
Abstract
Background and aims
Young Autistic children in the prelinguistic/emerging linguistic stage often exhibit difficulties in motor, social, and communicative skills. Analysis of gesture—a skill with motor, social, and communication components that emerges prior to spoken language—may provide insight into the interplay of these skills before the onset of speech, potentially leading to improved early intervention approaches.
Methods
This secondary analysis included data from 80 Autistic children aged 18 to 59 months who participated in one of the two larger studies. Video recordings of parent–child interactions and a standardized communication assessment were collected at baseline. Child gesture rate (gestures produced per 10 min) was extracted from these videos and analyzed for relationships with standardized measures of child motor and social skill. Further, child point gestures were coded for motor complexity (using a novel coding system) and social sophistication (number of coordinated communicative behaviors and level of communicative intention).
Results
Standardized measures of child social and gross (but not fine) motor skills each uniquely contributed to child gesture rate, with social skills exerting a stronger influence. Motor complexity of points was significantly positively related to both measures of social sophistication.
Conclusions
The results of the present study indicate related but unique roles for social and motor skill in the gesture production of young Autistic children.
Implications
These findings indicate the need for further research to explore the effectiveness of targeting motor skills into early intervention in support of later social communication.
Introduction
Autism spectrum disorder (autism) is a complex neurodevelopmental condition characterized by disruptions in social communication and restricted/repetitive behaviors and interests (American Psychiatric Association, 2022). Although not a core feature of autism, motor deficits are common, affecting as many as 50% to 100% of children with the condition (Bhat et al., 2012; Ghaziuddin & Butler, 1998). Evidence indicates motor deficits are present across the lifespan, with delays in motor skills present in the first year of life (Bhat et al., 2012; Karmel et al., 2010; Libertus et al., 2014; Ozonoff et al., 2008; Travers et al., 2013). Gesture—symbolic movement that serves a communicative function—is a communication skill at the intersection of motor and social domains that typically emerges prior to spoken language. As such, gesture allows infants and toddlers to engage in social interactions as intentional communicators without the need for speech. Thus, analysis of the gesture use of young Autistic children in the prelinguistic/emerging linguistic stage may provide insight into the interplay among motor, social, and communication skills–areas in which Autistic children have been found to experience difficulty–prior to the onset of speech. 1
Motor Deficits may Underlie Social Communication Deficits in Autism
While the social difficulties associated with autism have long received the attention of researchers, motor deficits have recently moved into focus. Some researchers have suggested early motor delays are responsible for the social differences observed in autism (Iverson, 2018; Leary & Hill, 1996; Mody & McDougle, 2019). For example, applying Dynamic Systems Theory, Thelen (2005) posited that the social differences common in autism are the product of a complex, dynamic system in which the infant's early actions affect their environment, which in turn affects the infant, and so on. Central to Dynamic Systems Theory is the concept that developmental milestones (in the present case, the onset of gesture skills) are “dynamically constructed” based on continual interactions of individual, environment, and task over time (Fidler et al., 2011; Thelen, 2005).
In a dynamic systems model, early gross motor difficulties might interfere with an infant or toddler's ability to explore their environment and to engage with others, which then influences the input the child receives (Iverson, 2018; Mody & McDougle, 2019). For example, infants later diagnosed with autism tend to be delayed in sitting unsupported, spending more time than their typically developing (TD) peers in a lying posture (Iverson, 2018). In a lying posture, it is more difficult for infants to initiate eye contact with adults (as the adult must move into the infant's field of view), which may influence how adults respond to the infant (Iverson, 2018). As such, infants delayed in sitting may have fewer social and linguistic experiences than infants with typical motor development, resulting in cascading effects on language and social development. A child's motor skills might also influence the quality of their social interactions, for example, by supporting the coordination of walking with gestures such as giving and showing (moving bids; Calabretta et al., 2022; Iverson, 2022), or by affecting their ability to produce speech. Moreover, as shown in De Froy et al. (2021) and other studies, parents of Autistic and non-Autistic children tend to respond differentially to child communication based on the developmental sophistication of the communicative act, which can have downstream effects on development (see also Choi, Nelson, et al., 2020; Choi, Shah, et al., 2020; Gros-Louis et al., 2006; Donnellan et al., 2020; Leezenbaum et al., 2014). Notably, changes to the child (e.g., improvements in motor skill) or environment (e.g., changes in parent responses to child; intervention) may be sufficient to interrupt these developmental cascades (Adamson et al., 2020).
A dynamic systems account provides a framework of how early motor and social skills may be related, and why it is important to explore the role of motor skills in the social communication skills of Autistic children.
Evidence for the Roles of Motor and Social Skills in the Gesture of Autistic Children
Gesture development in Autistic children follows a similar trajectory as in TD children but is characterized by slower growth (Sowden et al., 2008; Talbott et al., 2020). Discrepancies in gesture production between Autistic and TD children emerge as early as 9 to 12 months of age, as TD children quickly begin to gesture more frequently and for more purposes (Colgan et al., 2006; Heymann et al., 2018; Watson et al., 2013). Over the past few decades, researchers have explored whether these differences in gesture development are primarily a reflection of the motor or social domain. Results of some studies indicate Autistic children have intact fine motor abilities to point to regulate another's behavior but exhibit reduced pointing to initiate mutual attention, suggesting a social origin for gesture deficits (Baron-Cohen, 1989; Goodhart & Baron-Cohen, 1993). In contrast, Mundy et al. (1994) found Autistic children with a mental age under 20 months (a developmental level lower than the participants in Baron-Cohen, 1989 and Goodhart & Baron-Cohen, 1993) produced fewer points for both behavior regulation and mutual attention compared with their TD peers. Taken together, these data suggest the relative roles of motor and social skill on gesture production may change with development. However, little is known about the unique contributions of motor and social skills to the early gesture production of young Autistic children.
Assessing Motor and Social Skill of Gesture
To better understand the role of motor and social skills in gesture production, we distinguished between two distinct dimensions of their contribution: (1) how these skills influence the overall frequency of gesture use (i.e., gesture rate) and (2) the motor and social complexity involved in producing individual gestures.
Contributions of Motor and Social Skill to Child Gesture Rate
Standardized assessments may be used to estimate a child's overall motor and social skills. Evidence suggests, however, that gross and fine motor skills have different relationships to language skill (Gonzalez et al., 2019) and may also differentially influence how frequently children gesture. For example, gross motor skills have been found to predict later language in TD children, whereas fine motor skills are more strongly associated with concurrent language abilities (Gonzalez et al., 2019). These findings suggest that motor development may shape gesture rate by influencing a child's ability to initiate communication through movement. Children with weaker motor skills—particularly in gross motor domains—may gesture less often, either due to physical constraints or reduced opportunities for interaction. As discussed above, deficits in gross motor skills could contribute to cascading effects on gesture production.
Contributions of Motor and Social Skill to Individual Gestures
In addition to assessing overall motor and social skills with standardized measures, our approach focuses on identifying the specific motor and social abilities a child recruits during individual communicative acts. Here we consider measures of the motor complexity and social sophistication of gestural communication. In the present study, we focus specifically on the point gesture. Points are unique among early developing gestures in that they can convey a variety of communicative functions, differing in social sophistication and motor complexity, thus allowing for comparison among these measures. Our approach of focusing on the point gesture is consistent with previous research exploring the motor and social components of gesture in Autistic children (Baron-Cohen, 1989; Goodhart & Baron-Cohen, 1993; Mundy et al., 1994).
