
Abstract
Introduction:
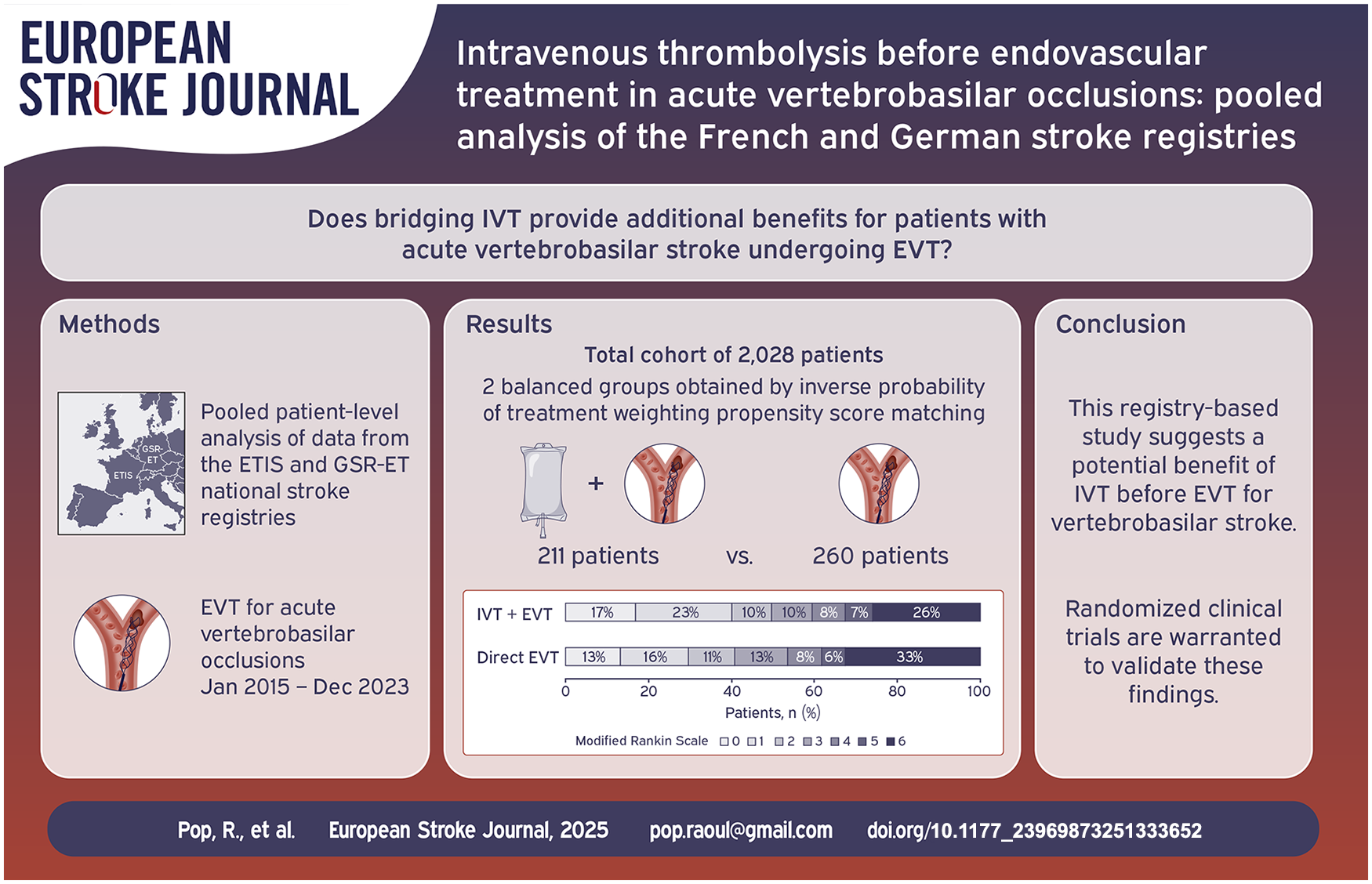
Whether intravenous thrombolysis (IVT) provides additional benefit in eligible patients with acute vertebrobasilar occlusion who undergo endovascular treatment (EVT) remains an open question.
