
Abstract
Background:
Patients with acute basilar artery occlusion (BAO) and low-to-moderate symptoms (National Institutes of Health Stroke Scale [NIHSS] < 10) are poorly represented in thrombectomy trials. Our objective is to compare thrombectomy and best medical management (BMT) in this population.
Methods:
We compared data of all consecutive patients presenting with an initial NIHSS < 10 and acute symptomatic BAO included in two registries. The main outcome was the proportion of patients achieving a 3-months favorable outcome (mRS 0-2 or equal to the pre-stroke value). Secondary outcomes included the proportion of patients with an excellent outcome (mRS 0-1 or equal to pre-stroke value), overall mRs distribution (shift analysis) and mortality. Effect sizes for thrombectomy versus BMT alone were calculated using binary or ordinal logistic regression model before after considering confounders using the inverse probability of treatment weighting (IPTW) propensity score method.
Results:
One hundred twenty-seven patients were included: sixty-four patients treated with thrombectomy (mean ± SD age: 63.4 ± 16.1) and sixty-three with BMT (mean ± SD age: 69.0 ± 14.3). There was no significant difference between groups for the rate of 3 month-favorable outcome or mortality. After propensity-score adjustment, thrombectomy was associated with a significantly higher chance of excellent outcome at 3 months (mRS 0-1 or equal to pre-stroke value; adjusted OR, 2.68; 95%CI, 1.04–6.90; p = 0.041).
Conclusion:
Our study suggests that thrombectomy in patients with low-to-moderate symptoms (NIHSS < 10) due to BAO does not improve the rate of favorable outcome but could lead to a higher chance of excellent outcome at 3 months.
Trial Registration: ETIS Registry. http://www.clinicaltrials.govNCT03776877
Keywords
Introduction
Acute basilar artery occlusion (BAO) is a rare subtype of strokes with large-vessel occlusion associated with a high morbidity and mortality. 1 Even though two randomized controlled trials (RCTs) had failed to show superiority of EVT over best medical management (BMT) in patients with acute BAO,2,3 thrombectomy has been widely offered to these patients 4 who often present with severe symptoms 5 and have a poor prognosis especially in the absence of complete and timely revascularization. 6 Two more recent RCTs have demonstrated the superiority of EVT over BMT in this particularly severe type of stroke.7,8 The vast majority of patients included in these four trials2,3,7,8 had severe symptoms at presentation (i.e. a high initial National Institutes of Health Stroke Scale (NIHSS)), and patients with milder symptoms (i.e. an initial NIHSS < 10) were either excluded from the trial 8 or enrolled in insufficient numbers to allow firm conclusions in subgroup analyses.2,3,7 Observational studies of patients with BAO strokes and mild symptoms treated with and without EVT show inconclusive results.9,10
The purpose of this study was to use data from the large, multicenter Endovascular Treatment in Ischemic Stroke (ETIS) registry to compare 3-month functional outcomes in patients with an acute BAO and low-to-moderate symptoms (NIHSS < 10) treated with EVT versus those treated with BMT during the same time period.
Methods
Standard protocol approvals, subjects and patient consent
We performed a multicenter cohort study with data extraction from two French prospective clinical registries of consecutive patients admitted to comprehensive stroke centers (CSC) for acute ischemic stroke: (1) the Endovascular Treatment in Ischemic Stroke (ETIS) registry (NCT03776877) which prospectively collected clinical and imaging data from consecutive patients with acute ischemic stroke who underwent EVT and (2) one prospective registry of patients with BAO treated with BMT only.11,12 For this study, data from January 2012 to May 2019 were used. The local ethics committees approved the use of patient data for this retrospective analysis. Since this study only used anonymized data, the local committees judged that obtaining patients’ consents was not required.
Population
Inclusion criteria were: (1) Clinical symptoms of AIS of the posterior circulation, confirmed by cerebral imaging, with NIHSS < 10 on admission; (2) BAO confirmed on initial noninvasive imaging (cerebral Magnetic Resonance Imaging (MRI) or computed tomographic angiography). Exclusion criteria were patients without primary functional independence (modified Rankin score > 2), non-occlusive thrombus, BAO stenosis without complete occlusion, or isolated posterior cerebral or vertebral artery occlusion.
