
Abstract
Introduction:
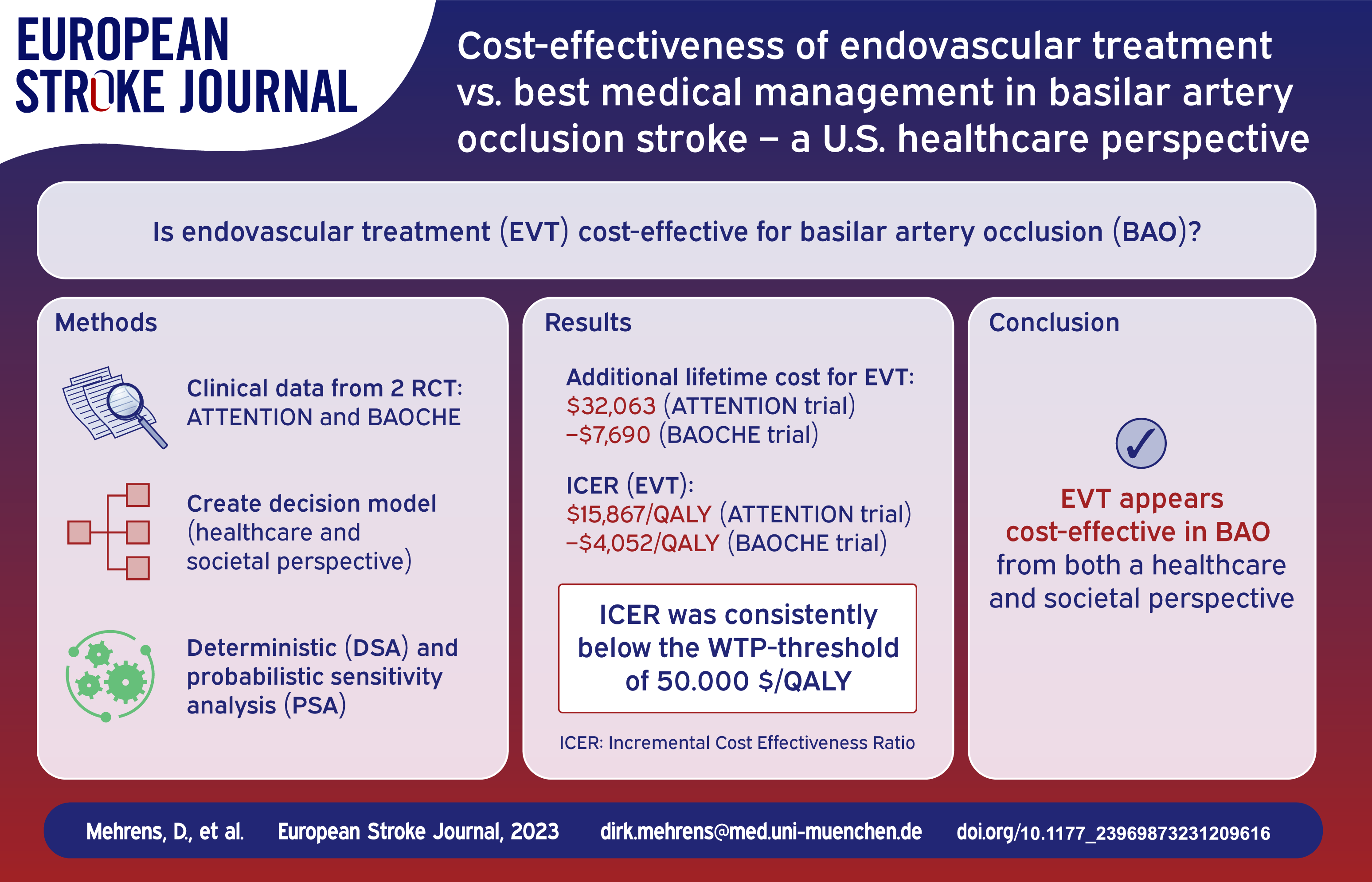
Two recent studies showed clinical benefit for endovascular treatment (EVT) in basilar artery occlusion (BAO) stroke up to 12 h (ATTENTION) and between 6 and 24 h from onset (BAOCHE). Our aim was to investigate the cost-effectiveness of EVT from a U.S. healthcare perspective.
Materials and Methods:
Clinical input data were available for both trials, which were analyzed separately. A decision model was built consisting of a short-run model to analyze costs and functional outcomes within 90 days after the index stroke and a long-run Markov state transition model (cycle length of 12 months) to estimate expected lifetime costs and outcomes from a healthcare and a societal perspective. Incremental cost-effectiveness ratios (ICER) were calculated, deterministic (DSA) and probabilistic (PSA) sensitivity analyses were performed.
Results:
EVT in addition to best medical management (BMM) resulted in additional lifetime costs of $32,063 in the ATTENTION trial and lifetime cost savings of $7690 in the BAOCHE trial (societal perspective). From a healthcare perspective, EVT led to incremental costs and effectiveness of $37,389 and 2.0 QALYs (ATTENTION) as well as $3516 and 1.9 QALYs (BAOCHE), compared to BMM alone. The ICER values were $−4052/QALY (BAOCHE) and $15,867/QALY (ATTENTION) from a societal perspective. In each trial, PSA showed EVT to be cost-effective in most calculations (99.9%) for a willingness-to-pay threshold of $100,000/QALY. Cost of EVT and age at stroke represented the greatest impact on the ICER.
