
Abstract
Purpose:
The purpose of this study is to evaluate primary care provider satisfaction and perceived impact of clinical pharmacy services on the disease state management in primary care.
Methods:
A cross-sectional survey with 24 items and 4 domains was distributed anonymously to pharmacy residency program directors across the United States who were requested to forward the survey to their primary care provider colleagues. Primary care providers were asked to complete the survey.
Results:
A total of 144 primary care providers responded to the survey, with 130 reporting a clinical pharmacist within their primary care practice and 114 completing the entire survey. Primary care providers report pharmacists positively impact quality of care (mean = 5.5 on Likert scale of 1–6; standard deviation = 0.72), high satisfaction with pharmacy services provided (5.5; standard deviation = 0.79), and no increase in workload as a result of clinical pharmacists (5.5; standard deviation = 0.77). Primary care providers would recommend clinical pharmacists to other primary care practices (5.7; standard deviation = 0.59). Primary care providers perceived specific types of pharmacy services to have the greatest impact on patient care: medication therapy management (38.6%), disease-focused management (29.82%), and medication reconciliation (11.4%). Primary care providers indicated the most valuable disease-focused pharmacy services as diabetes (58.78%), hypertension (9.65%), and pain (11.4%).
Conclusion:
Primary care providers report high satisfaction with and perceived benefit of clinical pharmacy services in primary care and viewed medication therapy management and disease-focused management of diabetes, hypertension, and pain as the most valuable clinical pharmacy services. These results can be used to inform development or expansion of clinical pharmacy services in primary care.
Introduction
The role of today’s pharmacist continues to evolve with an increasing proportion of pharmacists practicing globally in clinical settings that are distinct from the traditional dispensing role. Although previously unfavored, pharmacists assuming clinical roles have almost become a necessity in light of the recent growth in the aging population and larger focus on primary health care.1,2 Almost half a century ago, pharmacists were considered closer to the role of a technician rather than a professional by physicians, patients, and even fellow pharmacists. 3 Pharmacists were thought to not be living up to their fullest potential. 3 The shift from the dispensing role has been in motion for decades, which facilitates pharmacists capitalizing on their expertise to optimize patient care 1 in a fashion that complements care provided by other clinicians, including physicians, mid-level practitioners, and nurses.
Prior assesssment on the impact of clinical pharmacists on patient care clearly supports value. 4 Clinical pharmacists have also demonstrated improvements in clinical outcomes and quality of life for patients in low- and middle-income countries with chronic conditions, including diabetes, hypertension, and asthma. 5 Integration of a clinical pharmacist into an inner city primary care clinic setting improved quality measures such as controlled hypertension, appropriate usage of aspirin, statin, asthma medications, evidence-based pharmacist consultations, and medication consultations. 6 Pharmacist-run diabetes clinics report significant improvements in glycemia,7–9 which may be attributed to timely medication management and close follow-up by the clinical pharmacist. 7 The benefits of pharmacist-managed medications also extend to other chronic disease states, including blood pressure control,4,10 smoking cessation rates, 11 chronic kidney disease, 4 cardiovascular disease, 4 dyslipidemia, 4 polypharmacy, 4 and depression.4,12
Additionally, patient satisfaction with clinical pharmacists has been well established by previous studies.13–17 Interaction with a pharmacist during a hospital stay improved patient satisfaction with the amount and clarity of information provided regarding medication therapy and improved overall satisfaction with the medical care while hospitalized. 18 When considering pharmacists with prescribing capabilities, patients report satisfaction with the pharmacists’ management of hypertension, coronary heart disease prevention, asthma, chronic obstructive pulmonary disease (COPD), diabetes, family planning, and infections. 19
Some studies have also assessed provider satisfaction with clinical pharmacy services. An early study in 1986 found physicians were antagonistic toward the expansion of clinical pharmacy roles in the community and that nurses felt threatened by clinical activities that encroached on their roles. 1 Physicians were previously thought to be opposed to pharmacists performing autonomous decision-making tasks, which were largely influenced by limited exposure to clinical pharmacy services and lack of understanding of the pharmacists’ scope and capabilities. 20 However, more recent studies have reported positive provider satisfaction with pharmacy services and clinical pharmacists in various clinical settings, including pharmacist-led annual wellness visits, anticoagulation, and lipid clinics.14,15,21,22 One study looking at the impact of a collaborative care model on depression in the primary care setting reported high approval ratings from providers. 12 This change in primary care provider (PCP) perception of pharmacists was also observed before and after integration of clinical pharmacists into family practices. 23 In total, 36 PCPs responded to a survey regarding their perception of their own and pharmacists’ contributions to medication management before and after integration of clinical pharmacists into their practice. Initially, PCPs underestimated clinical pharmacists’ role, which gradually evolved to PCPs recognizing the expertise and competence of the clinical pharmacists as the integration of clinical pharmacy services progressed. 23 Lack of interaction with clinical pharmacists outside of the community setting may have contributed to lower assigned values initially. This shift in provider satisfaction and assignment of value over time highlights the importance of promoting clinical pharmacy services and may be reflective of pharmacists’ expanded and more clinical role on patient care teams. Prior to integration of clinical pharmacists in primary care, PCPs generally report positive opinions regarding the idea of having a pharmacist in primary care to provide services such as medication review, medication information, quality prescribing initiatives, and education to patients and themselves. 24 Previous studies have looked at provider satisfaction with specific clinical pharmacy services implemented within a primary care setting.12,14,15,21,22 However, there is limited information describing overall provider satisfaction or perceived impact on patient care of clinical pharmacists who are already integrated in primary care settings and performing multiple clinical pharmacy services. Additionally, information on which clinical pharmacy services are most valued by PCPs is also lacking.