Patients and methods:
We conducted a pooled analysis using data from two national stroke registries, the ETIS registry in France and GSR-ET registry in Germany. Patients who underwent EVT for vertebral and/or basilar artery occlusions from January 2015 to December 2023 were included. The primary efficacy outcome was a favorable shift toward better functional outcomes on modified Rankin Scale (mRS) scores at 90 days. Safety outcomes included 90-days mortality and symptomatic haemorrhagic transformation (sICH). Comparisons between IVT + EVT and direct EVT groups were made combining inverse propensity score matching, probability of treatment weighting (IPTW) and regression models.
Results:
Among 2028 patients treated during the study period, 797 (39.2%) received IVT before EVT, while 1231 (60.7%) had EVT alone. After IPTW matching, we compared 211 patients treated with IVT + EVT to 260 direct EVT patients. Patients in the IVT + EVT group had a favorable shift across the 90-day mRS distribution (common aOR 1.43 per 1-point mRS improvement, 95% CI 1.01–2.04; p = 0.046), higher odds of 90-day favorable functional outcome (aOR 1.56, 95% CI 1.00–2.44; p = 0.049) and lower odds of 90-day mortality (aOR 0.62, 95% CI 0.39–0.99; p = 0.045). IVT was not associated with increased risk of sICH (aOR 1.65, 95% CI 0.62–4.35; p = 0.313).
Discussion:
This registry-based study suggests a potential benefit of IVT before EVT in eligible patients with vertebrobasilar occlusions.
Introduction
Endovascular treatment (EVT) is the standard of care for anterior circulation large vessel occlusions and is increasingly used for vertebral and/or basilar artery occlusions with moderate and severe symptoms after recent publication of two positive randomized trials1,2 and an individual patient data meta-analysis. 3 In the anterior circulation, six clinical trials evaluated the benefit of bridging intravenous thrombolysis (IVT) before EVT in patients with acute anterior circulation large vessel occlusion presenting directly to an EVT capable center.4–9 These individual trials and a pooled patient-level analysis 10 did not prove superiority nor non-inferiority of direct EVT compared to IVT + EVT. Consequently, current guidelines11,12 continue to recommend IVT + EVT for eligible patients with acute anterior circulation large vessel occlusion presenting to an EVT capable center or to a primary stroke center.
Conversely, there is little data available in the literature regarding the efficacy and safety of IVT administered prior to EVT for vertebrobasilar occlusions. The two pivotal clinical trials which demonstrated the benefit of EVT in this population – ATTENTION 2 (Endovascular Treatment for Acute Basilar-Artery Occlusion) and BAOCHE 1 (Basilar Artery Occlusion Chinese Endovascular) – had very low rates of IVT in their EVT arms (31% and 14%, respectively). Criteria for IVT treatment differs in posterior circulation compared to anterior circulation strokes: IVT can be administered for up to 12 and even 24 h after symptom onset in basilar occlusion strokes, compared to 4.5 h in anterior circulation stroke (or 9 h with perfusion imaging selection).12,13 Moreover, symptomatic intracranial hemorrhage after IVT is less frequent in vertebrobasilar stroke compared to the anterior circulation, possibly due to reduced infarct volume and better collateral circulation.14,15 Updated guideline recommendations 13 are likely to encourage the broader adoption of EVT for vertebrobasilar stroke. However, low quality data is available to inform clinicians about the appropriateness of administering IVT to eligible patients before EVT. Given the noted differences between strokes in the two distinct circulations, extrapolating data from anterior circulation stroke trials is not advisable.
To address this knowledge gap, we aimed to assess the efficacy and safety of IVT administration prior to EVT in eligible patients with vertebrobasilar occlusions, using a pooled cohort from two prospective national stroke registries, representative for current clinical practices in Europe.
