
Abstract
Background and aims
Young children with language delays or other factors that heighten risk for autism spectrum disorder often show reduced gesture use. In particular, deictic gestures such as pointing and showing are reported to be deficient in young children with autism spectrum disorder, and their use has been found to predict expressive vocabulary development. The first aim of this study was to examine the production of two types of gestures (deictic and conventional) for two communicative functions (behavior regulation and joint attention) across two observational contexts in a sample of 18-month-old toddlers with significant language delays compared to typical controls. The second aim was to examine if and how gesture use (type and communicative function) at 18 months is associated with later receptive and expressive language.
Methods
Toddlers with significant language delays (n = 30) or typical development (n = 62) were drawn from longitudinal studies of early language delay as a risk factor for autism spectrum disorder. Toddlers identified with early language delay were classified based on a diagnosis of autism spectrum disorder (n = 12) or non-autism spectrum disorder (n = 18) after an evaluation at 36 months. Gestures were coded from video recordings of the Communication and Symbolic Behavior Scales Developmental Profile–Behavior Sample and a naturalistic parent–child interaction obtained at 18 months. Language outcomes included receptive and expressive age equivalents from the Mullen Scales of Early Learning and the number of words produced on the MacArthur–Bates Communicative Development Inventories.
Results
At 18 months, toddlers with language delay showed reduced deictic and conventional gesture use in both the Communication and Symbolic Behavior Scales Developmental Profile–Behavior Sample and parent–child interaction compared to toddlers with typical development. Within the language delay group, toddlers with an autism spectrum disorder diagnosis at outcome also produced significantly fewer deictic gestures than those without an autism spectrum disorder diagnosis across both communicative functions and observational contexts. While all groups of toddlers gestured more in the Communication and Symbolic Behavior Scales Developmental Profile–Behavior Sample, the mean difference in gesture use between the Communication and Symbolic Behavior Scales Developmental Profile–Behavior Sample and parent–child interaction was significantly larger in toddlers with typical development than language delay for deictic gestures, as compared to the difference between the two contexts for conventional gestures. In the combined sample, a significant association was found between deictic gestures used in the Communication and Symbolic Behavior Scales Developmental Profile–Behavior Sample and change in the number of words produced from 18 to 36 months, accounting for significant demographic and developmental confounders.
Conclusions
Findings show that early language delay is associated with reduced deictic and conventional gestures across observational contexts. Importantly, deictic gesture use, but not conventional, was associated with the development of expressive language in toddlers with and without language delays.
Implications
Deictic gestures play an important role in the development of expressive language in toddlers, including those with language delays. Assessment of young children with language delays should include evaluation of types of gestures used and communicative function of gestures, with assessments utilizing communicative temptations yielding higher rates of gesture production. Directly targeting both gesture type and function in early intervention may be important in facilitating the development of language.
Introduction
Gestures involve movements of the body, particularly the fingers, hands, and head, that are interpreted as a form of intentional communication (Iverson & Thal, 1998). Reduced gesture use has been reported in toddlers with language delays (LD) early in development (Hsu & Iyer, 2016; Iverson et al., 2018; Luke, Ritterfeld, Grimminger, Liszkowski, & Rohlfing, 2017), and is a prominent prodromal feature of autism spectrum disorder (ASD; Yirmiya & Charman, 2010). Studies of infants at increased genetic risk for ASD due to having an older sibling diagnosed with the disorder indicate that reduced gesture use is present in infancy (Mitchell et al., 2006) and persists over time (Iverson et al., 2018) in infants later diagnosed with ASD. Both the type and the communicative function of gestures are important to examine in young children who display features that put them at heightened risk for ASD (see Manwaring, Stevens, Mowdood, & Lackey, 2018 for review), as these social communication behaviors can be directly and successfully targeted in early intervention (Chang, Shire, Shih, Gelfand, & Kasari, 2016; Goldin-Meadow, 2015; Law, Neihart, & Dutt, 2018).
Children most commonly produce two main types of gestures—deictic and representational (Iverson & Thal, 1998). Deictic gestures, such as pointing, establish reference to indicate or call attention and can be used to indicate a wide range of meanings in the immediate environment (Bates, Camaioni, & Volterra, 1975). Representational gestures identify a referent and carry fixed semantic meaning. Representational gestures may include (a) culturally defined conventional gestures (e.g., shaking head for “no,” waving for “bye”), (b) iconic gestures (e.g., moving arms in the air to represent an airplane flying), or (c) baby signs, which involve hand movements deliberately taught by an adult (e.g., bringing the hands together and tapping the fingertips to indicate “more”).
Deictic and representational gesture types may be used to communicate a variety of communicative functions or intentions, including behavior regulation and joint attention (Bruner, 1981). Behavior regulation involves communicating for an instrumental or imperative function, such as protesting an action/object or requesting to elicit supportive action or aid from another person (Bruner, 1981; Wetherby & Prizant, 2002). Gestural examples of behavior regulation include a child pointing to an item (e.g., snack, toy) to request, giving an object to an adult to request help, or shaking head “no” to protest. Joint attention involves communicating to direct another person's attention to something to share interest or comment on the object or event, with the child's goal being to get the other person to notice something (Bruner, 1981; Wetherby & Prizant, 2002). Gestural examples of communicating for joint attention include pointing to or showing an object to get another person to notice it, or flipping hands in the air to indicate “uh oh” in response to an event.