Treatments
Patients were divided into two groups according to the initial treatment decision: (1) BMT group: patients treated with best medical treatment according to current guidelines. 13 This included the administration of IVT and/or blood-thinners when judged to be indicated by the treating physician. (2) EVT group: patients treated with immediate EVT in addition to BMT. EVT was defined by an endovascular attempt to mechanically extract the clot inside the basilar artery. Patients with a failed EVT (e.g. because of a failure to access the basilar artery) were kept in this group. EVT approach was based on the operator’s preference and etiology, and included mechanical thrombectomy (aspiration, stent-retriever), and stenting with or without angioplasty when judged necessary. The use of pre- and peri-procedural medication (heparin, aspirin, clopidogrel or prasugrel, anti-GpIIB/IIIA antibodies, nimodipine), as well as the anesthesia technique, were left to the operators’ discretion.
Data collection
The following data were retrieved: (1) clinical data (demographic characteristics – age, sex, vascular risk factors, history of stroke, atrial fibrillation, pre-stroke antithrombotic medication), pre-stroke modified Rankin scale (mRS) score, time of symptoms onset or last seen well (LSW), time between LSW and IVT and EVT start, blood pressure at admission, stroke severity (using the National Institutes of Health Stroke Scale (NIHSS) score on admission and at 24 h), 3-months mRS score (by telephone or during a face-to-face interview with an experienced nurse dedicated to clinical research at each center, blinded to the early clinical outcomes). (2) Imaging data: The Posterior Circulation Alberta Stroke Program Early CT Score (PC-ASPECTS)14,15 on diffusion weighted-imaging (DWI) on magnetic resonance imaging (DWI-pc-ASPECTS) or computed tomography was calculated to measure infarct extent on initial imaging. Day-1 follow-up imaging was performed as part of standard care and was used to assess the presence of a hemorrhagic transformation. (3) Treatment data: IVT and EVT time metrics; outcomes of EVT using the modified Thrombolysis in Cerebral Infarction (mTICI score). A successful recanalization was defined as a final mTICI score = 2b−3. (4) Stroke etiology was defined as atheromatous, cardio-embolic, dissection, other certain causes, or undetermined when no cause was found despite exhaustive exploration.
Outcome measures
The primary clinical efficacy outcome was the rate of patients with favorable functional outcome at 90 days, defined as a modified Rankin Scale (mRS) 0–2 (or equal to pre-stroke mRS) at 3 months (favorable outcome). Secondary outcomes were the rate of patients with excellent outcome (mRS 0-1 or equal to pre-stroke mRS) and good outcome (mRS 0-3 or equal to pre-stroke mRS).
Safety outcomes were the rate of patients with hemorrhagic transformation (according to the European-Australasian Co-operative Acute Stroke Study (ECASS) 2 criteria) 16 at day-1 imaging, which was categorized as asymptomatic or symptomatic (defined by a NIHSS score increase of ⩾4 points), and mortality at 3 months follow-up.
Statistical analysis
Quantitative variables are expressed as means (standard deviation) in the case of normal distribution or medians (interquartile range) otherwise. Categorical variables are expressed as numbers (percentage). Normality of distributions was assessed using histograms and the Shapiro-Wilk test. Baseline characteristics were described according to the center’s therapeutic approach (EVT vs BMT) and the magnitude of the between-group differences was assessed by calculating the absolute standardized difference; an absolute standardized difference >10% was interpreted as a meaningful difference. 17 We assessed the effect of the therapeutic approach on main clinical binary outcomes using univariable logistic regression models and calculated the odds ratio (OR) for thrombectomy relative to the BMT group as effect size. We also compared the 90-day overall distribution of mRs (after combining mRs 5 and 6 together) using an ordinal logistic regression model (shift analysis); the common OR (cOR) per 1-point improvement in mRs for thrombectomy relative to the BMT group was calculated as effect size. In order to reduce the effects of potential confounding factors in the between-group comparisons, we also assessed the effect of the therapeutic approach after taking into account these factors using the inverse probability of treatment weighting (IPTW) propensity score method (using stabilized inverse propensity score as weighty in logistic regression models). 18 The propensity score was estimated using a non-parsimonious multivariable logistic regression model, with therapeutic approach as the dependent variable and all the characteristics listed in Table 1 as covariates. Since a strong imbalance in admission NIHSS persisted in IPTW propensity score adjusted cohort (Figure 1), admission NIHSS was added as covariable into the IPTW logistic regression models. Statistical testing was conducted at the two-tailed α-level of 0.05. Data were analyzed using the SAS software version 9.3 (SAS Institute, Cary, NC)
Baseline characteristics.