Discussion:
From an economic standpoint with a lifetime horizon, EVT in addition to BMM is estimated to be highly effective and cost-effective in BAO stroke.
Introduction
Endovascular treatment (EVT), when indicated, has become the favorable therapy for large-occlusive ischemic stroke in the anterior circulation compared to intravenous thrombolysis (IVT) with better short-term and long-term clinical outcomes. 1 Acute ischemic stroke (AIS) of the posterior circulation, especially basilar artery occlusion (BAO) represents a less frequent entity with ambiguous symptoms and unfavorable clinical outcomes even after IVT.2,3 Previous randomized controlled trials that aimed to generate high-level randomized evidence for EVT in BAO stroke failed because of lack of equipoise that led to biased enrollment, and high cross-over rates from the medical management to the EVT arm.4,5 Thus, for a long time, no formal evidence for the efficacy of EVT in the setting of BAO stroke was available. This has however changed now, since recently two randomized controlled trials comparing EVT in BAO with best medical management (BMM) alone have been successfully completed and published.6,7 Both studies were conducted in China, including patients up to 12 h from symptom onset (ATTENTION) or within 6 to 24 h (BAOCHE) before EVT, and showed improved functional outcome at 90 days post procedure.
In this cost-effectiveness analysis, we used data from the ATTENTION and BAOCHE trials to compare the long-term costs and cost-effectiveness of EVT in addition to BMM versus BMM alone in AIS patients with BAO.
Methods
We conducted the analysis both from a healthcare perspective and a societal perspective in accordance with the recommendations of the Second Panel on Cost-Effectiveness in Health and Medicine 8 (see CHEERS 2022 Checklist as online Supplemental File). The analyses for both trials were conducted separately.
Study sample
Clinical data were derived from the ATTENTION as well as BAOCHE trial. Inclusion criteria were symptom onset within 12 h or less (ATTENTION), or 6–24 h (BAOCHE) with pre-stroke modified Rankin Scale 0–1 (BAOCHE) or 0–2 (ATTENTION) and NIHSS-score of 6 or higher (BAOCHE) as well as 10 points (ATTENTION) at presentation. The population of both trials were otherwise similar (ATTENTION trial N = 340 (randomization 2:1 ratio, 226–114 patients), mean age 66 ± 11 years (thrombectomy group) and 67 ± 10.2 years (control group) respectively; BAOCHE trial N = 217 (randomization 1:1 ratio, 110–107 patients), median age 64.2 ± 9.6 years (thrombectomy group) and 63.7 ± 9.8 years (control group)). Patients who were randomized to the control arms of the respective trials were treated with BMM, including intravenous thrombolysis if indicated. Those randomized to the EVT arms were treated with EVT in addition to BMM.
Model structure
A decision model was developed using the TreeAge Pro 2022 software, version 22.2.0, TreeAge, Williamstown, MA), see Figure 1. First, a short-run model was used to analyze costs and outcomes within the first 3 months after the index stroke, followed by a long-run Markov state transition state model with a cycle length of 12 months, estimating costs and outcomes over the patients’ lifespan up to 120 years. In the short-run model, patients could enter one of seven health states as defined by the mRS following treatment (i.e. EVT and best medical management in the EVT arm; best medical management alone in the control arm). In each cycle of the long-run model, patients could maintain the same health status (i.e. the same mRS category), suffer a recurrent stroke followed by either recovery to the same mRS category or change to a worse mRS category, or die, either as a result of age-related mortality or stroke-survivor specific mortality. In the base case analysis of this study, we assumed a patient age at stroke onset of 66.5 years (ATTENTION trial) and 65 years (BAOCHE trial) from the clinical data available. The decision model is available on request from the corresponding author.