The American Association of Medical Colleges predicted a significant shortage in primary care physicians by 2025. 25 In response, the workforce for primary care nurse practitioners and physician’s assistants are projected to grow and increase by 30% and 58% by 2020, respectively; however, even with the predicted growth of mid-level providers, there is still a potential for a shortage. 26 Clinical pharmacy services may help to alleviate the workload for providers to allow for more time for patient care activities. Understanding provider satisfaction and perceptions of specific pharmacy services is needed and can assist with tailoring the expansion of clinical pharmacy services.
Objectives
The objectives of this study were to describe the types of clinical pharmacy services currently offered in primary care and evaluate PCP satisfaction and perceived impact of clinical pharmacy services on the disease state management in primary care.
Methods
A 24-item survey was developed by the authors. Prior surveys were used as a template for the development of the demographic and clinical characteristic questions, while questions pertaining to provider satisfaction and perception on impact of care were developed de novo, given a paucity of pertinent questions published in the literature. Questions were developed with the intent to be multiple choice or select all; therefore, numeric values were reported in ranges. The survey underwent cognitive testing with 12 PCPs to assess for content validity. These PCPs were primarily physicians with one mid-level practitioner who all practiced within a primary care clinic and had a clinical pharmacist at the practice setting. They were not actively excluded from the study. Revisions were made based on the feedback received from the PCPs. Questions were categorized into four domains and included Likert scale questions with a range of 1–6 (1 = strongly disagree; 6 = strongly agree). Domain 1 included demographic and clinical characteristic questions such as practice setting/location and patient volume, classification of practice site, provider characteristics, and pharmacy presence. Domain 2 included questions to describe the types of clinical pharmacy services that were available at the PCPs’ practice. Domain 3 assessed PCP perception of the impact of clinical pharmacy services on quality of patient care. Domain 3 also asked PCPs to rank the top 5 general and top 5 disease-focused clinical pharmacy services that they perceived to have the greatest impact on patient care. Domain 4 assessed provider satisfaction with clinical pharmacy services.
The survey was distributed electronically using Qualtrics, an online survey program. Given barriers to obtaining a list of PCP email addresses, the survey was distributed to pharmacy residency program directors (RPD) across the United States, who were requested to forward the survey link to their PCP colleagues. A complete list of RPDs was obtained from the American Society of Health-System Pharmacists (ASHP) directory of residency listings. The survey was distributed to all RPDs and was not limited to those who practiced in primary care. The survey was anonymous; thus, it was not possible to track which RPDs or how many RPDs forwarded the survey to their PCP colleagues. However, PCPs were able to provide their contact information and the contact information of the person who forwarded the email to them in order to be entered into a random drawing to receive a small monetary incentive. The monetary incentive was in the form of a gift card which was awarded to five PCP responders and five individuals who forwarded the survey to PCP responders and was used to increase response rate. All recipients were picked randomly using an electronic random number generator.
Providers were asked to complete different portions of the survey depending on whether they practiced in primary care and whether they had a clinical pharmacist in their practice. Only providers who indicated they practiced in primary care and had a clinical pharmacist in their practice were able to complete the entire survey. Providers who identified themselves as PCPs without a clinical pharmacist in their practice were able to complete only the demographic questions in domain 1.
The survey was open for 4 weeks with a reminder email sent at the end of the second week. Responders were required to answer all questions in order to submit the survey. A postcard consent was included in the distribution email with a link to the electronic survey. Written consent was not obtained from responders. This study was deemed exempt by the Colorado Multiple Institutional Review Board.