ASD: absolute standardized difference; BP: blood pressure; BMT: best medical treatment; EVT: endovascular treatment; IPTW: Inverse Probability of Treatment Weighting; IVT: intravenous thrombolysis; MRI: magnetic resonance imaging; mRS: modified Rankin score; NIHSS: national institutes of health stroke scale; pc-ASPECTS: posterior circulation Alberta stroke program early computed tomography score.
Values are expressed as no./No. (%), mean (±standard deviation) or median (interquartile range).
3 missing values in patients treated with thrombectomy.
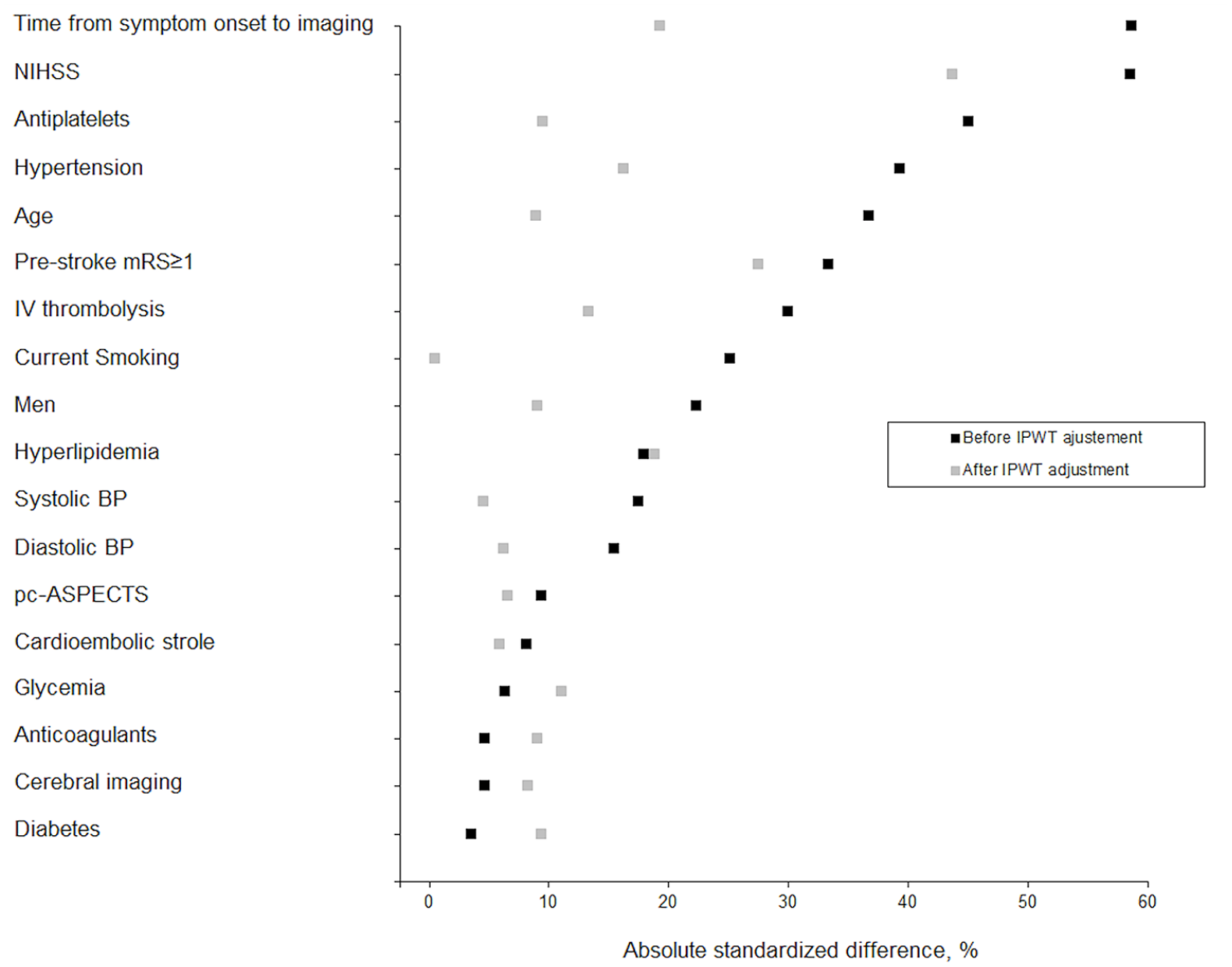
Absolute standardized differences between thrombectomy and best medical treatment groups before and after inverse probability weighting treatment.
