
Abstract
Introduction:
Maintaining continuity of care is one of the most critical components of providing great care in primary health care. This study aimed to explore continuity of care and its predictors in primary healthcare settings among patients with chronic diseases in Saudi Arabia.
Method:
Face-to-face cross-sectional interviews were conducted with patients with chronic diseases who had at least four visits to primary care facilities in Riyadh, Saudi Arabia, between November 1, 2022 and March 3, 2023. We determined patients’ continuity of care levels using the Bice–Boxerman continuity of care index. A Tobit regression model was used to determine the effects of several factors on the continuity of care index.
Results:
The interviews were conducted with 193 respondents with chronic diseases of interest. The mean continuity of care index of the entire sample was 0.54. Those with asthma had the highest median continuity of care index at 0.75 (interquartile range, 0.62–0.75), whereas those diagnosed with thyroid disease had a much lower continuity of care index (0.47) (interquartile range, 0.3–0.62). Tobit regression model findings showed that employed respondents with poorer general health had a negative effect on continuity of care index levels. By contrast, a higher continuity of care index was significantly associated with elderly respondents, urban residents, and those diagnosed with dyslipidemia, diabetes, hypertension, or asthma.
Conclusions:
According to our findings, the continuity of care level in Saudi Arabia’s primary healthcare setting is low. The data demonstrate how continuity of care varies among study group characteristics and that improving continuity of care among chronic disease patients in Saudi Arabia is multifaceted and challenging, necessitating a coordinated and integrated healthcare delivery approach.
Introduction
Chronic diseases are a significant healthcare challenge in Saudi Arabia, accounting for a large percentage of healthcare spending and causing significant morbidity and mortality. 1 Around 83,100 people die from chronic diseases annually, accounting for 73% of all fatalities in the country. 2 Chronic diseases such as diabetes, respiratory disease, cardiovascular diseases, cancer, and hypertension are prevalent among the population of Saudi Arabia. 2
As the population ages and increases, chronic diseases place an increasing financial burden on individuals, families, and healthcare systems. They also use a disproportionate amount of available resources in the healthcare system because they make more trips to the doctor, have a higher incidence of visits to the emergency department (ED) and hospitalizations, and run a higher risk of being readmitted after discharge from the hospital. 3
Owing to the complexity of their medical diseases, there is a concern that those suffering from chronic diseases are at risk of receiving suboptimal medical treatment. Chronic diseases, for instance, are linked to coordination difficulties for patients and medical professionals who treat them, which often include several different physicians and facilities of treatment. 4 Inadequate coordination of healthcare services over time and across different healthcare providers, settings, and levels of care resulting from fragmented and disjointed care delivery. Fragmented care is characterized by poor communication among healthcare providers, lack of shared patient information, duplication of tests and services, and inadequate follow-up and monitoring. 5 For instance, a patient with multiple chronic diseases who sees multiple doctors for different health issues may experience conflicting treatment plans, drug interactions, and missed appointments. This can lead to unnecessary hospitalizations, emergency visits, and medication errors, jeopardizing the patient’s health and increasing the burden on the healthcare system. Moreover, fragmented care can worsen health disparities, especially for vulnerable populations such as older adults and low-income individuals, who face more barriers to accessing and navigating healthcare services. 6
From this perspective, providing continuity of care (CoC) is essential for the care offered to patients with chronic diseases. 7 The World Health Organization recommends the practice of CoC in primary healthcare to maximize the management of noncommunicable diseases. This recommendation is based on the framework for integrated people-centered health services. 8 The concept of CoC refers to the delivery of treatment that is continuous and “seamless” through several healthcare professionals and settings. 9 Prior observational research indicates that CoC is associated with greater patient satisfaction, fewer ED visits and hospitalizations, reduced mortality risk, and lower care costs. 10
The Saudi Arabian Ministry of Health undertook health sector reform as part of a broader agenda for transforming all government sectors, as envisioned in Vision 2030 and the National Transformation Program 2020. Primary health care (PHC) practice is at the core of this transformation. PHCs are vital components of the Saudi Arabian healthcare system and provide an essential point of contact for patients with chronic diseases. The Ministry of Health provides various preventive and curative services, with a particular focus on PHC services such as health promotion, disease prevention, and early detection of illnesses. There is a greater emphasis on pushing PHC practices to seek accreditation standards anchored in patient-centeredness. Thus, this reform shifted the focus and funding from secondary and tertiary healthcare facilities toward reshaping and reforming PHC, which included more than 2398 PHC centers. 11
Unfortunately, a comprehensive study found that PHC services are not being used to their full potential, with just two visits per person per year. Consequently, a road plan for primary healthcare reform that spans 2016–2020 was devised to elevate the overall level of service and ensure that PHC centers focus more on providing patient-centered care and maintaining the CoC. 12 Various factors may impact the level of CoC, including socioeconomic status, age, education level, and comorbidities. However, the results of studies examining these factors have been inconsistent. 13
To our knowledge, there has not been any previously published research in Saudi Arabia that evaluated CoC while it was being used in PHC settings until we began writing this article. As patients with chronic diseases are among those most likely to benefit significantly from CoC, this study aimed to explore CoC and its predictors in PHC settings in patients with chronic diseases in Saudi Arabia. It is hoped that this study will identify the strengths and weaknesses of CoCs in PHC settings and delineate strategies for their improvement.