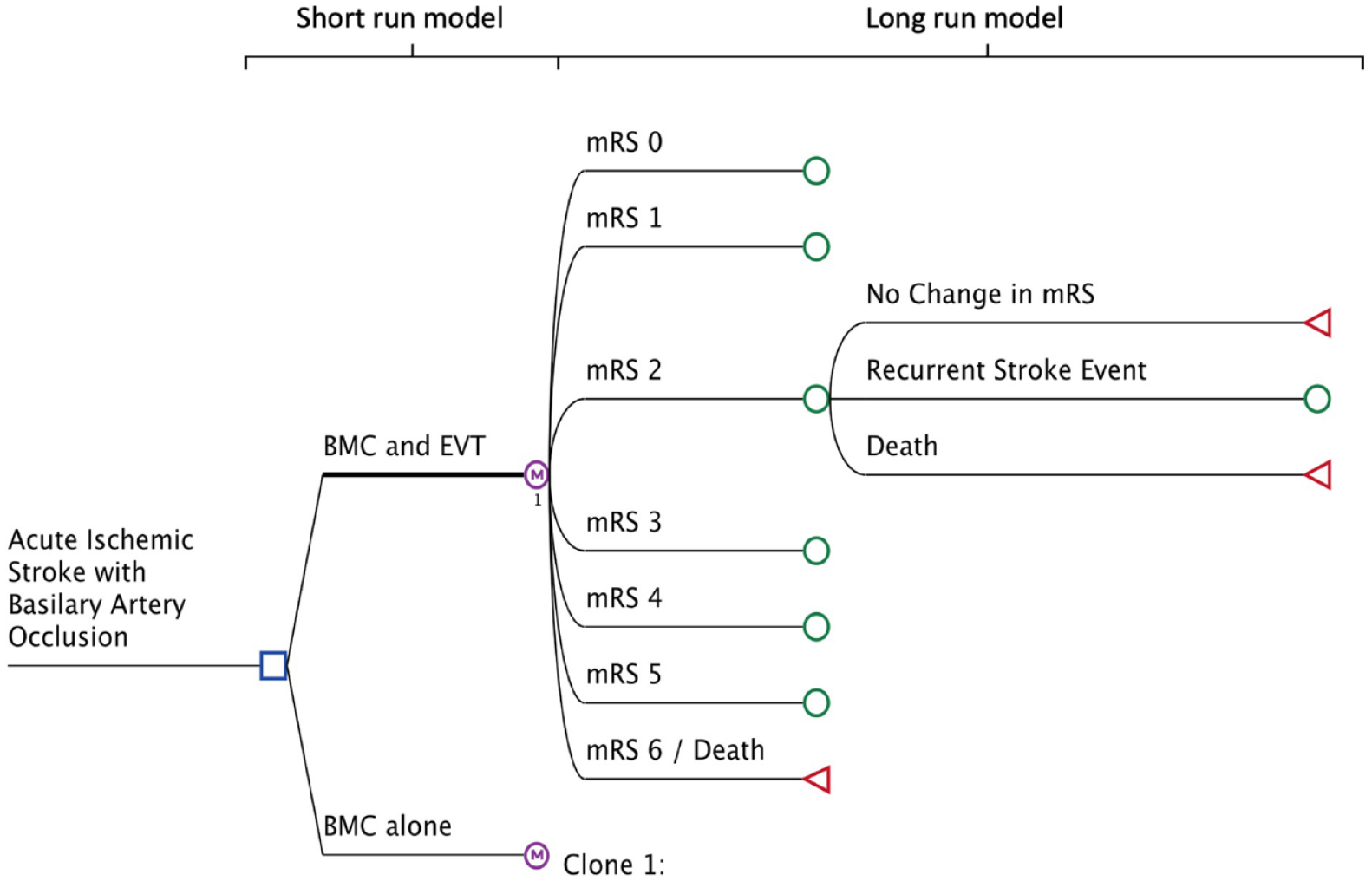
Decision model structure.
Model parameters
Outcome probabilities
The probabilities of achieving a certain mRS state at 3 months in the short-run model were derived from the ATTENTION and BAOCHE trials. Probabilities for long term outcomes beyond 3 months were extracted from large prospective cohort studies9,10 and United States Life Tables 11 , as described previously,12,13 taking into account the risk of recurrent stroke, death, and changes in mRS over time in post-stroke survivors. mRS-specific utility measures were derived from a large prospective cohort study. 14 Other parameters that were used in the model have been published previously.12,13
Healthcare costs (US data)
Estimated treatment cost was derived from the National Inpatient Sample 15 and available literature, as described previously.12,13,16 The cost of EVT over and beyond BMM was estimated to be $15,510, which includes all devices and other procedure-related materials. 16 Costs of BMM, which include the cost of intravenous thrombolysis if indicated, were estimated at $7,421. To account for the fact that not all patients received intravenous thrombolysis as part of BMM, the cost of intravenous thrombolysis was multiplied by the probability of patient receiving intravenous thrombolysis (ATTENTION trial: 31% in the EVT arm vs 34% in the BMM arm; BAOCHE trial: 14% in the EVT arm vs 21% in the BMM arm; modeled with a beta-distribution and assuming a standard deviation of 20%). Healthcare costs other than procedure-related costs that were considered in the first 3 months (short-run model) included supported discharge, rehabilitation, and community care, according to the degree of disability as measured by the mRS at 3 months. 17 Long term costs beyond 3 months from the index stroke included rehabilitation and ongoing costs, according to the degree of disability as measured by the mRS at 3 months. 16 All costs were inflated to November 2021 U.S. Dollars using the medical care component of the consumer price index. 18 Annual discounting of 3% for treatment costs and gained QALYs was applied.
Societal costs (US data)
Costs and cost-effectiveness of EVT in addition to best medical management compared to BMM alone were assessed using the human capital approach, including costs caused by lost productivity and informal care (estimated based on United States Census Bureau wages 19 and United States Bureau of Labor Statistics 20 age-specific employment rates12,13), costs of informal care 13 and costs of lost productivity due to stroke-related premature mortality and disability, as described previously. 13 Details of the model parameters and respective references are shown in Table 1.
Base-case values and model input parameters.