Statistical analysis
Survey responses were summarized by frequency of response for provider demographics and clinical characteristics. PCP rankings of general and disease-focused clinical pharmacy services provided were summarized by mean ranking and standard deviation (SD) for each response option (e.g. medication therapy management (MTM)); services ranked highest by a PCP were assigned a 5, while services ranked lowest were assigned a 1, and services not ranked in the top 5 were assigned a 0. PCP perception responses for each question pertaining to survey domain 3 (Perception of Pharmacy Service Impact on Quality of Patient Care) and domain 4 (Satisfaction with Pharmacy Service) were summarized by mean and SD, and Cronbach’s alpha was used to evaluate the internal consistency of responses to domains 3 and 4. An alpha of 0.8 or higher was used as an indication of good internal reliability between responses within a given domain, and a mean score was calculated for each domain. A small number of factors hypothesized to influence PCP perception and satisfaction were evaluated using two-sample t-tests or one-way analyses of variance (ANOVAs); PCP Perception of Pharmacy Service Impact on Quality of Patient Care was summarized as a mean score based on responses from four questions within domain 3, and PCP Satisfaction with Pharmacy Service was summarized as a mean score based on responses from five questions within domain 4. Mean scores were then compared by PCP type (physicians vs mid-levels and other), PCP setting (classified by primary setting as academic, federally qualified health center (FQHC), or other), number of years practicing (0, between 0 and 15, and 15 or greater), how a pharmacist conducts practice (in person vs other), and prescribing abilities of pharmacist (prescribes in some manner vs no prescribing abilities). Analyses were performed using version 9.4 of the SAS/STAT™ software, Copyright © 2013, SAS Institute, Inc.
Results
The survey was distributed to 1603 RPDs who were instructed to forward the survey to PCP colleagues. From 23 June to 21 July 2015, 144 PCPs responded to the survey. The majority of these PCPs were physicians who had completed a residency and/or fellowship or resident physicians (83%). Most responders were practicing in an academic center, community, and/or FQHC (52%, 27%, and 22%, respectively), with the majority practicing in an accredited patient-centered medical home (PCMH; 85%). PCPs reported an average age of 36–45 years, seeing an average of 13–48 patients a week, and 59% of the PCPs were female. Their practices were also likely to have comanagement services such as mental or behavioral health sciences (64%), case or care management (67%), or social work (70%). Of the 144 PCPs who responded, 130 (90%) had a clinical pharmacist within their practice. Table 1 describes the demographic and clinical characteristics of the PCPs who responded to the survey.
Provider demographics.
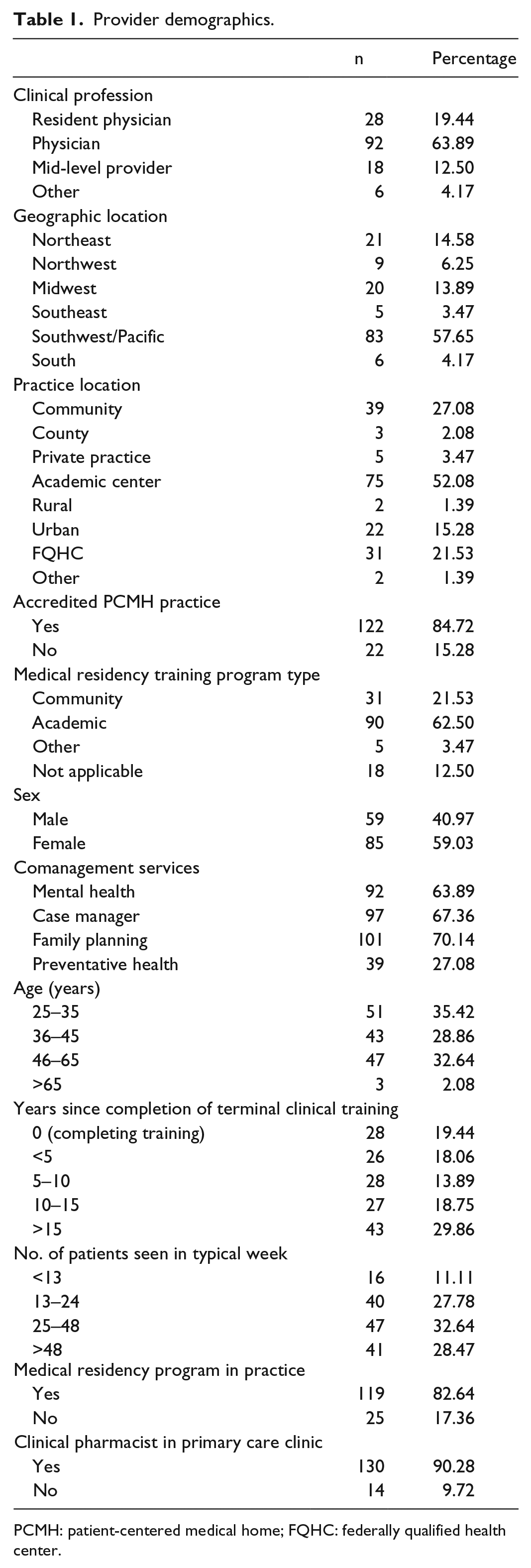
PCMH: patient-centered medical home; FQHC: federally qualified health center.