Other terms have been used to express these communicative functions of behavior regulation and joint attention, particularly as they relate to deictic gestures. Proto-imperative has been used to denote a requesting (behavior regulation) function, and proto-declarative to indicate a commenting (joint attention) function of deictic gestures (Bates et al., 1975), particularly the point gesture (Colonnesi, Stams, Koster, & Noom, 2010). For purposes of this study, we use the terms behavior regulation and joint attention to be consistent with terminology used in the standardized assessment utilized in this study—The Communication and Symbolic Behavior Scales Developmental Profile (Wetherby & Prizant, 2002). Children are typically communicating for both the function of behavior regulation and the function of joint attention by the end of the first year of life; however, this may vary based on the specific gesture type (Crais, Douglas, & Campbell, 2004).
Young children with or at-risk for language disorders often exhibit delays or differences in the use of gestures (Capone & McGregor, 2004); however, the presence and pattern of gesture deficits appear to vary across and within specific delayed populations (see LeBarton & Iverson, 2017 for review). Previous findings from studies examining early gesture use in toddlers with LD have been somewhat mixed, and suggest that differences may relate to the magnitude or type of LD. For example, some toddlers with LD, particularly those with an expressive-only delay, may compensate for their delay in spoken language by gesturing as much or more than age- and language-matched controls (Thal & Tobias, 1992, 1994), while toddlers with an additional delay in receptive language are more likely to show reduced gesture use compared to toddlers with typical development (TD) or expressive-only LD (Ellis & Thal, 2008; O'Neill & Chiat, 2015; Thal & Tobias, 1992; Thal, Tobias, & Morrison, 1991).
Gesture deficits have been identified as one of the earliest social communication indicators of ASD (Iverson et al., 2018; Mitchell et al., 2006; Yirmiya & Charman, 2010). Young children with ASD may demonstrate particular difficulty with deictic gestures compared to toddlers with TD (LeBarton & Iverson, 2016; Manwaring et al., 2018; Ozcaliskan, Adamson, & Dimitrova, 2016). Differences in the communicative function of gestures used by young children with ASD have also been found. Although there is some variability in findings across studies, reduced gestures used for behavior regulation have been reported in toddlers with ASD (e.g., Clifford & Dissanayake, 2008; Ozcaliskan, Adamson, & Dimitrova, 2016; Rozga et al., 2011; Watson, Crais, Baranek, Dykstra, & Wilson, 2013). A more pronounced deficit has been found in the use of gestures for joint attention in children with ASD compared to children with TD or other developmental delays (e.g., Watson et al., 2013; Werner & Dawson, 2005). This pronounced impairment in joint attention has important implications for the development of language, with substantial literature supporting an association between joint attention and receptive and expressive language development (see Bottema-Beutel, 2016 for review).
Researchers examining gestures in young children have typically measured gesture type (e.g., Barbaro & Dissanayake, 2013; Winder, Wozniak, Parlade, & Iverson, 2013) and gesture function (e.g., Chiang, Soong, Lin, & Rogers, 2008; Rozga et al., 2011; Watson et al., 2013) independently. However, a recent study examined both type and function of gestures in 31-month-old (range = 21–37 months) toddlers with ASD and 18-month-old toddlers with TD comparable on expressive language at the group level (Ozcaliskan, Adamson, & Dimitrova, 2016). This study measured gesture type and function using the Communication Play Protocol (Adamson & Bakeman, 1999), a 20-minute semi-naturalistic parent–child interaction (PCI) during which the parent was provided with cues to facilitate communication while interacting with the child during four 5-minute contexts. Two interactions are designed to encourage joint attention and two interactions to encourage requesting. Results indicated that children with ASD produced fewer deictic gestures across the whole session compared to children in the TD group, while differences on representational gestures (conventional and iconic) were not observed. Examination of gesture types across communicative functions revealed that children with ASD produced significantly fewer deictic gestures in both commenting and requesting contexts and fewer conventional gestures in the requesting context compared to children with TD.
Decades of research have revealed a robust correlation between gesture use and the later development of receptive (Rowe & Goldin-Meadow, 2009; Rowe, Ozcaliskan, & Goldin-Meadow, 2008; Watt, Wetherby, & Shumway, 2006) and expressive (Acredolo & Goodwyn, 1988; Iverson & Goldin-Meadow, 2005; Rowe & Goldin-Meadow, 2009) language in TD. Recent findings suggest that the two broad types of gestures (deictic and representational) may differentially impact later language development, depending on the presence or type of developmental delay (Ozcaliskan, Adamson, & Dimitrova, 2016; Ozcaliskan, Adamson, Dimitrova, Bailey, & Schmuck, 2016). For example, deictic, but not conventional, gestures used for joint attention and behavior regulation were found to predict expressive vocabulary one year later in both toddlers with ASD and those with TD (Ozcaliskan, Adamson, & Dimitrova, 2016). In contrast, in a sample of toddlers with Down Syndrome, representational baby signs but not conventional or deictic gestures were significantly related to expressive vocabulary measured one year later (Ozcaliskan, Adamson, Dimitrova, et al., 2016). These differential relationships between gesture use and language in children with varied neurodevelopmental problems suggest that profiles of gesture use in clinical populations should be examined to potentially aid in differential diagnosis and further understanding of language prognostics.