Data availability statement
Access to the data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Patient characteristics
From January 2012 to May 2019, 606 patients with an acute symptomatic BAO were admitted to the participating CSCs. Among them, 127 patients had an NIHSS < 10 on admission and were included in the present study (flow diagram shown in Figure 2): 64 patients from the ETIS registry and 63 from the medical cohort. Table 1 shows baseline characteristics of these patients.
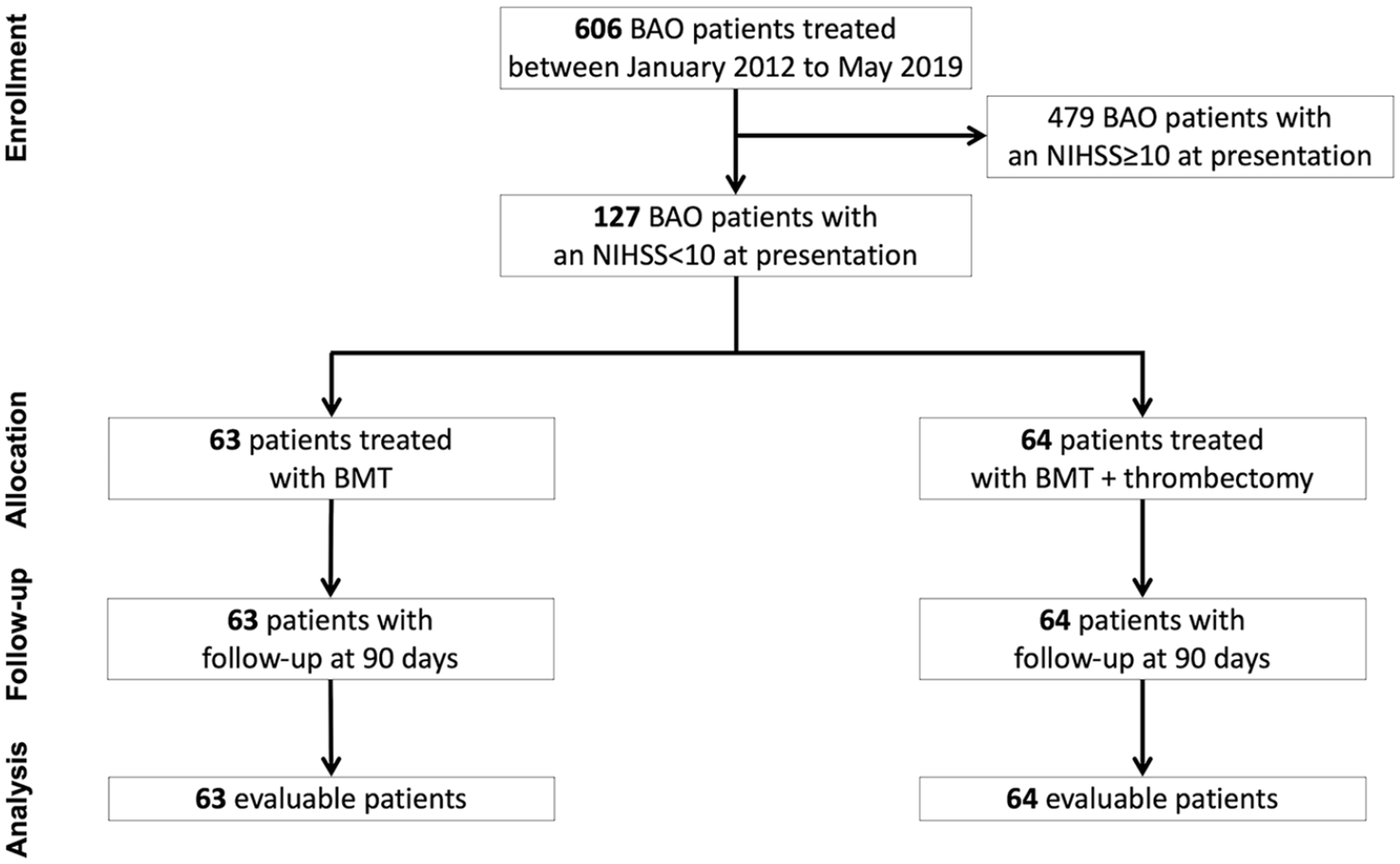
Flow diagram.