Description of pharmacy services in primary care
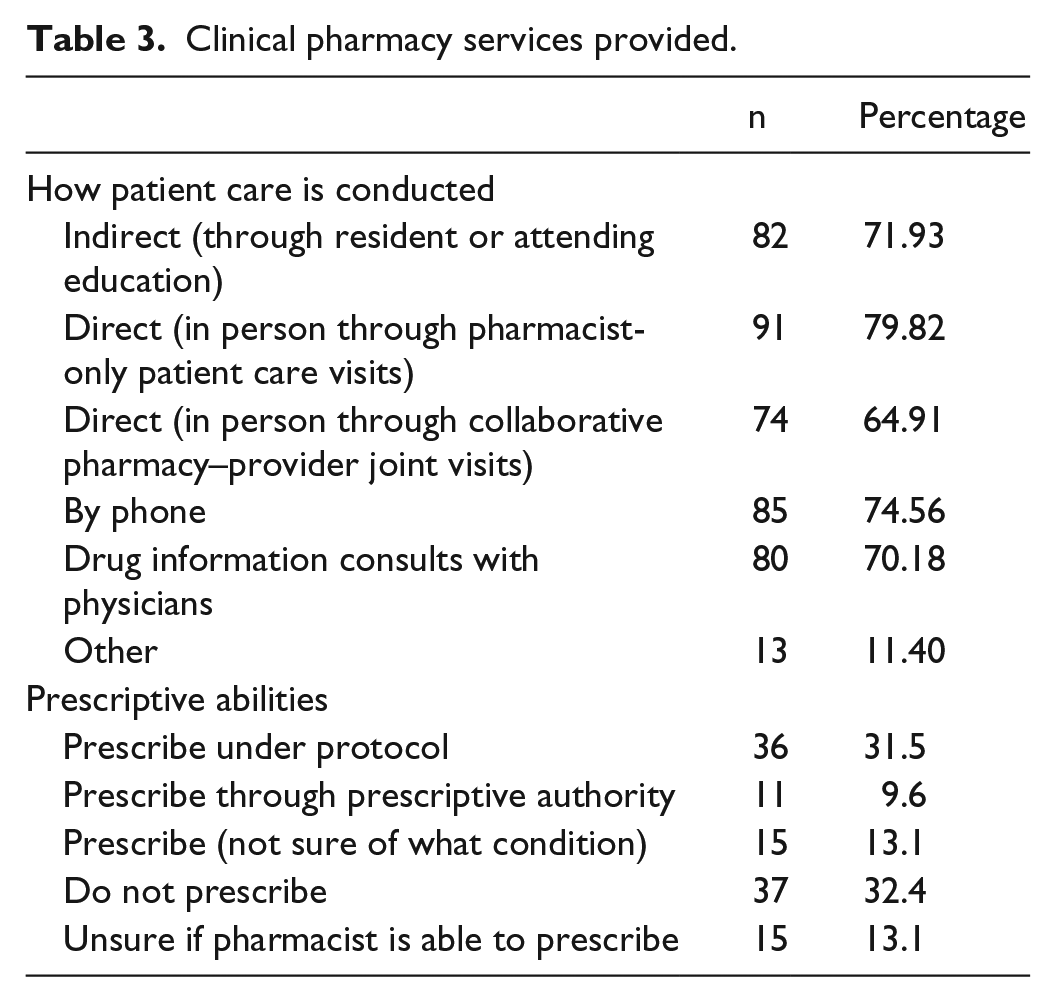
A total of 114 of the 130 PCPs had a clinical pharmacist in their practice and completed the survey in its entirety. The remaining PCPs did not complete the entire survey and were not included in the analysis. Table 2 describes the presence and utilization of clinical pharmacists within primary care settings as reported by the PCPs. The majority of PCPs (82%) reported one or two clinical pharmacists in their practice and 72% reported they consulted or referred patients to the pharmacist(s) zero to five times per week. Approximately half of PCPs indicated that the clinical pharmacists in their practice prescribed under various conditions. Table 3 describes how clinical pharmacists conduct patient care. PCPs indicated the most common pharmacy services offered were MTM or comprehensive medication review (CMR), diabetes disease-focused management, medication reconciliation, and drug information resources. MTM or CMR was defined in the survey as “not diseased-focused, but a comprehensive review of all medications.” Table 4 describes the types of clinical pharmacy services provided in primary care as reported by the PCPs.