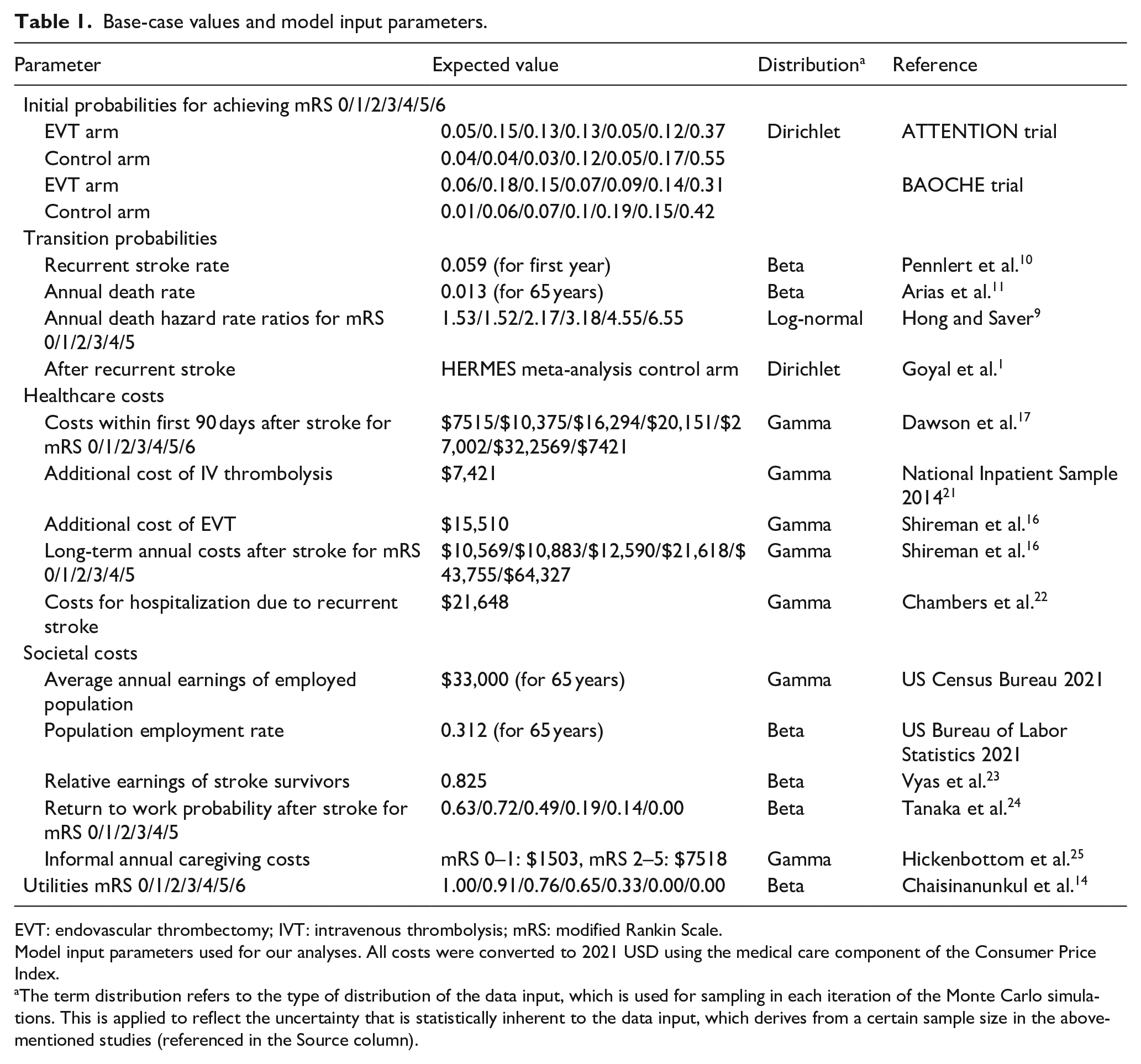
EVT: endovascular thrombectomy; IVT: intravenous thrombolysis; mRS: modified Rankin Scale.
Model input parameters used for our analyses. All costs were converted to 2021 USD using the medical care component of the Consumer Price Index.
The term distribution refers to the type of distribution of the data input, which is used for sampling in each iteration of the Monte Carlo simulations. This is applied to reflect the uncertainty that is statistically inherent to the data input, which derives from a certain sample size in the above-mentioned studies (referenced in the Source column).
Outcomes
Cost-effectiveness of EVT in addition to BMM was assessed with the incremental cost-effectiveness ratio (ICER), which reflects the difference in costs between EVT with BMM and BMM alone and the respective gain in quality-adjusted life years (QALYs).
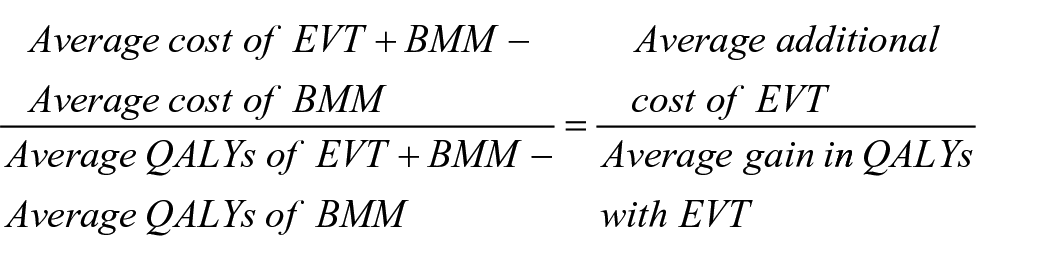
QALYs hereby reflect both survival time and quality of life: 1 year of life in a completely healthy state results in one QALY, and 1 year of life with any health-related impairment results in <1 QALY, depending on the nature and degree of impairment. 26 QALYs for each mRS category were calculated using utility values associated with each mRS state. Further, the net monetary benefit (NMB) of EVT with BMM and BMM alone was calculated. The NMB equals the mean QALYs per patient gained with EVT multiplied by the willingness-to-pay (WTP) for one QALY minus the mean additional cost of EVT (compared to BMM) per patient. According to common convention, upper and lower WTP thresholds were set at $100,000 and $50,000 per QALY.