Study purpose
The present study builds on the work of Ozcaliskan and colleagues (2016) to increase understanding of gesture use (both type (deictic and representational) and function (behavior regulation and joint attention)), and the association between gesture and language development in several important ways. First, we examined gesture types and functions in a sample of younger toddlers with significant LD with and without ASD as a diagnostic outcome, matched on chronological age to toddlers with TD. Second, we examined if and how the production of gestures (type and communicative function) is associated with later expressive and receptive language. A third unique contribution of this study was the elicitation or sampling contexts used. Specifically, we examined gesture use across two observational contexts—a naturalistic parent–child free play interaction as well as the Communication and Symbolic Behavior Scales Developmental Profile-Behavior Sample (CSBS; Wetherby & Prizant, 2002), a more semi-structured standardized examiner-led assessment that involves both a clinician and parent and is designed to provide communication opportunities. A key difference between our PCI and the Communication Play Protocol used by Ozcaliskan and colleagues (2016) is that during the Communication Play Protocol, parents are provided with cues to faciliate communication during specific contexts designed to elicit communicative behaviors for behavior regulation (two contexts) and joint attention (two contexts), whereas our parents are instructed to “play with your child as you normally would at home.” The Communication Play Protocol also differs from our second context, the CSBS, in that a clinician administers the CSBS and provides specific communicative temptations across the assessment to encourage communciative behaviors that can be directed to either the clinician or the parent.
To our knowledge, researchers have not examined the effects of observational sampling context on the measurement of early gesture use in toddlers with delays. Limited research examining communicative acts (which may involve but do not require the presence of a gesture) in toddlers with TD suggests some differences in communicative functions across structured vs. unstructured sampling contexts (Coggins, Olswang, & Guthrie, 1987; Wetherby & Rodriguez, 1992). For example, toddlers with TD have been found to communicate more for requesting purposes during a structured clinician-guided sampling context, with similar amounts of commenting used across both structured and unstructured contexts (Wetherby & Rodriguez, 1992). Thus, the present study sought to examine gesture use across two observational contexts to examine whether one context may be more sensitive to group differences and capture diagnostically relevant differences in gesture use in toddlers with early LD.
Based on previous research including populations with heightened risk for ASD (i.e., infant siblings), we hypothesized that in both observational contexts, toddlers with significant LD, particularly those with ASD diagnoses as outcomes, would demonstrate reduced gesture use compared to toddlers with non-ASD outcomes or TD. We further hypothesized that these differences would be greater in deictic gestures and in gestures used to communicate for the purpose of joint attention compared to behavior regulation. We also hypothesized that the production of deictic gestures used for both behavior regulation and joint attention would be positively associated with later receptive and expressive language in all children.
Method
Participants
The present study included toddlers with early LD (n=30) or TD (n = 62) drawn from longitudinal studies conducted at the University of Utah and the National Institute of Mental Health. Participants completed an initial in-person evaluation at 12 or 18 months ( ± 2 months) to determine eligibility for enrollment. Of the 92 eligible toddlers, 67 (73%) enrolled at the 18-month time point.
All toddlers met the following inclusion criteria at study entry: born full-term (≥36 weeks), no known genetic disorder or significant medical or motor impairments, and English reported as the primary language spoken in the home. Toddlers meeting criteria for the LD group had both receptive and expressive language scores in the very low range (T scores ≤ 30) on the Mullen Scales of Early Learning (MSEL; Mullen, 1995) at the time of the initial evaluation, and toddlers in the TD group had MSEL scores on all domains within normal limits (no more than 1.5 standard deviations (SDs) below the mean). As part of the longitudinal study, toddlers were assessed at 18 (n = 92; mean age = 18.60 ± 1.12), 24 (n = 87; mean age = 24.61 ± .79), and 36 (n = 81; mean age = 36.74 ± 1.39) months. Five participants are missing 24-month data (n = 2 LD; n = 3 TD) and a total of 11 are missing 36-month data (n = 5 LD; n = 6 TD) due to moving or unavailability for follow-up.
Toddlers identified with early LD were classified as ASD (LD–ASD; n = 12) or non-ASD (LD–NonASD; n = 18) based on a diagnostic evaluation at 36 months. ASD was diagnosed in toddlers who met or exceeded algorithm cutoffs for ASD on the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2; Lord et al., 2012), with confirmation by clinical judgment of expert doctoral-level clinicians using criteria from the Diagnostic and Statistical Manual for Mental Disorders, 5th edition (American Psychiatric Association, 2013). Using these criteria, 12 of the LD toddlers (40%) were classified as LD–ASD. The remaining 18 toddlers in the early LD group (60%) were classified as LD–NonASD. For the five toddlers in the LD group with missing data at 36 months, the same criteria from the most recent evaluation (18 or 24 month) were used to classify as LD–ASD or LD–NonASD. Specifically, the 24-month time point was used for three toddlers who were classified as LD–NonASD, and the 18-month time point was used for two toddlers who were classified as LD–NonASD. None of the toddlers in the TD group had ASD outcomes.
Summary of participant demographics and characteristics.

Note: Maternal education not reported for one participant in LD-NonASD group.