Pharmacy characteristics within PCP setting.

PCP: primary care provider.
Clinical pharmacy services provided.
Types of pharmacy services available in primary care.
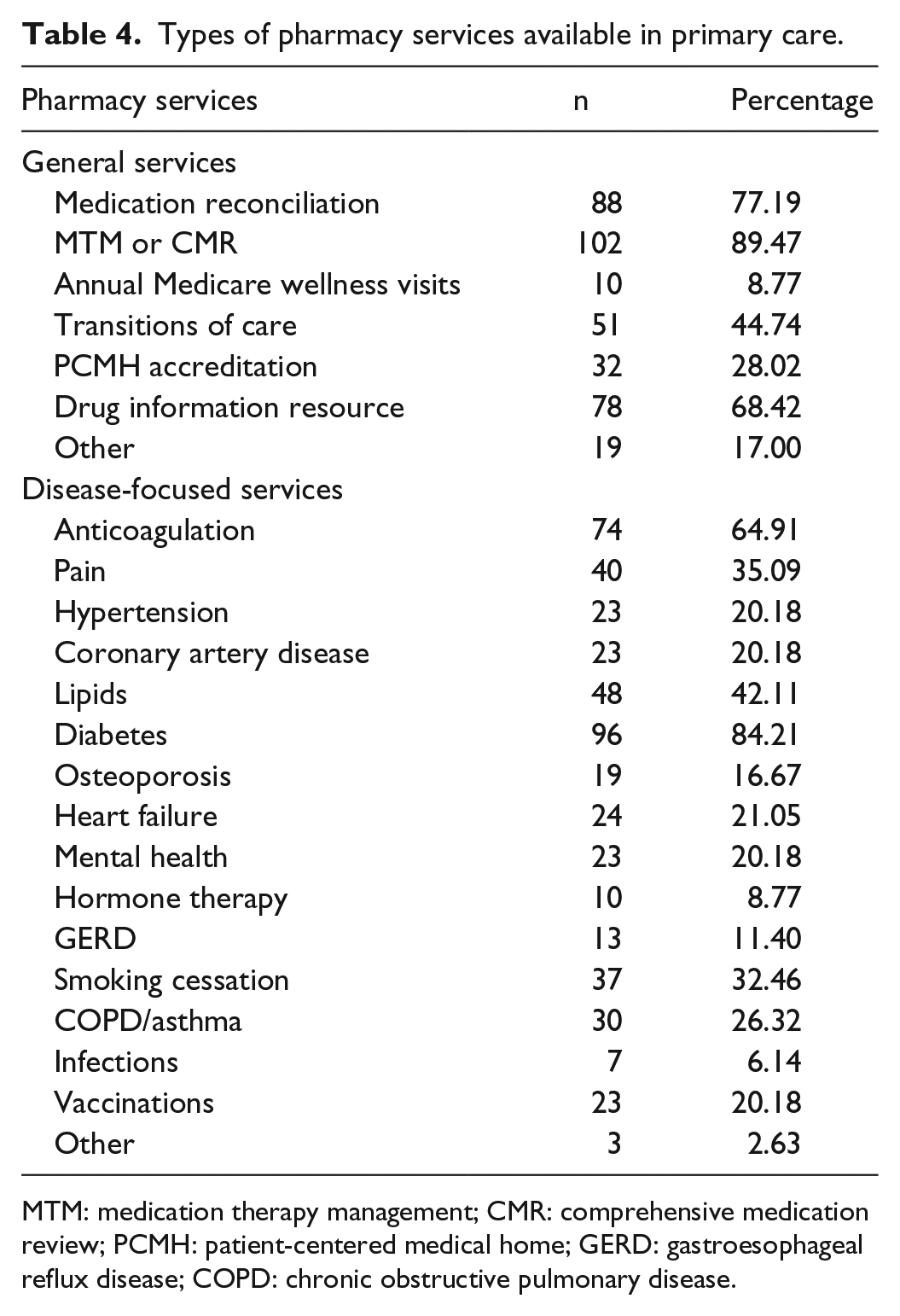
MTM: medication therapy management; CMR: comprehensive medication review; PCMH: patient-centered medical home; GERD: gastroesophageal reflux disease; COPD: chronic obstructive pulmonary disease.
