
Abstract
Introduction:
In Sri Lanka in 2013, 16 medicines were identified as priority to manage non-communicable disease (NCD), and in 2017, 48 NCD medicines were price-regulated.
Objective:
The aim of the present study was to describe the experiences on availability of drugs and out-of-pocket expenditure (OOPE) for drugs among patients with NCDs in Sri Lanka.
Methods:
This community-based, household survey was conducted in nine districts of the country. The survey included 1100 adults (aged 50 years and above) with a diagnosis of NCD for 5 years. They were interviewed by trained pharmacy students.
Results:
Approximately 66%, 49% and 21.6% suffering from hypertension, diabetes and ischaemic heart disease, respectively, with a majority having more than one NCD. The evidence showed that prescribers align to drugs that have been recognized to be made more available and more affordable. Of all, 14% had prescriptions with all NCD medicines classified in the list, while 40% had only one or two of the drugs prescribed which are not in the list. Most of the prescribed drugs were also included in the price regulation – with 29% having all medicines included, while 31.6% having only one or two drugs prescribed out of the list. Approximately, two-thirds (64.2%) had exclusively used government hospitals for NCD care during the past 5 years. A majority (58.3%) had all prescribed drugs available at the last visit to the state sector clinic, while almost all of the others (35.7%) had some of the drugs available.
Conclusion:
The study concluded that patient experiences in Sri Lanka showed good availability and access to NCD medicines in Sri Lanka.
Introduction
The burden of non-communicable diseases (NCDs) is increasing in Sri Lanka,1–3 and apart from lifestyle changes, access to essential NCD medicines can be considered as the single most vital intervention in preventing morbidity and mortality. Improved access to essential medicine is an expected outcome to achieve the goal of ‘one billion more people benefiting from Universal Health Coverage’ of the General Programme of Work 13 of the World Health Organization (WHO).4–6
Access to medicines in the state sector in Sri Lanka is free of charge. 7 However, in the event of the drugs prescribed in a state sector consultation not being available, the patients are expected to purchase the drugs from a private pharmacy through out-of-pocket expenditure (OOPE). However, healthcare costs in the private sector are totally borne by the patients through OOPE. According to the Household Income and Expenditure Survey (HIES 2016) conducted by the Department of Census and Statistics in 2016, 14.6% and 15.7% of the Sri Lankan households received out-patient treatment services from private and government hospitals, respectively, within a period of 1 month prior to the survey, 8 indicating almost equal usage of both sectors.
Documented measures for reducing the OOPE on medicines include price regulation, improving the supply chain and reimbursement of medicine costs. Only the first two are applicable to Sri Lanka. At present, there is no means of reimbursement of costs of medicines. The rationale for price regulation of medicines in Sri Lanka is the failure of market discipline to operate in markets for medicines.
With the prime objective of ensuring availability and access to medicines and thereby reducing the need of the patients who utilize the state sector to purchase the medicines, the Ministry of Health, Sri Lanka, identified 16 NCD medicines and issued a circular (02-174/2013) in 2013 indicating them as a list of priority drugs to manage NCD at primary-level healthcare institutions, mandating them to be available in the healthcare institutions at all times. 9 Thereafter, as a direct step to reduce OOPE on medicines, the government regulated the price of 48 commonly prescribed groups of medicines by setting a price ceiling through a notice by Extraordinary Gazette’s on 21 October 2016, revised in December 2017. 10 These 48 included 18 NCD drugs and 16 of them were also identified in the 2013 list of priority drugs to manage NCD at primary-level healthcare institutions (Annexure A in Appendix 1). The pricing regulation announced in 2017 was based on a mechanism that uses the median price of any drug that commands a 2% or more market share by volume.
Although it is imperative that the impact of the key interventions of the government of Sri Lanka to improve the availability and affordability of NCD drugs be evaluated, such an evaluation has not been conducted. Information on NCD medicines availability is from nationally representative institution-based studies of pharmacies, and these studies were conducted prior to the 2017 directive on price control.