LD: language delay; ASD: autism spectrum disorder; TD: typical development; MSEL: Mullen Scales of Early Learning; Developmental Quotients = DQ; CDI: McArthur-Bates Communicative Development Inventories.
Because some children achieved the lowest possible standard score on the MSEL, DQs, based on age equivalents divided by chronological age × 100, were used to more fully characterize individual variation. Verbal DQ was calculated from the average of the Receptive and Expressive Language scales. Nonverbal DQ was calculated from the average of the Fine Motor and Visual Reception scales.
Procedure
An Institutional Review Board at both study sites approved this research, and parents/guardians of participants signed consents. Child evaluations were conducted by doctoral-level clinicians in a child-friendly clinical research laboratory setting, with a caregiver present throughout the evaluation. Measures of gesture, language, and ASD symptoms were collected as part of the evaluation. For the present study, gestures were examined at 18 months, with language outcomes measured at 36 months.
Gesture coding and reliability
Gesture measurement contexts. Gestures were coded from videotaped recordings of two measures completed at 18 months: The CSBS (Wetherby & Prizant, 2002) and a PCI. The CSBS is a semi-structured standardized evaluation of the child interacting with a parent and a clinician during a series of activities (e.g., windup toy, bubbles) designed to elicit spontaneous social communication behaviors, including gestures. The mean length of the CSBS was 22.7 ± 3.7 minutes across groups (LD–ASD = 23.0 ± 3.3, LD–NonASD = 22.7 ± 3.6, TD = 22.6 ± 3.8). The PCI consisted of toddlers and parents engaging in a 15-minute free play session with a standard set of age-appropriate toys, including a ball, barn with animals, car and garage, baby doll and kitchen play set, blocks, books, and a puzzle. The only instruction provided was to “play with your child as you normally would at home.” The mean length of the PCI was 15.0 ± 1.2 minutes (LD–ASD = 14.7 ± 2.1, LD–NonASD = 15.1 ± 0.9, TD = 15.0 ± 1.0).
Gesture coding. All communicative deictic and representational gestures produced by children during the CSBS and the PCI were coded using ELAN, a computer software program that allows for the annotation of audio/videotaped language and gesture data (Lausberg & Sloetjes, 2009). Deictic gestures included those used to establish reference in order to indicate or call attention to an object, person, location, or event (Iverson & Thal, 1998) and included pointing, showing, giving, reaching, and other deictic (i.e., indicative gesture in which the child uses his whole hand rather than isolating a finger in a point). Representational gestures included: (a) conventional gestures, which have a culturally defined form and meaning (e.g., waving “hi” or “bye,” shaking head “no”), (b) iconic gestures used to depict the actions or attributes of something (e.g., waving arm in the air to indicate airplane flying), and (c) signs, which include symbolic hand movements from a sign system such as American Sign Language (e.g., bringing the hands together and tapping the fingertips to indicate “more”). Only empty-handed representational gestures were coded.
The communicative function of each gesture was coded, with the functions of behavior regulation and joint attention examined in the present study. Behavior regulation was defined as gesturing for an instrumental or imperative function, such as protesting or requesting objects or supportive action or aid from another person. Joint attention involved gesturing to direct another person's attention to something of interest for a declarative function—to share interest or comment on the object. Of note, any gesture (e.g., pointing) could be used to communicate for either communicative function; specific gestures were not assigned specific communicative functions a priori. The communicative function was determined uniquely for each gesture across both the CSBS and the PCI.
Gesture reliability. Coders were trained on the gesture coding scheme using videotaped samples of children not included in the present study. Independent coding of data for the present study began once a coder reached 85% agreement on all coding categories across three consecutive videos. Ongoing reliability was assessed by having a second coder code a minimum of 15% of the videotaped CSBS and PCI samples for both LD and TD groups. The first step in examining reliability was to assess agreement on identification of gesture. For each gesture identified by both coders, reliability was calculated for classifying the gesture type (e.g., point, show) and communication function. Inter-coder reliability was 89.1% for the CSBS and 91.9% for the PCI (range = 81–100%) for identifying gestures, 95.3% for the CSBS and 95.6% for the PCI (range = 75–100%) for classifying the gesture type, and 94.1% for the CSBS and 93.5% for the PCI (range = 83–100%) for communicative function. Intraclass correlation coefficients ranged from 0.97 to 1.00 across variables in the CSBS, and ranged from .94 to 1.00 across variables in the PCI.
Measures
MSEL (Mullen, 1995). The MSEL is a standardized measure of nonverbal cognitive and language development for children from birth through 68 months. Five domains are assessed including gross motor, fine motor, visual reception, receptive language, and expressive language. Receptive and expressive age equivalent scores were used in the present study as measures of language development. The receptive language domain assesses understanding of verbal directions, memory for commands and general information, and auditory–spatial and auditory–quantitative concepts. The expressive language domain assesses vocalizations and utterances as well as verbal responses to tasks, including the expression of underlying concepts and high-level concept formation. In addition, developmental quotients were calculated as the ratio of mental age to chronological age to characterize individual variability more fully. NVDQ was calculated using the mean age equivalent of the visual reception and fine motor domains, and verbal developmental quotient (VDQ) was calculated using the mean age equivalent of the receptive and expressive language domains.