The median age of patients was 69 ± 14.3 years in the BMT group versus 63.4 ± 16.1 in the EVT group. Before IPTW adjustment, several significant differences were found, with the the strongest one (i.e. with an absolute standardized difference >50%) being a higher presenting NIHSS in the EVT group: median NIHSS score was 4 (IQR 2-6) in the BMT group versus 6 in the EVT group (IQR 4-6). There was also a lower rate of unknown symptom onset strokes in the EVT group compared with BMT group. These differences were reduced after IPTW adjustment, except for admission NIHSS (absolute standardized difference = 44%; Figure 1).
Procedural characteristics and angiographic outcomes of patients treated by EVT are reported in Table 2. Overall, successful reperfusion was achieved in 98.4% (including 56.3% TICI 3). Of note, 23.4% of patients required adjunctive mechanical therapy (intracranial angioplasty and/or stenting).
Procedural characteristics and angiographic outcomes of patients in the EVT group.

EVT: endovascular treatment; mTICI: modified treatment in cerebral infarction.
Distributions of the 90-day mRS in both groups is shown in Figure 3. Ordinal shift-analysis of mRS between groups showed a common odds ratio per 1-point improvement in mRs (after 5 and 6 combined together) of 1.32 (95%CI, 0.70–2.45; p = 0.39) in unadjusted analysis and 1.79 (95%CI, 0.81–3.96; p = 0.15) in IPTW analysis adjusted for admission NIHSS. A favorable outcome (mRS 0-2 or equal to pre-stroke mRS) at 3 months was achieved in 68.3% of patients in the EVT group and in 71.4% in BMT group (unadjusted OR = 0.86; 95%CI, 0.40–1.84), with no difference in IPTW-adjusted cohorts (adjusted OR = 1.49; 95%CI, 0.55–4.05, Figure 4). There was also no statistical difference between groups regarding good outcome (mRS 0-3 or equal to pre-stroke mRS). The rate of excellent outcome (mRS 0-1 or equal to pre-stroke mRS) at 3 months was significantly higher in the EVT group (57.1% vs 46%) in IPTW adjusted analysis (adjusted OR, 2.68; 95%CI, 1.04–6.90). Clinical worsening occurred in 6 patients (5/6 due to ischemic reason) in the BMT group (9.5%), leading to death in 3 patients (1 respiratory failure, 1 large vertebrobasilar stroke, 1 palliative care decision in a patient in their 90s). Two patients who experienced clinical worsening were initially treated with IVT, four patients with antiplatelet therapy or anticoagulants. No rescue EVT was performed for these patients.
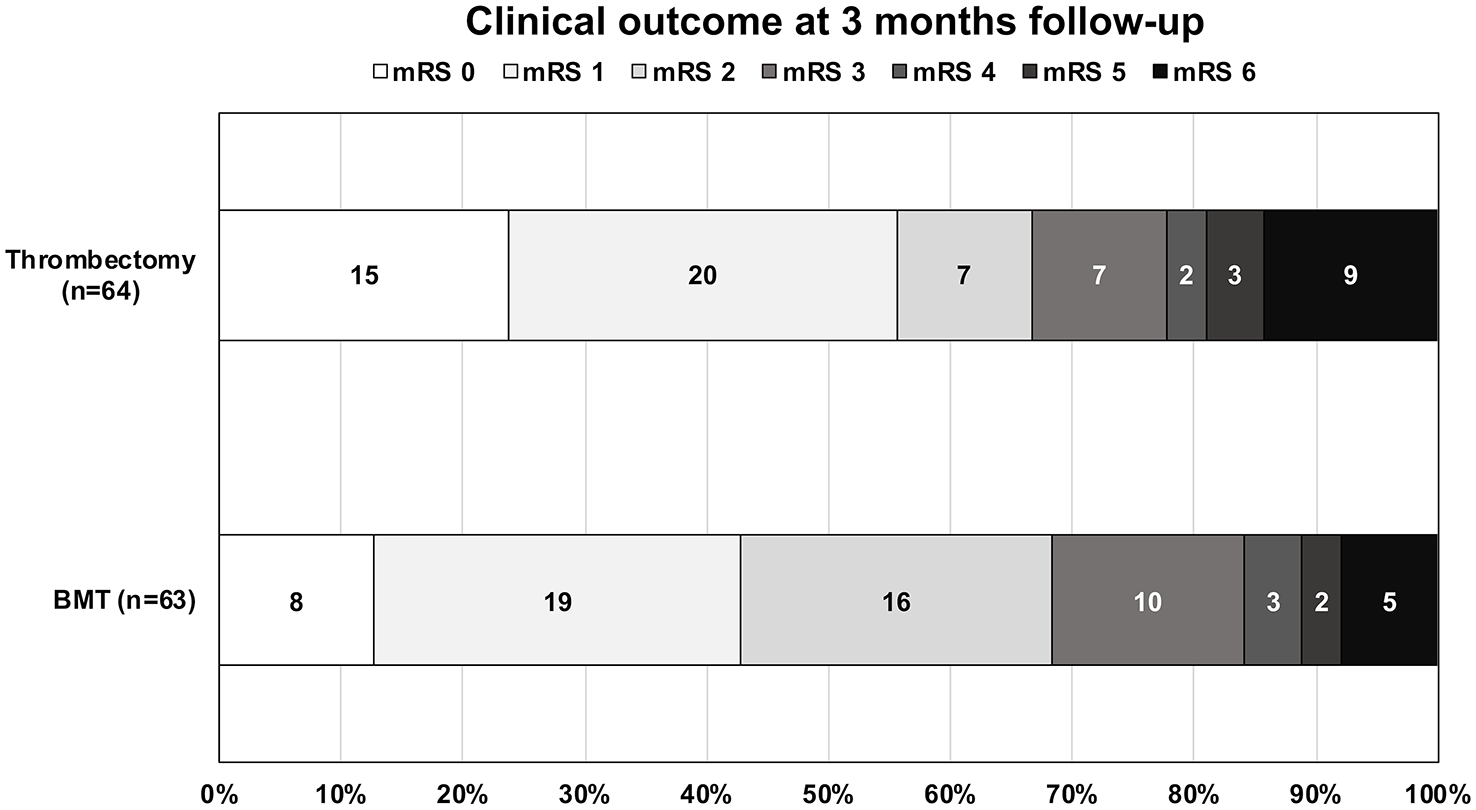
Distribution of 90-day modified Rankin scale in each group. The common odds ratio per 1-point improvement in mRs (after 5 and 6 combined together) was 1.32 (95%CI, 0.70–2.45; p = 0.39) in unadjusted analysis and 1.79 (95%CI, 0.81–3.96; p = 0.15) in IPTW analysis adjusted for admission NIHSS.
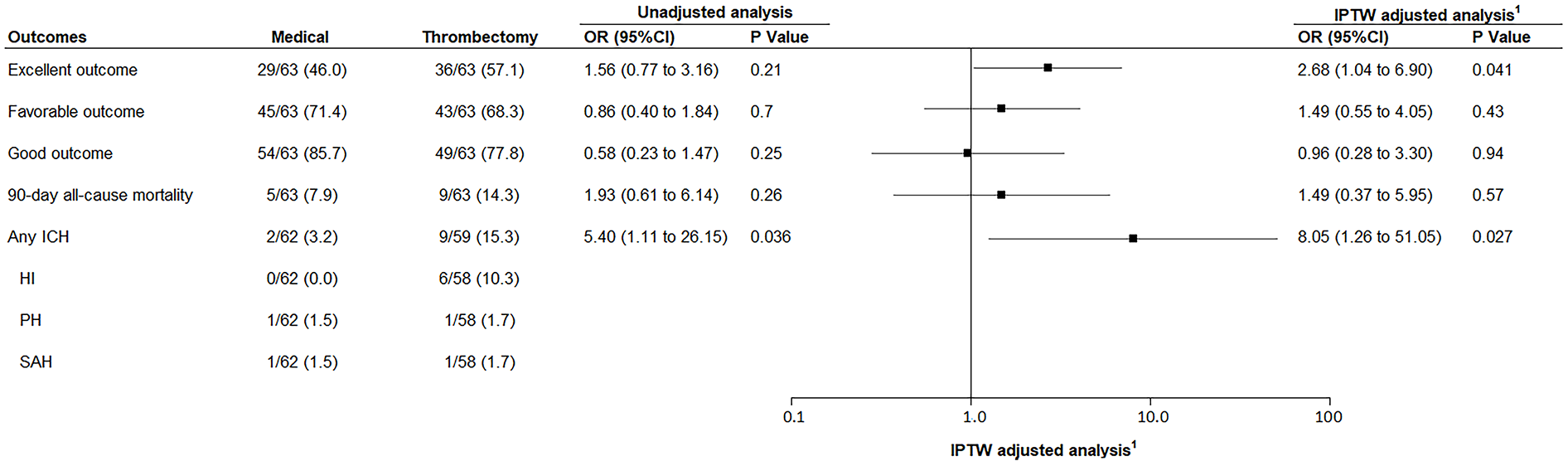
Outcomes in EVT and BMT groups before and after IPTW adjustment.