Below, we describe our approach to analyzing these two aspects of gesture complexity: motor complexity and social sophistication.
Social Routines are supported by the adult, with caregivers providing opportunities for the child to contribute a response within a predicable routine or activity, such as playing peek-a-boo, reading books, or naming objects (Bruner, 1983; Ninio & Bruner, 1978; Ninio & Snow, 1996; Snow et al., 1987). Within these predictable interactions, the adult is attending to the child and is awaiting their response as prescribed by the routine. Furthermore, since routines provide a known framework and the adult awaits the child's response within it, the child does not need to capture or direct the adult's attention for the communicative act to be successful. In contrast, for communicative acts within Behavior Regulation or Mutual Attention to be successful, the child often needs to gain or direct the adult's attention (e.g., to an object of interest) because the focus of the interaction is not already shared with the adult. Social Routines can therefore be conceptualized as having a lower level of social demand than Behavior Regulation and Mutual Attention.
In addition to the three socially motivated categories described above, vocalizations, words, or gestures may also be directed toward objects rather than a person (e.g., labeling an object without regard for the attention of the adult; Object Direction). These acts may not be intended to share information with another person and are therefore considered to involve the lowest level of social demand. Nonetheless, parents may interpret such acts as having shared information, which could in turn support the development of social communication (Rollins et al., 2022).
Current Study
In this secondary analysis of data collected from two larger studies, we aimed to address a gap in the literature regarding the interplay of motor and social skills in the gesture production of young Autistic children. Specifically, we examined this interplay in two ways (Figure 1). First, we explored the roles of motor and social skill (as measured by standardized assessments) on the rate of child gestures. Second, we examined how the social sophistication of communication (i.e., the social demand of each communicative act and the coordination of temporally overlapping communicative behaviors) relates to the motor complexity with which gestures were produced. Further, we chose to study Autistic children at the prelinguistic or emerging linguistic stage of development because this is a key developmental window for the emergence of intentional communication, including gesture. Understanding how motor and social skills contribute to gesture production at this stage may provide insight into early developmental pathways and inform intervention. The following research questions (RQs) guided this study: RQ 1 (Contributions of Motor & Social Skill to Child Gesture Rate): For young Autistic children in the prelinguistic/emerging linguistic stage of development, are there unique contributions of motor and social skills on concurrent gesture rate? RQ 2 (Contributions of Motor & Social Skill to Individual Gestures): For young Autistic children in the prelinguistic/emerging linguistic stage of development, what is the relationship between motor complexity and measures of social sophistication (level of social demand of the communicative intention and coordination of communicative behaviors) during the production of individual gestures?

Research Questions and Measures.
RQ 1 will provide insight into the relative roles of motor and social skill in the gesture production of young Autistic children. If motor skill is a significant predictor of gestural skills, this would provide support for theories that purport motor skills play a role in the social communication deficits often observed in autism. We hypothesize both motor and social skills will contribute unique variance to child gesture rate.
RQ 2 is an exploratory question that will provide information about the relationships between motor and social skill during gestural communication. We will assess the relationship between motor complexity of point gestures and two measures of social sophistication: level of social demand and coordination of communicative behaviors.
Methods
Participants
Participants for the present study were 80 racially/ethnically and socioeconomically diverse young Autistic children and a parent who took part in one of two more extensive randomized control trials (RCTs) assessing Pathways Early Autism Intervention in Dallas, TX (see De Froy et al., 2021; Rollins & De Froy, 2022). For both RCTs, families were recruited through local infant-toddler programs, community centers, advocacy groups, physicians’ offices, social media, and word of mouth. The inclusion criteria for the original RCTs were identical except for the age range of the children at baseline (i.e., < 40 months for children in Rollins et al., 2021 and <60 months for children in Rollins & De Froy, 2022). Other inclusion criteria for the original RCTs were (1) receiving an “autism spectrum” classification on the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2, Lord et al., 2012) administered by research reliable study personnel and confirmed with clinical judgment; (2) having no other known medical, neurological, or genetic concerns as reported by the caregiver; and (3) having a primary home language of English or Spanish. For the present study, three additional inclusion criteria were imposed (Figure 2): (1) a video-recorded administration of the Communication and Symbolic Behavior Scales Developmental Profile (CSBS DP; Wetherby & Prizant, 2002); (2) a standard score of < 85 on the Mullen Scales of Early Learning, Early Learning Composite (MSEL; Mullen, 1995); and (3) a Total Calibrated Severity Score ≥ 5 on the ADOS-2. These final two inclusion criteria were imposed to ensure a more homogenous sample by excluding children whose developmental profiles differed from the majority; in particular, these children were beyond the prelinguistic/emerging linguistic stage relevant to the present paper.

Study flow: Participants from Studies 1 and 2 Included in the Present Study.
Participant characteristics are summarized in Table 1. Sample demographics were broadly representative of that of Dallas County, except that our sample contained a larger percentage of Asian and a lower percentage of Black/African American participants (United States Census Bureau, n.d.). Child age ranged from 18 to 59 months. All children were in the prelinguistic/emerging linguistic stage of development, and many also exhibited cognitive delays.
Child, Participating Parent, and Family Baseline Characteristics (n = 80).