McArthur-Bates CDI, Second Edition (Fenson et al., 2006). The CDI is a parent-report measure of early communication and language development, and was used as a measure of expressive vocabulary. The measure consists of two forms: the Words and Gestures form and the Words and Sentences form. At a given time point in the present study, participants received different versions of the CDI, depending on their language level. Thus, we created a variable to capture the number of words produced that are common to both versions. Specifically, this was calculated as the number of words (out of the 394 words that are found on both the Words and Gestures and the Words and Sentences form) that a parent reported the child produced. In cases (n = 2 at 36-month time point) where parents completed both versions of the CDI at a given time point, data from Words and Sentences form were used.
Statistical analysis
The total number of each gesture type (deictic, conventional, iconic, and signs) toddlers produced during the 18-month CSBS and PCI was computed, as well as the number of gestures used for each communicative function. Iconic and sign gestures were found to be rare in all groups. In the CSBS, 7.6% of toddlers produced at least one iconic gesture and 30.4% of toddlers produced a sign. The mean frequency was .16 ± .73 for iconic gestures and 1.60 ± 4.59 for signs in the CSBS. In the PCI, 8.9% of toddlers produced an iconic gesture and 14.4% of toddlers produced a sign. The mean frequency was .10 ± .34 for iconic gestures and .42 ± 1.64 for signs in the PCI. Due to the low occurrence of iconic and sign gestures, they were not included in analyses described below.
Negative binomial generalized linear models were used to assess group differences (LD–ASD, LD–NonASD, and TD) in gesture type (deictic and conventional) and function (behavior regulation and joint attention) in the CSBS and the PCI. These models accounted for confounders identified from a pool of potential confounders based on a cutoff of 10% change-in-estimate criterion. The potential confounders considered in all models used to assess group differences in gesture type and function included race, ethnicity, level of maternal education, sex, age, and NVDQ. Linear regressions were also used to examine the mean difference in deictic and conventional gesture use (total, behavior regulation, and joint attention) between the CSBS and PCI, controlling for the confounders chosen by the 10% criterion. Cohen's d was used as a measure of effect size, calculated with pooled SD, using least square estimated values from the general linear model. Values of d = .20, .50, .80, represent a small, medium, and large effect, respectively.
Generalized linear models were then conducted to characterize the association between 18-month gesture use (deictic and conventional) in the CSBS and PCI and (1) language at 36 months (MSEL receptive and expressive age equivalents and CDI words produced), as well as (2) change in language from 18 to 36 months (change in MSEL receptive and expressive age equivalents and change in CDI words produced). Each model controlled for confounders identified by the 10% criterion described above, with the following potential confounders considered in all association models: race, ethnicity, level of maternal education, sex, age, NVDQ, VDQ, and CDI words produced. In addition, the effects of communicative function were examined in the linear regression models. Group was forced in all models to control for the impact of group on the association between gesture use and language development.
The analyses were completed in R version 3.4.4 (2018-03-15) with the statistical significance set at p < 0.05.
Results
Differences in gesture use in two contexts
Group differences in frequency of deictic and conventional gesture use (total, behavior regulation, and joint attention) in the CSBS and PCI.

Note: LD: language delay; ASD: autism spectrum disorder; TD: typical development; CSBS: Communication Symbolic Behavior Scales Developmental Profile–Behavior Sample; PCI: Parent Child Interaction.
Confounders identified and accounted for included age and nonverbal developmental quotient (NVDQ) in the CSBS, and NVDQ in the PCI.
The post hoc column indicates significant group differences. Groups are presented in order of means from lowest to highest. The arrows indicate the direction of the difference. Groups separated by commas are not significantly different.
In the CSBS, compared to toddlers with TD, toddlers with LD (both LD–ASD and LD–NonASD) produced significantly fewer deictic gestures in total and for joint attention, and toddlers in the LD–ASD group produced significantly fewer deictic gestures for behavior regulation. Within the LD group, toddlers with LD–ASD used significantly fewer deictic gestures in total, and for behavior regulation and joint attention than the LD–NonASD group. Toddlers with LD–ASD and LD–NonASD produced significantly fewer total conventional gestures than those with TD. Effect sizes associated with group differences for the LD groups in the CSBS were medium to large for deictic gesture use and small for differences in conventional gesture use.
In the PCI, toddlers in the LD–ASD group produced significantly fewer total deictic gestures than those with TD, and fewer deictic gestures for joint attention than both the TD and LD-NonASD groups. No significant group differences were found for deictic gestures used for behavior regulation in the PCI. Toddlers in both LD groups produced significantly fewer total conventional gestures than those with TD, and toddlers in the LD-NonASD group used significantly fewer conventional gestures for behavior regulation and joint attention compared to toddlers in the TD group. Effect sizes associated with group differences for the LD groups in the PCI were small to medium.
Based on the different patterns of group differences observed between the CSBS and PCI, we further investigated the mean difference in the number of deictic and conventional gestures (total, behavior regulation, and joint attention) between the CSBS and PCI among the three groups (mean difference = CSBS − PCI). Results indicated significant differences for deictic gestures used for both behavior regulation and joint attention, with the largest mean differences in the TD group (see Figure 1 for details). Model estimates, associated confidence intervals, and effect sizes are presented in Supplementary Table 1 in Supplemental Material.