PCP-perceived impact of pharmacy services on patient care
Cronbach’s alpha coefficient for internal consistency of questions regarding clinical pharmacy service on quality of patient care was 0.92. The overall mean score on the Likert scale for impact of the clinical pharmacy service on quality of patient care was 5.5 with an SD of 0.72. PCPs agreed or strongly agreed that the quality of their patients’ health care improved due to the involvement of a clinical pharmacist (mean = 5.5, SD = 0.74), clinical pharmacists improved the quality of the medication decisions they make (mean = 5.5, SD = 0.84), and play an integral part in medication management for patients whose care they are involved in (mean = 5.5, SD = 0.79). Additionally, PCPs agreed or strongly agreed that clinical pharmacists provided patients with a unique and valuable service that could not be achieved to the same extent by a nonpharmacy provider (mean = 5.5, SD = 0.81).
The top five clinical pharmacy services that PCPs perceived to have the greatest impact on patient care were as follows in the descending order: MTM, disease-focused management, medication reconciliation, drug information resource, and transitions of care. The top five disease-focused clinical pharmacy services that PCPs perceived to have the greatest impact on patient care were as follows in the descending order: diabetes, hypertension, pain, mental health, and heart failure. Of note, anticoagulation was not included in the original service options and was most frequently noted in the free text “other” section of the survey most often (89% of those who answered “other”). Figure 1 summarizes PCP rankings of the top five general and top five disease-focused clinical pharmacy services perceived to have the greatest impact on patient care.
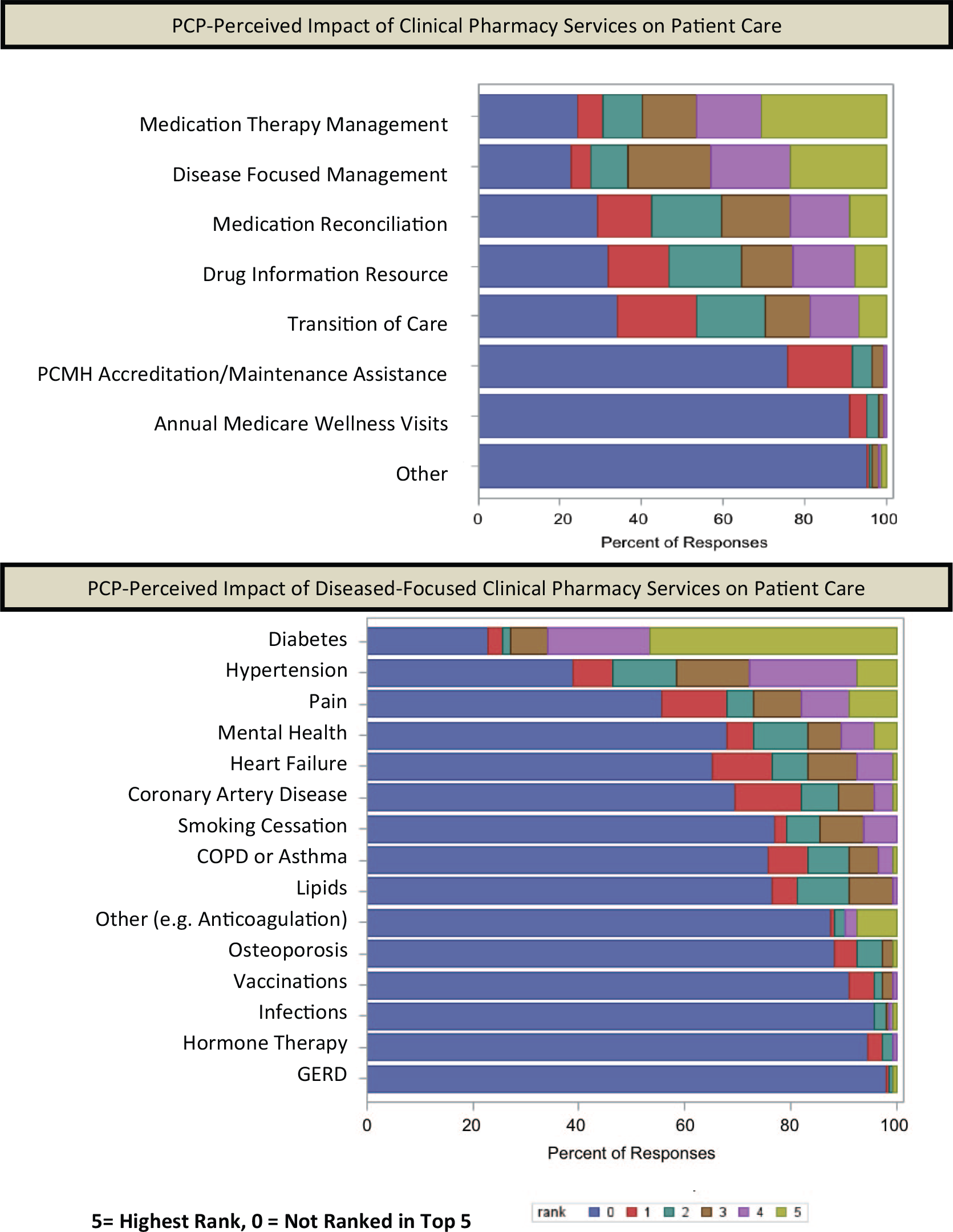
PCP-perceived impact of specific types of pharmacy services.
