
Abstract
Objectives:
The psychological distress of people living with diabetes is increased and associated with poorer glycemic outcomes and self-care. We aimed to examine the frequency of depression, anxiety, and diabetes-related distress (DRD) of individuals with type 2 diabetes (T2D) in primary care (PC) and their comparative associations with clinical, self-care, and socio-demographic characteristics, testing for possible different roles on glycemic control and self-care.
Methods:
This is a cross-sectional study of 182 adults with a T2D diagnosis of at least six months, recruited between August 2019-March 2020 and May-October 2020, from an urban PC unit. Participants were screened for symptoms of depression (Patient Health Questionnaire-9 (PHQ-9)), anxiety (Generalized Anxiety Disorder-7 (GAD-7)), and DRD (Diabetes Distress Scale (DDS)). Clinical, self-care, and socio-demographic parameters were recorded.
Results:
The frequency of clinically significant symptoms of depression was 16.6%, (PHQ-9 score ⩾10), anxiety 17.7% (GAD-7 score ⩾10), and DRD 22.6% (DDS score ⩾2). All PHQ-9, GAD-7, and DDS scores intercorrelated, and higher scores were found to be associated with female gender, lower income, and prior diagnosis of depression. Higher PHQ-9 and GAD-7 scores were found to be associated with lower education, more hypoglycemia episodes, more blood glucose self-tests and antidepressant or benzodiazepine use. The retired/housewives scored significantly lower in GAD-7 and DDS compared to the unemployed participants. Higher DDS scores were associated with higher glycated hemoglobin, higher fasting plasma glucose, and insulin use. It was also noted that higher PHQ-9 scores were associated with lower uric acid levels and were significantly higher in the sedentary lifestyle group.
Conclusion:
DRD was associated with poorer glycemic outcomes while depressive symptoms were associated with lower physical activity perhaps sharing different roles for glycemic control and self-care. The psychological burden of individuals with T2D may be considered in PC.
Introduction
A challenging and multifaceted disease like diabetes mellitus is characterized by an increased prevalence of mental health comorbidities, for example, depression, anxiety, and eating disorders1,2 and by a variety of diabetes-specific psychological effects like the diabetes-related distress (DRD). 3 Reciprocally, psychological distress is considered to be a risk factor for poorer glycemic outcomes in people affected by diabetes or even to contribute to the onset of new cases. 4 During the last 20 years, the cross-national Diabetes Attitudes Wishes and Needs (DAWN, DAWN2) studies5,6 highlighted that 41% of patients report poor psychological well-being and 44.6% of them report DRD, while healthcare providers report about 61–72% of patient’s psychological problems (e.g. depression, anxiety, and stress). Emerging evidence demonstrates a substantial increase in both general and diabetes-related stress during the COVID-19 crisis with significant impact on diabetes management. 7
The gold standard for a clinical diagnosis of a depressive disorder (clinical depression, i.e., Major Depressive Disorder (MDD)) or of an anxiety disorder is a structured clinical interview, according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-V), irrespectively of cause.8,9 However, psychological distress is a negative emotional response (irritability, fear, nervousness, sadness) not necessarily pathological, toward a specific adverse or unpleasant stressor and is common among medical patients in relevance to their adjustment (successful or not) to a chronic illness. 9 In this sense, DRD refers to the worries, fears and concerns of an individual struggling with a demanding and progressive chronic disease like diabetes. 10 It is common in a busy clinical setting or in research that psychological distress is assessed by a variety of validated self-report questionnaires that measure elevated depressive symptoms (EDS or depressive symptoms) or elevated anxiety symptoms (EAS or anxiety symptoms) that can identify a likely clinical disorder based on psychometrically set cutoff scores.9,11
