
Abstract
Introduction:
Recent randomized controlled trials demonstrated superiority of mechanical thrombectomy compared to medical therapy in acute basilar artery occlusions, however, little data is available to guide clinicians in functional prognosis and risk stratification.
Patients and Methods:
Data from the retrospectively established PC-SEARCH Thrombectomy registry, which included patients with basilar artery occlusion from eight sites from January 2015 to December 2021, was interrogated. Outcomes were dichotomized into 90-day favorable (mRS ⩽ 3) and unfavorable (mRS > 3). Multivariate logistic regression analysis was performed with respect to the outcome groups and were adjusted for potential confounding baseline characteristics.
Results:
Four-hundred-forty-four patients were included in this analysis. Mean age was 66 [SD 15], with 56% male, and comprised of 76% Caucasian. Patients presented with an initial median NIHSS of 18 and 199 patients (44.8%) achieved favorable 90-day functional outcomes. Independent predictors of favorable outcomes included younger age, pc-ASPECTS > 8 (OR 2.30 p < 0.001), and TICI ⩾ 2b (OR 7.56 p < 0.001). Unfavorable outcomes were associated with increasing number of passes (OR 1.29 p = 0.004) and sICH (OR 4.19 p = 0.015). IA-tPA was an independent risk factor for sICH (OR 7.15 p = 0.002) without improving favorable functional outcomes.
Conclusion and Discussion:
PC-ASPECTS > 8, successful recanalization (TICI ⩾ 2b), first-pass recanalization, and younger age are independent predictors of favorable 90-day functional outcome in thrombectomy treated patients with acute basilar artery occlusion. Conversely, sICH were independent predictors of unfavorable outcomes. IA-tPA and unsuccessful recanalization are independently associated with sICH.

Keywords
Introduction
Pivotal trials demonstrated mechanical thrombectomy (MT) efficacy in anterior circulation large vessel occlusions (LVOs). Yet, until recently, patients with basilar artery occlusion (BAO), an important cause of disability and mortality, were treated without high level of evidence.1–5 Logistical difficulties due to the lower incidence, higher disease mortality, variable presentation, and technical challenges previously limited prospective studies.6–8 While BEST and BASICS did not show MT benefit in BAO, both studies suffered from several shortcomings such as slow enrollment and high rate of crossover.9–11 Recently, the Trial of Thrombectomy 6–24 h after Stroke Due to Basilar-Artery Occlusion (BAOCHE) and Trial of Endovascular Treatment of Acute Basilar-Artery Occlusion (ATTENTION) demonstrated clear benefit of MT compared to medical management alone.12–14 The BEST, ATTENTION, and BAOCHE trials were restricted to Han Chinese patients, and there remains a paucity of data regarding the outcome of this treatment in other ethnicities. In addition, ATTENTION and BAOCHE excluded patients with mild deficit and had low female representation. Several prospective studies exist in an Asian population, however, other than the BASICS prospective registry, no recent dataset exists to validate these findings in a Western population.15–19
The purpose of this multicenter retrospective analysis was to investigate the predictors of functional outcome in patients with posterior circulation stroke treated with mechanical thrombectomy.
Methods
The study was approved by the Institutional Review Board (IRB) at the participating sites. The requirement for informed consent was waived due to the retrospective nature of the study and appropriate under the auspices of Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 20
Registry design
The Posterior Circulation Ischemic Stroke Evaluation: Analyzing Radiographic and Intra-Procedural Predictors for Mechanical Thrombectomy (PC-SEARCH Thrombectomy) registry evaluated consecutive basilar artery occlusion (BAO) patients retrospectively from January 2015 to December 2021. The registry is a multi-center collaboration between eight high-volume comprehensive stroke centers in the United States. All participating centers were invited and compiled de-identified datasheets. Patients were included in this registry if they were over the age of 18 and experienced an acute BAO confirmed by CTA, MRA, and/or Digital Subtraction Angiography (DSA) that was treated by mechanical thrombectomy. All management was performed according to the standard of care per each facility’s procedures and protocols. No exclusion criteria exist for this registry.
Study elements
Baseline demographic data including age, gender, ethnicity, hypertension, history of stroke, vascular risk factors, active COVID, and pre-morbid modified Rankin Scale (mRS) scores were documented. Stroke characteristics included in the database were last known well (LKW), time of decompensation, time of first ER arrival, time of arrival to the comprehensive stroke center, transfer to facility with higher level of care, initial National Institute of Health Stroke Scale (NIHSS), administration of thrombolysis, time of thrombolysis administration, door-IV thrombolysis times, total and itemized Posterior Circulation Alberta Stroke Program Early Computerized Tomography Scores (PC-ASPECTS), anterior-posterior collateralization scores, location of clot, and tandem occlusions.