Sensitivity analysis
Every parameter used in the decision model was assigned a distribution type reflecting its probability density function. We then performed probabilistic sensitivity analysis using 10,000 second order Monte Carlo simulation runs to assess for the influence of simultaneous changes in model input parameters. Median costs, QALYs, and ICER for both EVT with BMM and BMM alone were obtained from the 10,000 simulations and graphed in a scatter plot.
For both studies we performed additional deterministic sensitivity analyses from a healthcare as well as societal perspective for the following parameters. Age at stroke (range from 65 to 80 years of age), costs for EVT ($12,408−$46,530), costs for IVT ($5637−$8905), rate of IVT in the EVT group and BMM group (15%–100%, respectively) as well as annual discounting (3%–10%). The results were presented as tornado diagrams, sorting the parameters by their impact on the ICER.
Results
Both trials reported good functional status (modified Rankin Scale of 0–3) at 90 days in 46% (ATTENTION trial) and 55% (BAOCHE trial) of patients in the EVT group compared to 23% (ATTENTION trial) as well as 43% (BAOCHE trial) in the control group. The mortality in both trials was lower after EVT (37% in the ATTENTION trial and 31% in the BAOCHE trial) compared to the control group (55% and 42%, respectively). Clinical outcomes with EVT and BMM are reported in detail elsewhere.6,7
Base case analysis
Analysis of the ATTENTION as well as BAOCHE trials showed similar results. Both trials led to incremental QALYs of 2.0 (ATTENTION) and 1.9 (BAOCHE), thereby doubling treatment effectiveness regarding clinical outcome. From a healthcare perspective, EVT in addition to BMM resulted in increased lifetime costs in both trials ($37,389 in the ATTENTION trial and $3516 