
Abstract
Background and aims
Young children use deictic gestures, such as pointing, to indicate referents in their immediate environment. Early deictic gesture use is important in facilitating the development of language. In toddlers with or at-risk for autism spectrum disorder, the emergence and use of gestures may be delayed, and deficits in deictic gesture may inform clinical practice regarding early identification, differential diagnosis, and early intervention. The aim of this scoping review was to investigate the extent to which deictic gesture use has been examined in young children with or at-risk for autism spectrum disorder ≤ 36 months of age.
Methods
Four databases (PubMed, PsycINFO, CINAHL, and ERIC) were comprehensively searched for relevant articles. Articles were reviewed in two phases: titles and abstracts followed by full text. Key variables related to participant/study characteristics and group differences on deictic gesture use were extracted. A narrative review was used to synthesize findings across studies.
Main contribution
Nineteen studies met inclusion criteria – 12 studies of toddlers with autism spectrum disorder and 7 studies of high-risk infant siblings of children diagnosed with autism spectrum disorder. Overall, toddlers with autism spectrum disorder were found to demonstrate reduced gesture use across deictic gesture types and ages compared to those with typical development. Findings were more variable when comparing toddlers with autism spectrum disorder to those with other developmental delays and in high-risk infant sibling studies. Although only measured in a limited number of studies, results suggest differences in gesture use in toddlers with autism spectrum disorder based on communicative function.
Conclusions
This review provides insight into the gesture use of toddlers with or at-risk for autism spectrum disorder. Results indicate the particular types of deictic gestures that may be delayed and the age ranges we might expect to observe these deficits in toddlers with autism spectrum disorder compared to those with typical development and other developmental delay groups. Results also reveal variability across studies in the measurement of gestures, and highlight where gaps remain in understanding deictic gesture use in young children with autism spectrum disorder.
Implications
Findings have research and clinical implications related to profiling and targeting gesture use as part of the assessment and treatment process, including identifying patterns of strength and weakness in deictic gesture use of young children with or at-risk for autism spectrum disorder.
Introduction
Gestures are a form of intentional communication that involve movement of the body – typically the fingers, hands, arms, or head. Young children’s gestures are commonly separated into two main categories: deictic and representational (Iverson & Thal, 1998). Deictic gestures indicate a referent in the immediate environment (Bates, Camaioni, & Volterra, 1975). Representational gestures stand for a referent and establish semantic content. They are typically iconic, conveying actions or attributes (e.g. moving arm in air to indicate an airplane is flying), or conventional, with culturally defined meaning (e.g. waving bye, nodding head for “yes”).
Young children with or at-risk for autism spectrum disorder (ASD) exhibit delays in the emergence of gestures. In fact, impairment in gesture use is included in the diagnostic criteria for ASD (American Psychiatric Association, 2013) and plays an important role in early identification of the disorder (Zwaigenbaum et al., 2005). Deictic gestures have been shown to be particularly problematic for young children with ASD (Ozcaliskan, Adamson, & Dimitrova, 2016; Shumway & Wetherby, 2009). However, findings of specific deictic gestures (e.g. pointing versus showing) that may distinguish individuals with ASD from other developmental delays in the toddler years vary across individual studies (e.g. Cox et al., 1999; Wetherby et al., 2004). Examining deictic gesture across studies may provide insight into the degree to which gesture deficits are specific to ASD, particularly during the first years of life.
Typical deictic gesture development
Early in development, gestures provide a means for infants and young toddlers to communicate prior to the development of spoken language. Typically developing infants begin to use deictic gestures before their first birthday (Capone & McGregor, 2004; Crais, Douglas, & Campbell, 2004). Deictic gestures most commonly include pointing, reaching, showing, and giving (Iverson & Thal, 1998). While operational definitions vary across studies, pointing is generally defined as extension and isolation of the index finger, and includes distal (points that do not make contact with an object/person) or contact (points in which contact is made between the child’s finger and the object/person). Some studies have also examined palm points or tapping within the deictic gesture category, which are used to indicate a referent but do not include isolation of the index finger. Reaching involves extending the arm with an open palm or repeated opening/closing of the hand toward an object, person, or location. Reaching has been termed request or ritualized request in some studies (e.g. LeBarton & Iverson, 2016b), although broadly speaking, a reach gesture does not only correspond with requesting. Showing involves holding up or extending an object toward another person, while giving entails the child transferring an object to another person. Of note, the term give has also been used to describe gestures that involve extending the hand with an open palm toward objects to receive them (Ozcaliskan & Goldin-Meadow, 2005), which is similar to reaching (defined above). Unlike representational gestures, which carry fixed semantic meaning (e.g. shaking head indicates “no”), deictic gestures are not referent specific and thus can be used to indicate multiple meanings, actions, or objects.
Although there is significant individual variability in the acquisition of specific deictic gestures and the communicative functions for which they are used, research indicates a sequence of emergence (Capone & McGregor, 2004; Crais et al., 2004). In a study examining the hierarchical development of specific deictic gestures from 6 to 24 months of age in typically developing children, Crais et al. (2004) reported that reaching gestures begin to emerge between 6 and 7 months of age as infants reach to be picked up. Infants expand their reaching gestures between 7 and 11 months to include reaching with the whole hand or repeated opening and closing of the hand. Giving, showing, and pointing typically emerge between 9 and 11 months, although the order of emergence may vary based on the communicative function or intention for which the gesture is used (Crais et al., 2004).
Early communicative functions
Bruner (1981) identified three major communicative functions that typically emerge by the end of the first year of life, including behavior regulation (requesting actions/objects), social interaction (drawing attention to self), and joint attention (directing another’s attention to object/event to share interest). Young children use gestures to communicate for these three functions or intentions (Crais et al., 2004), which are often evaluated on assessment measures of prelinguistic communication in young children (Seibert, Hogan, & Mundy, 1987; Wetherby & Prizant, 2002).
Other terms have been used to express these communicative functions. Proto-imperative and proto-declarative are commonly used to denote the communicative function of deictic gestures, with imperatives serving a requesting (behavior regulation) function and declaratives serving a commenting (joint attention) function (Bates et al., 1975). Initiating Joint Attention (IJA) and Initiating Behavior Regulation (IBR) are also terms commonly used to classify the communicative function of deictic gestures. Specifically, the Early Social and Communication Scales (ESCS), a measure of prelinguistic communication, categorizes deictic gestures using the terms IJA and IBR (Seibert et al., 1987). As defined on the ESCS, IJA (high level) includes pointing or showing to initiate shared attention to objects or events with another person (declarative/commenting). IBR (high level) includes pointing or giving to elicit aid in obtaining an object or event (imperative/requesting). Some research suggests that young children use gestures for requesting/imperative functions before commenting/declarative functions (Bates et al., 1975); however, as described, this may vary based on the specific gesture type (Crais et al., 2004).
Deictic gesture use in toddlers with ASD
Gesture deficits are one of the earliest observable markers of social communication impairments in children later diagnosed with ASD (Mitchell et al., 2006; Veness et al., 2012) and may present in various ways. For example, compared to children with typical development or other developmental delays, children with ASD gesture at a significantly lower rate or frequency (Loveland, Landry, Hughes, Hall, & McEvoy, 1988; Mundy, Sigman, & Kasari, 1990). Children with ASD also show a reduced range in diversity of gesture types (Colgan et al., 2006). Furthermore, differences in the communicative function of gestures have been found in individuals with ASD. Specifically, while children with ASD demonstrate reduced gesturing overall, including reduced use of gestures for behavior regulation, a more pronounced deficit in gesturing for joint attention is observed (Watson, Crais, Baranek, Dykstra, & Wilson, 2013). This pattern of impairment in joint attention or difficulty jointly attending to and drawing another’s attention to external stimuli is diagnostic of ASD (Bruinsma, Koegel, & Koegel, 2004) and has important implications for the development of language. Substantial literature provides evidence of a strong relationship between joint attention and both receptive and expressive language development in children with ASD (for review see Bottema-Beutel, 2016).