Rates of 3-month mortality were similar between groups. There was a significantly higher proportion of hemorrhagic transformations in the EVT group (3.2% vs 15.3%, adjusted OR = 8.05; 95%CI, 1.26–51.05) mostly because of the higher proportion of Hemorrhagic-Infarction (HI) type hemorrhages (Figure 4). There was no symptomatic intracranial hemorrhage in both groups.
Discussion
In the large national multicenter ETIS registry, 64 consecutive patients with BAO and NIHSS < 10 underwent EVT from 2012 to 2019. For this study, they were compared to one medical cohort of 63 patients. Our study of minor to moderate stroke with BAO did not show any significant difference between EVT plus BMT versus BMT alone for our primary outcome, which was the proportion of favorable outcome (defined by an mRS 0-2 or equal to pre-stroke mRS at 3 months). However, it did show a significantly higher proportion of patients with an excellent outcome (defined by an mRS of 0-1 at 3 months) in the EVT group as compared to BMT alone. EVT was also associated with a significantly higher proportion of hemorrhagic transformation (of any type) at day-1 imaging, without increased rate of symptomatic intracranial hemorrhage.
Two previous RCTs have failed to demonstrate superiority of EVT over BMT alone for stroke patients with an acute BAO.2,3 The Acute Basilar Artery Occlusion: Endovascular Interventions vs Standard Medical Treatment Trial (BEST) was thought to have suffered from a lack of equipoise19,20 due to difficulty recruiting patients without crossovers and did not find any significant difference in the intention-to-treat analysis. 2 There was no threshold for selection in terms of initial NIHSS but the majority of patients enrolled had a high score and there was no sub-group analysis performed for the group of patients with an initial NIHSS < 10. 2 The BASICS trial also suffered from slow recruitment and failed to show a significant difference between groups. 3 Their subgroup analysis was inconclusive among patients with low-to-moderate deficits (i.e. an initial NIHSS score < 10 – total of 61 patients). 3
Recently, the BAOCHE trial 7 enrolled patients with a basilar stroke 6 h–24 h after onset and showed significant superiority of EVT over BMT alone. However, it included only 12 patients with an initial NIHSS < 10 (6 in each group) and was therefore unable to perform comparisons for this subgroup. 7 The ATTENTION trial 8 enrolled patients within 12 h of onset and also demonstrated clear benefits of EVT, but it excluded patients with an initial NIHSS score < 10. 8
It is well known that the natural history of BAO strokes is often dismal in the absence of treatment, especially in case of severe symptoms at presentation.3,5,21,22 Conversely, patients with milder symptoms are thought to have a better prognosis: they usually have an initial cerebral infarct that is small and/or in non-strategic areas, and their outcome is thus driven by successful recanalization (whether spontaneous or induced by chemical/mechanical treatment). Nevertheless, some of these patients can also have unpredictable and rapid clinical deterioration which of course worsens their prognosis. We are not yet able to predict who these patients are that will deteriorate.23,24
EVT is thought to lead to high rates of successful recanalization which can help clinical recovery6,25 or at least limit cerebral infarct extension and clinical deterioration. EVT can also present technical challenges depending on the type of occlusion and its localization. One commonly encountered and feared situation is the presence of an underlying lesion of the basilar artery or intrinsic basilar stenosis (usually because of atherosclerotic disease) which is known to be a technical challenge for successful and safe recanalization.26–28 Intrinsic basilar stenosis can be met even in cases with low-to-moderate symptoms. This occurred in close to one fourth of EVT patients in our study and required either angioplasty and/or intracranial stenting which undoubtedly impacted the global outcomes. 28 While it is impossible to know if BMT alone would have led to different outcomes, we believe research on predictive factors for these intrinsic lesions would be useful to tailor the management and should be the subject of future randomized control trials.