Materials and methods
Data were collected from two large prospective national registries for endovascular stroke interventions: the Endovascular Treatment in Ischemic Stroke (ETIS) registry is conducted at 33 tertiary stroke centers in France (NCT03776877) and 25 tertiary stroke centers contribute to the German Stroke Registry – Endovascular Treatment (GSR-ET; NCT03356392). Patients were selected for IVT and EVT using local institutional protocols, without prespecified inclusion or exclusion criteria. Patients who underwent EVT from January 2015 to December 2023 were included in the study if any EVT pass attempted and arterial occlusion location was recorded as vertebral artery and/or basilar artery. Hence, pure diagnostic-level catheter angiography was not considered as EVT. Patients’ baseline clinical and radiologic characteristics, procedure details, and outcomes were collected using standardized definitions.
Outcomes
The primary efficacy outcome was a favorable shift toward better functional outcomes in the distribution of the 90-day modified Rankin Scale (mRS) scores. Secondary efficacy outcomes included excellent functional outcome at 90 days (defined as mRS 0–1), favorable functional outcome at 90 days (mRS 0–2), moderate functional outcome at 90 days (mRS 0–3) and recanalization status at the end of the procedure (quantified according to the modified Thrombolysis in Cerebral Infarction (mTICI) classification). Secondary safety outcomes included 90-day mortality, procedural complications(iatrogenic arterial dissection, arterial perforation or embolization to new arterial territory) and symptomatic hemorrhagic transformation at day 1 (quantified according to European Cooperative Acute Stroke Study (ECASS) III criteria). Functional outcome at 90 days was assessed by board-certified vascular neurologists during routinely scheduled clinical visits or, if the patient was unable to attend in person, by a study nurse certified in administering the mRS during a standardized phone interview. Imaging variables, including mTICI scores, were adjudicated by senior interventionalists at the local centers.
Statistical analysis
Quantitative variables are expressed as the mean (SD) for normally distributed parameters or median [interquartile range (IQR)] otherwise. Categorical variables are expressed as numbers (percentage). The patients were divided into two groups according to the administration of IVT before EVT. Baseline characteristics were compared between the two groups using the Student’s t-test for Gaussian continuous variables, Mann–Whitney U-test for non-Gaussian continuous variables, or χ2 test (or Fisher’s exact test when the expected cell frequency was <5) for categorical variables, as appropriate.
In order to reduce the effects of potential confounding factors in between-group comparison, we used propensity-score methods. The propensity score was used to assemble two well-balanced groups (propensity score-matched cohort) and was estimated using a generalized linear mixed model with a binomial distribution and a logit link. The effect of the therapeutic approach was estimated using inverse probability of treatment weighting (IPTW) propensity score method (using inverse propensity score as weight in univariate and multivariate logistic regression models). The propensity score for each individual was defined as the probability of being on the treatment (IVT) given the patient’s age, sex, hypertension, hypercholesterolemia, smoking, diabetes, pre-stroke mRS, pre-stroke antiplatelet treatment, pre-stroke anticoagulation treatment, initial systolic blood pressure, initial National Institutes of Health Stroke Scale score (NIHSS), stroke etiology, admission mode, anesthesia method and time from symptom onset to puncture. Next, weights were calculated as the inverse of the propensity score and were applied to the study population to create a pseudo-population in which confounders were equally distributed across exposed and unexposed groups. Comparison in binary outcomes between groups was made using inverse propensity score weighted logistic models and odds ratios (OR) were calculated. Comparison in the overall distribution of mRS (shift analysis) was performed with an inverse propensity score weighted ordinal logistic model; common OR for 1-point improvement was derived from this model as effect size. Comparisons in outcomes were further adjusted for prespecified confounders (age, admission NIHSS and time from symptom onset to groin puncture). Finally, we assessed heterogeneity of outcomes according to age (⩽80 vs >80 years), admission mode (mothership vs drip and ship), NIHSS at presentation (⩽10 vs >10), time from onset to puncture (⩽6 h vs 6–24 h), arterial occlusion location (vertebral artery vs basilar artery) and initial imaging type (MRI vs CT) by including the corresponding interaction into multivariable inverse propensity score weighted models. Effects are presented as OR with 95% confidence intervals (CI) and were calculated with univariate and multivariate logistic regression models adjusted for age, NIHSS and time from symptom onset to puncture. Statistical analyses were conducted at a two-tailed α level of 0.05. The data were analyzed using STATA version 17 (StataCorp LLC, College Station, Texas, USA).