Intraprocedural variables included time-of-puncture, door-to-puncture times, puncture-to-first pass times, puncture-to-recanalization times, Thrombolysis in Cerebral Infarction (TICI) scores, recanalization at first pass (RFP) (defined as achieving TICI scores 2b or greater in a single pass), presence of underlying intra-cranial atherosclerosis, use of balloon-guided thrombectomy, specific devices used during passes one to five, placement of permanent intra-cranial stenting, type of stent used (if applicable), type of subsequent anti-platelet therapy used for stent placement, total number of passes, evidence of downstream embolization (defined as any embolization of the primary clot in the distal vascular territory), artery affected by downstream embolization, and successful thrombectomy for downstream embolization.
Clinical outcomes included, 90- and day mRS scores. Safety outcomes including intra-procedural perforation, Safe Implementation of Thrombolysis in Stroke Monitoring Study (SITS-MOST) symptomatic intra-cranial hemorrhage (sICH), SITS-MOST asymptomatic intra-cranial hemorrhage (aICH), post-procedural subarachnoid hemorrhage, non-procedural neurological complications (cerebral edema, hydrocephalus, malignant edema, and seizures), and non-procedural hospital complications (itemized by organ system) were recorded. 21
Primary and safety outcomes
Primary Outcome: Identify predictors of favorable functional outcome, defined as mRS of 0–3 in acute basilar artery occlusion patients treated with thrombectomy.
Primary Safety Outcome: Identify predictors of symptomatic intracranial hemorrhage in acute basilar artery occlusion patients treated with thrombectomy.
Statistical analysis
Univariable analysis was performed with respect to the outcome groups. Continuous and scale variables were expressed as means or medians with standard deviations or interquartile ranges, respectively. Comparison of parametric continuous variables were analyzed by student t-test and non-parametric variables were analyzed with Mann-Whitney U-test. Ordinal variables were represented as crude numbers and percentages and subsequently analyzed via Chi-Squared test or Analysis of Variable (ANOVA) were performed as appropriate. Simple and multiple logistic regression analysis was performed with respect to the outcome groups and were adjusted for potential confounding baseline characteristics (if p value was less than or equal to 0.20 on univariable comparison). Multicollinearity was additionally performed on this model.
Statistical significance was defined as two tailed and reaching a p value less than 0.05. Analysis was performed using IBM SPSS Statistics Version 28 (IBM Corp., Armonk, NY).
Results
Registry characteristics
Five hundred nineteen patients were included in this registry with 444 patients included in this analysis. (Figure 1) Seventy-five patients were excluded for not having primary outcome data. Mean age was 66 years (SD 15) and 246 (55.5%) were male. Three hundred thirty-eight (76.0%) patients were White, 69 (15.5%) Black, 3 (0.1%) Asian, and 19 (4.3%) were unspecified. Seventy-nine patients (17.8%) had a prior stroke while 326 (73.4%) patients had a baseline mRS scale of 0. There were 137 (30.9%) patients presenting with NIHSS less than 10, 112 (25.2%) with NIHSS 10–19, and 187 (42.1%) with NIHSS 20 or greater (Table 1).
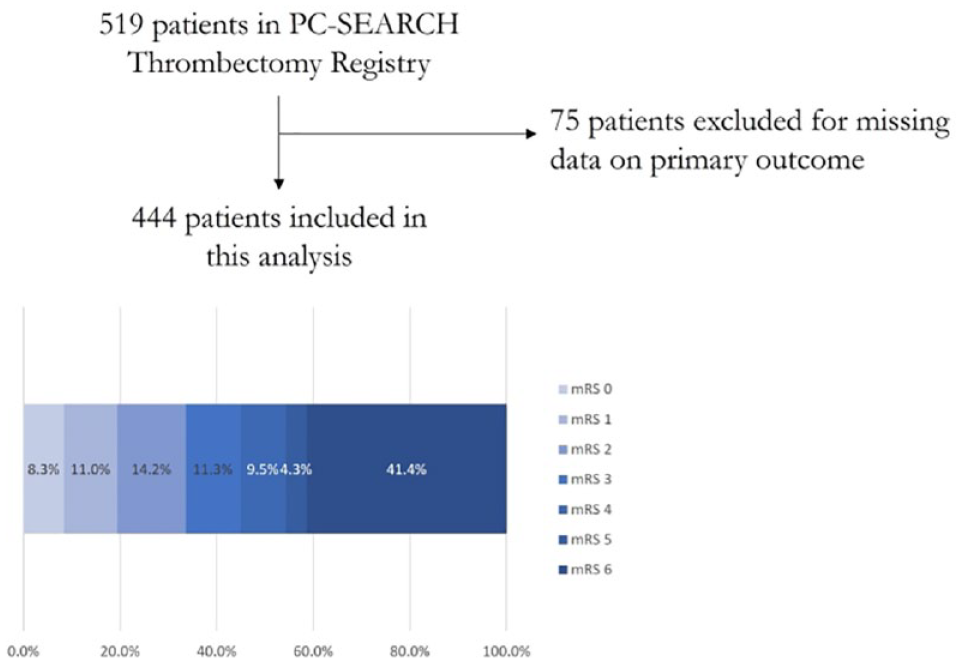
Flow diagram of patients included in this analysis.