Methods
Study design and study population
Between November 1, 2022 and March 3, 2023, face-to-face cross-sectional interviews were conducted with respondents who visited primary care facilities in Riyadh, Saudi Arabia. To ensure a successful approach to collecting data, we opted for face-to-face interviews instead of self-administered questionnaires. This method allows for personalized assistance and clarification, which can be particularly helpful for individuals who may have difficulty completing a written survey. We aimed to maximize the efficiency and accuracy of our data collection process by prioritizing the comfort and needs of our participants. The PHCs were selected using a stratified random sampling method based on patient load. Four centers, two with high and two with low patient numbers, were chosen out of 26 in the city.
The inclusion criteria were respondents aged 18 years or older who had at least four prior visits to the PHCs within the past year and had at least one of the following chronic diseases: hypertension, dyslipidemia, diabetes mellitus, congestive heart failure, kidney disease, thyroid disease, psychiatric disease, and anemia. Individuals not of Saudi nationality were included to ensure a more diverse and representative sample for the study of PHCs. The exclusion criteria included insufficient ability to participate in the survey and inability to provide consent.
Because patients with chronic diseases may lack interest in participating in studies due to their chronic conditions, the study employed convenience sampling and recruited all eligible participants. Patients were asked if they could participate, discuss the study, and obtain consent to participate. Recruitment continued until it was determined that a representative sample across demographic groups and health services was obtained, and we had reached data sufficiency. The minimum sample size required for this study was calculated using the Raosoft calculator to be 184 individuals, with a significance level of 95%, a margin of error of 5%, and a 50% response distribution. However, to ensure an adequate sample size, 193 participants were enrolled.
Data collection and questionnaires
The respondents participated in face-to-face interviews using a structured questionnaire that lasted approximately 12 min. To address our research objectives, we thoroughly searched pertinent literature and used it to construct a questionnaire. Our research team meticulously examined the questionnaire to ensure its content validity. In addition, we carefully translated the questionnaire into Arabic, verifying its accuracy through multiple rounds of translation. Before finalizing the questionnaire, we made necessary adjustments to ensure its clarity and ease of comprehension, pretesting it with 25 Arabic-speaking individuals and making modifications as needed. Respondents were questioned using a questionnaire divided into three sections on sociodemographic and clinical profile characteristics and healthcare service utilization in the preceding 12 months. After a comprehensive review of the study materials, field experts validated the structured questionnaire and verified its accuracy. As part of the pilot study, the questionnaire was administered to 15 individuals twice, with a 2-week gap between each administration, to verify its reliability. Each completed questionnaire was evaluated for its internal validity. To guarantee reliability and consistency throughout the interviews, teams of highly trained interviewers, who had previously been instructed to administer the survey, were selected.