In this backdrop, the primary objective of the study was to describe the patient experiences of access and affordability of NCD drugs. Owing to the growing body of evidence that patient satisfaction is a more important outcome measure for evaluating the extent to which the healthcare sector meets patients’ needs and expectations, this study focused on the end-user ‘the patient’. 11
Methods
This was a community-based, household survey carried out in all nine provinces. Data collection was performed in May 2018.
The study populations were adults aged 50 years and above, with a physician-confirmed diagnosis of either hypertension, ischaemic heart disease (IHD), diabetes mellitus, asthma or chronic obstructive airway diseases for at least 5 years.
In the absence of estimates of proportion of adults with NCDs in Sri Lanka who experienced shortages of NCD drugs, the sample size was calculated based on 50% to obtain the maximum required sample. Using an absolute precision of 5%, and a design effect of 2% and a non-response rate of 20%, the sample size was estimated to be 923, which was rounded off to 1000.
Sample was selected to represent all NCD patients in nine provinces. In the first stage, one district was randomly selected from each province, except the Western province – from which two districts were selected as the province records the largest population. From each district, two Medical Officer of Health (MoH) areas were randomly selected in the second stage. From each of the MoH areas, two Grama Nildharai (GN) areas were selected randomly to be included in the survey, and a GN area was considered as the primary sampling unit and a cluster. A cluster was defined as a groups of eligible study units living in a GN area and the cluster size was determined as 25. Each selected district was allocated four clusters. Thus, the survey included 40 clusters to recruit the required sample of 1000.
A total of 25 study units were included in each cluster in a household survey. The first house of a cluster was selected by random selection of a house from the voter’s list. The second household was the one which is nearest to the first household, matching the inclusion criteria. This procedure was repeated until 25 eligible participants were identified. A household was defined as members of a family sharing the same kitchen. Among all the members in the households who fulfilled the eligibility criteria, only one was selected using a random method. If the selected member was not present in a particular household, the household was re-visited twice prior to considering him/her as a non-respondent.
An interviewer-administrated questionnaire administered by trained graduate pharmacy students gathered the required information. In most instances, the respondent was the study unit himself/herself. Written informed consent of the study unit was obtained prior to the interview. In the instances where the required information was not known by the study unit, the adult in charge of follow-up care of the selected study unit was used as the respondent.
In data analysis, the sample was weighted according to the adult population of provinces based on data of 2012 census in Sri Lanka, to account for the variation of adult population in different provinces (Annexure B in Appendix 1).
Experiences related to availability of drugs and OOPE for drugs among patients with NCDs will be described using descriptive statistics. Weighted frequency tables were calculated for relevant variables. Analyses were performed using Statistical Package for Social Sciences (SPSS) version 22.
Administrative clearance was obtained from Director General of Health Services, Ministry of Health Nutrition and Indigenous Medicine, Sri Lanka. Ethical clearance was obtained from the Ethics Review Committee of National Institute of Health Sciences of the Ministry of Health, Sri Lanka (NIHS/ERC/1 8/03).
Results
Background characteristics
A total of 1100 eligible study units were invited to fulfill the required number of 1008 eligible adults, giving a response rate of 91.6%. The sociodemographic characteristics of the participants are shown in Table 1. The proportion of females was slightly higher than males in the sample. Approximately, one-third (31.7%) were in the youngest age category of 50–59 years. Notably, 13.5% have had no formal school education. Approximately, half (55.4%) showed an education level above grade 5 level. Sinhalese (78.1%) were the great majority. Most (63.4%) of the participants were not gainfully employed with 30.1% being housewives, 11.9% retired and 21.4% reporting not occupied. Majority (70.1%) had no regular source of income. Furthermore, 36% indicated that none in the family had a regular income.
Distribution of study sample by selected sociodemographic characteristics.

GCE O/L: General Certificate of Education Ordinary Level; **GCE A/L: General Certificate of Education Advanced Level.
Regarding the NCDs the participants were diagnosed with 66%, 49% and 21.6% were found to be suffering from hypertension, diabetes and IHD, respectively. Asthma and chronic obstructive airway disease were less common with 6.9% and 3.0% reporting the conditions, respectively.