Results
Population
During the study period, 2028 patients were treated with EVT for acute vertebrobasilar occlusion. Most patients (85.8%) had basilar artery occlusions while 287 (14.2%) had vertebral artery occlusions. 797 patients (39.2%) received IVT before EVT, while 1231 (60.7%) did not. The majority of patients treated with IVT received alteplase; only 30 patients (3.8%) were administered tenecteplase. Selected baseline characteristics, procedural metrics and unadjusted outcomes are shown in Table 1. Several baseline characteristics were imbalanced between the two groups. Patients who received IVT had more favorable baseline characteristics: they had lower prevalence of hypertension and previous stroke and had shorter symptom onset to femoral puncture times. They were also less likely to be on oral anticoagulant therapy and more likely to be initially admitted to a primary stroke center (drip-and-ship). Because the posterior circulation-Alberta Stroke Program Early Computed Tomography Signs (pc-ASPECTS) scores were available in only 19.2% of cases, this variable was not used for adjusted analyses. After propensity score and IPTW matching, two balanced groups were obtained: 211 patients were treated with IVT + EVT and 260 with direct EVT (Table 2 and Supplemental Figure 1).
Baseline characteristics, procedural metrics and unadjusted outcomes.

EVT: endovascular treatment; IVT: intravenous thrombolysis; SD: standard deviation; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; pcASPECTS: posterior circulation Alberta Stroke Program Early CT Score; mRS: modified Rankin Scale; SR: stent retriever; CA: contact aspiration; mTICI: modified Thrombolysis in Cerebral Infarction scale; ICH: intracranial hemorrhage.
Values expressed as numbers (percentage) unless otherwise indicated. Bold denotes statistical significance.
Selected baseline characteristics and procedural metrics in the propensity matched cohort.

EVT: endovascular treatment; IVT: intravenous thrombolysis; SD: standard deviation; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin Scale; SR: stent retriever; CA: contact aspiration; mTICI: modified Thrombolysis in Cerebral Infarction scale; ICH: intracranial hemorrhage.
Values expressed as numbers (percentage) unless otherwise indicated.
Outcomes
In the initial patient cohort, bridging IVT was associated with a favorable shift across the 90-days mRS scale, increased odds of favorable 90-days functional outcome (mRS 0–2), lower odds of mortality and increased rate of first pass reperfusion (mTICI 2b-3) – Supplemental Table 1.
Table 3 illustrates the comparisons of outcomes between the two matched groups. Bridging IVT was associated with a favorable shift across the 90-days mRS scale compared to direct EVT (aOR 1.43 per 1-point mRS improvement, 95%CI 1.01–2.04, p = 0.046 – Figure 1). Bridging IVT was also associated with favorable 90-days functional outcome (aOR 1.56, 95% confidence interval (CI) 1.00–2.44, p = 0.049) and lower odds of mortality (aOR 0.62, 95%CI 0.39–0.99, p = 0.045). There were no significant differences in the rates of hemorrhagic transformation, symptomatic hemorrhagic transformation, procedural complications, final or first pass successful recanalization.
Comparison of efficacy and safety outcomes in the propensity matched cohort.

EVT: endovascular treatment; IVT: intravenous thrombolysis; mRS: modified Rankin Scale; mTICI: modified Thrombolysis in Cerebral Infarction scale; sICH: symptomatic intracranial hemorrhage.
Populations matched for age, sex, hypertension, hypercholesterolemia, diabetes, pre-stroke mRS 0–2, pre-stroke antiplatelet treatment, pre-stroke anticoagulation treatment, initial systolic blood pressure, initial NIHSS score, stroke etiology, admission mode, initial imaging modality, anesthesia method, time from symptom onset to femoral puncture.
Values expressed as numbers (percentage). Bold denotes statistical significance.
Further adjustment for age, initial NIHSS and time from symptom onset to puncture.