Deictic gesture use and language development
As described, gestures provide a way for infants and young toddlers to communicate prior to the development of spoken language. Furthermore, gesture use in the first years of life facilitates the development of receptive and expressive language in typically developing children (Rowe & Goldin-Meadow, 2009; Watt, Wetherby, & Shumway, 2006), including predicting first words and two-word combinations in a child’s verbal lexicon (Iverson & Goldin-Meadow, 2005). Specifically, children’s use of deictic gestures to draw their parents’ attention to an object (joint attention) provides opportunities for parent translation of the gesture into words, facilitating child vocabulary development (Kishimoto, Shizawa, Yasuda, Hinobayashi, & Minami, 2007; Ozcaliskan & Dimitrova, 2013). Gesture use has also been shown to predict both receptive and expressive language development in children with ASD (Gordon & Watson, 2015; Luyster, Kadlec, Carter, & Tager-Flusberg, 2008; Manwaring, Mead, Swineford, & Thurm, 2017). A recent study examining a range of gestures in an observational context found that deictic gesture use, in particular, is important in the development of spoken language of young children with ASD (Ozcaliskan, Adamson, & Dimitrova, 2016).
Purpose of study
Significant advances have been made in the early identification of ASD over the past decade (Zwaigenbaum et al., 2015; Zwaigenbaum, Bryson, & Garon, 2013). Research in this area suggests that gesture deficits are a useful indicator of ASD in early development, and that deictic gesture use is important in the development of language. To identify the extent to which deictic gesture use has been examined in young children with or at-risk for ASD ≤ 36 months of age and to identify gaps in the literature that inform future research, a scoping review was conducted. A scoping review is “a form of knowledge synthesis that addresses an exploratory research question aimed at mapping key concepts, types of evidence, and gaps in the research related to a defined area or field by systematically searching, selecting, and synthesizing existing knowledge” (Colquhoun et al., 2014, p. 1292). This scoping review specifically examined: (a) deictic gesture types that may differentiate young children with ASD from those with typical development or other developmental delays, (b) how differences in deictic gesture use in toddlers with ASD are related to communicative function or age, and (c) the relationship between deictic gesture and the development of language.
Methods
Inclusion criteria
Inclusion criteria for the present review were part of a larger scoping review project aimed at examining the development of a range of gestures in young children throughout early childhood. Inclusion criteria for the larger scoping review were defined as: (a) peer reviewed journal articles written in English, (b) human participants with no hearing loss or visual impairment, (c) mean age of participant groups ≥6 months and ≤5 years, 11 months, (d) quantitative study, and (e) one or more clearly identified measures of child gesture, with gesture data reported. The following additional criteria were applied for the present review: (a) study included a group of children with or at-risk for ASD that was compared (statistically) to a typically developing (TD) and/or non-ASD developmentally delayed (DD) group on at least one aspect of deictic gesture use, (b) mean age of all participant groups was ≤36 months, and (c) deictic gesture use was examined in an observational context and reported on independent from other gesture types.
For purposes of this review, children considered at-risk for ASD specifically included high-risk infant siblings of children diagnosed with ASD (HR-ASD sibs). Gesture use in young children with or at-risk for ASD has been examined within a variety of contexts and across different measures, including standardized observational measures, detailed coding from video recordings collected in laboratory or home settings, as well as parent report measures. Parent report measures generally report a gesture composite score (including both deictic and representational gestures), without detailing results on individual gestures (e.g. pointing). In contrast, observational and direct measures often report on individual gestures and gesture categories, including deictic gestures. For purposes of this review, studies reporting on gestures measured through observational methods were included to allow for examination of the full range of individual deictic gestures.
Deictic gestures included pointing, showing, giving, and reaching, or some combination of these gestures. Pointing was defined as index finger pointing and could be distal or contact. This was in contrast to reaching, which was defined as extending the arm with an open palm or repeated opening/closing of the hand. Showing was defined as holding up or extending an object toward another person, and giving involved transfer of an object to another person.
Search procedures
Methodology for this scoping review was in accordance with guidelines from The Joanna Briggs Institute, a leader in developing tools and standards for evidence syntheses such as scoping reviews (The Joanna Briggs Institute, 2015). A librarian conducted a comprehensive literature search on 10 February 2016 in four electronic databases: PubMed, PsycINFO, CINAHL, and ERIC, using a combination of relevant keywords and controlled vocabularies such as MeSH terms. Search strategies were adjusted to each database. Strategies were intentionally designed to be sensitive (comprehensive) to include all relevant articles. Search strategies and limits for all databases are provided in Supplemental Information. Searches were limited to peer-reviewed journal articles published in English on or after 1 January 2003, as the present review was designed, in part, to follow up and supplement a previous review of gesture in typical and impaired populations (Capone & McGregor, 2004). A PubMed status subset search was conducted on 18 February 2016 to capture additional articles that had not yet been indexed by the date the literature search was conducted (Pubmed Help [Internet]). Further, the reference lists of included articles were reviewed by hand to identify additional articles (Booth, Sutton, & Papaioannou, 2016; Higgins & Green, 2011).
Study selection
The process for final study selection is outlined in Figure 1 (following Moher, Liberati, Tetzlaff, & Altman, 2009). Citations from the four databases were downloaded and deduplicated using EndNote X7. Remaining citations were uploaded into Covidence systematic review software (“Covidence Systematic Review Software,” n.d.). Articles were reviewed in two phases: titles/abstracts followed by full text review. Prior to reviewing titles and abstracts, a random sample of three sets of 25 articles was selected to establish reliability among reviewers. As phase one (title/abstract review) was designed to be over-inclusive (i.e. include all potentially relevant articles), all reviewers were required to achieve 100% reliability for “kept” articles.
PRISMA four-phase flow diagram for selection of articles.
In the first phase, six reviewers examined titles and abstracts to identify relevant articles, with all titles/abstracts reviewed by two reviewers independently. In the second phase, three reviewers (including the first two authors) assessed the full-text of all potentially relevant articles for eligibility, with all articles reviewed by two reviewers independently. Discrepancies among reviewers were resolved through consensus with the first author.
Data extraction
Extracted data were compiled in an electronic Microsoft Excel template that included the following study and participant characteristics: study groups and diagnoses, sample size, participant ages (i.e. chronological, verbal, and nonverbal mental age), matching procedures, deictic gesture types measured and corresponding definitions, observational measurement context, communicative function of the gesture(s) if provided (e.g. declarative versus imperative pointing), and results related to group differences on deictic gesture use as well as the relationship between deictic gesture and concurrent or later language (receptive or expressive).
Studies were determined to have matched on chronological age if an explicit age-matching statement was provided or if participants were examined at specific age points (e.g. 12 and 18 months). The determination of whether a study matched on language and/or nonverbal level was based on explicit statement(s) of matching procedures outlined in each study. Verbal and nonverbal mental ages of participants for studies that measured these skills at a different time point than when gesture was measured were not included. Therefore, to be considered matched on language or nonverbal development, a study needed to measure those variables at the same time point as the gesture measurement.