Impact of interventions of the government of Sri Lanka
This study evaluated the number of prescribed NCD drugs based on whether they are included in the list of priority drugs to manage NCD at primary-level healthcare institutions (published in 2013) or the list of price-regulated drugs (published in 2017). This provides an indication of how much the prescribers align their prescriptions to the NCD drugs that have been recognized to be made more available (Table 2). Of all, 14% (males, 15%; females, 13%) had prescriptions with all NCD medicines classified in the list of priority drugs to manage NCD at primary-level healthcare institutions (published in 2013). Nearly 40% had only one or two of the drugs prescribed which are not in the list (males, 38.6%; females, 40.5%). The evaluation of whether the prescribed drugs were included in the list of price-regulated drugs published in 2017 showed that approximately one-third (29%) had (males, 28.7%; females, 29.5%) all medicines included, while 34.6% (males, 32.7%; females, 36.2%) had only one or two of the drugs prescribed which are not included in the list. It is noteworthy that in 15.1% (males, 16.1%; females, 14.3%), four of the prescribed medicines were not included in the list of priority drugs, while the proportion who had been prescribed more than four drugs that were not included in the price-controlled medicines of 2017 was 8.3% (males, 9.8%; females, 6.4%). The pattern of the number of prescribed NCD drugs, based on whether they are included in the list of priority drugs to manage NCD at primary-level healthcare institutions (published in 2013) or the list of price-regulated drugs (published in 2017), between males and females was similar (p < 0.05).
Distribution of the study population by the number of prescribed NCD drugs (based on verified information through prescriptions) based on whether they are included in the list of priority drugs to manage NCD at primary-level healthcare institutions (published in 2013) or the list of price-regulated drugs (published in 2017).

NCD: non-communicable diseases.
The number of study units is weighted for the population of adults at provincial level.
Self-reported experiences on NCD medicines over the past 5 years were used in this study to evaluate the impact of interventions of the government of Sri Lanka on end-users.
The experiences over the past 5 years (2013–2017) of the participants (n = 1008) on health facility usage for NCD care and availability and affordability of NCD medicines are presented in Table 3. Approximately two-thirds of participants (64.2%; males: 60.9%, females: 67.2%) had exclusively used government hospitals for NCD care during the past 5 years, while another 9.4% (males, 10.5%; females, 8.3%) had mostly used the state sector for NCD care during the past 5 years. The difference of the sector used for NCD care among males and females was not significant (p = 0.057).
Distribution of the study population by experiences of health facility usage for medical follow-up related to NCDs in the past 5 years.

NCD: non-communicable diseases.
The number of study units is weighted for the population of adults at provincial level.
A clear majority (58%) reported their frequency of using health services for NCD follow-up care as bi-weekly or monthly during the past 5 years (males, 56.4%; females, 59.7%).
Inquiring into whether the study units changed the provider of NCD follow-up care during the past 5 years, it was revealed that 75 have done so (Table 4). Of the 75 who had changed places of obtaining NCD treatment, approximately three-fourths (72%) had changed from government sector to private sector. The proportion of males (75.7%) who had changed over to private sector was higher than females (68.4%). When considering the main reason for change, issues related to medicines were the reason for less than half of the study units (40.7%) (males, 40%; females, 41.3%) (p = 0.4). Of the 21 who changed from the private to government sector, the commonest main reason was not being able to afford the private consultation (38%; males, 44.4%; females, 33.3%) and not being able to afford to buy the drugs in the private sector (38%; males, 33.3%; females, 44.4%). The reasons by males and females were similar (p = 0.78).
Distribution of the study population who changed the provider of NCD follow-up care during the past 5 years.

NCD: non-communicable diseases.
The number of study units is weighted for the population of adults at provincial level.