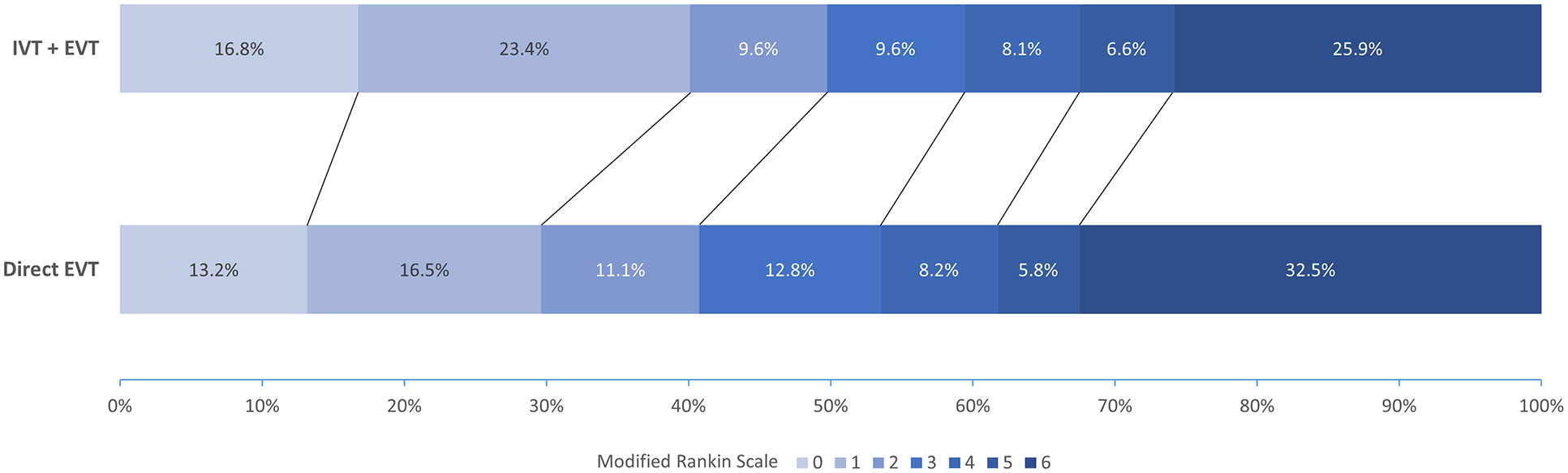
Distribution of the modified Rankin Scale (mRS) scores at 90 days in the propensity matched cohort.
Sensitivity analysis
Since propensity score matching substantially reduced the sample size, we conducted a sensitivity analysis to assess the robustness of our findings and improve statistical power. Specifically, we compared outcomes in the two groups using IPTW and multivariable adjustment, without prior application of propensity score matching – Supplemental Table 2. The association between bridging IVT and improved 90-day clinical outcomes remained unchanged. Additionally, bridging IVT was linked to a reduced number of thrombectomy passes. However, the sensitivity analysis altered the findings on the main safety outcome: bridging IVT was significantly associated with a higher rate of sICH (aOR 2.15, 95% CI 1.05–4.37, p = 0.034).
Subgroup analyses
Figure 2 illustrates an analysis of the treatment effect of bridging IVT on the proportion of favorable functional outcome at 90 days across subgroups. There was no evidence that the effect of IVT would be modified by admission mode, age, imaging modality, symptom severity and treatment delay. There was a trend for significant interaction with arterial occlusion location (vertebral vs basilar artery) without reaching statistical significance (p = 0.058). A trend toward greater benefit from IVT was observed in specific subgroups: mothership admission, age ⩽ 80 years, selection with magnetic resonance imaging, basilar artery occlusion, higher admission NIHSS score (>10) and when EVT was initiated within 6 h after symptom onset.