These self-report measures are sensitive enough to capture the severity of psychological distress but they yield many false-positive results by ignoring the cause of common non-psychiatric distress experienced by people living with diabetes, i.e. overpathologizing DRD as MDD. 12 In the continuum of emotional distress, assessing for both severity (depressive/anxiety symptoms to MDD/anxiety disorder) and cause (DRD) minimizes the confusion between the definitions and directs appropriate clinical intervention. 10 In type 2 diabetes mellitus (T2D), which accounts for the vast majority of diabetes cases, DRD and EDS have been proved to be more prevalent and chronic than MDD and clinical anxiety. 13 Furthermore, DRD has been proved to be more strongly related to glycated hemoglobin (A1C) than MDD,13–15 clinical anxiety, 13 EDS,14,16,17 or EAS 18 and to self-care behaviors than MDD.14,15
In T2D, anxiety disorders and depression are highly comorbid with each other, 19 while DRD is highly comorbid with EDS. 20 However, the relevance of DRD with EAS is less explicit, 9 and the comparative relationship of DRD and EDS with aspects of self-care behavior is rather inconclusive.16,21 In Greece, particularly, while evidence emerges for DRD,22,23 the psychological status of people living with T2D is less investigated.24,25 Given this evidence, the objective of this study was to examine the frequency of depression, anxiety, and DRD in individuals with T2D attending urban primary care (PC) in Greece and to identify the strongest associations with clinical, self-care, and socio-demographic characteristics, testing possible different roles on glycemic control and self-care.
Method
Study design, setting, and participants
This cross-sectional study took place in the Local Health Team unit, an urban PC unit with a certified specific interest in the care of people with diabetes, of a city of Greece with population of 23.000. The data were collected during August 2019-March 2020, before the first country lock-down due to the COVID-19 pandemic and May-October 2020, before the authorities imposed a second lock-down. The participants were adult ambulatory outpatients with a T2D diagnosis of at least six months, registered in the study setting and presenting for any medical reason referring to diabetes. The participants were screened for symptoms of depression with Patient Health Questionnaire-9 (PHQ-9), symptoms of anxiety with Generalized Anxiety Disorder-7 (GAD-7), and DRD with Diabetes Distress Scale (DDS). These questionnaires were used for screening and non-diagnostic purpose. Inclusion criteria were willingness to participate in the study and ability to communicate in Greek and complete questionnaires. Patients with other forms of diabetes, active cancer, dementia, and psychosis were excluded.
Data collection
Upon consent, persons eligible and willing to participate were asked a series of questions regarding their background data (i.e. age, marital status, years of education, employment, monthly income, smoking habit, physical activity level, and self-monitoring of blood glucose (SMBG) (number of blood glucose self-tests) per week). The history of prior (lifetime) depression diagnosed by a health care provider, the long-term use of an antidepressant and a benzodiazepine (even intermittently), during the last month and the number of hypoglycemia episodes during the last six months were also recorded. Finally, data derived from the clinical examination, that is, blood pressure (BP), Body Mass Index (BMI) (weight (Kg)/height (m2)), waist circumference, and recent (until up to six months before) laboratory results (A1C, fasting plasma glucose (FPG), lipid status, and uric acid (UA)) were gathered. The low-density lipoprotein cholesterol was calculated via the Friedewald formula 26 and values were not used if triglyceride > 400 mg/dL. BMI categories were defined according to the World Health Organization, 26 and the threshold for an abnormal waist circumference was set at ⩾102 cm for men and ⩾88 cm for women.
Another researcher assisted the participants in answering the PHQ-9, GAD-7, and DDS questionnaires and collected the data blindly from the other researchers.