in the BAOCHE trial). Nonetheless, EVT in addition to BMM yielded a higher NMB compared to BMM alone at the higher (EVT: $185,119 (ATTENTION)/$196,027 (BAOCHE) vs BMM only: $20,431 (ATTENTION)/$9739 (BAOCHE)) and lower (EVT: $−15,791 (ATTENTION)/$−26,425 (BAOCHE) vs BMM only: −$79,440 (ATTENTION)/−$117,811 (BAOCHE)) WTP thresholds. The ICER amounted to $18,502 (ATTENTION) as well as $1853 (BAOCHE).
The societal perspective yielded equally favorable results. In addition to BMM, EVT resulted in lifetime cost savings of $7690 in the BAOCHE trial and only minor additional lifetime costs of $32,063 in the ATTENTION trial. EVT in addition to BMM again yielded a higher NMB compared to BMM alone at the higher (EVT: $114,661 (ATTENTION)/$117,245 (BAOCHE) vs BMM only: −$55,354 (ATTENTION/−$80,250 and lower (EVT: −$86,249 (ATTENTION)/−$105,208 (BAOCHE vs BMM only: −$155,225 (ATTENTION/−$207,801 (BAOCHE)) (BAOCHE)) WTP thresholds. The ICER equaled $15,867 (ATTENTION) and $−4,052 (BAOCHE) (Table 2).
Base case results.
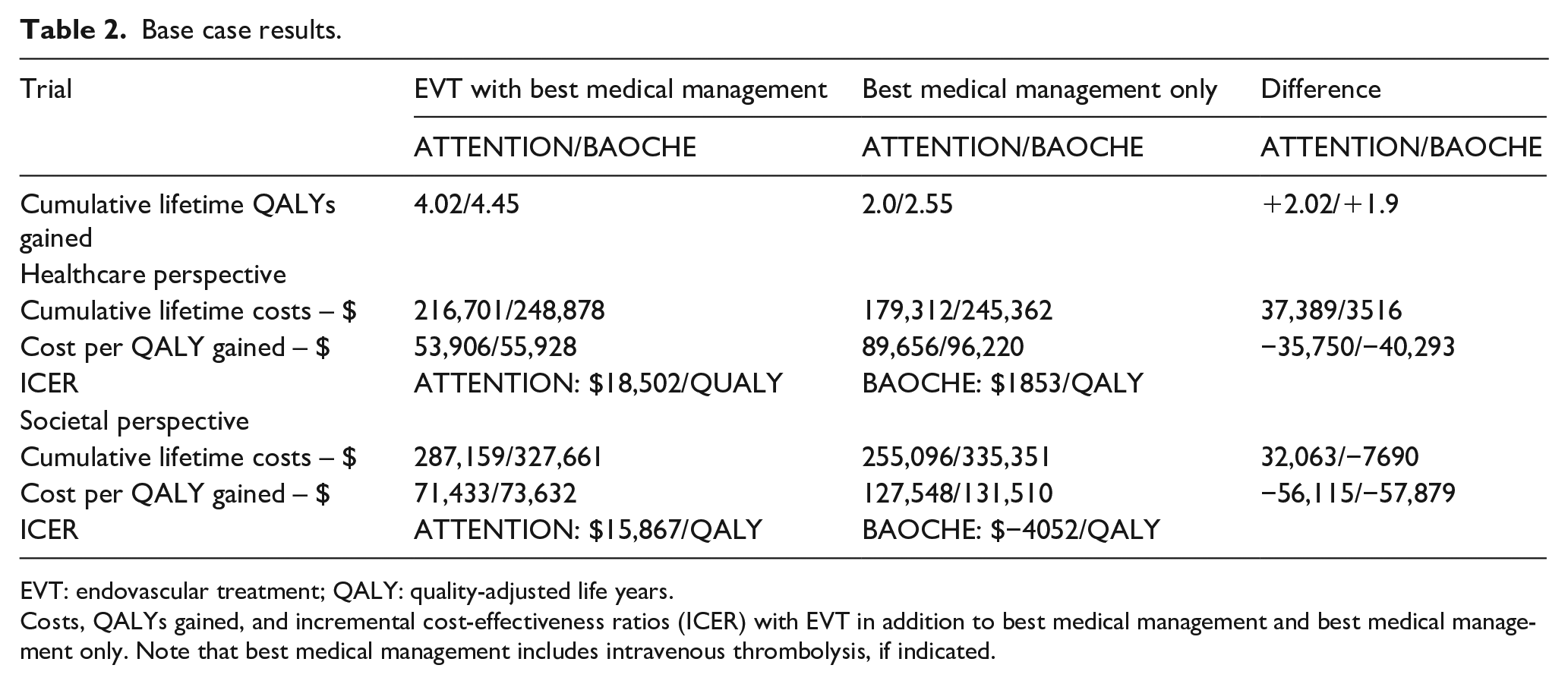
EVT: endovascular treatment; QALY: quality-adjusted life years.
Costs, QALYs gained, and incremental cost-effectiveness ratios (ICER) with EVT in addition to best medical management and best medical management only. Note that best medical management includes intravenous thrombolysis, if indicated.
Sensitivity analysis
In both studies EVT in combination with BMM proved to be the cost-effective option in nearly all Monte Carlo Simulation runs from a healthcare as well as societal perspective (see Figure 2). This was the case for WTP threshold of $50,000/QALY (>98% of simulations) and $100,000/QALY (>99% of simulations) attributing to the robustness of our base case results.
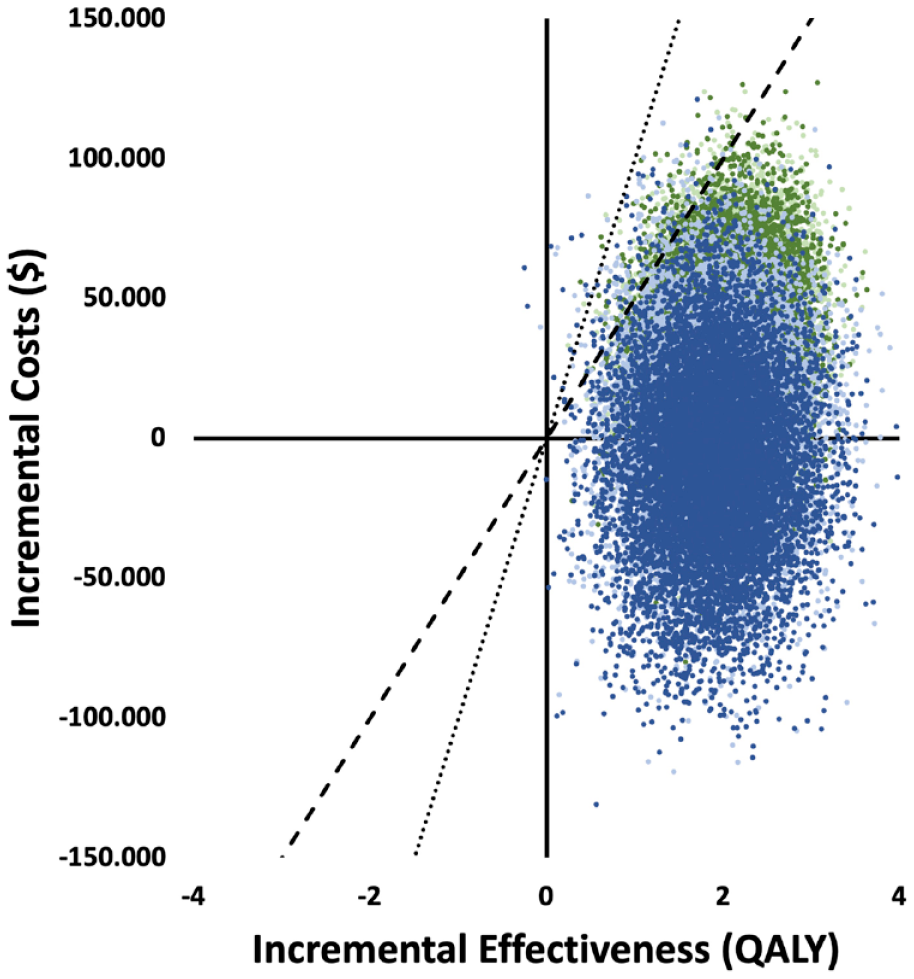
Probabilistic sensitivity analysis.