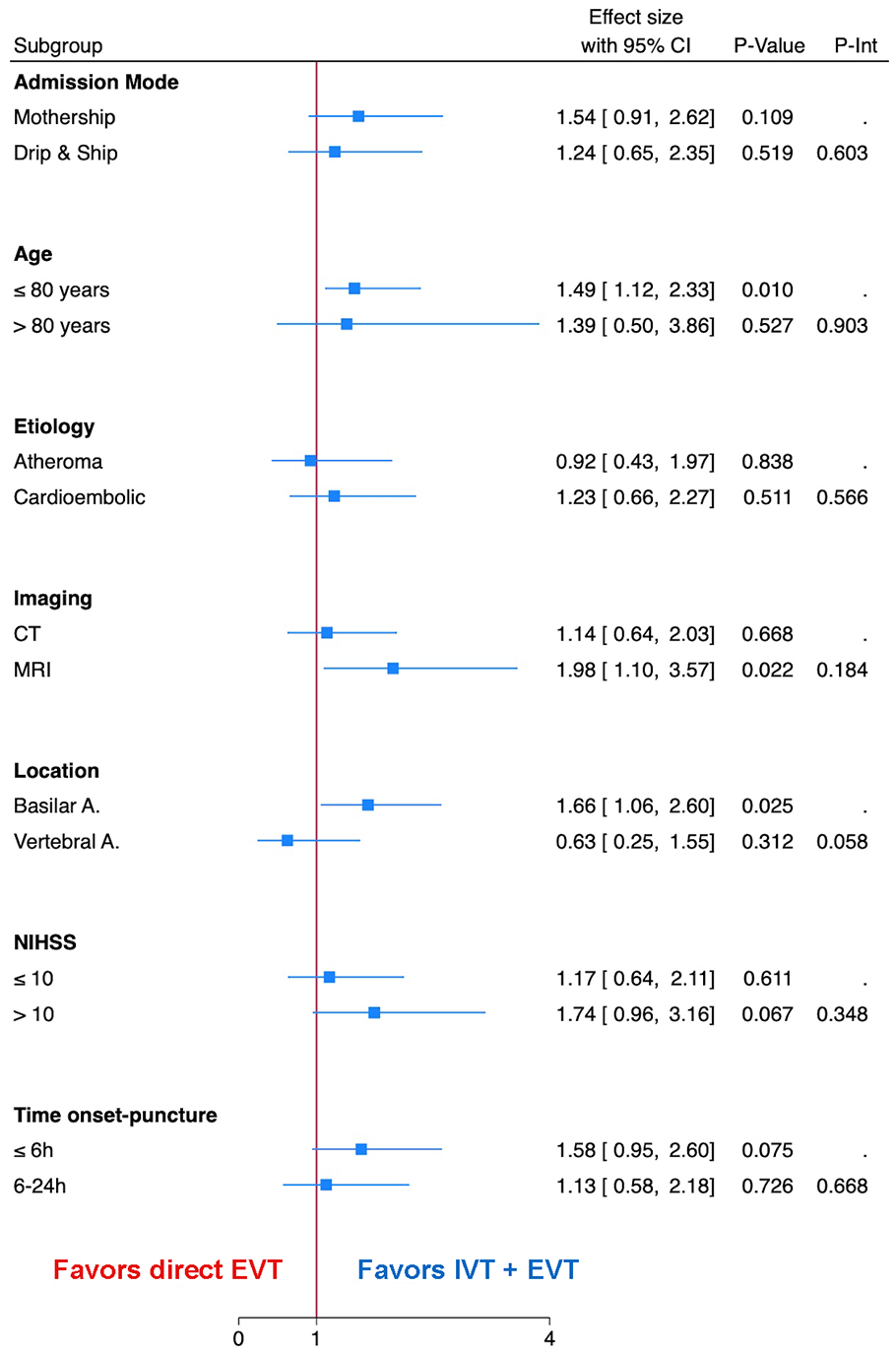
Subgroup analysis. Forest plot for favorable functional outcome (mRS 0–2) at 90 days across key subgroups, depending on admission mode, age, stroke etiology, imaging modality, arterial occlusion location, symptom severity and EVT delay.
We performed a subgroup analysis for two subgroups within the matched cohort, depending on arterial occlusion location. Among 384 patients with basilar artery occlusion, bridging IVT was associated with increased rates of favorable and excellent functional outcome at 90 days, favorable shift across the mRS scale and lower odds of 90-day mortality. (Supplemental Table 3 and Supplemental Figure 2). No significant differences were observed within the 87 patients with vertebral artery occlusions. (Supplemental Table 4 and Supplemental Figure 2).