Synthesis of results
A narrative synthesis was conducted, as a meta-analysis was not feasible due to differences across studies in variables reported and assessment methods. Summary statistics (e.g. means, standard deviations) associated with each group comparison were extracted, and where possible, an effect size was calculated. Cohen’s d was used as the effect size statistic when means and standard deviations or standard errors were provided, with d = .2, .5, .8, representing a small, medium, and large effect size, respectively (Cohen, 1992). When percentages or proportions were reported, the data were transformed so that an approximation to Cohen’s d could be calculated. Each proportion was transformed using the square root of the arcsin of the proportion and the effect size reported is the difference of these transformed proportions (Lipsey & Wilson, 2001).
Results
Summary of included studies
Study characteristics.

ASD: autism spectrum disorder; HR-ASD sibs: high-risk infant siblings of children diagnosed with ASD. Where HR-ASD Sibs is target group, information in parentheses indicates the specific groups the study examined. ESCS: Early Social Communication Scales; CSBS: Communication and Symbolic Behavioral Scales; ADOS: Autism Diagnostic Observation Schedule.
Note: Target Group represents primary group examined.
Pointing/showing to initiate shared attention to object/event.
Pointing/giving to obtain an object/event.
Gesture measured at one time point.
Deictic gesture measurement
The studies varied in the specific deictic gestures measured, with some examining individual gestures (e.g. pointing) and others examining multiple deictic gestures together (e.g. total deictic). Gestures included in the total deictic category varied across studies. The most frequently measured gesture was pointing, with all studies measuring the point gesture in some way. Specifically, 10 of the 19 studies reported on pointing apart from other gestures, while the remaining studies examined pointing in combination with other gestures (e.g. as part of IJA/IBR or a total deictic category). Sixteen studies measured the show gesture, with seven of these studies (four ASD, three HR-ASD sibs) reporting on showing apart from other gestures. Giving and reaching were the least examined gestures. Reaching was examined in seven studies, with four (two ASD, two HR-ASD sibs studies) reporting on the reach gesture in isolation. Giving was examined in four studies, but only reported on in isolation in one study of HR-ASD sibs (Winder et al., 2013).
One of the 19 studies reported on deictic gesture use paired with speech. Specifically, Winder et al. (2013) examined the frequency of deictic gestures that overlapped with speech, including Deictic Gestures + Communicative Non-word Vocalizations and Deictic Gestures + Words. One study focused specifically on deictic gestures that referred to objects the child did not produce in speech, excluding gestures the children used to refer to objects also expressed in speech during the observation (Dimitrova, Ozcaliskan, & Adamson, 2016). In other studies, gestures with speech (vocalizations or words) were not specifically examined or reported on separately. Definitions of gestures across several studies, such as those measuring gesture using a semi-structured standardized assessment tool (described below), indicated that gestures may have been accompanied by speech (or eye contact or other aspects of verbal and nonverbal interaction), but that speech was not required to be present for a gesture to be coded. Other studies made no mention of gestures in relation to spoken language.
Observational context
Studies varied in the observational context in which gestures were measured (see Table 1). Five studies utilized naturalistic or semi-naturalistic parent–child interactions, three of which conducted home observations (all HR-ASD sib studies). Three studies retrospectively examined home videotapes of children later diagnosed with ASD. One study observed gesture use in community hospitals using an observational screening tool (Huang et al., 2014). The 10 remaining studies observed gesture within more semi-structured contexts, for example, the ESCS (Seibert et al., 1987), the Behavior Sample from the Communication and Symbolic Behavior Scales-Developmental Profile (Wetherby & Prizant, 2002), or the Autism Diagnostic Observation Schedule (Lord et al., 2000).
Communicative function
Eight of the 19 studies reported on gesture use in relation to communicative function. Five studies examined IJA (i.e. pointing or showing to initiate shared attention to objects or events with another person) and IBR (i.e. pointing or giving to elicit aid in obtaining an object or event) as measured on the ESCS (Seibert et al., 1987). Two other studies examined pointing and/or showing in imperative (requesting) and/or declarative (commenting) contexts (Clifford, Young, & Williamson, 2007; Werner & Dawson, 2005), and one study examined total deictic and reaching in both commenting and requesting contexts (Ozcaliskan, Adamson, & Dimitrova, 2016).
Summary of participants
Participant characteristics for studies of autism spectrum disorder (ASD).
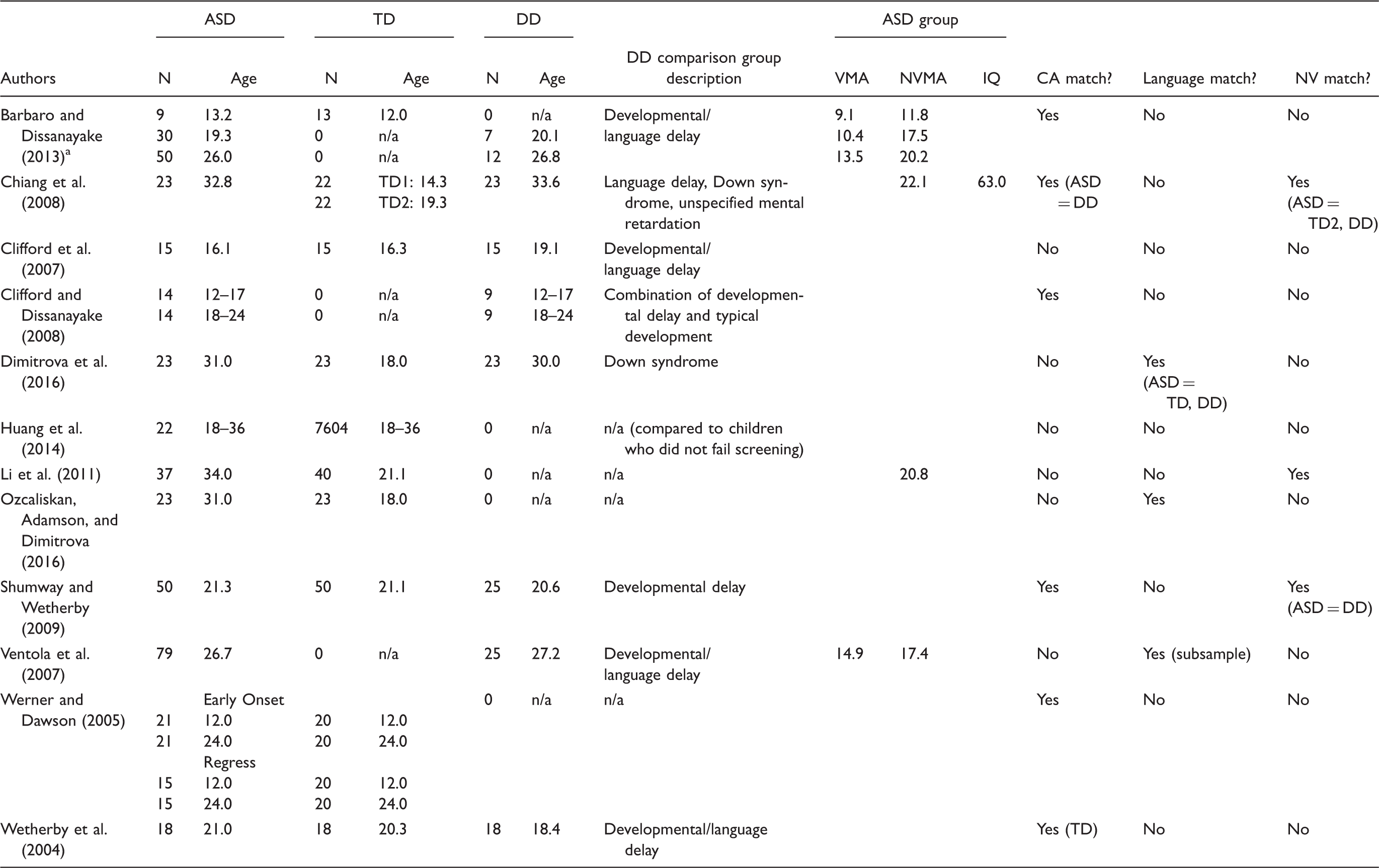
TD: typically developing; DD: developmental delay; CA: chronological age; VMA: verbal mental age; NVMA: nonverbal mental age.