Our overall results do not suggest any benefit of EVT over BMT using the standard efficacy outcomes used in the anterior circulation strokes (mRS 0-2) 29 or the recent randomized trials for BAO strokes (mRS 0-3).2,3,7,8 This could be explained by the fact that patients’ initial symptoms are often too mild to risk causing any significant disability at 3 months. Moreover, for patients with initial minor stroke, the more relevant outcome measure seems to be the 3-months excellent outcome (defined as an mRS of 0-1 or equal to pre-stroke mRS). In our study, we did find a significant benefit of EVT achieving an excellent outcome at 3 months (57.1% vs 46%), which suggests that EVT could offer a significantly higher chance of having no symptom or at least no disability at 3 months after their initial minor or mild stroke. In terms of safety, there was a significantly higher rate of hemorrhagic transformation at day-1 in the EVT group, which was driven by the higher incidence of hemorrhagic-infarction (HI). We can only speculate that this difference is due to a higher rate of blood-brain barrier disruption after endovascular recanalization, and/or that there was some contrast staining following EVT that was misread as blood on follow-up imaging. 30 Nevertheless, there was no significant difference in terms of symptomatic hemorrhagic transformation or mortality, which is more relevant to assess safety concerns.
Given the underrepresentation of patients with low-to-moderate symptoms in the recent RCTs,2,3,7,8 other types of non-randomized studies are currently the only source of information available in the literature. The BASILAR registry, which is the largest prospective, multicenter registry of consecutive patients treated for an acute stroke with BAO, suggested a benefit of EVT over BMT, however it did not include patients with an initial NIHSS < 10. 31 One recent multicentric observational study among 57 patients with minor stroke (NIH 0-5) and BAO, suggested that IVT + EVT could be beneficial in minor stroke with BAOs, as compared to IVT alone without safety concerns. 10 This study brings more insight into this problem yet, larger randomized trials are required to confirm these findings.
Limitations
The main limitation of this study is the potential confounding bias by indication, due to the observational design, which cannot be ruled out, even after propensity score analysis used to minimize the difference in baseline characteristic. In addition, some imbalanced persisted – in part due to the overall small sample, especially the admission NIHSS, which is a major independent predictor factor of good outcome. However, this imbalance was in favor of the BMT group, as initial NIHSS scores were overall higher in the EVT group. No formal study sample size was calculated, and therefore we could not exclude that some differences may have been overlooked due to the lack of adequate statistical power.
Conclusion
In this multicentric cohort study, there was no significant benefit of EVT over best medical treatment in patients with ischemic stroke secondary to basilar artery occlusion and low-to-moderate symptoms (NIHSS < 10) for favorable outcomes at 3 months, however, significantly more patients in the EVT group achieved excellent outcome (i.e. no new symptoms/disability) at 3 months. This population of patients has been poorly represented in recent randomized controlled trials and should be studied more in depth in future trials.
Footnotes
Glossary
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michel Piotin and Raphaël Blanc detain shares in Basecamp vascular.
Robert Fahed received consulting fees from Stryker Neurovascular and Yocan Medical Systems.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The local ethics committees approved the use of patient data for this retrospective analysis. Since this study only used anonymized data, the local committees judged that obtaining patients’ consents was not required.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Guarantor
Dr. Robert FAHED is the guarantor of the study.
Contributorship
Study design: Cyril Dargazanli, Julien Labreuche, Bertrand Lapergue, Robert Fahed.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Cyril Dargazanli, Mehdi Mahmoudi, Isabelle Mourand, Caroline Arquizan, Robert Fahed.
Statistical analysis: Julien Labreuche.
Supervision: Cyril Dargazanli and Robert Fahed.
All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Statistical analysis
Dr. Julien LABREUCHE, BSc, conducted all the statistical analyses.
Data sharing
Data, analytic methods, and study materials will be made available to any researcher for purposes of reproducing the results or replicating the procedure. Requests to receive these materials should be sent to the corresponding author, who will maintain their availability.