Evaluation instruments
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a nine-item questionnaire designed for the assessment of depressive symptoms and their severity in PC. 27 The respondents are asked to answer how frequently they have been bothered during the last 2 weeks by each of the nine items (each representing a criterion of MDD in DSM-V). 28 The items are scored on a 4-point Likert-type scale rated from 0 (“not at all”) to 3 (“nearly every day”), and the sum (range: 0-27) in the PHQ-9 total score represents the severity of depressive symptoms (EDS). 28 A PHQ-9 total score of 10 or above indicates likely CD that has to be confirmed by a clinical interview.27,28 The Greek version of PHQ-9 29 is freely available, and the translation and cut off of 10 has been validated for assessing MDD in Greek rheumatologic patients. 30
Generalized Anxiety Disorder-7 (GAD-7)
The GAD-7 is a seven-item questionnaire designed for the assessment of anxiety symptoms and their severity in PC. 31 The GAD-7 is based on the DSM-IV criteria for detecting likely Generalized Anxiety Disorder but also performs moderately well for identifying panic disorder, social anxiety disorder, and post-traumatic stress disorder. 32 The respondents are asked to answer how frequently they have been bothered during the last 2 weeks by each of the seven items (each representing different symptoms of anxiety).28,32 The items are scored on a 4-point Likert-type scale rated from 0 (“not at all”) to 3 (“nearly every day”), and the sum (range: 0-21) in the GAD-7 total score represents the severity of anxiety symptoms (EAS). 28 A GAD-7 total score of 10 or above indicates a likely anxiety disorder that has to be confirmed by a clinical interview. 27 We used the freely available Greek version of GAD-7. 33
Diabetes Distress Scale (DDS)
The DDS is a seventeen-item questionnaire designed by Polonsky and colleagues18,34 which assesses DRD consisting of four subscales according to the four broad domains that define DRD: the emotional burden (EB) (5 items) (feeling overwhelmed by the demands of living with diabetes), physician-related distress (PD) (4 items) (worries about access and trust to providers), regimen-related distress (RD) (5 items) (worries about self-care and medications), and interpersonal distress (ID) (3 items) (concerns about understanding and support from family and friends). The respondents are asked to answer how frequently they have been bothered during the last month by each of the seventeen items scored on a 6-point Likert-type scale rated from 1 (“not a problem”) to 6 (“a very serious problem”). Summing up the answers to all items and dividing by 17 estimates the total mean score and summing up the answers in the items of a subscale and dividing by the number of items estimates the mean subscale score. 34 A score of < 2 is considered as “little or no distress,” 2-2.9 as “moderate distress” and ⩾3 as “high distress.” 35 DDS was already available in Greek in the official website 36 of the original author, and the permission of the original author Polonsky et al. 34 was obtained.
Ethical considerations
The Declaration of Helsinki 37 ethical principles for research involving humans were applied throughout the study. The research protocol was approved by the Scientific Council of the 5th Regional Health Authority of Thessaly and Sterea (Central Greece), in which the study setting belongs (21.1.2020/89337). All potential participants were informed about the study’s purpose, the voluntary nature of their participation, and the right to withdraw at any time. All participants gave an informed verbal consent. The data were coded, and only the researchers had access to them.
Statistical analysis
Data were analyzed with the use of the statistical software IBM SPSS (Statistical Package for the Social Sciences) Statistics (20th version). Descriptive statistics were computed in order to describe the patient sample in terms of continuous and categorical variables. Statistical significance was defined at the .05 level. The relationships between the main psychological variables (PHQ-9, GAD-7, DDS, and DDS subscales, prior depression), A1 C, self-care behaviors, and other clinical parameters as well as potentially significant within-group differences on the main variables based on socio-demographic data were explored with the use of Pearson and Spearman correlation coefficient, independent samples t-tests, Mann–Whitney U-tests, one-way ANOVAs with Bonferroni’s correction, and Kruskal–Wallis tests.
Results
From the 224 persons initially recruited, 2 refused to participate and 40 were excluded from the analysis due to insufficient data collection. The final sample consisted of 182 consecutive, eligible T2D patients, of which 135 were enrolled between August 2019 and March 2020 and 47 between May–October 2020. Five participants belonged to an ethnic minority. No participant had renal/heart/liver end-stage disease or any diabetic foot complication or was infected by SARS-COV-2 throughout the duration of the study.