Mean age of children with autistic disorder and ASD.
Participant characteristics for studies of high-risk infant siblings of autism spectrum disorder (HR-ASD sibs).

TD: typically developing; CA: chronological age; VMA: verbal mental age; NVMA: nonverbal mental age.
Mean for ASD group.
Mean for HR-ASD sibs group.
The majority of participants in the seven HR-ASD sibs studies were younger than 24 months when gestures were examined. One study examined a group of toddlers at 24 and 36 months (LeBarton & Iverson, 2016b). In the three HR-ASD sibs studies that examined the subgroup of children later diagnosed with ASD, the number of participants with ASD ranged from 3 to 17, measured from 12 to 36 months of age. All HR-ASD sibs studies included a low-risk TD comparison group matched on chronological age in the majority (6/7) of cases.
Results of deictic gesture use in toddlers with or at-risk for ASD
Results on group differences and calculated effect sizes for deictic gesture use in ASD and HR-ASD sibs studies are described below. A summary of group differences for different deictic gesture types is presented first, followed by results relating to differences in gesture use based on communicative function and age. Of note, results related to group differences in IJA and IBR are specifically presented in the section on communicative functions.
Deictic gesture types
Group differences in gesture use for studies of children with autism spectrum disorder (ASD).
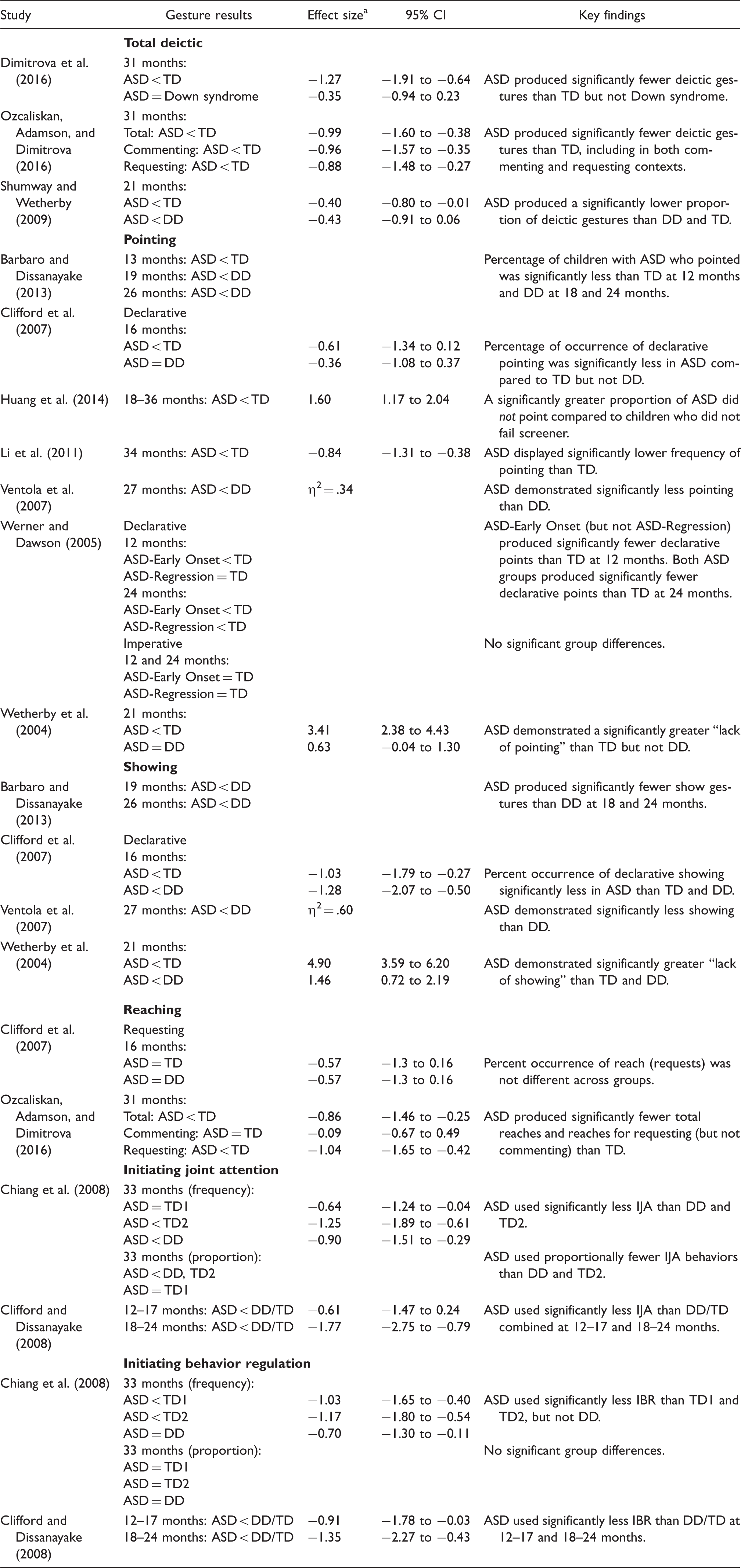
TD: typical development; DD: developmental delay.
Note: Significant group differences indicated by less than sign. Equal sign indicates no significant group difference. Ages reflect mean age of ASD group, rounded to nearest month.
Unless otherwise indicated, effect size is based on Cohen’s d. η2: Eta2 effect size reported in original study.
In relation to pointing, studies that compared toddlers with ASD and TD reported significantly reduced pointing in the ASD group as young as 12 months, with results of one study suggesting these differences may be related to communicative function (i.e. declarative versus imperative) and the onset of ASD symptoms (Werner & Dawson, 2005). Two of four studies that compared toddlers with ASD to those with DD found significant group differences on pointing around 2 years of age. Effect sizes for group differences on pointing ranged from medium to large (although not reported or calculated for all studies). All ASD studies that measured showing (n = 4) reported reduced showing in toddlers with ASD compared to those with TD and DD as young as 16 months of age, with large effect sizes. Giving was not examined in ASD studies. One of the two studies that compared toddlers with ASD to TD on reaching reported significantly reduced reaching in toddlers with ASD at 31 months (Ozcaliskan, Adamson, & Dimitrova, 2016). However, this difference in reaching appeared related to communication function (described below). In the only study that compared toddlers with ASD to a DD group on reaching (Clifford et al., 2007), no significant differences were found between the groups.
Group differences in gesture use for studies of high-risk infants siblings of children with autism spectrum disorder (HR-ASD sibs).

NonASD-Sibs: HR-ASD sibs who did not receive diagnosis of ASD at outcome; High-risk sibs included children with and without an ASD diagnosis; TD: typical development.
Note: Significant group differences indicated by less than sign. Equal sign indicates no significant group difference. Ages reflect mean age of target group, rounded to nearest month.
Effect size is based on Cohen’s d.