Independent variables
Sociodemographic characteristics included sex, age, marital status (married or unmarried), education level (illiterate/read/write, primary education, intermediate education, secondary education, or higher education), employment status (employed or unemployed), geographic location (rural or urban), health insurance status (yes or no), and whether they had a regular doctor (yes or no). Due to the high level of unreliability, 14 which includes the reluctance of individuals to reveal accurate information about their income, 15 researchers believe that a valid country-specific socioeconomic status index (SES index) is a better economic indicator for the individual than income. We measured SES using principal component analysis, which uses information from respondents’ asset holdings. 16 For each interview, we created an SES index based on various factors such as education level, work status, type and tenure of housing, car ownership, and asset ownership. Housing was categorized into traditional, apartment, floor inside a villa, or available housing, while housing tenure was divided into four subgroups: house ownership, home renting, home provided, and other types of tenure. Participants were also grouped based on their car ownership, with three categories: those who did not own a car, those who owned one, and those who owned two or more. Asset ownership was analyzed using eight dichotomous variables, including phone availability, television ownership, personal computer ownership, Internet access, library access, satellite TV, video ownership, and video game ownership. SES was divided into five quintiles, with the quintile that contained individuals with the lowest SES designated as the first quintile and the quintile that contained individuals with the highest SES designated as the fifth quintile. To assess chronic conditions, a standardized checklist was utilized. Participants had to answer with “yes” or “no” to indicate if they had been diagnosed with each condition. In addition, the participants in the study were asked to rate their own health status by selecting from a range of options including excellent, very good, good, fair, or poor.
Dependent variable
We determined the respondent’s level of CoC using the Bice–Boxerman continuity of care index (CoCI), a standard metric derived from the total number of times a respondent sees each of their physicians. 17 We selected this quantitative measure because of its applicability to respondents with multimorbidity, who may receive treatment to manage their chronic diseases from a wide variety of medical professionals. 18
The CoCI is a continuous variable with a range of 0–1. One number represents the highest CoC level when the same provider is shown at each stop, which suggests good continuity. The formula for the CoCI is as follows:

The total number of visits to providers is denoted by N, nj denotes the number of visits to a particular provider, and s denotes the total number of providers observed.
In PHC, we considered face-to-face assessment and management appointments with a clinician as a provider visit. Furthermore, we estimated that respondents’ CoCI focused only on appointments with primary care providers because we were interested in predicting the continuity of primary care.
CoCI does not include visits to specialists, subspecialists, or emergency rooms. Furthermore, we omitted procedure-only visits (e.g., vaccines) because they did not entail face-to-face interactions between the clinicians and patients. According to previous research, the stability of Bice–Boxerman CoCI increases with the number of visits. To avoid significant changes in the Bice–Boxerman CoCI calculation due to slight differences in care dispersion, a minimum of four visits are necessary. 19
Ethics, consent, and permissions
This study was approved by the institutional review board of the Ministry of Health, Saudi Arabia (IRB Log Number 22-490). This study complied with the ethical standards outlined in the Declaration of Helsinki of the World Medical Association. To protect the confidentiality of information, both anonymization of the data and their aggregation were used. Before beginning the research, consent was obtained from each participant in the form of a written statement indicating that the responder had been informed.
Statistical analysis
Descriptive statistics were used to characterize the participants. The mean, median, and interquartile range (IQR) were used to describe the CoC data. To ensure accuracy, we used Tobit regression models to examine the factors associated with CoCI. We constructed a model and assessed every potential confounding variable to determine its influence on the CoC. This was done by comparing the effects of each variable on CoC before and after each variable was added. Only the variables that caused a change of ⩾5% in the CoC coefficient were incorporated into the final models. The limited character of the dependent variable, CoCI, which was confined by a minimum and maximum value, led us to choose the Tobit model as our modeling tool instead of ordinary least-squares regression because its assumption of a normally distributed error term is commonly broken in certain situations, resulting in skewed results. All regression models were adjusted to consider the sociodemographic characteristics of the patients. In all analyses, a two-sided level of significance equal to or below 5% was considered statistically significant. SAS (version 9.4; SAS Institute Inc.) was used for all statistical analyses.
Results
The interviewer encountered 200 individuals with the chronic diseases of interest. After excluding six respondents who did not provide permission to participate in the research (representing 3% of the total) and those who did not provide the necessary information, we were left with 193 respondents. More than half of the patients who participated in the study were male (56.48%), and the majority of the patients were aged between 59 and 69 (28.5%) or between 60 and 69 (22.8%). According to the data collected from the survey, the vast majority of respondents were married (78.24%), Saudi (92.75%), had either a secondary education (31.09%) or a higher education (29.02%), were unemployed (54.6%), and lived in urban areas (90.16%) (Table 1).
Characteristics of the study population (n = 193).

SES: socioeconomic status.