The majority of the participants were male (56.6%), the mean age was 68.04 years (SD 9.23, range 43-88), and the mean duration of diabetes was 10.69 years (SD 8.92, range 0.5-48). The majority of participants (75.8%) were non-smokers. The mean duration of insulin use was 7.82 years (SD 8.35, median 6, max 37). Regarding self-care behaviors, participants performed an average of 5.01 SMBG per week (SD 5.64, median 3, range 0-35) and 78.9% of them performed some degree of physical exercise. Further participants’ background data and clinical parameters are shown in Table 1.
Participants’ background characteristics (N = 182).
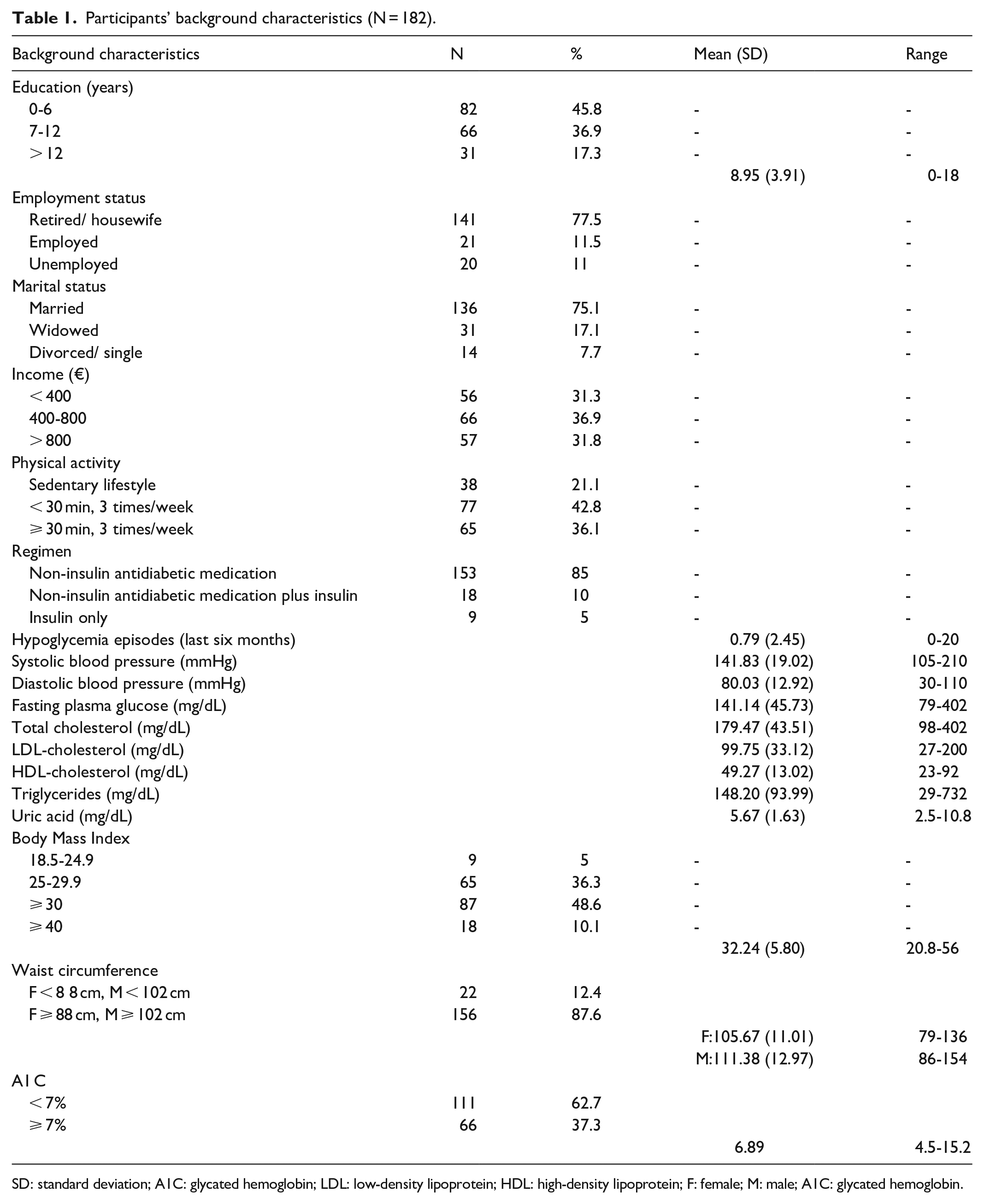
SD: standard deviation; A1C: glycated hemoglobin; LDL: low-density lipoprotein; HDL: high-density lipoprotein; F: female; M: male; A1C: glycated hemoglobin.