No HR-ASD sibs studies comparing siblings with and without an ASD outcome found significant group differences on pointing. Significantly reduced showing was found at 13 and 18 months (but not later) for HR sibs diagnosed with ASD compared to NonASD and TD sibs. Giving was measured in one study, with results indicating siblings later diagnosed with ASD gave significantly less than NonASD-Sibs at 18 months. The only significant group difference for the reach gesture in HR sibs later diagnosed with ASD was at 13 months, with toddlers with ASD producing fewer reaches than NonASD-Sibs.
Studies that compared a High-risk sibs group (i.e. siblings with and without a diagnosis of ASD) to TD reported significantly reduced pointing at 18 (but not 13) months and showing at 13 and 18 months, with effect sizes ranging from d = −1.01 to −1.26. No significant differences were found between High-risk sibs and TD on total deictic, giving, or reaching. Both HR-ASD sibs studies that reported on NonASD-Sibs (i.e. sibs that did not receive an ASD diagnosis) compared to a TD control group, reported significantly reduced total deictic (point/show combined) and pointing in Non-ASD-Sibs between 18 and 20 months (Leezenbaum et al., 2014; Toth et al., 2007). No significant differences between Non-ASD-Sibs and TD were found at younger ages (i.e. 13 months) or for other gestures (i.e. giving/reaching combined, showing in isolation).
Results from the one study (Winder et al., 2013) that examined deictic gestures that overlapped with speech indicated that HR-ASD sibs (with and without a later ASD diagnosis) produced Gesture + Non-word Vocalizations at a significantly lower rate than TD at both 13 and 18 months (d = −1.57, 95% CI = −2.39 to −0.75; d = −1.73, 95% CI = −2.57 to −0.89, respectively). Gesture + Word combinations were also significantly reduced in HR-ASD sibs at 18 (d = −2.28, 95% CI = −3.2 to −1.36) but not 13 months (d = 0.43, 95% CI = −0.30 to 1.15). The results were similar in the subgroup of HR sibs later diagnosed with ASD (n = 3) compared to NonASD-Sibs. Specifically, the subgroup of toddlers with ASD produced fewer Gesture + Non-word vocalizations at 13 and 18 months, and fewer Gesture + Word combinations at 18 months. The only effect size that could be calculated for the ASD versus NonASD-Sibs comparisons was for Gesture + Non-word vocalizations at 18 months (d = −3.56, 95% CI = −5.35 to −1.76), as all other means in the ASD group were zero.
Communicative function of deictic gestures
Findings from studies of toddlers with ASD indicated that group differences in the use of some deictic gestures varied based on communicative function. One study compared the frequency of total deictic gestures used for commenting versus requesting, and found that toddlers with ASD used significantly fewer total gestures for both functions compared to those with TD, with large effect sizes associated with group differences in both commenting and requesting contexts (Ozcaliskan, Adamson, & Dimitrova, 2016). Results of a study comparing declarative and imperative pointing suggest that differences in pointing between toddlers with ASD and those with TD may be related to communicative function, with toddlers with ASD using significantly reduced pointing for declarative (but not imperative) purposes as early as 12 months (Werner & Dawson, 2005). Clifford et al. (2007) found that declarative pointing and showing were significantly reduced in toddlers with ASD compared to TD, with a medium effect size for pointing (d = −0.61) and a large effect for showing (d = −1.03). However, only declarative showing (not pointing) differentiated children with ASD from those with DD, with an effect size of d = −1.28. Two ASD studies examined reaching for requesting, with toddlers with ASD producing significantly fewer reaches to request than toddlers with TD at 31 (Ozcaliskan, Adamson, & Dimitrova, 2016) but not 16 months (Clifford et al., 2007). Interestingly, toddlers with ASD and TD were not significantly different on reaches used for commenting (Ozcaliskan, Adamson, & Dimitrova, 2016). In relation to IJA and IBR, toddlers with ASD younger than 24 months used significantly less IJA and IBR compared to those with TD/DD, with effect sizes ranging from d = −.61 to −1.77. Group differences became more variable during the third year, as toddlers with ASD used significantly less IJA, but not IBR, than DD comparisons.
Three HR-ASD sibs studies examined the communicative function of gestures, specifically IJA and IBR, which were both measured as early as 8 months. HR-ASD sibs with an ASD outcome used significantly less IJA and IBR than TD and NonASD-Sibs at 12 months, with medium effect sizes for IJA and large effect sizes for IBR (Rozga et al., 2011). No differences were found on IJA or IBR between NonASD-Sibs and TD. Findings were more variable across the two studies that examined IJA and IBR in samples of High-risk sibs – children with and without an ASD diagnosis (Cassel et al., 2007; Yirmiya et al., 2006). One study reported significantly reduced IJA in High-risk sibs compared to TD at one time point (15 months), and both studies reported differences in IBR between 12 and 14 months, but not at other time points. Differences in sample sizes and matching procedures may have contributed to these variable findings.
Differences in deictic gesture use based on age
Summary of between-group differences across gestures and age in autism spectrum disorder (ASD) studies.

TD: typical development; DD: developmental delay.
Note: Plus (+) denotes that the mean of the ASD group was significantly lower than comparison group on a majority (>50%) of comparisons. Minus (−) denotes that the mean of the ASD group was not significantly lower than comparison group on a majority of comparisons. Numbers in parentheses indicate the number of comparisons that were significantly different out of the total number of comparisons in each age range.
Summary of between-group differences across gestures and age in studies of high-risk (HR) infants siblings of children with autism spectrum disorder (ASD).

TD: typical development.
Note: Plus (+) denotes that the mean of the target group was significantly lower than comparison group on a majority (>50%) of comparisons. Minus (−) denotes that the mean of the target group was not significantly lower than comparison group on a majority (>50%) of comparisons. Numbers in parentheses indicate the number of comparisons that were significantly different out of the total number of comparisons in each age range.
Results indicate that toddlers with ASD (including those from ASD and HR-ASD studies) demonstrate reduced use of some but not all deictic gesture types as early as 12 months of age. Specifically, at 12–13 months of age, differences between toddlers later diagnosed with ASD (identified in HR-ASD sibs studies) and other comparison groups (TD, NonASD HR) were found for total deictic, showing, and reaching, but not for pointing or giving. By 14–18 months, toddlers with ASD exhibited reduced pointing compared to those with TD. Across time (from 12 to 36 months), group differences vary based on comparison group and gesture. For example, a trend in the data can be seen in pointing versus showing in ASD studies. In particular, pointing was significantly reduced in toddlers with ASD compared to those with TD but not DD in a majority of comparisons from 14 to 16 through 36 months (with the exception of 22–24 months). In contrast, showing was significantly reduced in toddlers with ASD compared to those with TD and DD in a majority of comparisons as early as 12–13 months.
The lack of difference between toddlers with ASD and those with TD on pointing between 22 and 24 months appears to be related to communicative function, with toddlers with ASD exhibiting significantly reduced declarative but not imperative pointing (Werner & Dawson, 2005). Other findings related to communicative function indicated that toddlers with ASD showed reduced IJA and IBR compared to TD and DD comparison groups between 12 and 18 months (Clifford & Dissanayake, 2008; Rozga et al., 2011). By the third year (31–36 months), however, group differences in IJA and IBR were more variable. Specifically, toddlers with ASD used significantly less IJA than toddlers with TD and DD matched on nonverbal mental age, but were not different from a younger TD comparison group (Chiang, Soong, Lin, & Rogers, 2008). Toddlers with ASD were not different from those with TD or DD on a majority (>50%) of IBR comparisons between 31 and 36 months of age (Chiang et al., 2008).