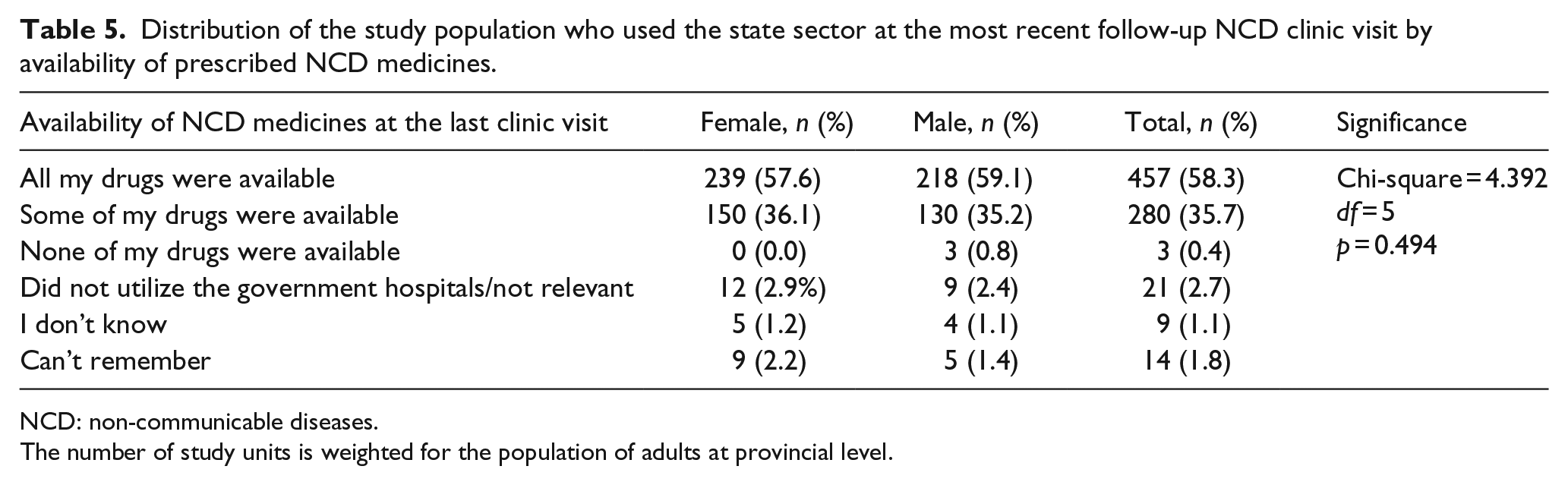
To capture recent experiences of the study participants (n = 1008), the details of the most recent follow-up care for NCD was inquired, as shown in Table 5. A clear majority (n = 784, 77.8%) had used a state sector facility. Experiences of availability of prescribed drugs from the clinic revealed that for a majority (58.3%) all the prescribed drugs had been available (males, 59.1%; females, 57.6%), while almost for all others (35.7%) had some of the drugs available (males, 35.2%; female, 36.1%).
Distribution of the study population who used the state sector at the most recent follow-up NCD clinic visit by availability of prescribed NCD medicines.
NCD: non-communicable diseases.
The number of study units is weighted for the population of adults at provincial level.
Those who did not get all the medicines free (n = 327) (males, 151; females, 176) from the state sector at the most recent follow-up clinic visit to the state sector were inquired into the details and consequences. Among those who did not receive the drugs free, the proportions that were not provided with more than two medicines were a minority (15.8%) (males, 15.5%; females, 15.3%). When comparing the proportions of males and females who did not receive the drugs free according to the number of drugs not provided free, the pattern was similar (p = 0.721). Of the study units who were not provided with all the medicines, a majority 57.5% (males, 60.7%; females, 54.8%) had purchased them for the full duration prescribed. It is noteworthy that a minority 4.6% (males, 2.0%; females, 6.8%) had not purchased them at all. The pattern of self-purchasing of the non-provided drugs was similar among males and females (p = 0.257).
Opinion of the study units on affordability showed that many responded as ‘can afford’ (41.6%; males, 38.8%; females, 44.1%) or ‘can afford with difficulty’ (48.6%; males, 52.6%; females, 54.2%). The pattern of affordability did not differ between males and females (p = 0.766) (Table 6).
Distribution of the study population who did not get all the medicines free from the state sector at the most recent follow-up clinic visit to the state sector by the details and consequences.

NCD: non-communicable diseases.
The number of study units is weighted for the population of adults at provincial level.