Throughout the study sample, the prevalence of depression (new (PHQ-9 ⩾10) and pre-existing (prior depression with PHQ-9 < 10) cases) was 26.05%. Sixteen out of 30 (53.3%) individuals exhibiting a score in PHQ-9 ⩾10 did not have a history of prior depression. Data for the participants’ psychological status are shown in Tables 2 and 3.
Descriptive statistics for psychological parameters (N = 181).

SD: standard deviation; DDS: Diabetes Distress Scale; PHQ: Patient Health Questionnaire; GAD: Generalized Anxiety Disorder.
Co-occurrence of depression-DRD, anxiety-DRD (N = 181).

DDS: Diabetes Distress Scale; PHQ: Patient Health Questionnaire; GAD: Generalized Anxiety Disorder.
Pearson correlations revealed positive associations between PHQ-9 and EB (r = .525, p < .001), PD (r = .269, p < .001), RD (r = .495, p < .001), and ID (r = 332, p < .001) and similarly, between GAD-7 and EB (r = .519, p < .001), PD (r = .270, p < .001), RD (r = .348, p < .001), and ID (r = .428, p < .001). All statistically significant associations are depicted in Table 4.
Statistically significant relationships.

DDS: Diabetes Distress Scale; PHQ: Patient Health Questionnaire; GAD: Generalized Anxiety Disorder; SMBG: self-monitoring of blood glucose; A1C: glycated hemoglobin; and ns: non-significant.
Independent samples t-tests revealed that gender had a significant effect on: PHQ-9 (t(152.07) = −3.45, p < .001)), with men scoring lower (M = 3.39, SD = 4.46) than women (M = 5.91, SD = 5.16) (p = .001); on GAD-7 ((t(179) = −2.70, p = .008)), with female patients scoring higher (M = 6.32, SD = 5.12) than men (M = 4.26, SD = 5.07); and on DDS (t(152.31) = −2.46, p = .015)), with women scoring higher (M = 1.73, SD = .74) as compared to men (M = 1.47, SD = .63).
Monthly income had a significant effect on PHQ-9 (Welch’s F (2,113.62) = 6.92, p = .001, η2 = .07), with participants of low-income (< 400 €) scoring higher (M = 6.20, SD = 5.41) as compared to those of higher income status (> 800€) (M = 2.84, SD = 4.13) (p = .001); on GAD-7 (F(2,175) = 4.65, p = .011, η2 = .05) with low-income patients (M = 6.84, SD = 5.60) scoring higher than patients of higher income (M = 3.95, SD = 4.70) (p = .009); and on DDS (Welch’s F (2,110.66) = 5.90, p = .004, η2 = .05) as the former group (M = 1.79, SD = .78) showed higher levels than the latter (M = 1.39, SD = .45) (p = .006). Regarding employment status, Kruskal–Wallis tests revealed a statistically significant difference across the groups studied in DDS (X2(2, n = 181) = 6,33, p = .042)), with retired/housewives (Md = 1.29) scoring lower than unemployed participants (Md = 1.73), as well as in GAD-7 (X2(2, n = 181) = 6,54, p = .038)), with retired/housewives (Md = 4.00) scoring lower than unemployed participants (Md = 7.00).