Demographics and stroke characteristics.

The median LKW to arrival was 332.5 min (IQR 86–667). Thrombolysis was administered in 116 (26.1%) patients with a median door-to-thrombolysis time of 59 min (IQR 38–103). The occlusion location was proximal in 119 (26.8%) patients, middle in 65 (14.6%), and distal in 138 (31.1%). The median door-to-puncture time and puncture-to-recanalization times were 92.5 min (IQR 31–511) and 42 min (IQR 24–70), respectively. Successful recanalization (TICI 2b or greater) was achieved in 361 (81.3%) patients with 169 (38.1%) achieving RFP. Patients received either first-line aspiration (ASP) catheter (170 [38.2%]) or first-line strentriever (STR) devices (153 [34.5%]); 122 patients did not have the first-line device listed. Downstream embolization was observed in 49 (11.0%) patients. Thirteen (2.9%) patients experienced intra-procedural perforation (Table 2).
Intraprocedural variables and complications.
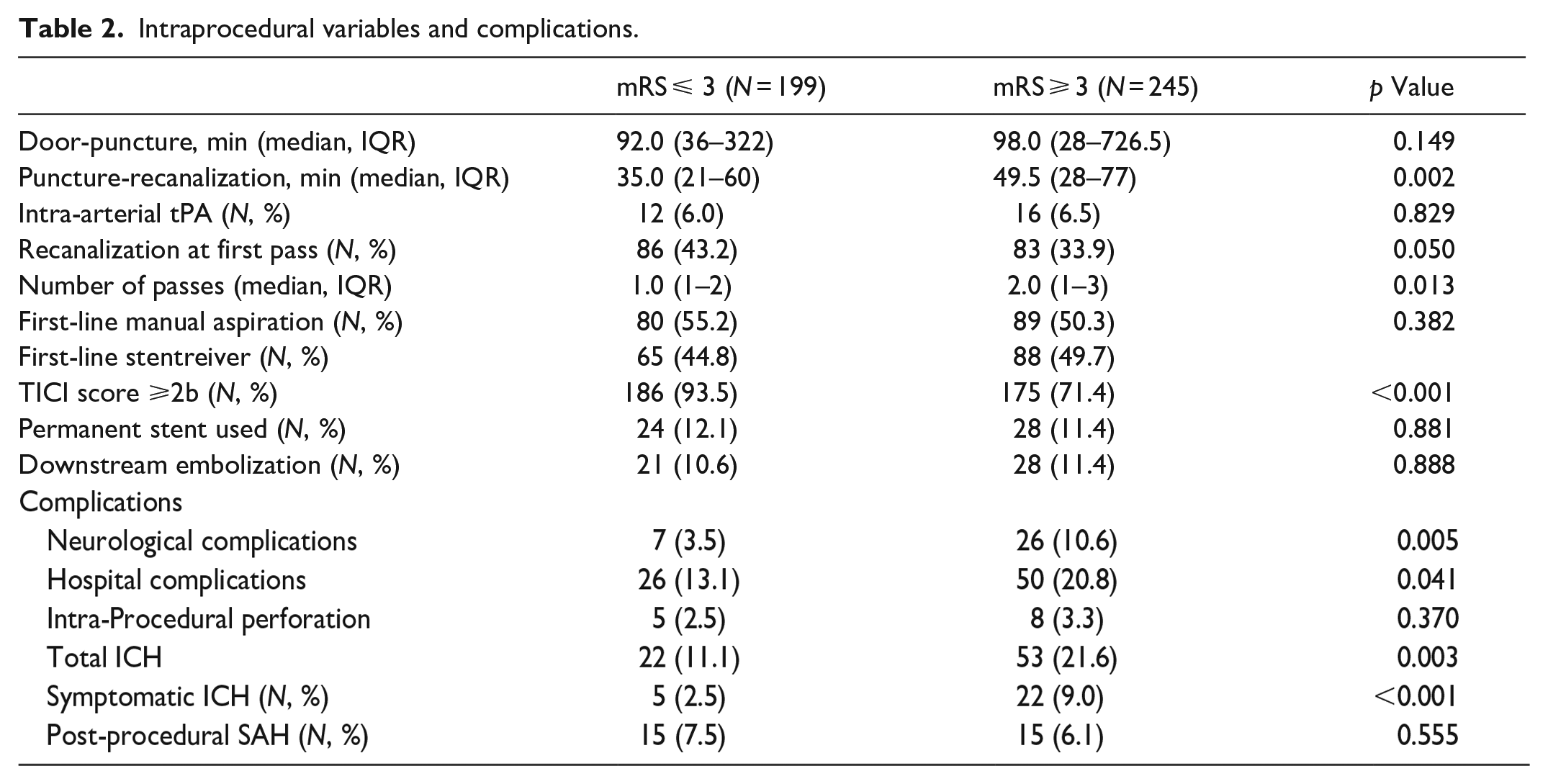
Overall, patients had a median 24-h NIHSS of 10 (IQR 4–20) with 199 (44.8%) patients achieving favorable functional outcomes at 90 days. Seventy-five patients (16.9%) experienced intraparenchymal hemorrhage with 27 (6.1%) symptomatic neurological complications occurred in 33 (7.4%) patients while hospital complications occurred in 76 (17.1%) patients. Multicollinearity diagnostic studies did not reveal any significant correlation between independent factors.