Discussion
In this study of individual patient data from two prospective stroke registries in Europe (France and Germany), bridging IVT before EVT for acute vertebrobasilar occlusions was associated with increased odds of favorable functional outcome and reduced mortality at 90 days without increased risk of haemorrhagic transformation. In contrast, most previous studies did not show significant differences in outcomes compared to direct EVT.
Four registry studies evaluated the efficacy and safety of bridging IVT before EVT for vertebrobasilar occlusions. Maier et al 16 studied a cohort of 385 patients from the ETIS registry, of which 243 (134 direct EVT and 109 IVT + EVT) were included after propensity score matching. No significant differences were found in rates of moderate or favorable functional outcome at 90 days, sICH or mortality. Knapen et al 17 compared outcomes in 248 patients from the MR-CLEAN registry (123 direct EVT and 125 IVT + EVT). There were no differences in mRS shift analysis, sICH, successful reperfusion, favorable functional outcome, first-attempt successful reperfusion or mortality. Heide and colleagues 18 communicated results from a cohort of 564 patients from the STAR registry (394 direct EVT and 170 IVT + EVT); bridging IVT was not associated with a higher likelihood of favorable functional outcome, nor was direct EVT safer. Napinni et al 19 studied 464 patients from the IRETAS registry and found no difference in successful reperfusion, functional outcomes, and mortality rates between direct EVT and IVT followed by EVT. No significant differences were found in two smaller retrospective institutional or multicenter studies20,21 while a third 22 showed better odds of favorable clinical outcome in IVT + EVT group. Similarly, a meta-analysis 23 of four retrospective cohorts comprising 1127 patients found improved clinical outcomes and reduced mortality with IVT + EVT. Another recently published meta-analysis 24 including data from 2 randomized trials and 10 cohort studies found that bridging IVT in patients with vertebrobasilar occlusions was associated with higher odds of functional independence and lower risk of mortality without increased intracranial hemorrhage as compared to direct EVT.
One possible explanation for the discordance with previously published registry studies is that our study utilized a larger cohort, achieved by pooling individual patient data from two prospective registries. This pooling allowed for the formation of two large groups following propensity matching, which enabled improved detection of a potentially small beneficial effect of IVT. Notably, all registry studies reported positive, albeit non-significant, odds ratios favoring the IVT + EVT approach, suggesting that the additional benefit of IVT may be modest and that large cohorts are required to achieve statistical significance. Another possible explanation may involve differences in subgroup compositions based on occlusion location, imaging modality, degree of neurological deficits, and EVT delay. In particular, the subgroup analysis indicated a trend toward significant interaction between the effect of IVT and arterial occlusion location. The beneficial effects of IVT were maintained in patients with basilar artery occlusions but were not observed in those with vertebral artery occlusions. Two factors may account for this result. First, the basilar artery has more perforators in a highly eloquent zone as compared to the intracranial vertebral artery, and the positive impact of IVT in basilar occlusions may be mediated by enhanced reperfusion of these small perforating arteries. Second, in patients with isolated V4 segment occlusion and patent contralateral vertebral artery, IVT may increase the risk of thrombus migration and distal embolization with negative clinical impact. This finding carries relevant implications for the design of a future randomized trial, suggesting that IVT treatment effect may be increased by excluding patients with isolated vertebral artery occlusion.
Interestingly, we observed a higher 90-days mortality rate in the direct EVT group despite a slightly lower sICH rate compared to the IVT + EVT arm. We can infer two possible explanations for this increase in 90-day mortality which did not seem to be driven by hemorrhagic transformation. First, the reduction in mortality in the IVT + EVT group may be related to an improvement in neurological deficits secondary to the index stroke, which is consistent with the rightward shift observed across the entire mRS scale. Alternatively, this difference could be due to residual indication bias. As noted in the study limitations, residual bias may persist, as patients who met the criteria for IVT had a more favorable baseline profile and complete elimination of residual bias is not feasible in this observational study.