PCP satisfaction with pharmacy services
Cronbach’s alpha coefficient for internal consistency of questions regarding PCP satisfaction with clinical pharmacy services was 0.87. The overall mean score on the Likert scale for satisfaction with clinical pharmacy services was 5.5 with an SD of 0.79. PCPs were satisfied and appreciated pharmacist recommendations regarding medication decisions for patients (mean = 5.6, SD = 0.67) and agreed or strongly agreed that their workload did not increase due to having clinical pharmacist(s) on the primary care team (mean = 5.5, SD = 0.77). PCPs also agreed or strongly agreed that they would recommend clinical pharmacist(s) to other primary care practices that do not currently have one (mean = 5.7, SD = 0.59) and their provider colleagues utilized the clinical pharmacist(s) to assist with the medication management of their patients (mean = 5.3, SD = 0.74). PCPs agreed that they are able to spend more time on patient care activities that are related to their area of expertise as a result of the clinical pharmacist (mean = 5.1, SD = 1.1).
Factors influencing PCP perception and satisfaction
When looking at differences between certain demographics, PCPs who completed the survey and identified themselves as mid-level or “other” provider type were marginally more satisfied with clinical pharmacists when compared to physicians (including resident physicians; mean of 5.7 and 5.4, respectively, p = 0.0459). Additionally, when compared to clinical pharmacists who have prescribing privileges, PCPs reported no difference in perceived impact on patient care or satisfaction with clinical pharmacy services. There was a trend towards PCPs in an academic or FQHC practice setting perceiving greater impact of the clinical pharmacist on patient care compared to other practice settings, but this did not reach statistical significance (mean of 5.6, 5.6, and 5.3, p = 0.0690). There was no observed difference in PCP perception of impact on patient care or satisfaction with clinical pharmacy services when comparing how a pharmacist conducts their care (in person vs other) or how long the PCPs were practicing clinically (years of experience practicing). Additional ad hoc analyses were performed to better understand factors influencing PCP perception and satisfaction. Specifically, we investigated whether perception and satisfaction were associated with the number of times a PCP refers a patient or consults with a pharmacist during a given week. Two-sample t-tests were performed for these analyses and indicate that PCPs who refer five or more patients per week to their clinical pharmacist(s) compared to those who referred less than five patients per week (mean of 5.4 and 5.6, p = 0.0210), and PCPs who consult with their clinical pharmacist(s) five or more times per week compared to those who consulted less than five times per week (mean of 5.6 and 5.3, p = 0.0071) reported slightly greater satisfaction with these services.