Frequency of deictic (left) and conventional (right) gesture use in the Communication Symbolic Behavior Scales Developmental Profile–Behavior Sample (CSBS; red) and Parent–Child Interaction (PCI; blue) for the three groups of toddlers. In the boxplots, the three horizontal lines of the boxes represent 25%, 50% (median), and 75% quantile and circles indicate outliers. The mean difference (CSBS–PCI) in gesture use between the CSBS and PCI was significantly higher in toddlers with TD than LD (both with and without ASD outcomes) for total deictic gestures and deictic gestures used for joint attention. The mean difference in gestures between contexts was also higher for the TD group than the LD-ASD group for deictic gestures used for behavior regulation. There was no significant mean difference between the CSBS and PCI for any groups in conventional gesture use. The difference in sample lengths between the CSBS and PCI did not account for the group differences in gesture use patterns between contexts.
Association between 18-month gesture use and language development
Association between 18-month gesture use in the CSBS and PCI and the development of language by 36 months.
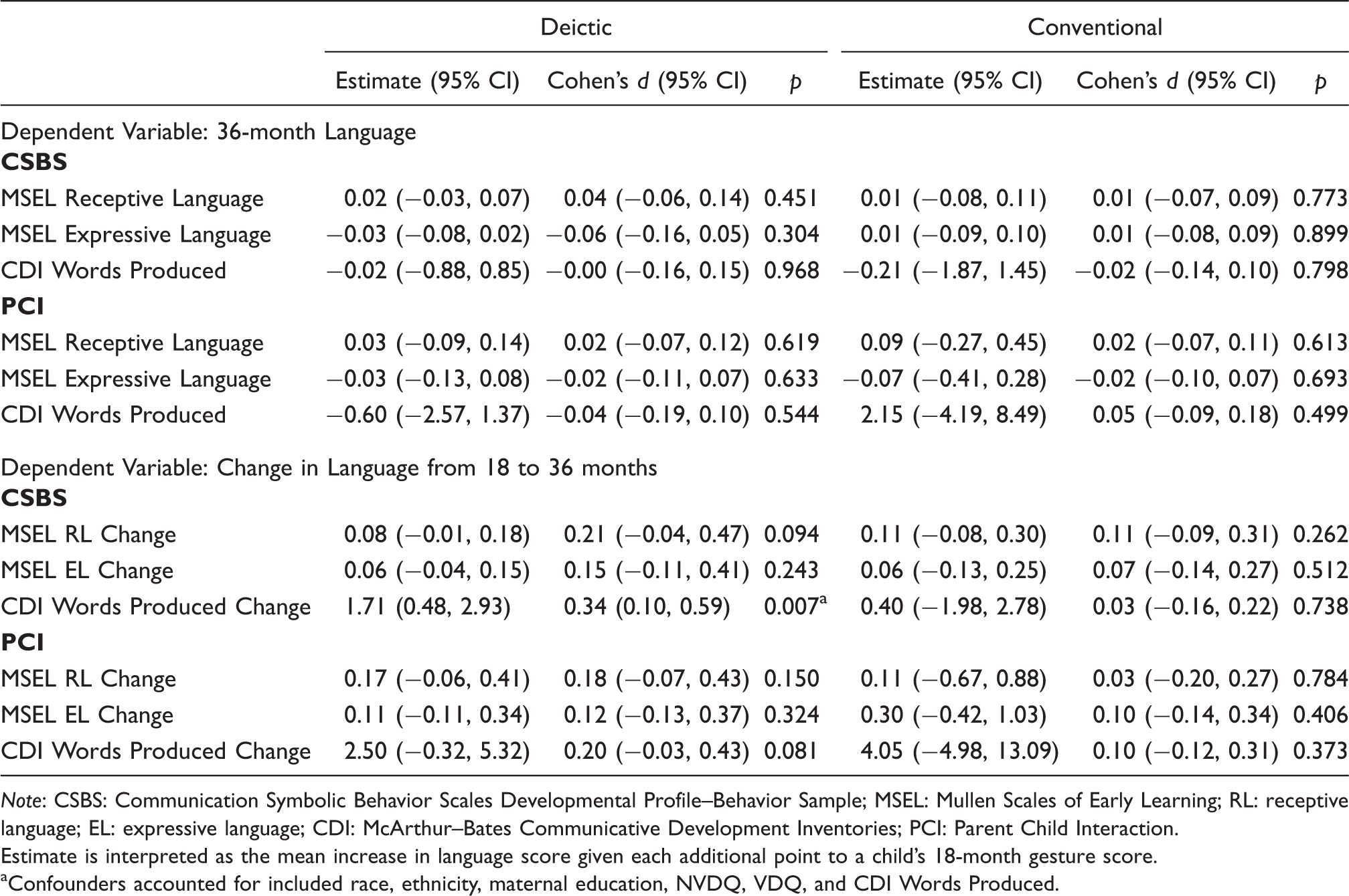
Note: CSBS: Communication Symbolic Behavior Scales Developmental Profile–Behavior Sample; MSEL: Mullen Scales of Early Learning; RL: receptive language; EL: expressive language; CDI: McArthur–Bates Communicative Development Inventories; PCI: Parent Child Interaction.
Estimate is interpreted as the mean increase in language score given each additional point to a child's 18-month gesture score.