Relationship between deictic gesture and language
Two of the 19 studies (one ASD and one HR NonASD-Sibs) reported on the relationship between deictic gesture use and language. Ozcaliskan, Adamson, and Dimitrova (2016) found that the number of total deictic gestures children with ASD produced at a mean age of 31 months (range 21–37) predicted expressive vocabulary as measured on the Expressive Vocabulary Test (Williams, 1997) approximately one year later (age range 34–49 months; rs = 0.72, p = 0.001). Significant correlations between deictic gestures and later expressive vocabulary were found in both commenting (rs = 0.56, p = 0.02) and requesting (rs = 0.74, p < 0.001) contexts. Reaching gestures (total, commenting, or requesting) were not significantly correlated with expressive vocabulary. In a sample of HR NonASD-Sibs, Leezenbaum et al. (2014) found no significant correlations between deictic gestures (points/shows or gives/reaches) at 13 months and non-word vocalizations or words at 18 months (correlations ranged from r = −.027 to .313).
Discussion
The aim of the present study was to review the literature on deictic gesture use in toddlers with or at-risk for ASD, to determine the extent to which deictic gesture use has been examined in and differentiates children with or at-risk for ASD from other DD or TD groups in the first three years of life. Given significant advances in understanding gesture use as a potential aid in early identification and differential diagnosis of ASD, this review was purposefully designed to examine studies that compared a group of children with or at-risk for ASD to one or more comparison groups on the use of deictic gestures. Identifying the range of available evidence to better understand potential deficits in deictic gesture use in toddlers with ASD is a critical step to inform further research and provide evidence to support early identification and differential diagnosis. Key findings related to the specific aims of this review are discussed below, including observed differences in deictic gesture types and how these differences are related to communicative function and age, as well as a discussion of the relationship between deictic gesture use and language development in toddlers with ASD.
Deictic gesture types in toddlers with ASD
Overall, results of this review indicate that deictic gesture deficits are pervasive in toddlers with ASD compared to toddlers with TD. These deficits manifest early in the second year of life, persist through the third year, and are present across several deictic gesture types. While a clear pattern of reduced gesture use in toddlers with ASD was found, results also reveal that toddlers with ASD do gesture. There were few studies in which the mean frequency (or other measure) of gesture was zero in the ASD group. This is a critical detail to consider in early identification and care should be taken to not rule out a diagnosis of ASD because a young child gestures. Furthermore, the evidence supporting deictic gesture deficits in toddlers with ASD is not spread evenly across all deictic gesture types. Overwhelmingly, the most frequently measured gestures were pointing and showing. In contrast, few studies examined giving and reaching. Nonetheless, toddlers with ASD were found to demonstrate reduced use of each type of deictic gesture compared to TD groups. This finding is not surprising, given that ASD is a disorder characterized by deficits in social communication and social interaction that may involve a reduced inclination or motivation toward social engagement (Mundy et al., 2007), reducing frequency of communicative gestures.
The more difficult and necessary question, and what continues to be less clear, is the degree to which deictic gesture deficits are specific to ASD or are common across developmental delays observed in the toddler years. The majority of ASD studies (8 of 12) in this review included a DD comparison group; however, the composition and matching of these groups varied across studies, making it difficult to determine with certainty the specificity of the deficits to ASD. Nonetheless, examination of findings from studies that directly compare toddlers with ASD to a DD group provides some insight into this question.
One finding that emerged is that not all types of deictic gestures are equally impaired in toddlers with ASD. For example, while pointing was significantly and consistently reduced in toddlers with ASD compared to those with TD, pointing did not consistently differentiate ASD from other DD, nor did it differentiate HR-ASD sibs later diagnosed with ASD from other HR (non-ASD) sibs. Showing, on the other hand, was significantly reduced in toddlers with ASD compared to those with TD and other DD from early in the second year, with large effect sizes associated with the group differences. These results suggest that reduced pointing in the second year is a marker for delay, but that reduced showing may be a more specific marker of ASD, at least until closer to 2 years of age.
There was less evidence across the studies reviewed to suggest that toddlers with or at-risk for ASD exhibit reduced giving and reaching in comparison to toddlers with other DD; however, giving was only examined in isolation in one study (Winder et al., 2013), with reduced giving found at 18 months but not earlier. Other studies examined giving in conjunction with other gestures, as with IBR, which consists of giving and pointing. Toddlers with ASD used IBR significantly less than those with TD and DD in the second year; however, it was unclear as to whether these differences may be attributable to deficits in pointing or giving. Another study combined giving with reaching (ritualized request) and found no differences between HR-ASD sibs later diagnosed with ASD compared to language-delayed siblings (LeBarton & Iverson, 2016b). While studies often classify giving as a gesture specifically used for behavior regulation, young children also use the give gesture to communicate for joint attention, and may do this earlier than for requesting purposes (Crais et al., 2004).
In sum, results of this review clearly point to deictic gesture deficits in toddlers with ASD relative to toddlers with TD. The current literature remains less clear for distinguishing toddlers with ASD from other DD and suggests variability in the specific deictic gesture types that may differentiate ASD in the toddler years. As will be discussed, results highlight factors such as communicative function, age, and onset of ASD symptoms that likely influence the manifestation of these gesture deficits. In addition to considering these factors, looking to research that has examined deictic gestures using observational methods in other delayed or at-risk populations (although not directly in comparison to ASD) may be helpful in clarifying the specificity of deictic gesture deficits to ASD. For example, late-talkers (Vuksanovic & Bjekic, 2013) and toddlers with pre- or perinatal unilateral brain lesions (Ozcaliskan, Levine, & Goldin-Meadow, 2013; Sauer, Levine, & Goldin-Meadow, 2010) as a group have been found to display similar levels of deictic gesture use to TD comparison groups. Toddlers born preterm have also been observed to display similar (Fasolo, D'Odorico, Costantini, & Cassibba, 2010; Sansavini et al., 2015) or even increased use of gesture compared to toddlers with TD (Suttora & Salerni, 2012). Findings from studies comparing deictic gesture use in toddlers with Down syndrome to those with TD have been mixed, with some reporting reduced deictic gesture use in Down syndrome (Dimitrova et al., 2016; Ozcaliskan, Adamson, Dimitrova, Bailey, & Schmuck, 2016), and others reporting no significant group differences (Fidler, Philofsky, Hepburn, & Rogers, 2005). In fact, some research suggests that gesture use may be considered a relative strength in children with Down syndrome (Capone & McGregor, 2004). While it is critical to consider the individual variability in gesture that certainly exists within any one of these groups of children, overall, findings from studies examining other at-risk and delayed populations (apart from ASD) indicate similar gesture use to children with TD. This literature adds supporting evidence to the specificity of gesture deficits in toddlers with ASD.
Young children use pointing and other deictic gestures to engage in interactions, and according to a social-cognitive view, to direct or change the attention of the communicative partner – to influence others’ intentional and mental states (Tomasello, Carpenter, & Liszkowski, 2007). Consideration of the social-cognitive foundations of gesture provides insight into the origin and nature of gesture deficits in individuals with ASD. In typical development, gestures emerge after the acquisition of other social-cognitive skills, such as understanding others’ intentions, attention, and shared knowledge, as well as motivations for cooperation and helping, which are thought to be prerequisite for gesture and linguistic communication (Tomasello et al., 2007). These social-cognitive abilities typically emerge between approximately 9 and 15 months of age. Young children with ASD demonstrate deficits in these early social-cognitive abilities, reducing joint intentions and attention in interactions with others (Landry & Loveland, 1988; Loveland & Landry, 1986; Sigman et al., 1999). The emergence of or deficits in early social-cognitive abilities can alter development in other areas, as well as interactions between parents and children (Siller & Sigman, 2008). Thus, it is critical to consider how early social-cognitive foundations of gesture may affect later gesture and ultimately language development in young children with ASD.