Cost for EVT as well as age at stroke were the single parameters with the strongest impact on the ICER on both trials from a healthcare as well as societal perspective (see Figure 3). It should be noted that the range of these parameters was considerably wider than that of the remaining parameters. However, within the given input ranges none of the deterministic sensitivity analyses surpassed the WTP threshold of $50,000/QALY.
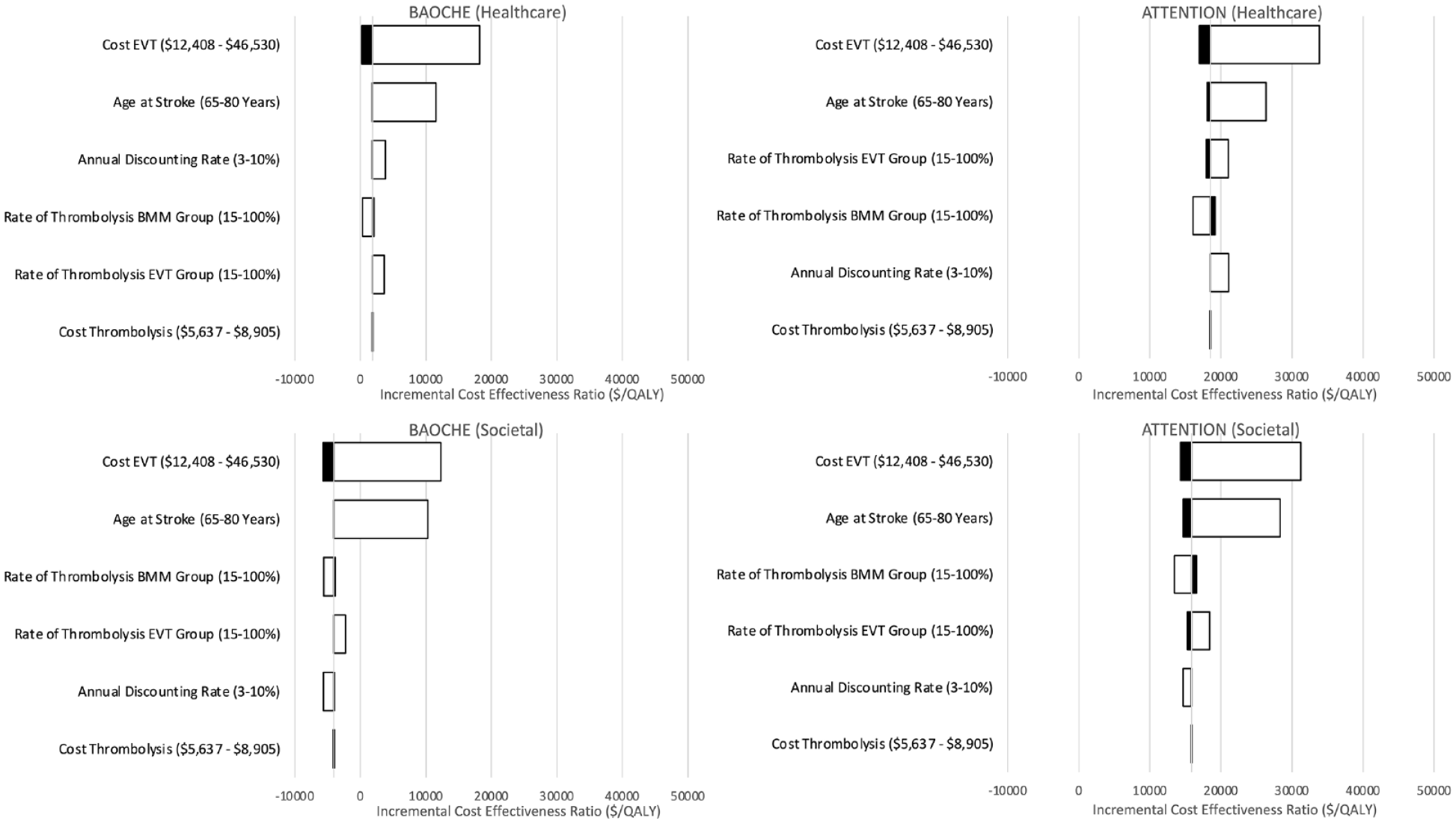
Deterministic sensitivity analysis.
Discussion
In this cost-effectiveness analysis, EVT in addition to BMM for BAO stroke resulted in a gain in QALYs at only minor additional costs and – in certain cases – decrease in lifetime costs compared to BMM alone.
Our results are in line with previous cost-effectiveness studies on EVT in acute stroke. 27 The differences in health-economic benefit of EVT between the two studies we observed, was mostly due to differences in 90-day mortality and morbidity. Lower percentages of patients with a mRS 3 and 4 treated in the BAOCHE trial compared to the ATTENTION trial led to less long-term treatment costs and income losses with a slightly lower ICER for EVT in this trial.