Confounders accounted for included race, ethnicity, maternal education, NVDQ, VDQ, and CDI Words Produced.
Discussion
The purpose of this study was to compare two gesture types and two functions in a sample of toddlers with significant early receptive and expressive LD, with and without ASD diagnosed by 36 months, including a typically developing control group. We examined associations between gesture type and function at 18 months to language outcomes at 36 months. Gesture use was observed in two contexts—a naturalistic PCI as well as a more structured standardized assessment designed to provide communication opportunities (CSBS). This study was designed to build on the work of Ozcaliskan and colleagues (2016), extending previous research by comparing gesture use across two observational contexts, and including both receptive and expressive language outcomes in toddlers.
Gesture deficits in toddlers with LD across contexts
As expected, toddlers with ASD outcomes demonstrated significant deficits in gesture use, with these differences found across gesture types, communicative functions, and observational contexts (Dimitrova, Ozcaliskan, & Adamson, 2016; Ozcaliskan, Adamson, & Dimitrova, 2016; Shumway & Wetherby, 2009; Wetherby, Watt, Morgan, & Shumway, 2007; Winder et al., 2013). In contrast to toddlers with ASD, less is known about gesture differences in toddlers with early LD without ASD. We found reduced deictic and conventional gesture use in toddlers with early LD without ASD outcomes, although there was variability in relation to communicative function and measurement context. These findings of gesture deficits in our sample of toddlers with both expressive and receptive LD (without ASD outcomes) support indications that delays in receptive language increase the risk for reduced gesture use (Ellis & Thal, 2008; O'Neill & Chiat, 2015; Thal & Tobias, 1992; Thal et al., 1991).
In addition, toddlers diagnosed with ASD (LD–ASD) by 36 months showed a particular and more pronounced deficit in deictic gestures at 18 months compared to those without ASD outcomes (LD–NonASD). Thus, while toddlers with early LD, regardless of ASD outcome, showed some reduced gesture use at 18 months compared to toddlers with TD, an ASD diagnosis was associated with greater deictic gesture deficits. This finding was based on an analysis that controlled for nonverbal cognitive development, adding to previous work that found differences in deictic gesture use in young chidlren with ASD cannnot be accounted for by LD alone (Ozcaliskan, Adamson, & Dimitrova, 2016). This is an important finding given that a majority of children (66.7%) in the LD–ASD group demonstrated delays in nonverbal cognition along with their LD, and previous research has found a strong relationship between gesture use and nonverbal cognitive ability (Luyster, Kadlec, Carter, & Tager-Flusberg, 2008; Manwaring, Mead, Swineford, & Thurm, 2017; Wetherby et al., 2007).
In relation to gesture use across the two contexts (CSBS and PCI), we found that even when accounting for sample length differences, toddlers produced more of both types of gestures in the CSBS. Fewer gestures were used in the PCI, and the PCI was also less sensitive to group differences, particularly for deictic gestures in toddlers with early LD. While this increased gesturing in the CSBS is not surprising, given that it is a measure specifically designed to elicit prelinguistic communication through the use of communicative temptations, findings do suggest that such a semi-structured, standardized, and examiner-led context may be particularly helpful in capturing diagnostically relevant differences in gesture use in toddlers with early LD.
To further our understanding of gesture production across the two contexts, we calculated the mean difference in gesture use (types and functions) across contexts for each child and found that at a group level, the mean difference in deictic gestures (CSBS - PCI) varied across groups. Specifically, the difference between contexts in total deictic gesture use was smaller in toddlers with early LD (with and without ASD outcomes) than in the TD group, and significantly smaller in toddlers with ASD for deictic gestures used for both behavior regulation and joint attention. Conventional gestures did not seem to be as impacted by sampling context as deictic gestures.
Several factors may explain why toddlers with early LD show more similar gesture use across contexts than toddlers with TD. Previous research indicates that toddlers with delays in both receptive and expressive language generally show reduced compensation through gestures for their LD (Thal & Tobias, 1992), and this may be true even when the sampling context includes scaffolding to elicit communicative behaviors such as gestures. Deictic gesture use across communicative functions appears to differentiate toddlers with LD with and without ASD outcomes; toddlers later diagnosed with ASD use deictic gestures for joint attention significantly less regardless of context. This finding is unsurprising, as an impairment in joint attention is diagnostic of ASD (Bruinsma, Koegel, & Koegel, 2004) and deficits in gesture use specifically for joint attention have been previously documented in toddlers with ASD (Watson et al., 2013). In sum, sampling procedures appear to have a greater effect on toddlers with TD than those with early LD, particularly those with ASD outcomes.
Relationship between gesture and language development
There is a robust correlation between gesture use and the development of language, with research now indicating the relationship between gesture and language may vary depending on gesture type (e.g., deictic vs. conventional) and the presence or type of developmental delay (Ozcaliskan, Adamson, & Dimitrova, 2016; Ozcaliskan, Adamson, Dimitrova, et al., 2016), the communicative intention of the gestures (Colonnesi et al., 2010), and whether the linguistic focus is comprehension or production (Thal, Marchman, & Tomblin, 2013). We aimed to extend findings of recent research suggesting that deictic gestures are particularly important in facilitating the development of language in toddlers with ASD (Ozcaliskan, Adamson, & Dimitrova, 2016). Consistent with our hypothesis, we found that deictic but not conventional gesture use at 18 months was significantly associated with expressive language, specifically the change in expressive vocabulary from 18 to 36 months, but not expressive or receptive language age equivalents on the MSEL after controlling for important confounders including verbal development at 18 months.