Table 1 also reveals that the highest proportion of patients were from middle-class and wealthy SES quintiles (39.9% and 28.5%, respectively) and that the vast majority of people did not have health insurance (68.39%) or a doctor who treated them regularly (59.07%). Diabetes mellitus was the most prevalent self-reported chronic disease, accounting for more than half of the investigated sample (59.59%). According to research findings, hypertension was listed as the second most prevalent illness overall (57.51%), whereas dyslipidemia was identified as the third most prevalent illness (44.04%). A total of 33.68% and 22.28% of the individuals reported good and excellent health, respectively.
Descriptive statistical analyses and visual representations of boxplots were used to thoroughly explore the findings. A box-and-whisker plot is shown in Figure 1, which compares the CoCI for patients with various chronic diseases. The boxes illustrate the first- and third-quartile ranges that account for half of the available data. The median is represented by the horizontal line that runs through the middle of the box, whereas the mean is marked by the “O.” The top and bottom lines on the graph reflect the lowest and maximum possible values, respectively. Outliers are presented in this section. The mean CoCI of the entire sample was 0.54. Those who had asthma had the highest median CoCI levels at 0.75 (IQR, 0.62–0.75), while 0.7 (IQR, 0.42–0.78) and those who suffered from hypertension, and 0.68 (IQR, 0.5–0.68) for those who experienced a psychological disease. Patients diagnosed with thyroid illnesses had a significantly lower CoCI (0.47) (IQR, 0.3–0.62).
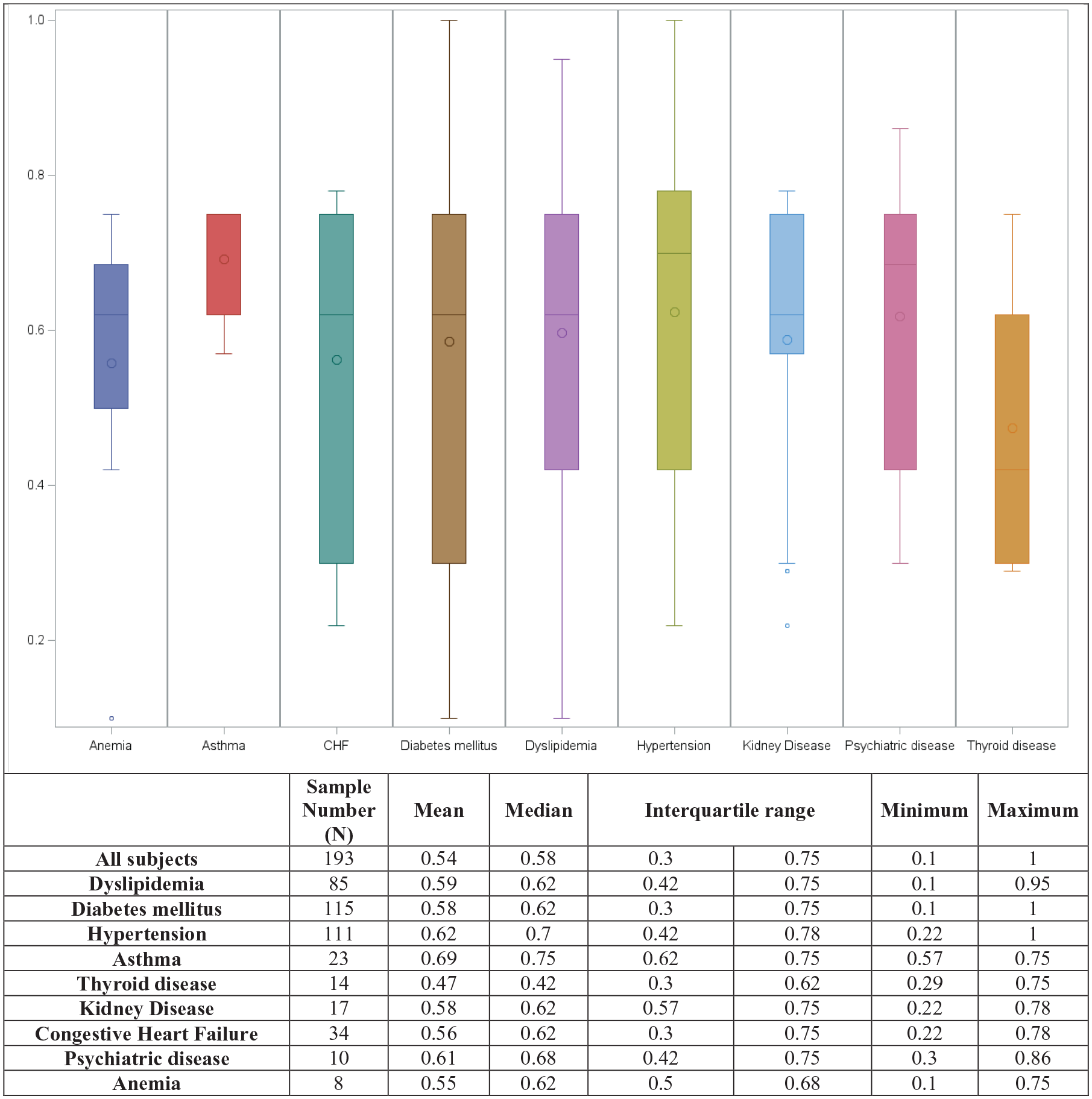
Box-and-whisker plot of the distribution of CoCI levels.