However, BAO stroke depicts a special disease entity. Compared to anterior circulation stroke, BAO is less common 28 with unfavorable clinical outcomes following treatment with IVT, 2 leaving patients with severe disabilities. Previous randomized controlled trials did not show benefit of EVT in addition to BMM,4,5 possibly due to recruitment issues and high cross-over rates. 29 Following the neutral outcome of these early trials, it has been debated whether it is feasible and ethical at all to obtain randomized evidence for the benefit of EVT in BAO stroke. The recent results of the ATTENTION and BAOCHE trial have finally settled this question since they demonstrated clear benefit for EVT over and beyond BMM in BAO stroke. However, several factors in both trials have to be accounted for, affecting, and also limiting our cost-effectiveness analysis. First, both trials were conducted in China, where incidence as well as mortality of stroke are the highest worldwide. 30 Furthermore, etiology of ischemic posterior circulation stroke differs between Caucasian and Asian individuals with higher prevalence of intracranial atherosclerosis in Asian patients as a potential explanation for higher rates of BAO in this population. 28
Furthermore, most patients included in both studies presented with an NIHSS-score of 10 or higher, leaving uncertainty about efficiency of EVT in patients with lower NIHSS-scores. Additionally, results from a meta-analysis including data from the BASICS and BAOCHE trial for patients with NIHSS-scores <10 found no certain benefits for EVT compared to BMM in this specific patient group. 31 As a result, we could not evaluate cost-effectiveness in patients presenting with baseline NIHSS-scores <10. However, a recent study investigating EVT and IVT in patients with anterior circulation large vessel occlusion stroke with NIHSS-scores <5 found poor functional outcomes compared to IVT alone, 32 assuming an advantage for EVT in patients with BAO stroke and a lower NIHSS-score. Moreover, the percentage of patients receiving IVT was low in both trials, since most patients presented outside of the treatment window of 4.5 h after onset of symptoms. Still, in studies concerning anterior circulation late vessel occlusion stroke like the SELECT Late Study clinical outcome was favorable for EVT compared to BMM, 33 assuming similar results for patients with BAO stroke. The fact that most patients had to pay for IVT in advance could have also led to selection bias. But since this applied to both the EVT and BMM arms, the low IVT rate most likely did not substantially influence the results of our cost-effectiveness study. In addition, the low IVT rate seems to have had no major influence on outcomes, since in both trials, patient outcome for the control group was comparable to a prior study on Han Chinese individuals with higher rates of IVT in the BMM group. 6 Furthermore, the deterministic sensitivity analysis showed no relevant influence of the rate of thrombolysis in the EVT and BMM group for both trials. All in all, it should be noted that IVT should be administered previously to EVT as noted in the ESO guidelines. 34 Both, the specific etiology of BAO in Asian individuals as well as the lower rate of IVT in the control group can affect translation of the trial results, and therefore also the results of the current cost-effectiveness study, to individuals with different ethnic backgrounds.
Cost-effectiveness analyses of the ATTENTION and BAOCHE trial yielded similar but slightly varying results. This is mostly due to differences in 90-day mortality and morbidity between both studies, affecting treatment costs and income losses, mostly of patients with severe morbidity.
Finally, our study has some limitation. First, treatment costs as well as societal costs were derived from a U.S. perspective, resulting in uncertainty of cost-effectiveness of EVT and BMM in other healthcare systems. Therefore, further studies will be required to analyze cost-effectiveness of EVT and BMM in BAO stroke in different national settings. Second, costs for EVT in BAO stroke were assumed to be equal to EVT in anterior circulatory stroke, which may not reflect clinical reality. However, we decided to use this approach as of today only limited data on treatment approaches in BAO stroke are available. Third, long-term outcome of patients with BAO stroke treated with EVT are not available at the moment, and we therefore used long-term outcomes that were derived from prospective cohort studies of anterior circulation stroke patients. These clinical factors impact our analysis leading to uncertainty of some input parameters. Probabilistic sensitivity analyses, however, showed that the results are robust to input parameter variation.
In conclusion, our analysis demonstrated that EVT is cost-effective in BAO stroke compared to BMM alone, both from a healthcare and a societal perspective. Future investments to cover this increasing demand for EVT in BAO stroke are therefore justified from a health economics standpoint.
Supplemental Material
sj-pdf-1-eso-10.1177_23969873231209616 – Supplemental material for Cost-effectiveness of endovascular treatment versus best medical management in basilar artery occlusion stroke: A U.S. healthcare perspective
Supplemental material, sj-pdf-1-eso-10.1177_23969873231209616 for Cost-effectiveness of endovascular treatment versus best medical management in basilar artery occlusion stroke: A U.S. healthcare perspective by Dirk Mehrens, Matthias P Fabritius, Paul Reidler, Thomas Liebig, Saif Afat, Johanna M Ospel, Matthias F Fröhlich, Julian Schwarting, Jens Ricke, Konstantinos Dimitriadis, Mayank Goyal and Wolfgang G Kunz in European Stroke Journal
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Informed consent
Not applicable.
Guarantor
DM.
Contributorship
DM, WGK, TL, and JR conceived and designed the analysis. MPF, PR, and KD collected the data. WGK, SA, JMO, MFF, JS, MG contributed data or analysis tools. MPF, PR KD, SA, MFF, JS, JMO, DM, and WGK performed the analysis. DM and WGF wrote the paper.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.