Predictors of functional outcomes
Presenting NIHSS ⩽ 15 associated with favorable outcomes
Patients who achieved favorable functional outcome were younger (62 vs 69, p < 0.001) and less likely to have HTN (64.8% vs 74.3%, p = 0.03). Other vascular risk factors did not differ between the two groups. See Table 1 for dichotomized variables. There was a significant difference in presenting NIHSS in the favorable and unfavorable outcomes groups when ordinally grouped (<10, 10–19, ⩾20). Receiver operator curve (ROC) analysis showed area under the curve (AUC) of 0.643 with a presenting NIHSS of ⩽15 having a sensitivity of 0.66 and specificity of 0.59 when plotted against 90-day functional outcomes. NIHSS delineated into ⩽15 and >15 cohorts were subsequently analyzed by multivariable logistic regression which revealed patients presenting with NIHSS ⩽ 15 achieving favorable functional outcomes (OR 2.86; 95% CI 1.87–4.38; p < 0.001). Tables 1 and 2 summarize characteristics for each group. Figure 2 for unadjusted and adjusted analysis.
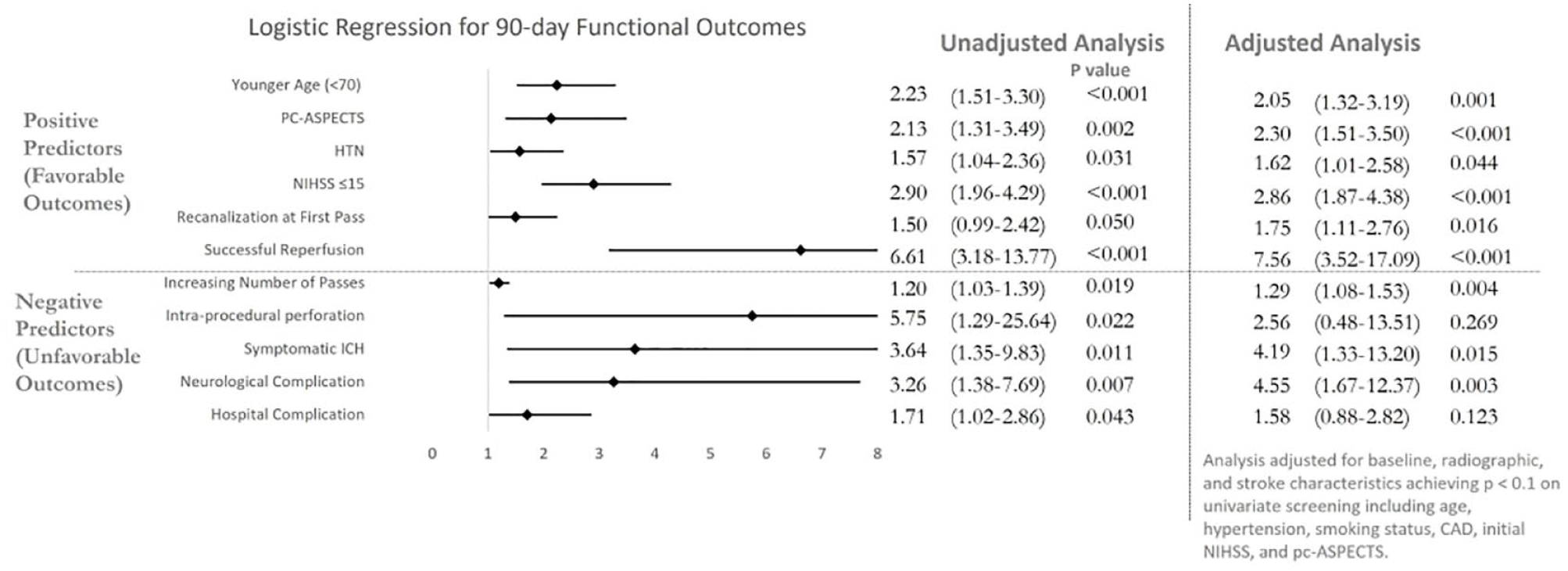
Forest plot of odds ratios with unadjusted and adjusted analysis.