According to the Tobit regression model findings (Table 2), we identified multiple aspects that substantially impacted the CoCI levels. Employees have a lower chance of receiving a good CoC. In addition, poor or fair general health had a significant inverse association with the CoCI level (p < 0.05). Upon analysis of the factors that contribute to a good CoC, it was discovered that individuals who fall within the age ranges of 50–59, 60–69, and 70 and above, as well as those residing in urban areas, display a positive correlation with good CoC. Individuals diagnosed with dyslipidemia, diabetes mellitus, hypertension, or asthma were also found to have a higher likelihood of receiving good CoC. Patients with a regular doctor were more likely to achieve high CoC than those without. Regarding self-rated health, patients who rate their health as “very good” were more likely to have a good CoC (p < 0.05)
Tobit regression predicts the CoCI level.
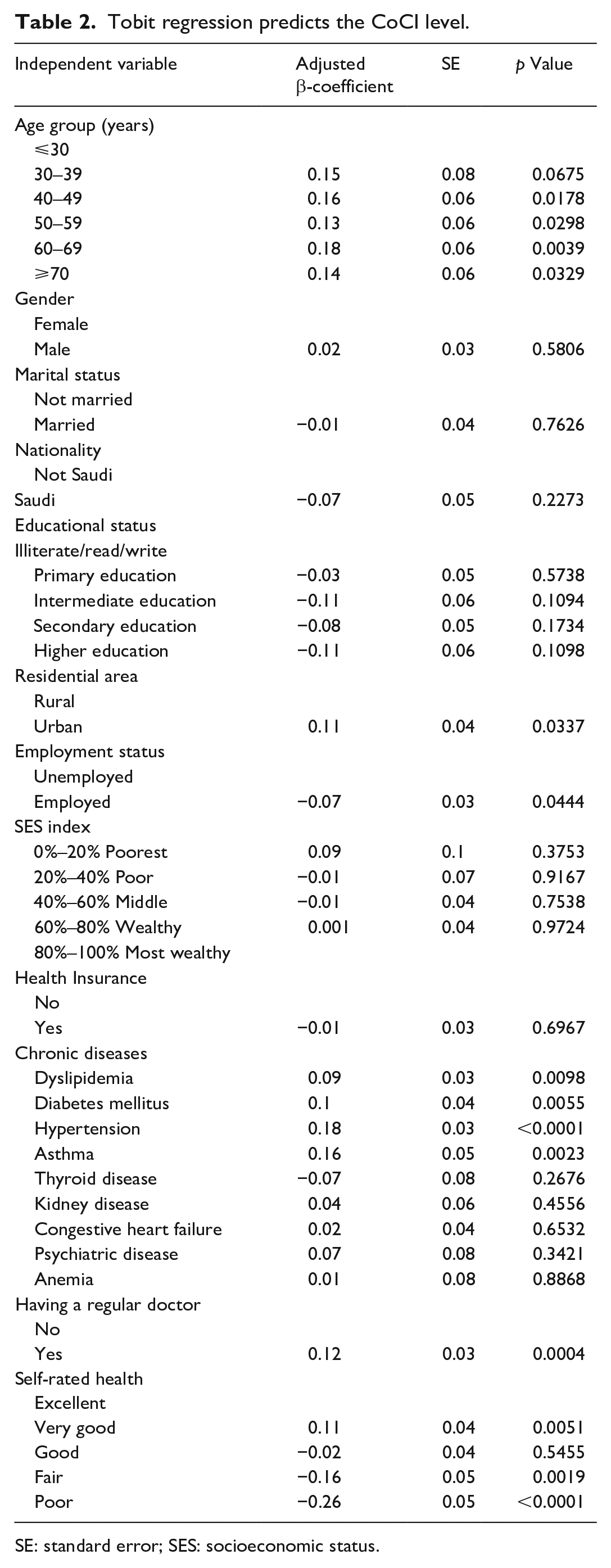
SE: standard error; SES: socioeconomic status.