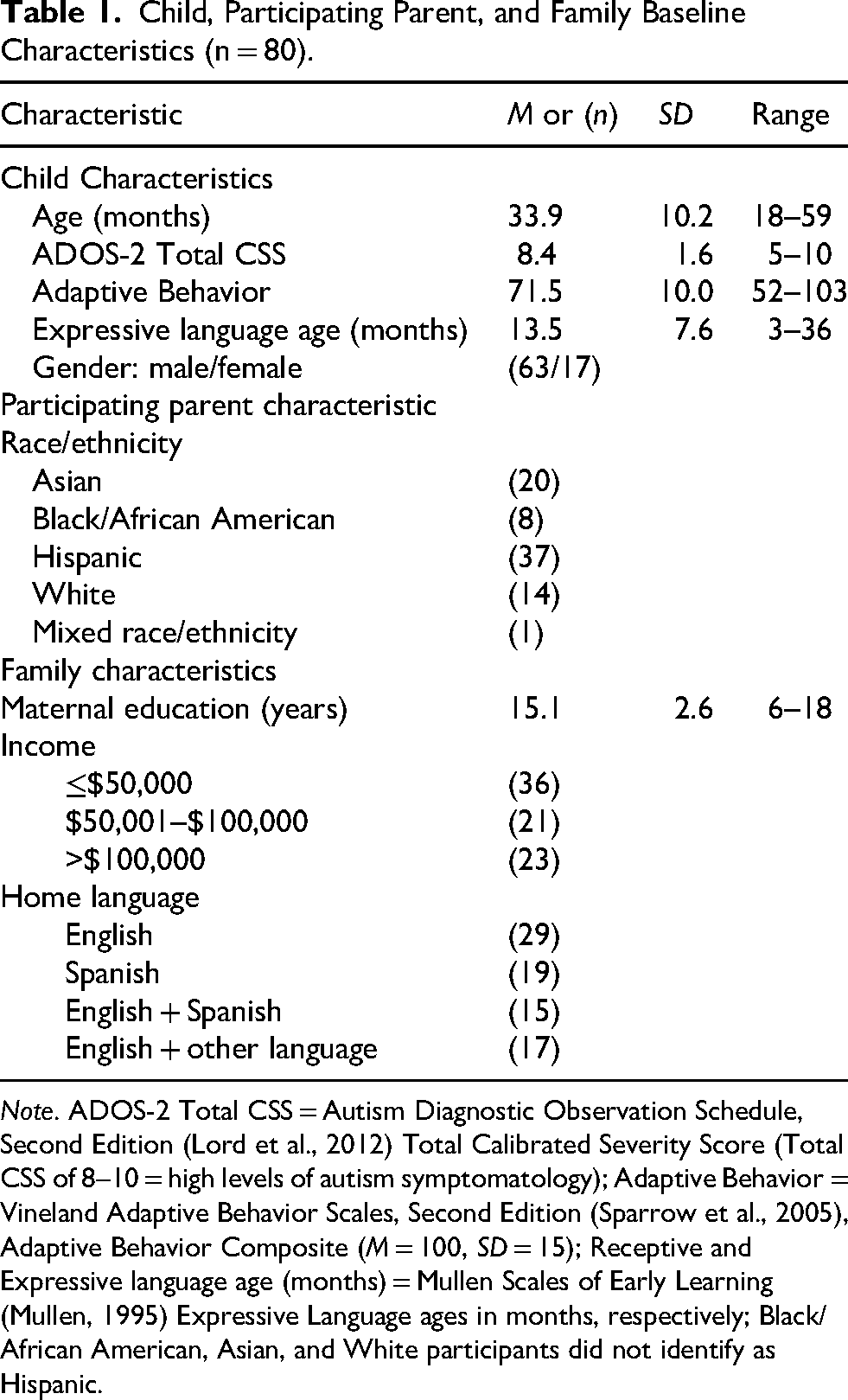
Note. ADOS-2 Total CSS = Autism Diagnostic Observation Schedule, Second Edition (Lord et al., 2012) Total Calibrated Severity Score (Total CSS of 8–10 = high levels of autism symptomatology); Adaptive Behavior = Vineland Adaptive Behavior Scales, Second Edition (Sparrow et al., 2005), Adaptive Behavior Composite (M = 100, SD = 15); Receptive and Expressive language age (months) = Mullen Scales of Early Learning (Mullen, 1995) Expressive Language ages in months, respectively; Black/African American, Asian, and White participants did not identify as Hispanic.
As RQ 2 only analyzes data from children who pointed, characteristics of the 39 children who pointed at least once (Pointers) during the interactions are compared to the 41 children who did not (Nonpointers) in Table 2. The data indicate that a larger proportion of Pointers than Nonpointers exhibited expressive language skills above the 9-month level, the age at which TD children begin to exhibit intentional communication (Ninio & Snow, 1996). On average, Pointers also exhibited stronger social and affective skills than Nonpointers, as evidenced by the groups’ CSBS Emotion and Eye gaze scores. Because pointing is often used for intentional social communication, it is expected that children capable of pointing would be more linguistically and socially advanced than their peers who may not yet be pointing (Carpenter et al., 1998; Crais et al., 2004). See De Froy and Rollins (2024) for further discussion of gesture types used by this sample.
Characteristics of Pointers Versus Nonpointers.

Note. ADOS-2 Total and Social CSS = Autism Diagnostic Observation Schedule, Second Edition Total & Social Calibrated Severity Scores, respectively (Total CSS 8–10 = high levels of autism symptomatology); Adaptive Behavior = Vineland Adaptive Behavior Scales, Second Edition, Adaptive Behavior Composite (M = 100, SD = 15); MSEL = Mullen Scales of Early Learning (MSEL Early Learning Composite M = 100, SD = 15); Receptive and Expressive language age (months) = Mullen Scales of Early Learning Receptive and Expressive Language ages in months, respectively; CSBS EE = Communication and Symbolic Behavior Scales Developmental Profile, Emotion and Eye Gaze subscale raw score; d = Cohen's d.
Study Design and Procedures
As discussed above, the present study is a secondary analysis of baseline data from Autistic children who participated in one of two larger RCTs. RCT 1 (Rollins et al., 2021) took place from 2016 to 2018 and RCT 2 (Rollins & De Froy, 2022) from 2018 to 2020 (before the COVID-19 pandemic). All participants received a battery of assessments at baseline prior to randomization into intervention groups, therefore all assessors were blind to group assignment. The assessment batteries included a study-specific demographic interview, standardized parent report interviews, standardized and direct assessments, and a parent–child interaction. Assessments were conducted in English and/or Spanish, depending on the family's primary language. Only data from these baseline assessments were used in the present study.
Research Clinician Qualifications and Training
As described in Rollins et al. (2021), six research clinicians were responsible for administering the assessments. Four were certified speech-language pathologists (SLPs), one a board-certified behavior analyst, and one held a bachelor's degree focused on infant/child development with over 30 years of experience working with parents and children birth to 5 years. Two of the SLPs and the bachelor-level clinician were bilingual (English/Spanish).
Prior to the beginning of the larger research studies, the research clinicians achieved reliability on the ADOS-2 (Lord et al. 2012) with one of the authors, who is an ADOS-2-reliable examiner. Specifically, each research clinician independently coded and scored video-recorded and live administrations of the ADOS-2, then checked point-by-point reliability until 90% interexaminer agreement was achieved with the ADOS-2-reliable examiner. This was repeated until 90% reliability was achieved on three consecutive ADOS-2 administrations, which could be video recorded or live. Taking into account the age and ability level of the children in the study, each research clinician demonstrated standardized administrations on three occasions for the Toddler Module and Module 1 only (i.e., they demonstrated that they could reliably and consistently administer these two modules of the ADOS-2 in the same way researchers are expected). During the two intervention studies, two clinical researchers were present for each assessment. One administered the ADOS-2 while the second assisted. The two researchers scored the assessments together and discussed any issues that might have come to light. Finally, each researcher clinician independently coded three separate ADOS-2s, every 3 months, to check that there was 80% reliability among the group, which was the case in each instance.
A similar procedure was followed to obtain reliability on other standardized assessments. Specifically, the clinical researchers reviewed administration and scoring procedures and subsequently practiced administering and scoring the test with nonproject children and adults until there was 90% reliability with one of the authors. Two clinical researchers were present for child assessments (one administered while the second assisted). All tests were independently scored by two people to check accuracy.
Video Data Collection and Coding Procedures
Child gestures were extracted from two interactions: a naturalistic parent–child interaction (NPCI) in the families’ homes and a structured interaction (CSBS DP) with an unfamiliar communication partner (research clinician) in a clinical setting. Parents were present during the CSBS DP but were not the primary interactional partner.