Inquiring into whether the money spent was reimbursed by insurance or social welfare revealed that less than 2% had them reimbursed. A total of 143 (43.7%) of the 327 who were not provided all the drugs free of charge by the state sector clinic were aware of the amount they spent to purchase the medicines from private pharmacies. Based on the information from them, on average, a study unit spent LKR1680.83 (weighted mean) to get the prescribed drugs that were not given free of charge at the most recent follow-up clinic visit (median, 1000; LKR IQR = 1500.00, IQR3 = 2000.00).
Discussion and conclusion
Writing a prescription is the end process for a doctor–patient consultation, but from the patient’s point of view, it presents many challenges, referred to as medicines burden, 12 which include worry about medicines accessibility, quality and financial burden. All of these can lead to non-adherence and poor clinical outcomes. Hence, as NCDs are on the increase in Sri Lanka and evidence indicates that appropriate use of medicines in the treatment and prevention of NCDs can reduce its burden up to 80%, 13 a cross-sectional survey was conducted among a representative sample of persons with selected NCDs such as hypertension, diabetes, IHD, asthma and obstructive lung disease from all nine districts of Sri Lanka, with an attempt to identify the burden of medicines.
Majority of the data were collected from the participant or his/her close relative. A sensitivity analysis was conducted to assess any evidence of misreporting between the two sources and the results revealed none. Hence, the accuracy of the information collected can be considered to be good. Demographics of our study sample are also representative of the national population statistics, 14 where there is a slight excess of females, majority Sinhala Buddhists, and 86.5% having education above grade 5 level.
Impact of interventions of the government of Sri Lanka
One of the main findings that emerged from this study was that a majority (>60%) prescriptions, irrespective of the source (government or private), the medicines prescribed were the drugs included in the list of priority drugs to manage NCD at primary-level healthcare institutions (published in 2013) or the list of price-regulated drugs (published in 2017). Another is the fact that there were no gender inequalities to either accessibility or affordability of medicines. But, it should be highlighted that only 14% were prescribed with all medicines included in the priority list of medicines published in 2013. The situation was better with the price-regulated list of 2016, where 29% had all medicines included and 31.6% had most except for one or two of the drugs which are not included in the list. Out of the participants who were not provided medicines in the state sector, only 9.6% (n = 20) claimed that between three and five medicines were not provided, while 1% (n = 2) claimed all the medicines were not provided. The number of drugs they were prescribed were three to four. This can be taken as evidence that even the medicines that were not included in the directive of 2013 had been available in the state sector. However, it should be noted that the WHO target for availability of essential medicines is 80% and that the findings was short of the WHO target. Medicines issued to patients in the state sector are those included in the hospital formulary. Therefore, it could be concluded that there is a disparity between the priority list published in 2013 and the 2018 hospital formulary. The interpretation of this finding is that a one-off directive which is not continuously updated does not ensure a continuous supply of medicines. In Sri Lanka, the National Drugs and Therapeutic Committee of the state Medical Supplies Division updates the essential medicines list and the hospital formulary, regularly in line with previous year’s consumption patterns. Unlike the priority list of 2013, the price-regulated list has also been updated regularly, and in 2018, after our study, prices of insulin, glimepiride, sitagliptin and atorvastatin were regulated.
A study conducted in Sri Lanka 15 in six districts assessed the experiences of health managers of government hospitals on availability of essential medicines through in-depth interviews. The managers had identified recurrent shortages of some essential NCD medicines in spite of the government directives.
Usage of healthcare services and perceptions on quality of medicines
This was studied to highlight both positive and negative experiences in both sectors: state and private. Majority of the participants with no significant gender differences had visited only or mostly state sector hospitals for treatment and follow-up of NCDs within the past 5 years. Hence, it could be interpreted that both genders were satisfied with the healthcare services for NCDs provided by the state free of charge.
Less than 10% of the sample (n = 75) had changed the place of getting treatment due to varied negative experiences and a larger number had changed from government to private sector (54 vs 21). But it was thought important to highlight that of them, only 17 (approximately 31.5%) claimed that they changed to the private sector because they perceived quality of the medicines in government sector was poor. Interestingly, one person changed to the government sector as he/she perceived the state sector medicines to be of better quality. Hence, it could be concluded that the majority of both genders were satisfied with the quality of medicines provided by the state.