Discussion
One of Saudi Arabia’s top priorities is ensuring that patients receive high-quality care in PHC settings. CoCs are fundamental components of such care. In addition, the high prevalence of chronic diseases in Saudi Arabia has highlighted the necessity of highly effective health systems established for primary care and guaranteeing that patients receive continuous care. 2 This is crucial to effectively manage and care for those who suffer from chronic diseases and comorbidities that are commonly linked with them. The present study was conducted in Saudi Arabia to analyze the level of CoC in PHC settings among patients with chronic diseases and determine their predictors.
Our study found that the CoC was low among patients with chronic conditions, suggesting that most patients lacked continuous care from the same providers. The findings of this particular observation are marginally less favorable than those of a local study that only looked at people with diabetes. 20 Several issues exist in straightforward and valid comparability with comparable previously published findings from other countries. The possibility that the observed discrepancies are related to changes in the setting or population investigated, periods, criteria for assessment, reporting techniques, and patients’ accessibility to medical care or the healthcare system cannot be ruled out. For example, compared to previous research populations, the population in this study had a better CoC than that reported for Medicare patients in the United States who were older than 65 years, 21 and in England among patients with long-term diseases. 22 By contrast, the CoCI value here is lower than those observed in patients with chronic disease in Norway, 23 in Canada among patients aged 18–105 years with at least one chronic disease, 24 and in patients with multimorbidity in Switzerland. 25
Although absolute or complete CoC may not always be the best choice, a plausible assumption based on the current CoC literature is that more continuity will create a better understanding between provider and patient, proving advantageous and creating value. Several studies have shown that a 0.1-unit increase in CoC can considerably decrease hospitalizations, ED visits, chronic disease problems, overused medical procedures, and expenses.9,26–28
The identification of variables that impact CoCs is one of the most crucial objectives of this study. Among the patients’ sociodemographic characteristics, employment or poorer general health status was likely to have a lower CoC. Similarly, in several studies, an exciting finding is that older patients have better CoC levels than younger patients.29–31 Studies have shown that older adults receive better CoC than younger adults. One reason for this is that older adults tend to have more chronic health diseases that require ongoing management, which naturally leads to a closer relationship with their healthcare providers. 32 Younger adults, on the other hand, tend to be healthier and may not require as much ongoing care, making it more challenging to establish a long-term relationship with a specific provider.
Our results also show that urban residents have better CoCs than rural residents. One factor contributing to the better CoC experienced by urban residents is that the sheer number of medical facilities and healthcare professionals in urban areas means that patients have access to an extensive infrastructure capable of providing continuous care. 33 However, for rural residents to have better CoCs, investments must be made in rural healthcare infrastructure, technology, and equipment to bridge the gap. By doing so, the state will ensure that everyone has access to continuous care regardless of location.
Despite the availability and accessibility of PHC, our analysis found that employed respondents do not utilize these services as often as those who are unemployed. This discrepancy is multifaceted but can be attributed to time constraints or a lack of perceived urgency regarding their health. This finding is consistent with findings in Canada 34 and the United States. 35
We also found that research has shown that patients with dyslipidemia, diabetes mellitus, hypertension, and asthma had better CoC scores than those with other chronic diseases. This is consistent with previous studies.36,37 The reasons for better CoC for these chronic diseases may vary. One contributing factor could be the availability and accessibility of the medications and medical devices required to manage these diseases. In addition, the education and training of healthcare providers in managing these diseases may impact the quality of the care provided. CoC is essential for managing chronic diseases, such as dyslipidemia, diabetes mellitus, hypertension, and asthma. Patients with these diseases require ongoing monitoring and management to prevent complications and improve health outcomes. Healthcare providers must prioritize CoCs for all chronic diseases to provide the best possible care for their patients.