For the NPCI, parent–child dyads were recorded for 10 min using two perspectives: a wide-angle view captured by an iPad 2, and a close-up view from hidden camera glasses worn by the parent to capture the child's eye gaze (Figure 3). Baseline data collection procedures were the same across the two RCTs, with the exception of the toys available during the NPCI. Participants in RCT 1 (n = 15; 2016–2018) used their own toys. Because all participants were under 3 years of age, we asked parents to select toys they believed their child would be most likely to engage with, to maximize child engagement and support a naturalistic context for interaction. Participants in RCT 2 (n = 65; 2018–2020) were provided with a standard set of developmentally appropriate toys (a drum, farm animal and tractor set, musical piggy bank, blocks, baby doll with accessories, shape sorter, ball, puzzles, snap lock toy, and picture books). Parents were asked to only have one toy out at a time. Notably, these differences in toy selection across the studies were evaluated in a published analysis using this sample. That study addressed potential task-specific differences in gesture production and found that children produced similarly low gesture rates during the NPCI (only 56% of children gestured during the NPCI compared with 96% during the CSBS DP; NPCI gesture rate [i.e., gestures produced per 10 min] Mdn = 1.00, IQR = 2.00), regardless of whether they were using their own toys or the standardized toy set (De Froy & Rollins, 2024). Further, results of a Kendall's tau correlation indicated the two groups did not gesture at significantly different rates (n = 80, p = .598). Based on these findings, we combined data from both RCTs for our analyses.

Hidden Camera Glasses Worn by Parent or Clinician During Assessments.
For both RCTs, before the video-recorded observation began, a research clinician described the purpose of the observation and the recording procedures. The research clinician instructed parents to interact with their child the way they normally would, and toy play was not required. The research clinician ensured both parent and child remained in view throughout the 10min session but did not intervene or comment on the interaction.
For the structured interaction with an unfamiliar communication partner, video recordings were obtained during administration of the CSBS DP. The CSBS DP is an assessment of a child's communication and symbolic skills consisting of five structured activities. Video recordings followed the same dual-perspective procedure used in the NPCI: one research clinician administered the assessment while wearing hidden camera glasses to capture the child's eye gaze, and a second research clinician recorded the wide-angle view using an iPad 2.
The recorded NPCI and CSBS DP assessments were sent to the lab, where the two streams of digitized videos (i.e., iPad 2 and glasses) were time linked, transcribed, and coded in the Computerized Language Analysis (CLAN) software package of CHILDES (MacWhinney, 2000). Using CLAN we created video-linked ASCII files, in which each time-aligned segment of the video is referred to as a bullet in CHILDES. Bullets defined the portion of video associated with a given transcript segment and allowed us to control the duration of each segment and manipulate the speed of video playback. This feature enabled us to have precise alignment between the video and transcription, supporting detailed coding of multimodal behaviors (e.g., verbal, vocal, and gestural acts) within each time-locked unit.
Transcription was conducted at the level of the utterance and included all verbal, vocal, and gestural behaviors bounded by a pause or change in conversational turn (Pan et al., 2005). For Spanish-speaking dyads, bilingual (English/Spanish) research assistants transcribed in Spanish and provided English translations on a secondary coding line. Transcription and coding were conducted by trained research assistants who were blind to group assignment. Specifically, research assistants trained on practice videos until they achieved substantial inter-rater agreement measured by obtaining a Cohen's kappa coefficient of .75 or above. Cohen's kappa accounts for agreement that occurs by chance (Yoder et al., 2018). Once reliable, research assistants were allowed to code study videos. To protect against coder drift, coders attended weekly lab meetings to discuss coding, and their reliability was checked by a master transcriber/coder every 3 months.
Measures
Autism Classification and Symptom Severity
The ADOS-2 was administered by a research-reliable clinician to confirm a research diagnosis of autism and to estimate overall symptom severity. The ADOS-2 is a semistructured evaluation of communication, social interaction, play, and restricted/repetitive behaviors for children suspected of having autism. The ADOS-2 has been used successfully with Spanish-speaking Autistic children (Ohashi et al., 2012; Stronach & Wetherby, 2017). The ADOS-2 is available in five versions (modules) selected based on the child's age and expressive language level. The Toddler Module, intended for children 12 to 30 months of age, was administered to 37 children. Module 1, intended for children aged 31 months and older whose language abilities range from no speech to simple phrases, was administered to 43 children. ADOS-2 scores were converted to Calibrated Severity Scores (CSS) to allow comparisons of symptom severity across modules. Total CSS was used as an estimate of overall autism symptom severity.
Adaptive Functioning
The English or Spanish version of the caregiver interview form of the Vineland Adaptive Behavior Scales, Second Edition (Vineland-II; Sparrow et al., 2005) was administered to measure child adaptive functioning skills. The Vineland-II is a standardized test of adaptive functioning for individuals from birth to age 90 years. This parent report measure yields an adaptive behavior composite (ABC) score and domain scores for communication, daily living, socialization, and motor development. The raw ABC score, which has good test–retest reliability (.94; Sparrow et al., 2005), was used in the present study as a proxy for developmental and adaptive functioning in everyday contexts. This measure was selected because a validated Spanish version of the VABS is available. Importantly, the Spanish version is a direct translation of the English version and uses the same normative data, allowing for meaningful comparisons across language groups. Further, the Vineland-II has been identified as suitable (having adequate reliability, validity, and responsiveness to change) as an appropriate endpoint for defining clinically meaningful estimates in autism research (Chatham et al., 2018; McCracken et al., 2021).
Motor Skills and Developmental Level
The MSEL was used to estimate child motor skills and developmental level. The MSEL is a standardized direct assessment of development for young children ages 0 to 68 months that yields scores for gross and fine motor skills, visual reception, and receptive and expressive language. For children whose primary language was Spanish, instructions were delivered in Spanish by bilingual (English/Spanish) research clinicians. Although the MSEL is not available in Spanish, expressive language raw scores from Spanish-speaking children were included in Table 1. This decision was supported by a strong correlation between MSEL expressive language scores and scores on the Spanish version of the Vineland-II expressive communication subscale (r = .80, p < .001), lending validity to the use of MSEL expressive scores for this group. Raw scores of the fine motor and gross motor scales of the MSEL (Mullen, 1995) were used to estimate child fine and gross motor skill, respectively. We used raw scores rather than standard scores for the present study as our purpose was not to compare the children in our sample against a broader population.
Social Skills
The CSBS DP Emotion and Eye Gaze subscale raw score was used to estimate child social skill. This subscale assesses the frequency a child uses gaze shifts and shares positive affect toward the examiner. Notably, the CSBS DP is a standardized direct assessment designed to evaluate early communication and symbolic skills in children 6 months to 6 years whose functional communication age is between 6 months and 2 years. Children in the current study all scored below the 50th percentile for 2-year-old children on the CSBS-DP total score, confirming functional language was within the range appropriate for this assessment. The CSBS DP has good internal consistency (.86–.89) and test–retest reliability (.77–.93; Wetherby & Prizant, 2002) and has been used successfully with Spanish-speaking Autistic children (Stronach & Wetherby, 2017).