Significant positive relationships were observed between A1 C and DDS total (r = .222, p = .003) and three of subscales: EB (r = .217, p = .004), RD (r = .166, p = .028), and ID (r = .169, p = .025) and between FPG and DDS (r = .218, p = .007). The application of one-way ANOVAs further revealed that physical activity had a significant effect on PHQ-9 (Welch’s F(2,90) = 8.10, p < .001, η2 = .09) as patients leading a sedentary lifestyle showed higher levels of PHQ-9 (M = 7.00, SD = 5.31) as compared to both subsequent groups (M = 4.32, SD = 5.00) (p < .001), (M = 3.03, SD = 3.80) (p < .001), respectively.
The presence of prior diagnosis of depression had an effect on PHQ-9 (t(33.49) = −5.13, p < .001) as participants with such a diagnosis scored higher (M = 9.45, SD = 5.92) than those without a diagnosis (M = 3.55, SD = 4.13); on GAD-7 (t(33.45) = −4.45, p < .001) with the former (M = 9.45, SD = 5.79) scoring higher than the latter (M = 4.37, SD = 4.67); and on DDS (t(176) = −2.17, p = .031) with previously diagnosed (M = 1.84, SD = .76) scoring higher than non-diagnosed patients (M = 1.54, SD = .76). Mann–Whitney U-tests revealed that the use of antidepressant therapy had an impact on both PHQ-9 (U = 839.50, z = −3.01, p = .003) and GAD-7 (U = 760.50, z = −3.37, p = .001). Patients receiving antidepressants scored higher on PHQ-9 (Md = 6.50) and GAD-7 (Md = 8.50) than those who did not receive (Md = 3.00 and Md = 3.00, respectively). Benzodiazepine therapy also had a significant effect on PHQ-9 levels (U = 1485.50, z = −2.81, p = .005) and on GAD-7 levels (U = 1691.50, z = −1.99, p = .046). Patients under therapy scored higher on PHQ-9 (Md = 6.00) and on GAD-7 (Md = 7.00) as compared to those who did not receive benzodiazepine (Md = 3.00 and Md = 4.00, respectively).
Finally, insulin use had an effect on DDS total (t(34,23) = −2,49, p = .018)) with insulin users scoring higher (M = 1.92, SD = .78) than non-users (M = 1.53, SD = .65). Age, marital status, smoking status, lipid status, BMI, waist circumference, and systolic BP did not have an effect on any of the main psychological variables.
Patients recruited before the COVID-19 crisis did not show statistically significant differences in their psychological status, except for PHQ-9 levels (t(179) = 2.10, p = .037)) as patients evaluated before COVID-19 crisis showed higher levels of PHQ-9 (M = 4.93, SD = 4.93) than those recruited during the crisis (M = 3.19, SD = 4.74).
Discussion
The psychological status of individuals with T2D that comprised our PC study sample was characterized by increased frequency of clinically significant symptoms of DRD (DDS ⩾ 2) (22.6%), followed by noteworthy levels of clinically significant symptoms of anxiety (GAD-7 ⩾ 10) (17.7%) and depression (PHQ-9 ⩾ 10) (16.6%). A more prominent psychological burden was reported in a recent study 25 performed in a diabetes-specific clinic (DSC) in Northern Greece that found a 50.6% of psychological distress in people with T2D. Another very recent Greek study 23 in a similar setting and population showed that the mean levels of DRD (2.2) (measured with DDS) were 1.36 times higher than that reported (1.62) in PC 22 before the COVID-19 crisis. It is usual for psychological distress to be more prevalent in individuals screened in DSCs than in PC perhaps because the former treats more complicated cases 4 or concerned patients 24 than the latter. Nevertheless, regarding depression relating to diabetes, some authors. 38 suggest that it is neither effective nor ethical to screen for this in any health care setting, without ensuring adequate diagnosis and treatment is available. A secondary, but equally important finding of the DAWN study 5 was that the PC providers were significantly more efficient in evaluating and offering support to the psychological problems of patients with diabetes, compared to the diabetes specialists. Consequently, perhaps PC, with the implementation of collaborative care protocols,11,39 may provide an important basis for a comprehensive approach of mental health issues in diabetes as DSCs.