Communicative functions of deictic gesture use in toddlers with ASD
Gesture use in young children with ASD has most often been assessed without reference to communicative function, with less than half of the studies in this review reporting on function. Results of studies that did examine the communicative function of gestures suggest key patterns of differences in this area, indicating an important avenue for understanding gesture differences between toddlers with ASD and other DD or TD. As described, the vast majority of studies found that toddlers with ASD gesture less than toddlers with TD. While there is some variability in the data, results also suggest that group differences for at least some deictic gestures may be related to communicative function, and that these differences may vary based on the specific deictic gesture type and/or age, as well as other factors (e.g. context, communicative partner, intervention) not examined in this review.
Results indicated specific reductions in gesturing for commenting or declarative purposes in toddlers with ASD. For example, differences (or a lack thereof) in pointing between toddlers with ASD and TD at 24 months were related to communicative function, with deficits in declarative but not imperative pointing in toddlers with ASD (Werner & Dawson, 2005). Early deficits in IJA (with a large effect size), persisted into the third year of life in toddlers with ASD, and specifically differentiated toddlers with ASD from those with other DD. These findings are consistent with the well-known joint attention deficits present in individuals with ASD (Dawson et al., 2004; Mundy, Sigman, & Kasari, 1994), and highlight that these deficits are also evident in gestures in the toddler years.
Toddlers with ASD were also found to demonstrate early deficits in gestures used for behavior regulation. For example, toddlers later diagnosed with ASD exhibited reduced IBR compared to those with TD or other DD as early as 12 months of age (Clifford & Dissanayake, 2008; Rozga et al., 2011). While these early deficits in IBR did not persist into the third year of life in the majority of group comparisons examined in this review, they did persist in some comparisons, particularly when comparing toddlers with ASD to those with TD (Chiang et al., 2008). Further, examination of specific deictic gestures (e.g. reaching) indicated deficits related to behavior regulation that persisted into the third year. For example, Ozcaliskan, Adamson, and Dimitrova (2016) found significantly reduced reaching for requesting (but not commenting) in toddlers with ASD at a mean age of 31 months compared to toddlers with TD matched on expressive language. Other research examining the communicative function of gestures in young children with ASD also suggests reduced gesturing for behavior regulation as a red flag for ASD. For example, Watson et al. (2013) found that toddlers with ASD were less likely than those with TD (but not other DD) to use gestures for behavior regulation at both 9–12 and 15–18 months of age. The researchers further examined differences in the subgroup of toddlers with ASD that did gesture (given that not all toddlers gestured), and found that by 15–18 months, the subgroup of toddlers with ASD that gestured were not different from toddlers with TD or other DD on behavior regulation gestures. Overall, findings indicate that exploring the communicative function of gestures over time may be particularly helpful in differentiating toddlers with ASD and provide important information, beyond the quantity of gesture use, to support early identification and early intervention efforts.
Deictic gesture use in toddlers with ASD based on age
Gesture changes over time and with development. For example, research shows that the quantity, types, and functions of gesture change with age (Capone & McGregor, 2004; Crais et al., 2004). Thus, it is critical to consider the influence of age on gesture production. Although findings from this review reveal significant gaps in the literature in understanding specific deictic gestures over time in the first years of life, results also reveal a pattern of reduced gesture use that is present from early in the second year of life (as early as 12 months) in toddlers with or at-risk for ASD. These gesture deficits were found to persist through 36 months of age. Thus, reduced gesture use may be particularly suggestive of persistent delays, even prior to the identification of a spoken language delay in identifying children with or at-risk for ASD.
The assessment of gesture use in toddlers with or at-risk for ASD requires consideration of individual differences in symptom onset patterns that may influence the age at which gesture or other social communication impairments manifest. Studies of symptom onset suggest a range of patterns (Shumway et al., 2011). These onset patterns reflect a “continuum of developmental derailment” (Landa, Stuart, Gross, & Faherty, 2013, p. 437), including an unfolding of ASD symptoms over time “through a process of diminishment of key social communication behavior” (Ozonoff et al., 2010, p. 256), which may influence the age at which children receive an ASD diagnosis (Bacon et al., 2017).
One study in this review examined gesture use (pointing) relative to symptom onset and found that differences in pointing between toddlers with ASD and those with TD varied based on whether ASD symptoms were present early in development or following a loss of skills (Werner & Dawson, 2005). Previous research has suggested that among children with ASD who do attain one or more deictic gestures early in their development, more than half (up to 56%, depending on the specific gesture) stop using the gesture after having used it for a month or longer (Thurm, Manwaring, Luckenbaugh, Lord, & Swedo, 2014). Thus, the age at which gesture deficits become apparent and help aid in the process of differential diagnosis will likely vary for different children.
Relationship between deictic gesture use and language development
Gesture and language are thought to “share a common social-cognitive, social-motivational infrastructure of shared intentionality” (Tomasello et al., 2007, p. 706), with gesture playing a critical role in language learning in typical development (Goldin-Meadow & Alibali, 2013). However, much remains to be learned about the association between gesture and language development in young children with ASD. The one ASD study in this review that examined the relationship between deictic gesture and language reported a large predictive correlation between deictic gesture use in both commenting and requesting contexts at 31 months and expressive vocabulary one year later (Ozcaliskan, Adamson, & Dimitrova, 2016). Findings of a strong correlation between deictic gesture and spoken language in toddlers with ASD highlight the importance of detecting and potentially treating gesture deficits as early as possible. Previous research indicates that children with language delays who compensate for the delay through gesture have better language outcomes than children who do not (Capone & McGregor, 2004; Goldin-Meadow & Alibali, 2013; Thal & Tobias, 1992), and emerging research suggests this is the case for young children with ASD (Ozcaliskan, Adamson, & Dimitrova, 2016).
Limitations and future research directions
Results and discussion of the findings from this review should be considered within the context of limitations of the review, as well as limitations of the studies that met inclusion criteria. In addition, as a scoping review, results obtained help identify areas for future research on deictic gesture use in toddlers with or at-risk for ASD. This section highlights limitations and provides specific needs for areas of future research.
Deictic gesture measurement
This review examined a specific subset of gesture types (i.e. deictic) within a specific measurement context (i.e. observational). Although this was intentional and consistent with our research aims, many studies that have examined other aspects of gesture (e.g. representational gestures), alone or in combination with deictic gestures in different ways (e.g. parent report), were excluded. In addition, the observational contexts varied across studies, ranging from naturalistic play at home with a parent to semi-structured and structured measures conducted in a laboratory setting. These different observational methods likely influence the use of deictic gestures and thus the results of this review. Given that various assessment measures potentially provide different information across deictic gesture types (Ellawadi & Ellis Weismer, 2014), it may be particularly helpful for future studies to include multiple measures and examine correspondence of gesture use across measures and contexts (parent report and direct observation) as well as communicative partners.