Video-Coded Gesture Measures
For the present study, gesture was defined as a symbolic movement of part of the body that serves a communicative function (e.g., Cartmill et al., 2012). Following Wetherby and Prizant (2002), communicative behaviors are those that were directed to the parent or clinician. Further, we used their criteria to determine whether a gesture was directed to an adult; as such, eye contact was not required to make this determination. In addition, child symbolic movements that were not directed to an adult (e.g., pointing to pictures in a book without clear regard for the adult's shared attention) were coded. These object-directed movements were included because they could be interpreted by caregivers as communicative and may play an important role in social communication development (Rollins et al., 2022). In contrast behaviors that acted on an object (e.g., pulling on parent's shirt) were not considered gestures unless the child was showing or giving the object (Dimitrova et al., 2016; Wetherby & Prizant, 2002).
Each of the gesture measures detailed below were extracted from the coded NPCI and CSBS DP transcript files using the utilities of CLAN (MacWhinney, 2000). To assess inter-rater reliability for the presence and type of gesture, a second coder independently coded 20% of the finalized baseline videos from RCT 1 and 20% from RCT 2, chosen at random. When disagreements were noted, the gestures were reviewed and differences in coding discussed.
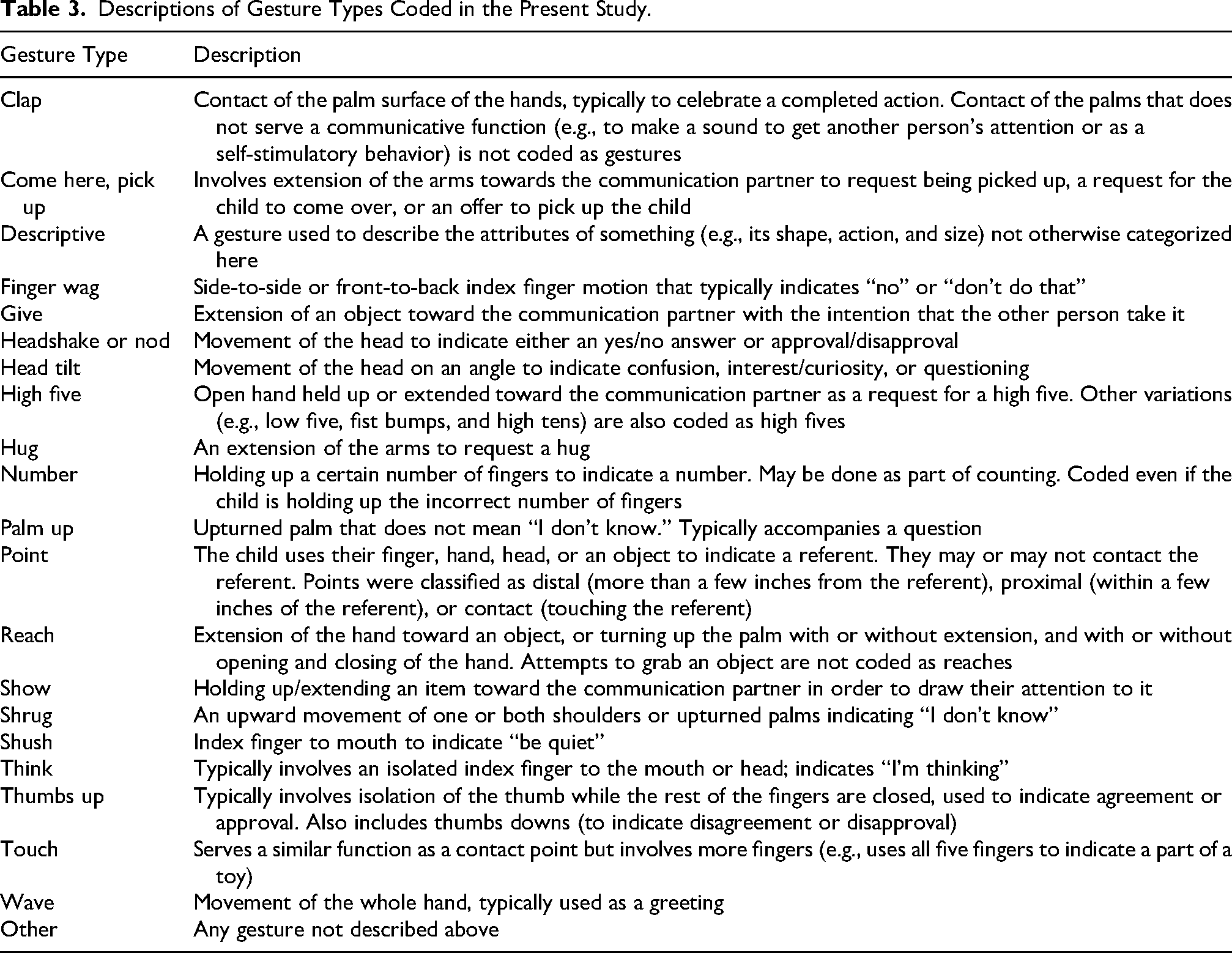
Descriptions of Gesture Types Coded in the Present Study.
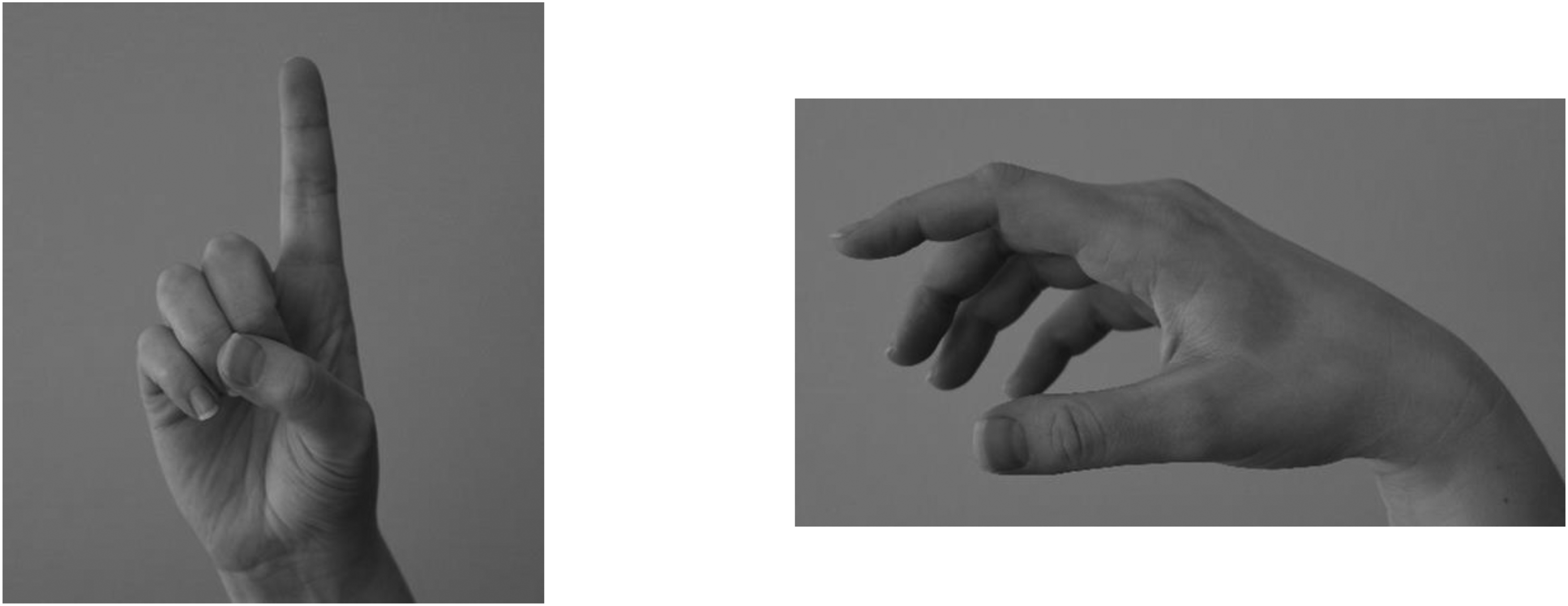
Examples of a Prototypical Point (Left) and a Neutral Position (Right).