In addition, our analyses, comparable to the extant literature,38–40 revealed that patients with a regular doctor were more likely to achieve CoC than those without a regular doctor. There are several possible explanations for this observation: First, patients with regular doctors can anticipate consistent, personalized care that considers their medical history and current health concerns. 41 This improves the patient’s experience and fosters a sense of trust between the patient and the healthcare provider. Second, patients with regular doctors often receive appropriate follow-up care from their doctors to track their progress and rapidly detect any changes in their health status. 42 In addition, when patients receive care from a consistent and dependable source, they are more likely to feel supported and secure. 43 This is especially essential for patients with chronic or long-term diseases for whom a regular physician can provide medical, emotional, and psychological support.
Moreover, because CoC is essential for ensuring better patient health outcomes, our findings confirm this observation, as we found that a lower CoC may be associated with poor health. Patients who experience inadequate CoC may experience adverse events, such as medication errors and unnecessary procedures, which can delay their recovery and increase their mortality risk.6,44 Furthermore, they may experience lower care satisfaction and treatment plan adherence. 45
These findings may have implications for healthcare professionals and those who establish performance indicators to improve the CoC of patients with chronic diseases. Patients are often seen in multiple clinics and hospitals and prescriptions and medical records are not always shared among institutions. This can lead to the duplication of tests and treatments and the risk of medical errors and adverse reactions. 6 To address this issue, it is essential to establish a coordinated care approach that involves multiple healthcare providers working together to ensure that patients receive comprehensive and integrated care. In addition, many patients with chronic diseases in Saudi Arabia are unaware of the importance of disease management and may not adhere to treatment plans. 46 This can lead to poor outcomes and complications. To address this problem, it is essential to provide patients with education and resources to manage chronic diseases, and support and guidance to help them adhere to their treatment plans. Finally, according to published reports, chronic care management-trained healthcare professionals are in short supply. 47 There are few specialists in chronic care management in Saudi Arabia; therefore, many patients are seen by general practitioners or specialists in other disciplines who may lack the expertise or resources to effectively manage chronic diseases. To tackle this problem, training and educating healthcare professionals in the specialized care of chronic diseases and encouraging the development of clinics and centers dedicated to chronic care is crucial.
This study had several limitations. First, the cross-sectional design of this study, as with other studies, prevents us from conclusively establishing causal relationships. Second, the results of this questionnaire survey were collected via face-to-face interviews and founded solely on participant reports. Third, while this is consistent with methodologies from previous studies on CoC, it is essential to recognize that patients may have numerous other interactions with the delivery system, including via telephone, which may also significantly affect the CoC. Fourth, owing to the difficulty in data acquisition, the study had a small sample size, which can limit its scope and generalizability. Finally, it should be noted that chronic conditions are based on self-reporting and cannot be verified using medical records. This study contributes to the understanding of CoC, despite its limitations, and its primary strength is that it is the first of its kind to be conducted in this geographic region.
Conclusion
PHCs are critical components of the Saudi healthcare system and may deliver CoCs to individuals with chronic diseases. According to our findings, the CoC level in Saudi Arabia’s PHC setting is low. The data demonstrate how CoCs vary among study group characteristics and that improving CoC among chronic disease patients in Saudi Arabia is multifaceted and challenging, necessitating a coordinated and integrated healthcare delivery approach. In addition, this study suggests that greater resources and efforts must be allocated to reduce barriers to care for disadvantaged patients with chronic conditions. Nevertheless, continuous investment in PHC facilities will ensure CoC and improve healthcare outcomes for Saudi patients with chronic conditions.
Supplemental Material
sj-docx-1-smo-10.1177_20503121231208648 – Supplemental material for Continuity of care in primary healthcare settings among patients with chronic diseases in Saudi Arabia
Supplemental material, sj-docx-1-smo-10.1177_20503121231208648 for Continuity of care in primary healthcare settings among patients with chronic diseases in Saudi Arabia by Ziyad S Almalki, Abdullah K Alahmari, Sarah AA Alajlan, Abdulhadi Alqahtani, Ahmed M Alshehri, Saleh A Alghamdi, Adel A Alanezi, Basil K Alawaji, Tareq A Alanazi, Rawan A Almutairi, Saad Aldosari and Nehad Ahmed in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia, for funding this research work through project number (IF-PSAU-2022/03/21718). The authors thank the Research Center at King Fahad Medical City, Riyadh for their valuable support in reviewing and proofreading this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from by the Institutional Review Board of the Ministry of Health, Saudi Arabia (IRB Log Number 22-490).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This Research was funded by the Deputyship for Research and Innovation, Ministry of Education, Saudi Arabia (grant number IF-PSAU- 2022/03/21718).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.