Another limitation of this review relates to the variability in the deictic gestures measured, as well as the definitions and coding practices for gestures types and rates across studies. Deictic gesture definitions were difficult to determine based on limited definitions provided in some studies. Providing clear and complete definitions of gestures that align with definitions across other previous studies will enhance reproducibility, allowing researchers to compare and extend findings. Furthermore, while decades of research have examined pointing and indicate it as one of the first ways infants with TD exhibit intentional communication associated with language development (Colonnesi, Stams, Koster, & Noom, 2010), less research has been done to examine other types of deictic gestures (Boundy, Cameron-Faulkner, & Theakston, 2016). Results of this review reveal a similar pattern to the TD literature, in that pointing was the most frequently measured gesture and was measured in all studies. The variability in group differences across deictic gesture types in the included studies suggests a great need to study other deictic gesture types, and to report on results for individual deictic gesture types in isolation in addition to a composite score or measure.
Range of comparison groups
The wide range of children categorized as DD may be a limitation of this review. Any comparison group not identified as TD was categorized as a DD comparison group. This resulted in variability across DD comparison groups in the type and severity of delays (see Table 2). This limitation also reflects the current state of the literature, such that studies examining young children with ASD have used a variety of comparison groups, ranging widely from study to study, with differing definitions or inclusion criteria.
While results show that toddlers with ASD demonstrate deficits in a range of deictic gestures compared to toddlers with TD, the findings were less clear when comparing toddlers with ASD to other DD groups. In part, this may be related to the variable nature of the DD comparison groups, as well as a reflection of delay generally, with gesture delays present in some young children with non-ASD delays in the first years of life. Thus, more research is necessary to examine the degree to which gesture deficits are part of a developmental phenotype for ASD risk or for delay generally. Rigorously designed studies would include well- and more narrowly defined language- and nonverbal-matched comparison groups (e.g. expressive- and receptive-language matched) to aid in determining whether reduced gesture use is specific to ASD or a more general indicator of a language or other developmental delay independent of etiology (Goldin-Meadow & Alibali, 2013). Further, the comparison groups must be described in sufficient detail to allow for fuller understanding of the makeup of the group(s) in order to help rule out alternative explanations for any group differences.
Impact of age and developmental level
Consideration of how age and developmental level may affect gesture use is important in interpreting results of this review and designing future studies. The majority of studies matched the ASD group to the comparison group(s) on chronological age, and these studies generally found gesture deficits in toddlers with ASD compared to age-matched TD toddlers. However, few studies matched (or reported) on nonverbal and/or verbal developmental level, making it difficult to draw strong conclusions about how these areas influence results. Studies (n = 3) that did match toddlers with ASD to a comparison group on nonverbal developmental level reported significantly reduced gesture use in the ASD group (with medium to large effect sizes), suggesting that gesture deficits in toddlers with ASD are not solely attributable to differences in cognitive deficits.
Studies (n = 3) that matched on verbal development found that children with ASD produced significantly fewer gestures compared to expressive language-matched TD groups. However, results of studies comparing toddlers with ASD to language-matched DD groups were more variable. For example, no significant differences were found between toddlers with ASD and those with Down syndrome matched on expressive language (Dimitrova et al., 2016). In contrast, when compared to a language-matched mixed DD group with developmental/language delays, toddlers with ASD demonstrated significantly reduced gesture use, with large effects (Ventola et al., 2007). Of note, these two studies matched on different measures of verbal ability (expressive vocabulary compared to the Communication domain of the Vineland Adaptive Behavior Scales).
Increased understanding is needed around how development in nonverbal and verbal areas influences gesture use in toddlers with ASD, moderates the relationship between gesture and language development, and whether patterns differ in other clinical groups. Controlling for or examining gesture use in relation to verbal and nonverbal development is critical to differential diagnosis. Related, measurement and reporting of verbal and nonverbal developmental levels in all groups of children will improve understanding of how abilities in these areas affect gesture use. For example, toddlers with low mental ages may use limited gesture regardless of etiology, emphasizing the need to consider differential diagnosis in the context of development generally. In addition, research is needed to examine gesture at multiple time points across the second and third years of life to determine how gesture use changes with age and language ability within and across populations and at what age(s) deficits in various types of deictic gestures may be identified in young children with ASD.
Factors influencing gesture use
A variety of other factors not fully considered in this review or in the studies that met inclusion criteria may also influence gesture use and contribute to group differences or a lack thereof. These may include factors such as socioeconomic status, severity of symptoms/risk, or development in domains other than language and nonverbal cognition (previously described). Development in one area is not independent of development in other areas, but rather intertwined in complex ways (Leonard & Hill, 2014), with different skill pathways interacting and building upon each other within the context of the child’s development and environmental contexts (Bennett et al., 2015).
As an example, development in gross and fine motor has been found to impact communication and language development (Leonard & Hill, 2014). Young children with or at-risk for ASD often exhibit motor delays (Bhat, Galloway, & Landa, 2012; LeBarton & Iverson, 2013), and these delays may have a cascading developmental effect on communication, including gesture (Iverson, 2010; LeBarton & Iverson, 2016a). Gesture use requires the integration of several developmental skills, and research in ASD supports theories of a developmental relationship of both motor and gesture as important for early language learning (Manwaring et al., 2017). Future studies of gesture in young children with or at-risk for ASD are needed to longitudinally examine the relationship between gesture and other developmental and environmental variables that may interact and influence language and other outcomes in children with ASD.
Future studies
Gestures provide young children a means to communicate nonverbally while spoken language is emerging, and facilitate the development of language; thus, it is critical to detect gesture deficits in a timely manner and work to increase children’s use of gestures. Future research may focus on examining the relationship between specific types of gestures and language in different populations to improve understanding of the facilitative role of gestures in language development in young children with ASD and potentially inform treatment studies. Specific research questions may include whether gestures serve the same function they do in children with TD in paving the way for language development, and if so, does this relationship vary by gesture type and age? Can we predict, as in TD, the specific words a child with ASD will produce by looking at the objects the child gestured to several months earlier (Iverson & Goldin-Meadow, 2005)? Does charting early gesture in children with ASD inform when a child is likely to acquire specific linguistic constructions (Goldin-Meadow, 2015)?
Research is also needed to determine if and when gesture plays a causal role in the development of language in young children with ASD. Emerging evidence suggests that manipulating (experimentally increasing) gesture in toddlers with TD leads to increases in language (LeBarton, Goldin-Meadow, & Raudenbush, 2015). While gesture is commonly targeted as part of comprehensive treatment programs for children with ASD, the extent to which specifically teaching or manipulating gesture use leads to increases in language in children with ASD is not known.
Summary
This scoping review provides an overview and synthesis of deictic gesture use in infants and toddlers with or at-risk for ASD. Results highlight where significant gaps in understanding of deictic gesture deficits in young children with ASD persist as well as some developmental patterns that may aid in early identification and intervention. Pointing and showing were markedly reduced in toddlers with ASD as early as 12 months of age. Pointing deficits, however, may be more related to general developmental delay than specific to ASD in the first two years of life, and patterns of differences are likely related to communicative function (commenting versus requesting). Reduced showing was found to differentiate toddlers with ASD from those with TD and DD early in the second year. Several factors including age, verbal/nonverbal cognitive ability, communicative function, and sampling context likely influence gesture use and patterns of group differences found across studies. Future research should consider these factors in order to advance understanding of gesture deficits and strengths in toddlers with or at-risk for ASD and other neurodevelopmental disorders.
Footnotes
Acknowledgements
The authors extend their gratitude to the research assistants in the Early Childhood Communication Lab, particularly Melissa Delmonte and Sarah Gariepy, for their helpful assistance with this review project. We also thank Molly McFadden at the Study Design and Biostatistics Center for her time and helpful guidance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This investigation was supported by the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant 5UL1TR001067-02 (formerly 8UL1TR000105 and UL1RR025764).
Supplementary material
Supplementary material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.