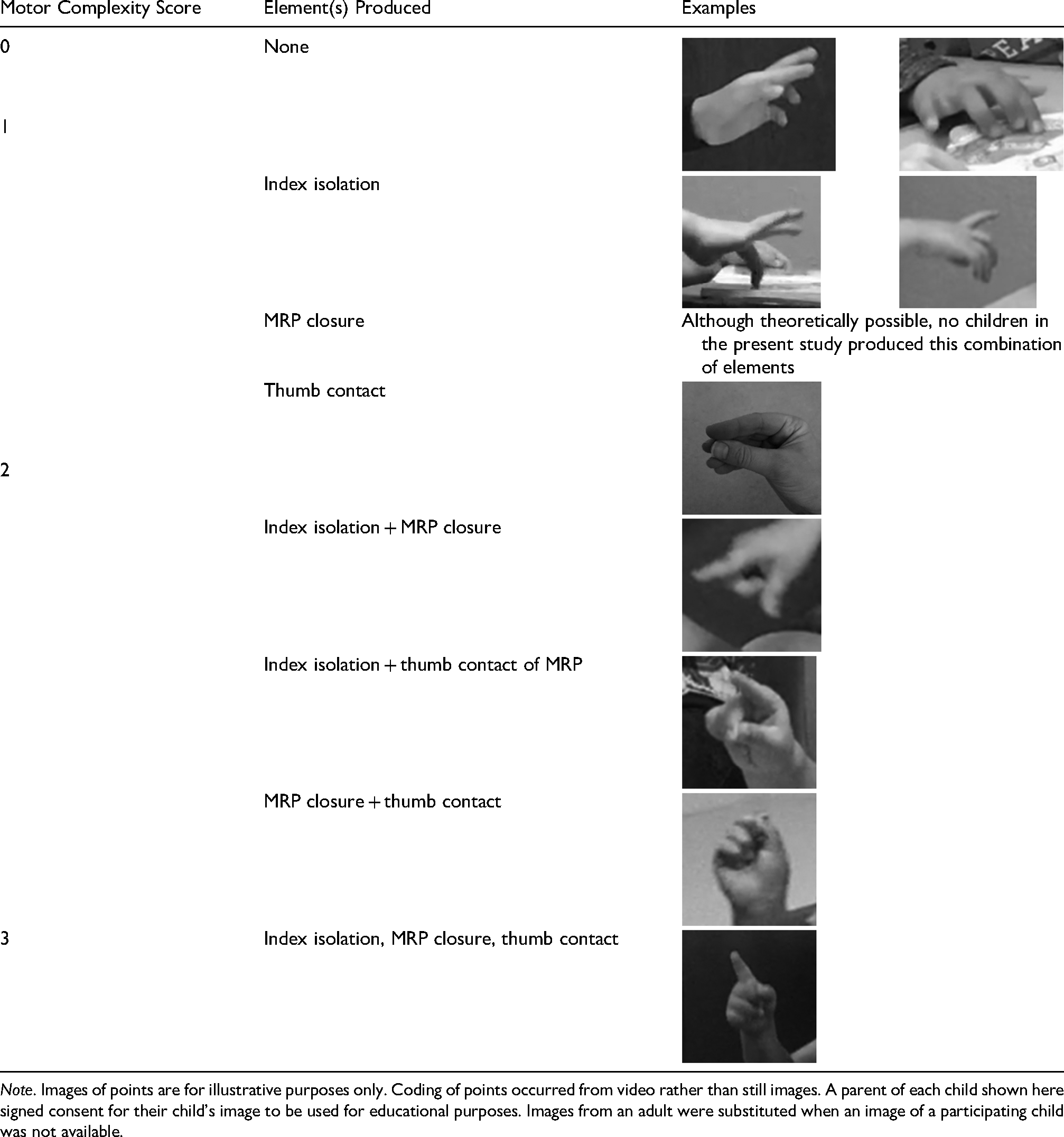
Motor Complexity Coding: Motor Complexity Score, Elements of a Prototypical Point Produced, and Photographic Examples.
Each communicative intention was then assigned a score based on the level of social demand (Table 5). Recall that for the present study we conceptualized the social demand of a context in which a communicative act occurred as whether (1) the behavior was communicative (i.e., if it was directed to another person) and (2) the child first had to get/direct the adult's attention. The lowest Social Demand score was assigned to Object-Directed behaviors, as these lack evidence that the child is attempting to communicate with the adult and the child therefore does not need to first gain/direct the adult's attention. The next highest Social Demand score was assigned to Social Routine. These acts are communicative, but the adult provides a frame and awaits the child's response within that frame as prescribed by the routine. As such, the child does not have to first gain or direct the listener's attention. Finally, the highest Social Demand score was assigned to Behavior Regulation and Mutal Attention as they both (1) demonstrate communicative intent and (2) lack a supportive framework for the child—as such, the child must first get or direct the adult's attention for communicative acts occurring within these communicative intentions.
Social Demand Scores of Communicative Intentions Used in the Current Study.

Analytic Approach
IBM SPSS Statistics version 28 was used to analyze the data. All significance tests were set at .05 based on a two-tailed test.
For RQ 1 (Contributions of Motor and Social Skill to Child Gesture Rate), we began by conducting analyses among background measures and the outcome variable (Child Gesture Rate) to identify potential covariates (Pearson correlations for continuous variables, point biserial correlations for dichotomous variables, and analyses of variance [ANOVAs] for categorical variables). We then used hierarchical linear regression to test the RQ, retaining identified covariates in each model. To satisfy the linearity assumption of correlation and regression, cube root transformations were applied to Child Gesture Rate.
For RQ 2 (motor complexity and social sophistication of point gestures), Kendall's tau (τ) correlations were used to assess the linear relationship between the measures. Kendall's tau was chosen as the data did not satisfy the assumptions of parametric statistics. To aid interpretation, we also present the conversion to r (using r = sin(.5πτ)).
Power Analysis
Sensitivity power analyses were conducted using G*Power version 3.1.9.7 (Faul et al., 2007) to estimate detectable effect sizes given α = .05, power = .80, and achieved sample sizes. For the regression analyses, results indicated small effects could be detected (f2 = .10 covariate and one predictor, f2 = .13 covariate and two predictors f2 = .14 covariate and three predictors).