The frequency of clinically significant symptoms of depression found in our study sample (16.6%) was close to that found (15.3%) in a community-based study 16 but far below the 33.4% previously reported in a Greek DSC. 24 Similarly, the levels of clinically significant symptoms of anxiety (17.7%) were far below the 42.2% reported for T2D in a meta-analysis mainly from tertiary care. 40 These differences perhaps confirm the lower psychological distress of T2D patients attending PC compared to DSCs. 4 Since the co-occurrence of depression in diabetes is incidental or mutually causative, 9 we aimed to estimate the prevalence of depression; this was found to be 26.05%, thus approaching the 28% reported in T2D in a recent meta-analysis. 41
Low education is a well-established social risk factor for the onset of depression 9 that is confirmed in the present T2D study sample, as lower education was associated with higher PHQ-9 and GAD-7 scores. Similar negative association was observed between the number of hypoglycemia episodes and both PHQ-9 and GAD-7 scores perhaps reflecting the connection between two dramatic experiences, a physical like hypoglycemia and a psychological like depression or anxiety. Regarding employment status, unemployed participants, compared to retired/housewives, showed higher levels of DRD and anxiety, which may indicate that unemployment, may present an extra psychological stressor among people with diabetes. In contrast, all psychological variables related to female gender, prior depression, and lower income so maybe these characteristics deserve our special clinical attention. The psychological vulnerability of women13,19,20,24,40,41 and of people with lower income 25 has also been reported in other studies as well as of people with a history of depression in a study from PC. 42
Regarding the medications, antidepressant or benzodiazepine use was associated with PHQ-9 and GAD-7 levels, while insulin use was associated with DDS levels. This possibly differentiates depression/anxiety from DRD in a way that the former are psychiatric conditions-perhaps deficiently treated in this study sample while the latter is a diabetes-specific psychological effect like the well-characterized “psychological insulin resistance.” 3
The significant correlation between PHQ-9 and GAD-7 scores found in the present study is consistent with the fact that depression and anxiety are internalizing disorders highly comorbid with each other in T2D. 19 Significant relationships were also evident between DDS (and subscales) and both PHQ-9 and GAD-7 scores which conceivably means that although they are conceptually different9,10 they exhibit some clinical overlap. 9 In the present T2D study sample, only DDS (EB, RD, and ID) scores showed a weak correlation with A1 C, while PHQ-9 and GAD-7 scores did not. This is also evident in many studies14,16–18,43 as well and perhaps confirms that these constructs are distinct with independent relationships to glycemic outcomes. 12 In this regard, in two studies44,45 implementing a diabetes self-management education intervention in T2D patients, the reduction in DRD and not in depressive symptoms was significantly associated with improvement in A1 C levels. Furthermore, studies using mediation analysis indicate that DRD serves as a pathway through which depressive46,47 and anxiety 18 symptoms may adversely affect A1 C.