The potential benefit of IVT before EVT justifies the need for a prospective randomized trial. Currently, no completed or ongoing randomized trials specifically evaluate the added value of IVT prior to EVT in patients with vertebrobasilar occlusions directly admitted in an endovascular-capable center. Such a trial will likely face challenges similar to those encountered in anterior circulation large vessel occlusion trials, where outcomes showed neither superiority nor non-inferiority, as treatment effect size of IVT in this context is likely reduced. 10 Additionally, the lower incidence of large vessel occlusions in the vertebrobasilar circulation compared to the anterior circulation will make patient recruitment more challenging. One ongoing randomized trial, the POST-ETERNAL trial (NCT05105633), involves patients with basilar artery occlusion presenting up to 24 h from symptom onset, randomized to receive IVT with tenecteplase versus standard management, which may include IVT with alteplase and/or EVT at the discretion of the physician. The study design does not require all patients to undergo EVT, although, given the inclusion criteria, it is expected that a high percentage of patients will receive EVT. This study aims to prove superiority of the tenecteplase group in terms of excellent functional outcome (mRS 0–1) at 90 days.
Limitations
The primary strengths of this study include a dataset obtained from two prospective nationwide registries of consecutive EVT procedures and a systematic and independent 90-day follow-up with adjudication of clinical outcomes. However, the study design has inherent limitations. First, despite propensity score and IPTW matching, residual bias may persist. In particular, indication bias cannot be fully excluded, as patients in the IVT + EVT group had more favorable baseline characteristics, which may have contributed to differences in outcomes. Second, the multivariate analyses were not adjusted for pc-ASPECTS score because of the large amount of missing data; however, most patients (67%) were selected using CT imaging, which has limited diagnostic accuracy for early ischemic changes in the posterior fossa. Third, we were unable to determine the specific location of the occlusion in the subgroup of patients with vertebral artery occlusions, as this information was not captured in the registry CRF. Fourth, we were unable to calculate the rates of arterial recanalization before EVT, as diagnostic angiographies without EVT were excluded to avoid potential bias. This exclusion was necessary because these diagnostic procedures are not systematically included in the registries. Fifth, we were unable to provide information on the final infarct volume or location, both of which are important mediators of outcome, as this data is not adequately captured in the registry CRF. Finally, the low percentage of patients treated with tenecteplase did not allow for subgroup comparison with alteplase treated patients.
Conclusion
In this large, real-world cohort representative of current European clinical practices, bridging IVT before EVT for acute vertebrobasilar occlusions was associated with increased odds of favorable functional outcome and reduced mortality at 90 days, without safety concerns compared to direct EVT. Prospective, randomized trials are warranted to confirm these findings and validate the observed associations.
Supplemental Material
sj-docx-1-eso-10.1177_23969873251333652 – Supplemental material for Intravenous thrombolysis before endovascular treatment in acute vertebrobasilar occlusions: Pooled analysis of the French and German Stroke Registries
Supplemental material, sj-docx-1-eso-10.1177_23969873251333652 for Intravenous thrombolysis before endovascular treatment in acute vertebrobasilar occlusions: Pooled analysis of the French and German Stroke Registries by Raoul Pop, Stephanos Finitsis, Bertrand Lapergue, Marek Sykora, Daniel Strbian, Joshua Mbroh, Xinchen Hui, Florian Hennersdorf, Ulrike Ernemann, Sven Poli and Benjamin Gory in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Local ethical committees in each of the participating centers approved data collection and analysis for the two national registries.
Informed consent
Verbal informed consent was obtained from the patients and/or their legal representatives before inclusion of data in the ETIS and GSR-ET registry.
Guarantor
BG.
Contributorship
BG and SP conceived the study. SF performed the data analysis. RP, SF and BG wrote the first draft of the manuscript. BL, MS, DS, JM, XH, FH, UE made a substantial contribution to design of the work and interpretation of data. All authors performed data acquisition, reviewed and edited the manuscript and approved the final version of the manuscript.
Data sharing statement
Data are available upon reasonable request
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.