Results
RQ 1: Contributions of Motor and Social Skill to Child Gesture Rate
Recall that for RQ1, we analyzed the unique contributions of child motor and social skill (as estimated by standardized measures) to Child Gesture Rate. Mean Child Gesture Rate across the NPCI and CSBS DP was 4.4 (Mdn = 3.2, SD = 4.4, range: 0–23). Correlational analyses revealed that both MSEL visual reception and Vineland-II Communication and Adaptive Behavior raw scores were correlated with Child Gesture Rate and with each other (Table 6). Consequently, MSEL visual reception and VABS ABC could not be entered into statistical models together. We chose to retain Vineland-II ABC as a covariate for subsequent analyses of child gesture because it is a proxy for developmental and adaptive functioning in everyday contexts. 2
Correlations Among Background Variables and Child Gesture Rate (n = 80).

Note. Child Gesture Rate = cube root of child gesture rate across the naturalistic parent–child interaction and Communication and Symbolic Behavior Scales Developmental Profile; VABS Comm and ABC = Vineland Adaptive Behavior Scales, Second Edition raw scores of the Communication subscale and Adaptive Behavior Composite, respectively.
*p < .003 (to correct for multiple comparisons, .05/15 comparisons); **p < .0007 (.01/15); ***p < .00007 (.001/15).
Results of hierarchical regression are presented in Table 7. Model 1 is the base model which includes the covariate (adaptive behavior) alone. Models 2a through 2c examined the individual contributions of each predictor variable—social skills, gross motor skills, and fine motor skills—added to the base model. Model 2a indicates that social skills accounted for a significant 15% of the variance in Child Gesture Rate, controlling for adaptive behavior. Similarly, Model 2b shows that gross motor skills accounted for a significant 10% of the variance, also controlling for adaptive behavior. In contrast, Model 2c indicates that fine motor skills did not contribute significantly to the model and were therefore excluded from further analysis.
Hierarchical Linear Regression Models for Social, Gross Motor, and Fine Motor Predicting Child Gesture Rate (n = 80).

Note. Child Gesture Rate = cube root of child gesture rate across the naturalistic parent–child interaction and Communication and Symbolic Behavior Scales Developmental Profile (CSBS DP); Adaptive Behavior = Vineland Adaptive Behavior Scales, Adaptive Behavior Composite raw score; Social = CSBS DP Emotion and Eye Gaze subscale raw score; Gross and Fine Motor = Mullen Scales of Early Learning, gross and fine motor scale raw scores, respectively.
ΔR2 is over model 1 (covariate only).
ΔR2 is over model 2a (covariate + social).
* p < .05; ** p < .01; *** p < .001.
Model 3 is the full model and includes the addition of gross motor to model 2a. Results indicate that while social skills explained 15% of the variation in gesture rate (ΔR2 for model 2a) the addition of gross motor skills only accounted for 5% of the variation in gesture rate (ΔR2 for model 3). This suggests that both domains contribute uniquely to children's use of gestures, with social skills having a more substantial effect overall.
RQ 2: Contributions of Motor and Social Skill to Individual Gestures
For RQ 2, we analyzed the relationship between the motor complexity and social sophistication of point gestures, using two measures of social sophistication (Coordination and Social Demand). From the 39 children who pointed, 258 points were extracted for the present analyses. Noteworthy, an analysis of outliers indicated no child exerted undue influence on the results (Supplemental Materials).

Motor Complexity Scores by Number of Communicative Behaviors as Percents (Top) and Raw Numbers (Bottom).

Number of Points Produced in Isolation, with 2 Coordinated Behaviors, and with 3 Coordinated Behaviors.
Characteristics of Participants Who Pointed Using One, Two, and Three Communicative Behaviors.

Note. ADOS-2 Total CSS = Autism Diagnostic Observation Schedule, Second Edition Social Total Calibrated Severity Score (Total CSS 8–10 = high levels of autism symptomatology); Adaptive Behavior = Vineland Adaptive Behavior Scales, Second Edition, Adaptive Behavior Composite (M = 100, SD = 15); Receptive and Expressive language age (months) = Mullen Scales of Early Learning Receptive and Expressive Language ages in months, respectively; MSEL ELC = Mullen Scales of Early Learning, Early Learning Composite (M = 100, SD = 15); CSBS EE raw = Communication and Symbolic Behavior Scales Developmental Profile, Emotion and Eye Gaze subscale raw score; categories are not mutually exclusive as children may have pointed using more than one level of coordination.
Correlational analyses indicated a statistically significant small relationship between motor complexity and coordination (τ = .117, r = .183, p = .036). Visual inspection of the data indicated that as motor complexity increased, coordination of communicative behaviors tended to increase (Figure 5, top).

Number of Points Produced within Each Communicative Intention.
Characteristics of Participants Who Pointed Within Each Communicative Intention.

Note. ADOS-2 Total CSS = Autism Diagnostic Observation Schedule, Second Edition Social Total Calibrated Severity Score (Total CSS 8–10 = high levels of autism symptomatology); Adaptive Behavior = Vineland Adaptive Behavior Scales, Second Edition, Adaptive Behavior Composite (M = 100, SD = 15); Receptive and Expressive language age (months) = Mullen Scales of Early Learning Receptive and Expressive Language ages in months, respectively; MSEL ELC = Mullen Scales of Early Learning, Early Learning Composite (M = 100, SD = 15); CSBS EE raw = Communication and Symbolic Behavior Scales Developmental Profile, Emotion and Eye Gaze subscale raw score; categories are not mutually exclusive as children may have pointed using more than one communicative intention.
Correlational analyses indicated a significant large relationship between Motor Complexity and the Level of Social Demand (τ = .367, r = .545, p < .001). Specifically, as the Level of Social Demand increased, Motor Complexity also increased (Figure 8).

Motor Complexity Scores by Communicative Intention as Percents (Top) and Raw Numbers (Bottom).
Discussion
While the social difficulties characteristic of autism have long received the attention of researchers, motor deficits have recently gained research attention. Gesture—symbolic movement that serves a communicative function—is a communication skill at the intersection of motor and social domains that typically emerges prior to spoken language. The analysis of gesture production in children in the prelinguistic/emerging linguistic stage of development may therefore provide insight into the very skills with which Autistic children have been found to have difficulties. However, little is known about the interplay of motor and social skills in the gesture production of children in this population. In this study, we analyzed the interplay of motor and social skills in the gesture production of young Autistic children within dyadic interactions in two ways: (1) the roles of motor and social skill (as measured by standardized assessments) on the rate of child gesture and (2) the relationship between social sophistication (estimated by the level of social demand communicative intention and coordination of communicative behaviors) and motor complexity of points.
Contributions of Motor and Social Skill to Child Gesture Rate
In partial support of our hypothesis for RQ 1, standardized measures of child social and gross motor (but not fine motor) skills each uniquely contributed to the gesture rate of young Autistic children (after controlling for adaptive behavior). Of note, social skills appeared to play a stronger role in child gesture rate: the standardized measure of social skills explained more variance (15%) in child gesture rate than did the standardized measure of gross motor skills (10%). Further, when the two measures were in the full model together, the standardized effect (beta) of social skills had a larger effect on gesture rate than did the gross motor measure. The standardized measure of social skills also consistently had a larger effect on child gesture rate than did the measure of adaptive behavior. Taken together, these data underscore the importance of social skills—a core deficit area of autism—for this population. This is consistent with previous research that highlights the role of social skills in the gesture production of Autistic children (e.g., Baron-Cohen, 1989; Goodhart & Baron-Cohen, 1993).