Predictive value in anatomical landmarks
PC-ASPECTS greater than 8 was noted more frequently in the favorable clinical outcome group (77.9% vs 62.2%, p = 0.002). Thalamic (16.2% vs 8.5%, p = 0.03), midbrain (17.4% vs 4.0%, p < 0.001), pontine (24.7% vs 13.4%, p = 0.01), and non-isolated cerebellar involvement (30.0% vs 15.4%, p = 0.002) were more common in the unfavorable outcome group. Anterior-posterior collateralization was equivalent between groups and did not reach statistical significance (44.7% vs 38.4%; p = 1.00). In multivariable analysis, thalamic (OR 2.58; 95% CI 1.10–5.84; p = 0.033), midbrain (OR 6.05; 95% CI 2.36–15.51; p < 0.001), and pontine (OR 2.01; 95% CI 1.15–3.95; p = 0.02) lesions were significantly associated with unfavorable outcomes. See Figure 2 for unadjusted and adjusted analysis. See Figure 3 for diagram of adjusted stroke location analysis.
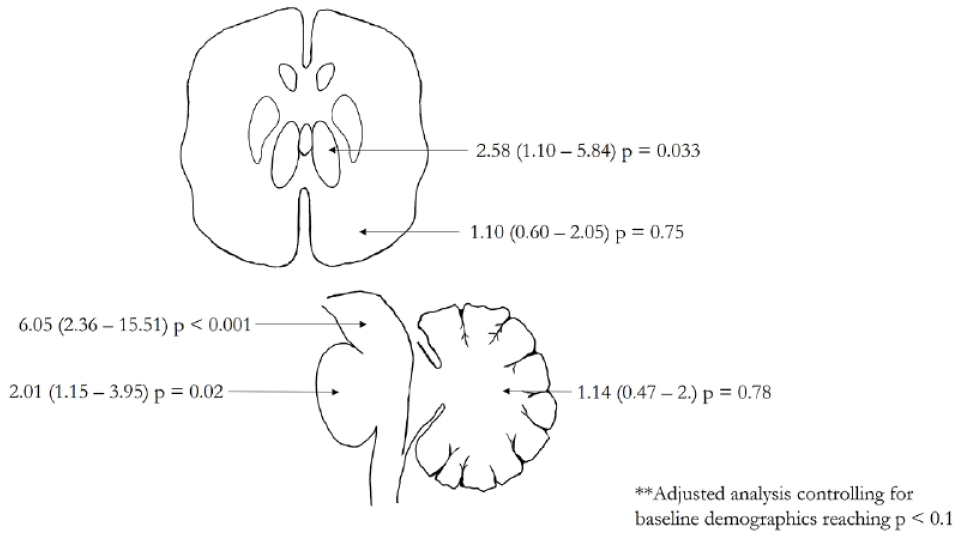
Adjusted odds ratios for ischemic lesions associated with 90-day unfavorable functional outcomes.
Successful recanalization leads to improved functional outcomes
Recanalization at first pass (43.2% vs 33.9% − OR 1.75; 95% CI 1.11–2.76; p = 0.016) and successful recanalization (93.5% vs 71.4% − OR 7.56; 95% CI 3.52–17.09; p < 0.001) were significant predictors of favorable 90-day functional outcomes on adjusted analysis. RFP (54.8% vs 45.3%; p = 0.39) and successful recanalization (51.5% vs 48.5%; p = 0.48) had equal proportions of first-line aspiration catheter and stentriever devices. Increasing number of passes (OR 1.29; 95% CI 1.08–1.53; p = 0.004), however, were associated with unfavorable outcomes. Intra-arterial thrombolysis was given in equivalent proportions in successfully recanalized and non-recanalized patients (6.0% vs 6.5% p = 0.85) without influencing functional outcome. See Figure 2 for adjusted and unadjusted analysis.
