participants experiencing more episodes of hypoglycaemia had higher scores in DDS total (r = 0.205, p = 0.017) and in the EB subscale (r = 0.279, p = 0.001). The higher the scores in DDS total (r = 0.206, p = 0.018) and in EB subscale (r = 0.226, p = 0.010), the higher were the values of HbA1c.
Discussion
DRD may adversely affects glycaemic control through deficient self-care behaviors 34 or through dysregulation of stress hormones. 35 The literature indicates that DRD, although modestly, is significantly associated with poor glycaemic control 16 , 34 and this association is probably bidirectional. 35 We also found a weak correlation between elevated scores in DDS and higher levels of HbA1c. Almost a quarter of our patients’ sample experienced moderate to high levels of DRD as assessed by DDS, while the high levels were found low, but not negligible. Both these findings should inform our practices towards the use of screening for DRD and addressing patients’ both physical as well as psychological healthcare needs.
In our PC study setting the proportion of patients with T2D affected by DRD was important although, in general, the frequency of DRD seems to be low in patients with T2D attending PC. 16 In a recent study from German PC, high levels of DRD were found to be as low as 1.2%. 36 The low prevalence of DRD in PC is also evident in studies comparing rural PC and DSTC both in Greece 15 and the Netherlands, 20 prompting some authors 20 , 36 to ask about the necessity to screen for DRD in PC. On the contrary, in a recent study from Indonesia 37 participants in PC had a 3.68 times higher likelihood of experiencing elevated levels of DRD than participants in tertiary care. The authors argued that this increase was influenced by a reformation of the health insurance system that strengthened the tiered referral procedure from PC to tertiary care that was inconvenient for patients formerly treated in tertiary care. 37 Our study was performed during a similar reformation of the public healthcare system establishing the institution of “family doctor” in urban PC. 28 This perhaps was unprecedented for Greek patients formerly used to be treated in private practices, DSTC or rural PC reflecting in notable levels of DRD. Possibly, DRD ranges in lower levels in a well-consolidated PC as in the Netherlands or in Germany and in higher levels in a newly-established PC as in Greece or in Indonesia.
Our findings that EB affects younger adults and total distress, EB and RD affect patients with longer disease duration, is in accordance with the literature. 15 , 20 , 27 , 36 This is perhaps attributed to the fact that younger people diagnosed with T2D are faced with a chronic and demanding disease in addition to many other responsibilities of daily life. Furthermore, since diabetes is a progressive disease and add-on therapy and increasing tasks of self-care are usually necessary to control blood glucose levels, patients are not unaffected by this intensification of therapy (RD).
Insulin use has been found to correlate with DRD in other studies as well. 15 , 20 , 27 The participants in the present study who were experiencing more episodes of hypoglycaemia reported higher scores in DDS, which may mean that hypoglycaemia, apart from the detrimental physical effects, 38 has adverse psychological effects as well. Besides, “psychological insulin resistance”, when adding insulin to a regimen, and “fear of hypoglycaemia”, are also two well-documented psychological effects in adults with diabetes. 39
Our finding that EB correlates to longer duration of insulin use is consistent with recent research. 40 In a study from German PC 36 a positive correlation was found between DRD and insulin dosage. In our study, the number of insulin injections per day correlated weakly to EB. This “insulin burden” (use, duration, dosage, number of injections) may contribute to a vicious circle of increasing insulin resistance (overweight/obese) and DRD. It is not to say that we should delay the initiation of insulin especially in a catabolic patient, but perhaps too much insulin is physically and psychologically futile. In the DUAL VII randomised clinical trial 41 the addition of a glucagon like peptide-1 receptor agonist (GLP-1RA) on basal insulin (fixed-ratio combination in one injection) elicited the same reduction in HbA1c as in a “basal-bolus” scheme (≤ 5 injections) with fewer episodes of hypoglycaemia and less insulin. Our study comes to add that possibly fewer insulin injections with less hypoglycaemia could contribute also to less emotional and total distress.
Since these novel agents, the GLP-1RAs, exert anti-apoptotic/neuroprotective effects in animal models 42 and exhibit potential antidepressant effect in humans, 43 to examine their possible effect on DRD could be an interesting topic for further research. Moreover, as these agents are mainly injectable and some are available in more convenient, once-weekly doses, further research on their psychological effect may elucidate whether or not the “fear of injection” is insulin-specific or relates to a non-insulin injection in general (e.g. daily or weekly injection).
In our study, participants with lower income and those with sedentary lifestyle experienced higher levels in all domains of DRD. Perhaps this highlights the importance of the holistic patient approach according to the notion that poor psychological well-being in diabetes is a prototypical example of mental-physical comorbidity and interventions that address both psychosocial and physical problems should go hand in hand. 44
The finding that EB was the dimension which correlated the most to the patients’ background characteristics perhaps signifies how much attention should be given on the patients’ support regarding emotional issues. The emotional burden of diabetes is usually estimated by self-report questionnaires that measure elevated depressive symptoms but the literature indicates that DRD correlates better with HbA1c and self-care than the depressive symptoms. 8 , 19 , 45 As DRD is more anxiety-driven, 35 further research could include complementary use of questionnaires for elevated anxiety symptoms to examine the relevance of anxiety with DRD, HbA1c, and self-care.
We decided to use the DDS to assess DRD because it applies specifically for T2D and it has been never studied again in a Greek primary healthcare environment and perhaps this is a strength of the present study. Further research on lacking validation of the Greek version of DDS could answer a basic limitation to the present study. Nevertheless, our findings need cautious generalisation due to the biases stemming from the relatively small sample size, the older mean age of the participants and the small sample of insulin users. Another limitation of our study is that of self-reporting surveys in general, as they have potential desirability bias of participants underreporting non-compliance and over-reporting distress and pain. Furthermore, as patients self-reported peripheral neuropathy, we probably overestimated this micro-vascular complication as the most prevalent. This subjective sense of daily, persistent pain perhaps contributed to the statistically significant correlation of micro-vascular complications with higher scores in DDS.
Conclusion
The finding that higher levels of DDS correlate with higher levels of HbA1c signifies that DRD is an important barrier in achieving optimal metabolic outcomes in patients with T2D. Since DRD ranges in notable levels in public urban PC in Greece, the care of patients with T2D needs to be holistic, taking into consideration the diabetes-related distress. Patients should be screened and monitored for DRD, as this is a non-costly and simple procedure, designates the problem, and serves as a platform for possible interventions. Special focus should be given to patients with higher levels of DRD and who, perhaps, are those who are younger, with longer disease duration, worse glycaemic control and on more intensified insulin regimens and present other problems as well, such as sedentary lifestyle and financial barriers. Efforts should also target to the avoidance of hypoglycaemia, as this leads to both physical and psychological adverse outcomes.
Footnotes
Declarations of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.