Our finding that gross motor skills also contributed to the gesture production of young Autistic children may be consistent with theories that motor skills play a role in the social communication deficits observed in Autistic children. For example, under a dynamic systems perspective, children who experience early gross motor difficulties may have fewer social communication experiences compared to their peers with intact motor skills. This may in turn have downstream effects on social communication skills, such as early gesture production. While testing Dynamic Systems Theory was beyond the scope of this study, such an account is a possible explanation for the relationship between gross motor and gesture rate in our participants.
The lack of a relationship between the standardized measures of fine motor and child gesture rate may be due, at least in part, to the types of gestures produced by the children in our sample. Results from a previous study conducted with this sample indicated that 76% of gestures produced were points, reaches, and gives (De Froy & Rollins, 2024). These early developing manual gestures may require less fine motor skill than more developmentally advanced gestures. As such, research with more developmentally advanced children who are able to produce more motorically complex gestures might reveal a different pattern.
It is important to recognize that standardized measures reflect a child's performance at a specific time point and are only an estimate of their true skills. The results presented here should be interpreted with this limitation in mind.
Contributions of Motor and Social Skill to Individual Gestures
For RQ 2, we explored the relationship between the motor complexity and social sophistication of points using two measures of social sophistication: coordination of communicative behaviors and the level of social demand of the communicative intention. First, we found the motor complexity with which points were produced was significantly positively related to the number of coordinated communicative behaviors, with a small effect size.
Further, we found motor complexity was significantly related to the level of social demand of the communicative intention with a large effect size. Specifically, motor complexity improved when the child was intentionally communicating (i.e., communicating to regulate behavior, participate in a routine, or for mutual attention, rather than directing a point to objects). Additionally, increased motor complexity was observed when the child needed to gain or direct the adult's attention (behavior regulation and mutual attention) as opposed to communication that occurred while the child was already engaged in an interaction with the adult and the adult could anticipate the child's response (participation in a routine). These results suggest that young Autistic children may increase the motor skill of point gestures, perhaps to clarify their message in order for the communicative act to be successful. Turning again to a dynamic systems perspective to interpret our results, this may suggest the need to clarify one's message is sufficient to move a child from a stable pattern of pointing with lower motor complexity to one of higher motor complexity.
Summary
Our results indicate related but unique roles for social and motor skill in the gesture production of young Autistic children. First, standardized measures of social and gross motor skill were positively related to gesture rate. In addition, our results indicated that as the social sophistication (level of social demand, coordination of communicative behaviors) of a gesture increased, its motor complexity was also likely to increase. It is notable that this relationship between social and motor of given gestures is not solely a reflection of overall child development—children produced gestures at varying degrees of motor complexity and social sophistication (e.g., children capable of producing more motorically complex points also produced less complex points).
This relationship between motor and social in gesture production may suggest both domains should be considered as intervention targets in early intervention for young Autistic children. Several early autism interventions target early social skills, as impairments in this domain are a core feature of the condition (Brian et al., 2017; Kasari et al., 2015; Rollins et al., 2021; Schertz et al., 2018; Wallace & Rogers, 2010; Wetherby et al., 2018). However, there are few empirically supported early autism interventions that target early gross motor skills in support of later social communication (Odeh et al., 2020). Future research should assess the relationship between early motor skills and later social communication to assess the suitability of this approach.
Limitations
A limitation of the present study is that we analyzed data from a single time point. A longitudinal study beginning in infancy would be better suited to assess the contributions of early motor and social skills on later child gesture, thus further testing a dynamic systems account that early skills have cascading effects on later gesture.
A second limitation of this study is that our motor measures were limited to the MSEL fine motor and gross motor subtests. Because this was a secondary analysis of data from an intervention study where motor skills were not the focus, a separate motor test was not administered. Further, while the MSEL is normed on English-speaking Hispanic children, it is not normed on Spanish-speaking children. Future studies should include a measure specifically designed to assess motor skills.
An additional limitation of this secondary analysis relates to the sample. Because these data were analyzed during the COVID-19 pandemic, we were unable to recruit additional participants who might have represented a broader range of developmental abilities. As a result, we were limited in our ability to fully explore the variability in the relationship between motor and social skills. Further research is needed to clarify whether these relationships are consistent across Autistic children with a wider range of developmental profiles.
More broadly, as stated above, the use of standardized assessment measures presents a limitation. Standardized tests capture a child's abilities at a specific time, under structured testing conditions. Consequently, a child's performance on a standardized assessment may not reflect their ability to perform similar skills in real-world conditions. While every effort was made to ensure each child performed to the best of their abilities, we recognize that factors such as discomfort or unfamiliarity with the testing environment can impact test performance. Therefore, all results relying on standardized measures should be interpreted with caution.
Finally, inter-rater reliability was not calculated for translations from Spanish to English in the transcripts of Spanish-speaking children. However, the impact of this on the present study is minimal as the children's utterances were very simple (primarily single words and phrase speech) and the translations served only to provide context for the non-Spanish-speaking coders (i.e., child verbalizations were not analyzed).
Conclusions and Implications
The results of the present study indicate both motor and social skills play an important role in the gesture production of young Autistic children. This may have important implications for intervention, although additional research is needed to explore the effectiveness of targeting motor skills into early intervention in support of later social communication.
Supplemental Material
sj-docx-1-dli-10.1177_23969415251355460 - Supplemental material for Contributions of Motor and Social Skill to the Gesture Production of Young Autistic Children in the Prelinguistic/Emerging Linguistic Stage
Supplemental material, sj-docx-1-dli-10.1177_23969415251355460 for Contributions of Motor and Social Skill to the Gesture Production of Young Autistic Children in the Prelinguistic/Emerging Linguistic Stage by Adrienne De Froy and Pamela Rosenthal Rollins in Autism & Developmental Language Impairments
Footnotes
Acknowledgements
The authors would like to thank the children and families who participated in this study, the research clinicians, and the graduate students who assisted in coding the data.
Ethical Considerations
This project has received IRB approval (IRB 16-81 and 18-149) from the University of Texas at Dallas. All procedures involving human participants were conducted in accordance with the ethical standards of the University of Texas at Dallas.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research grants from the Texas Higher Education Coordinating Board's (THECB) Autism Grant Program (Rollins, PI; grant number 17273 [NCE 20177], 20476 [NCE 22842]).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported by research grants from the Texas Higher Education Coordinating Board's (THECB) Autism Grant Program (Rollins, PI). The THECB did not play a role in study design, data collection/analysis/interpretation, or writing of this manuscript, nor did they place restrictions on the submission of this manuscript for publication.
Data Availability Statements
The participants in this study did not provide informed consent for their data to be shared publicly.
Informed Consent
All parents provided informed consent on behalf of themselves and their children to participate in the study. The opinions and conclusions expressed in this document are those of the authors and do not necessarily represent the opinions or policy of the THECB.
Supplemental Material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.