IA-tPA and failure to recanalize are risk factors for symptomatic ICH
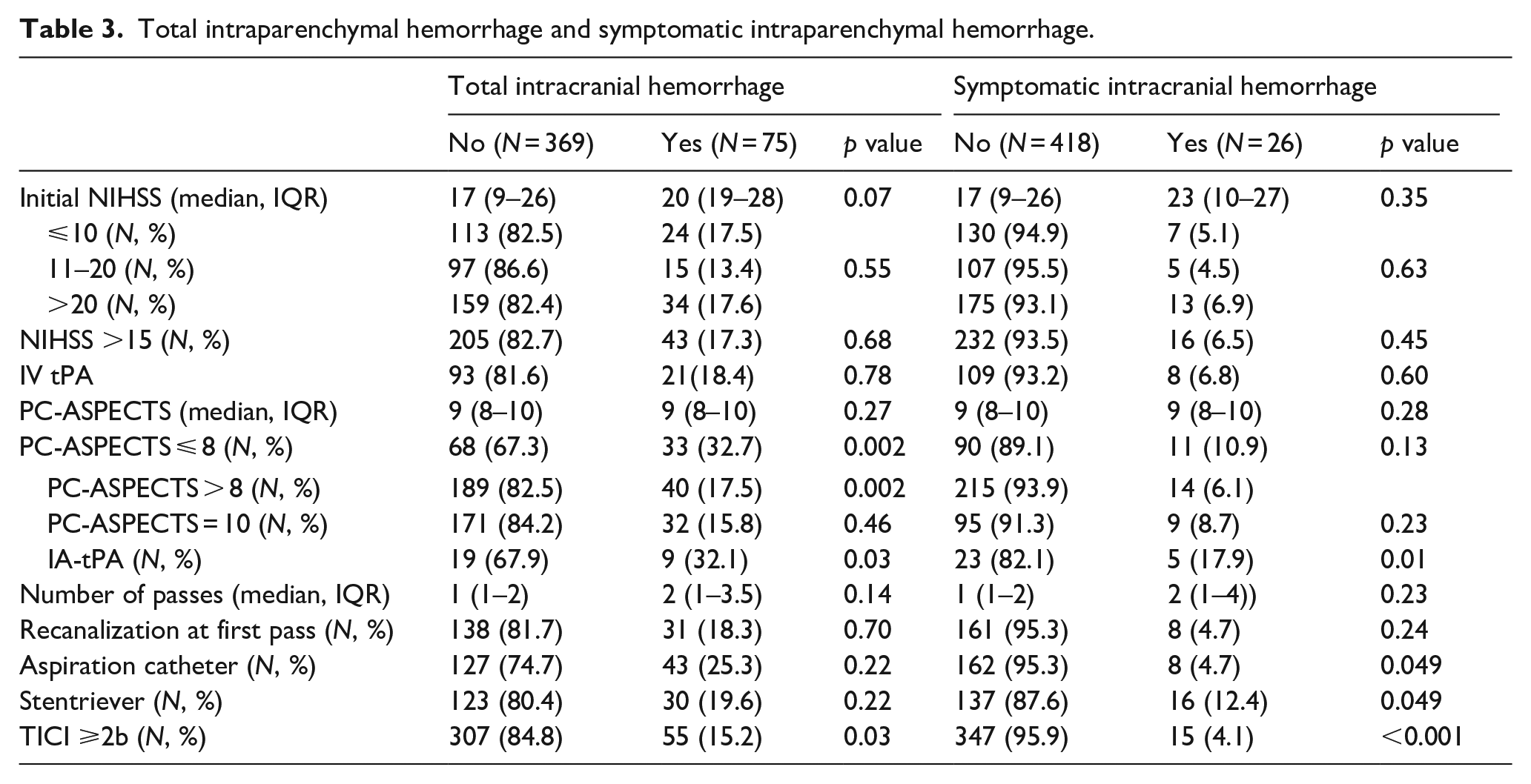
Total ICH (11.1% vs 21.6% − OR 3.26; 95% CI 1.25–8.53; p = 0.016) and sICH (2.5% vs 9.0% − OR 4.19; 95% CI 1.33–13.20; p = 0.015) were associated with achieving unfavorable 90-day functional outcomes on multivariable analysis. More patients received intra-arterial tPA in the sICH group (19.2% vs 5.5% − OR 4.10; 95% CI 1.42–11.86; p < 0.001) and this association retained significance after adjusting for clinical, radiographic, and intra-procedural confounders (OR 7.15; 95% CI 2.00–25.59; p = 0.002). Patients who did not achieve successful reperfusion were more likely to experience ICH (16.8% vs 26.7%; p = 0.007). This association remained significant after adjusting for clinical, radiographic, and intra-procedural variables (OR 3.94; 95% CI 1.46–10.60; p = 0.007). See Figure 2 for adjusted and unadjusted analysis. See Table 3 for dichotomized variables and Table 4 for unadjusted and adjusted total and symptomatic ICH with respect to IA-tPA.