Discussion
Compared to early studies assessing provider perception of clinical pharmacy services, our results demonstrate that PCPs recognize the impact of clinical pharmacists on patient care and are satisfied with their clinical pharmacists. It is important to note that not only were PCPs likely to recommend collaborating with a clinical pharmacist, but PCPs also felt that their workload did not increase as a result of working with clinical pharmacists. These data support the role of clinical pharmacists as extenders of PCPs. Considering the PCP shortage, which is likely to increase due to more patients having access to health insurance under the Patient Protection and Affordable Care Act, clinical pharmacists are essential in primary care. 27
These results highlight a positive PCP perception of clinical pharmacists, which likely represents a change in culture from decades ago. 3 This change in culture regarding clinical pharmacists may be due to expanded roles and more advanced training of pharmacists in addition to the increased importance of interprofessional practice. This shift may also be influenced by PCPs who are required to accept pharmacists as extenders given PCP shortage/demands. However, PCPs are reporting that clinical pharmacists contribute to and improve the quality of patient care in a unique way that could not be achieved by other professions, suggesting the PCP shortage/demands may be less influential. These results were in line with results reported after the integration of a clinical pharmacist to a family medicine practice in Canada. 28 Physicians within the practice expressed that practice-level benefits after the integration of a pharmacist included freeing up resources, providing a link with community pharmacists, providing group education, and fostering a team environment. 28
PCPs indicated that the most impactful clinical pharmacy services were MTM, disease-focused management of diabetes, hypertension and pain, and medication reconciliation. It is possible that PCPs indicated these services to be most impactful because they were most familiar with these services that were most commonly already offered across the primary care practices. However, this is consistent with previous studies that report prioritizing similar services when developing and implementing new clinical pharmacy services.28,29 A similar survey distributed to providers within a PCMH identified top-tier clinical services as medication counseling, reconciliation, adherence assessment, polypharmacy assessment, and drug information consultations. 30 Of note, pain management was only reported to be offered in 35% of the practices but was ranked as one of the most impactful in our study. Our data can help guide clinical pharmacists to tailor their services to best fit the needs of their practice site.
Limitations
Our study did have several limitations that warrant consideration. Given that our initial distribution sample was 1603 RPDs, our yield of responses was low at approximately 9%. Due to funding restrictions, access to Listservs containing direct contact information for primary care physicians was not attained. Additionally, while we attempted to expand the reach of our survey by distributing to RPDs across the nation, the majority of the responders were from the Southwest/Pacific. We did not utilize one-time use survey links and were unable to track the RPDs who forwarded the email to providers; therefore, we are unable to describe the nonresponders. Additionally, due to the distribution to RPDs and not to the providers directly, we are unable to verify whether all respondents to the survey were providers and involved in primary care practice.
We were also unable to capture the PCP population that may not be affiliated with a residency program. Selection bias may have resulted if RPDs withheld distribution of the survey due to a lack of a strong relationship with their PCP colleagues and fear of a negative survey response. Additionally, because we only distributed the electronic survey to RPDs, it is more likely that the PCPs that were forwarded the survey would have worked with clinical pharmacists previously. It is also possible that the data are biased if there was a higher proportion of responses representing a specific clinical pharmacist, which we tried to prevent by distributing the survey to a large and national cohort of pharmacists whom we asked to forward the email. Because responders were able to disclose the email addresses of the person who forwarded the survey to them, we are able to identify some RPDs who were more active in forwarding the survey, which could possibly be contributing to bias in responses.
The active survey phase was for 4 weeks and may have been a limiting factor in generating a larger sample size. Additionally, as discussed before, we had a low yield rate of responses given our distribution sample. The survey distribution was not extended beyond 4 weeks due to a significant drop in response rate by the fourth week despite reminder emails sent after the second week of distribution, and the study investigators did not anticipate significantly more responses. The sample size exceeded the size required of our power calculations aimed at estimating reliability (Cronbach’s alpha statistic), and the survey was stopped after 4 weeks. Out of the 144 responses, 16 were incomplete. We examined the responses that were incomplete and did not find any commonalties between the responders within this pool. As this was an electronic survey that could be taken on a mobile device and had multiple domains, there may have been confusion while navigating the survey leading to an unexpected early termination of the survey.
We were able to analyze the data collected to evaluate associations between certain demographic groups and provider satisfaction and perception of clinical pharmacy services. However, due to the categorical response options for number of patient referrals (and other variables), we were unable to estimate correlations between this and provider demographics; this may have limited our ability to assess other factors that may have influenced provider response. Additionally, we did not look at the billing capabilities or activities of the clinical pharmacists in the PCPs’ practice sites. This would help to identify whether financial contributions by the clinical pharmacists would improve PCP satisfaction. However, billing/reimbursement for clinical services performed by pharmacists is not currently a common practice due to regulatory restrictions; therefore, we felt that this would not be pertinent for the majority of our responders.
Conclusion
PCPs report high satisfaction with clinical pharmacy services and perceive that clinical pharmacy services have a positive impact on patient care. The PCPs surveyed recommend clinical pharmacists to practices that currently do not have one. Comprehensive MTM and disease-focused management of diabetes, hypertension, and pain were identified as the most valuable clinical pharmacy services. These perceptions should be considered when developing or expanding clinical pharmacy services.
Footnotes
Acknowledgements
This work has been previously presented as a scientific poster at the American College of Clinical Pharmacy Annual Meeting 2015.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The University of Colorado’s Multiple Institutional Review Board (COMIRB# 14-2077).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.