The positive weak correlation of DDS scores with A1 C and FPG could be explained by a proposed mechanism through which DRD might directly dysregulate the hormones of stress leading to hyperglycemia. 9 The observed negative correlation of PHQ-9 score with UA levels is consistent with a recent finding from the general population that UA levels were significantly lower in patients with depression compared to controls. 48 A possible explanation is that serum UA is a strong antioxidant and its depletion leads to increased oxidative stress that links to neurodegenerative diseases and depression. 48
Finally, with reference to the aspects of self-care behavior, the present study showed a positive correlation of PHQ-9 and GAD-7 scores with SMBG which could indicate that SMBG is experienced by people with T2D more as a burdensome rather than as a reassuring task of self-care. On the contrary, in two studies21,43 comparing depressive symptoms and DRD with aspects of self-care behavior, only depressive symptoms were associated with lower self-care21,43 and less frequent exercise. 21 Furthermore, the significant inverse association of depressive symptoms with physical activity in T2D is well-established in a recent meta-analytic review. 49 The latter are consistent to the finding of the present study that DRD or anxiety symptoms did not statistically differ between the levels of physical activity while depressive symptoms were more prominent among subjects leading a sedentary lifestyle. This perhaps confirms a proposed indirect way through which depressive symptoms might adversely affect glycemic control via deficient self-care behavior. 9
This study has several limitations including that one-third of our study sample was recruited during the COVID-19 crisis, which negatively influenced patients’ mental health and access to health care. 7 However, a proactive management of diabetes and mental health comorbidities during the COVID-19 crisis has been acknowledged and implemented through remote counseling and monitoring. 50 Other limitations involve the selection biases resulting from face-to-face consultation and exclusion of participants with missing data. The negative association of UA with PHQ-9 levels should have been corrected for the use of antidepressants that interfere with the levels of UA, and this is also a limitation. Further limitations include the lack of validation of DDS and GAD-7 questionnaires in the Greek language, the lack of a standardized tool to measure physical activity and self-care, the lack of power analysis for sample size calculation and the biases stemming from the self-report questionnaires in general (social-desirability or recall bias) that cannot substitute a structured clinical interview. An important ethical limitation is the verbal, instead of written, informed consent obtained. Thus, our results should be interpreted with caution.
Conclusion
The psychological distress experienced by people with T2D, although lower in PC than in DSCs, is an element that we may consider in terms of a holistic approach provided in PC. In this study, only DRD was associated with higher A1 C and FPG, while only depressive symptoms were associated with physical inactivity perhaps presenting different roles for glycemic control and self-care behavior. All psychological variables correlated with each other and were especially high among women, people with lower income, and prior depression. The unemployed were more likely to be affected by anxiety symptoms and DRD compared to retired/housewives. Both depressive and anxiety symptoms increased as educational level decreased and the number of hypoglycemia episodes and SMBG also increased. Finally, depressive symptoms were associated with lower levels of UA, a finding consistent with recent research. This requires further investigation but inappropriate lowering of UA may be avoided.
Supplemental Material
sj-doc-2-smo-10.1177_20503121221096605 – Supplemental material for Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: Different roles for glycemic control and self-care
Supplemental material, sj-doc-2-smo-10.1177_20503121221096605 for Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: Different roles for glycemic control and self-care by Kyriakos Kintzoglanakis, Anna Gkousiou, Paraskevi Vonta, Agisilaos Sagmatopoulos and Panagiota Copanitsanou in SAGE Open Medicine
Supplemental Material
sj-docx-1-smo-10.1177_20503121221096605 – Supplemental material for Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: Different roles for glycemic control and self-care
Supplemental material, sj-docx-1-smo-10.1177_20503121221096605 for Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: Different roles for glycemic control and self-care by Kyriakos Kintzoglanakis, Anna Gkousiou, Paraskevi Vonta, Agisilaos Sagmatopoulos and Panagiota Copanitsanou in SAGE Open Medicine
Footnotes
Acknowledgements
The authors would like to thank Professor William Polonsky for the permission to use the DDS questionnaire, Mrs Beverley Gray Linnecor MSc, BSc (Hons), Guernsey, Channel Islands, for the language check of the manuscript and the participants of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Scientific Council of the 5th Regional Health Authority of Thessaly and Sterea (Central Greece), number of license 21.1.2020/89337.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The verbal type of informed consent obtained in this study was approved by the Scientific Council of the 5th Regional Health Authority of Thessaly and Sterea (Central Greece).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.