Total intraparenchymal hemorrhage and symptomatic intraparenchymal hemorrhage.
Odds ratios of symptomatic ICH as a function of intra-arterial tPA.

Analysis adjusted for clinical, radiographic, and intraprocedural characteristics achieving p < 0.1 on primary analysis.
Discussion
Mechanical thrombectomy was recently established to provide benefit in patients with acute basilar artery occlusion, and our primary outcome was to identify predictors of functional outcome in this population.22–25 As such, this multicenter retrospective study analyzed the largest US-based thrombectomy-treated posterior circulation LVO registry (PC-SEARCH Thrombectomy Registry). We correlated patient demographic, stroke, radiographic, and intra-procedural characteristics as well as complication rates to 90-day functional outcomes. Patient demographics are typical and reflect those seen in the stroke literature, however, presenting NIHSS in this registry was slightly lower (18 IQR 9–26) than that of the ATTENTION and BAOCHE trials.13,14
Predictors of favorable functional outcomes in this study included younger age, favorable PC ASPECTS, lower stroke severity at presentation, and successful reperfusion. Conversely, symptomatic intracranial hemorrhage, and neurological complications were independent predictors of unfavorable functional outcomes at 90-days. This is concordant with other observational studies and suggests that younger patients with milder symptoms and favorable radiographic studies fare better while those with stroke-related complications have poor prognosis.26–30
Furthermore, ischemic lesions on admission CT scan involving thalamic midbrain, and pontine were independently associated with unfavorable outcomes after multivariable analysis. Lesions within these areas result in higher morbidity/mortality since they harbor high density of structures for consciousness, bulbar function, and voluntary movement. This is unlike large cerebellar ischemic strokes which can be managed effectively with medical and surgical methods without severely influencing the patient’s outcome.
Hospital complications were categorized based on organ systems and post hoc analysis revealed that the majority of hospital complications in the registry were related to infectious etiology (57.3%). These complications were more common in patients with poor functional outcomes (20.8% vs 13.1%) which coincides with the higher likelihood of hospital/ventilatory associated pneumonias and catheter associated urinary tract infections.
Symptomatic intracranial hemorrhage conveys poor prognosis in ischemic stroke, including acute basilar artery occlusion.31–34 As such, our primary safety outcome identified predictors of symptomatic intracranial hemorrhage in acute basilar artery occlusion patients treated with thrombectomy. First, our study confirms the previously observed association between sICH and unfavorable outcome (OR 4.19; 95% CI 1.33–13.20). Second, although previous studies correlated higher rates of sICH in thrombectomy patients treated with IV tPA, we did not demonstrate any significant differences in sICH rates with respect to IV tPA. 35 Similar findings were demonstrated in anterior circulation studies.36,37 Third, the ATTENTION prospective registry evaluated IA thrombolysis following thrombectomy and found no functional benefit which aligns with results of our study. However, our study demonstrated higher rates of sICH with IA-thrombolysis (7.15; 95% CI 2.00–25.59) on multivariable analysis, in contrast with the findings of the ATTENTION registry. 38
The CHOICE trial demonstrated that adjunctive IA thrombolysis after successful thrombectomy in the anterior circulation resulted in greater likelihood of achieving the primary efficacy outcome (mRS 0–1 at 90 days). 39 In our study, there were equivalent rates of IA thrombolysis administration in both cohorts (6.0% vs 6.5%) and no significant associations were made following multivariable analysis (OR 0.64; 95% CI 0.23–1.72). It is important to acknowledge the significant differences in the methodology between the CHOICE trial and our analysis, encompassing variations in study design, patient population, and primary outcome. While these differences likely contribute to the contrasting results regarding of the role of IA thrombolysis, there are also substantial differences in anterior and posterior circulation large vessel occlusions. It is conceivable that specific subgroup populations of patients with basilar artery occlusions may still derive benefits from adjunctive IA thrombolysis following successful recanalization. this approach has potential to improve the microvascular clot burden and ultimately lead to improved functional outcome. This analysis also demonstrated higher rates of recanalization at first pass in the favorable functional outcome cohort (OR 1.75; 95% CI 1.11–2.76) which is in line with previous studies.15,40 Most studies evaluating recanalization at first pass included anterior circulation large vessel occlusions. A recent analysis of the Endovascular Treatment in Ischemic Stroke (ETIS) registry exhibited higher rates of primary outcome in patients achieving recanalization at first pass with acute basilar artery occlusion. 24 The effect size was more robust in the aforementioned study but differs from our analysis in which the primary outcome was defined as 90-days mRS 0–2 as opposed to our trial which defined it as mRS 0–3.