Very few 9 complained of medicine shortages as a reason for change to private sector. However, it is important to highlight that though small in number, 21 participants changed from private to government, as they could not afford OOPE both to consult a doctor and purchase medicines thereafter. Medicines for NCDs in Sri Lanka are in schedule 2 and need the intervention of a doctor for the prescription. In a previous study, it has been highlighted that in Sri Lanka to privately consult a doctor for the prescription rather than purchase of medicines constituted a major portion of the OOPE. 13 There were no gender differences regarding access and affordability of medicines and perceived quality of medicines in our study.
In this study, adherence to a clinic or doctor follow-up visit was high with a monthly (57%) or bi-monthly (30%) follow-up visits during the past 5 years, and there were no gender inequalities seen. This identified gap should be closed by making use of the pharmacists more effectively in the NCD healthcare teams.
OOPE on purchasing NCD medicines
Regarding OOPE on purchasing NCD medicines, of 39% who claimed they bought medicines, 60% claimed they bought medicines for the full duration of regimen at the mean of expenses of LKR1680 per month or LKR56 per day (US$1 = LKR180). With regards to who paid for the medicines, less than 1% claimed that it is provided by insurance or employer and only 0.5% claimed it is provided by social welfare systems.
Although both genders claimed that medicines were affordable, when viewed in the context of the HIES-2016 survey findings in Sri Lanka the estimated average monthly income of the households of the poorest 40% (first to fourth decile) was LKR22,423 (LKR747 per day) money spent on purchasing medicines would be approximately 7%–8% of their income per day. Although this may not lead to a catastrophic situation by the WHO 16 definition of catastrophic household expenditure, it will certainly cause them severe financial inconveniences. The study in 2016 15 also included 195 patient exit interviews in which it was identified that 50% of the patients had to spend OOPE for drugs that were not prescribed and or under laboratory investigations.
Hence, the current price controlling of essential medicines should be periodically reviewed to make more essential medicines affordable as availability in government institutions is below the WHO target of 80%.
Among several strengths, the study is not free from limitations. The study did not measure or report on the perception of the users on the effectiveness of drugs in terms of whether the NCDs were well-controlled in patients with good adherence. Furthermore, we could not present the analysis to assess whether the medications that were not available are consistently the same.
In conclusion, the usefulness of this study is that it provides real-life experiences of patients on the burden of medicines in their chosen healthcare facility. Studies done in the past on availability and affordability at the pharmacy is only part of the story. This study has attempted to cover more of the story, but a gap still remains on outcome experiences. Although we did not use previously validated tools, the findings of this study highlight the high dependency on the state for provision of NCD treatment and long-term follow-up of NCDs by the majority of persons over 50 years and above, and their positive and negative experiences regarding accessibility and affordability of medicines for NCDs, gender equalities in usage of healthcare facilities, accessibility and affordability of NCD medicines, low impact of a state intervention to increase accessibility of medicines for NCD without regular updates and the higher impact of price regulation. The information would be beneficial to government policy makers in achieving sustainable goals of improved access to essential medicines set out in the global NCD targets and the sustainable development goals (SDGs) as the majority of the Sri Lankan population with common NCDs shows a high dependency on the state healthcare system.
Footnotes
Appendix 1
Distribution of the sample by district, number of clusters and the sample weights.

| Province | District | Number of clusters | Sample collected | Sample weight |
|---|---|---|---|---|
| Western | Gampaha and Colombo | 8 | 202 | 0.33 |
| Northern | Jaffna | 4 | 100 | 1.81 |
| Eastern | Batticaloa | 4 | 100 | 1.21 |
| North Central | Anuradhapura | 4 | 102 | 1.50 |
| Central | Kandy | 4 | 100 | 0.74 |
| North Western | Puttalam | 4 | 100 | 0.81 |
| Uva | Badulla | 4 | 100 | 1.50 |
| Sabaragamuwa | Kegalle | 4 | 102 | 1.00 |
| Southern | Hambantota | 4 | 102 | 0.78 |
| Total | 40 | 1008 | 9.68 | |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.