No significant difference in device selection was observed between cohorts in our study, which may support the conclusion that RFP is not only influenced by thrombectomy device but other factors, such as clot composition, length, vessel tortuosity and underlying atherosclerosis. 41 This finding is supported by the ASTER trial which observed similar rates of RFP between the two established techniques (aspiration and stentriever) and reaffirmed the positive first pass effect. 42 Although RFP and total number of passes were associated with better outcomes, multivariable analysis showed that successful reperfusion had a stronger association (OR 7.56; 95% CI 3.52–17.09). This implies that safe and successful recanalization has more substantial impact on final functional outcome compared to the rate of RFP in acute basilar artery occlusions.
Our study has limitations. First, the retrospective design without a control group limits any causative determinations from its results. Second, each site independently reviewed its own imaging without the use of a standardized core lab of the PC-ASPECTS and ICH, allowing for a resultant potential operator bias. This raises a further point that our sites utilize CT imaging for thrombectomy selection, as opposed to MRI, which may underestimate ischemia. As such, thrombectomy candidates should continue to be evaluated on multiple factors rather than solely on imaging criteria. Since this is a retrospective study, patient selection bias may have prevented intervention in low pc-ASPECTS CT scans and further prospective investigations will be needed to elucidate the associated magnitude of this finding.
Conclusion
This retrospective analysis conducted with data from eight high-volume comprehensive stroke centers found that younger age, PC-ASPECTS greater than 8, and successful recanalization were associated with good functional outcomes in patients with BAO treated with MT. Intra-arterial tPA was shown to have higher rates of sICH without conferring any benefit. This study corroborates existing literature on predictors of favorable outcome in BAO. It is limited by its retrospective, observational design and further prospective studies are needed to establish these relationships.
Supplemental Material
sj-docx-1-eso-10.1177_23969873241234713 – Supplemental material for Predictors of outcome and symptomatic intracranial hemorrhage in acute basilar artery occlusions: Analysis of the PC-SEARCH thrombectomy registry
Supplemental material, sj-docx-1-eso-10.1177_23969873241234713 for Predictors of outcome and symptomatic intracranial hemorrhage in acute basilar artery occlusions: Analysis of the PC-SEARCH thrombectomy registry by Adam T Mierzwa, Ashley Nelson, Sami Al Kasab, Santiago Ortega Gutierrez, Juan Vivanco-Suarez, Mudassir Farooqui, Ashutosh P Jadhav, Shashvat Desai, Gabor Toth, Anas Alrohimi, Thanh N Nguyen, Piers Klein, Mohamad Abdalkader, Hisham Salahuddin, Aditya Pandey, Zachary Wilseck, Sravanthi Koduri, Niraj Vora, Nameer Aladamat, Khaled Gharaibeh, Ehad Afreen, Hisham Al-Hajala, Julie Shawver, Syed Zaidi and Mouhammad Jumaa in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors listed do not have any conflicts of interest to disclose. The following payments are reported by the listed authors but do not conflict with this analysis. Dr. Mouhammad Jumaa has received general payments (<$1000) and academic funding from Chiesi USA, Genentech, Medtronic, and Stryker. Dr. Sami Al Kasab has received general payments (<$1000) from AstraZeneca Pharmaceuticals, MicroVention, and Stryker. Dr. Santiago Ortega Gutierrez has received general payments and academic funding from Medtronic, and Siemens Medical Solutions USA, Stryker. Dr. Ashutosh P Jadhav has received general payments (<$1000) and academic funding from Medtronic, Viz AI, and Medical Device Business Services, Inc. Dr. Toth Gabor has received general payments (<$1000) and academic funding from BioSense Webster, Medtronic, and Stryker. Dr. Thanh Nguyen has received academic funding from AtriCure.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Each institution was responsible for approval from their local Institutional Research Boards.
Informed consent
Informed consent was waived due to the retrospective nature of the analysis.
Guarantor
Dr. Mouhammad Jumaa
Contributorship
Adam Mierzwa, Ashley Nelson, and Mouhammad Jumaa researched literature and conceived the study. Adam Mierzwa, Ashley Nelson, and Mouhammad Jumaa was involved in protocol development, gaining ethical approval, patient recruitment and data analysis. Adam Mierzwa, Ashley Nelson, and Mouhammad Jumaa wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.