The finding of a significant association between gestures and expressive vocabulary on the CDI but not language scores on the MSEL may be related to several factors, such as differences in the measures themselves or differences in the constructs they measure. For example, the MSEL is a more comprehensive and observational measure of language, whereas the CDI measures expressive vocabulary based on parent report. In addition, deictic gestures may more specifically help directly build spoken vocabulary compared to other expressive language skills. Although Ozcaliskan and colleagues (2016) did not examine the correlation between deictic gestures and a broad measure of language, their finding of a correlation between deictic gestures and expressive vocabulary a year later is consistent with the present findings. Overall, our findings provide additional evidence for deictic gestures playing a unique role in the development of language. Children's early deictic gestures may facilitate language through eliciting input and spoken language from adults (Dimitrova et al., 2016), as well as other means such as reducing the child's cognitive load (see Ozcaliskan, Adamson, & Dimitrova, 2016, for discussion).
We did find that 18-month gestures in the CSBS (but not the PCI) were significantly associated with the development of language. However, the pattern or trends of associations are similar across contexts, and the statistical difference in findings across the two contexts is likely related to the reduced gesturing and thus reduced variability in the PCI. The association between gesture and expressive language was not moderated by group or by communicative function, and importantly, remained after controlling for critical demographic and developmental confounders.
Strengths and limitations
This study included several strengths. First, we examined gesture use in an understudied population of toddlers with significant receptive and expressive LD at 18 months, and followed the sample to 36 months of age to examine ASD outcomes. The majority of research on gesture use in toddlers later diagnosed with ASD has relied on samples of infants at heightened genetic risk based on having an older sibling with the disorder (e.g., Iverson et al., 2018; Leezenbaum, Campbell, Butler, & Iverson, 2014; Mitchell et al., 2006; Winder et al., 2013), and findings from these studies may not generalize to other at-risk populations. An additional strength of this study is the examination and comparison of gesture use across observational contexts, as well as examining both gesture type as well as function, providing a more comprehensive profile of gesture use. Much of the previous literature examining gesture use in toddlers has only used parent report (e.g., Mitchell et al., 2006) and has not combined the examination of both gesture type and function.
Limitations included the small sample size, particularly in the LD–ASD group, which could have affected the power to detect group differences and associations. Future research with a larger sample size is needed. In addition, we only followed the sample to 36 months, limiting understanding of long-term outcomes in the sample. Given the risk of experiencing less than optimal outcomes into the school-age years (e.g., Capone Singleton, 2018; Reilly et al., 2010), following the sample and conducting evaluations beyond 36 months would provide important information about language and other outcomes of toddlers with significant early LD.
Conclusions and implications
This study found that toddlers with early delays in language, regardless of ASD outcome, showed reduced deictic and conventional gesture use compared to toddlers with TD, and that deictic gestures in particular support the development of spoken language. Reduced gesture use in the toddler years has the potential to influence the development of language in several important ways, with a lack of compensation through gesture for LD increasing a child's likelihood of exhibiting persistent LD (Thal & Tobias, 1992). Deictic gestures provide toddlers a way to refer to objects and events as they are developing spoken language, and provide caregivers an opportunity to contingently respond to and translate the child's gesture into words (Dimitrova et al., 2016). These bidirectional influences between parents and their children help scaffold the development of language (LeBarton & Iverson, 2017).
Findings from this study have implications for the assessment and treatment of children with early LD who are at increased risk for outcomes such as ASD and other neurodevelopmental disorders. First, assessment should include evaluation of both the types of gestures a child uses as well as the communicative function or purpose of their use, with a more structured measure providing more opportunities for gesture production. In designing and implementing treatment plans for toddlers with significant LD, it is critical to consider foundational prelinguistic communication skills, which develop prior to and are predictive of spoken language. A specific focus of treatment in toddlers with delays in language should be on increasing gestural communication, particularly deictic gestures used for behavior regulation and joint attention, with the goal of facilitating the development of later language. Some interventions for toddlers with LD emphasize building gesture use and other prelinguistic and social cognitive skills (e.g., Fey et al., 2006; Peters-Scheffer, Huskens, Didden, & van der Meer, 2016; Wetherby et al., 2014). Given that early deictic gesture use affects the rate of growth in spoken vocabulary, interventions targeting gesture use may benefit from a specific and early focus on increasing deictic gestures as well as directly measuring changes in a child's use of these gestures.
Supplemental Material
Supplemental material for The gesture–language association over time in toddlers with and without language delays
Supplemental Material for The gesture–language association over time in toddlers with and without language delays by Stacy S Manwaring Department of Communication Sciences and Disorders, University of Utah, Salt Lake City, UT, USA Lauren Swineford Washington State University Health Sciences, Spokane, WA, USA Danielle L Mead San Jose State University, San Jose, CA, USA Chih-Ching Yeh, Yue Zhang Division of Epidemiology, Department of Internal Medicine, University of Utah, Salt Lake City, UT, USA Audrey Thurm in Autism & Developmental Language Impairments
Footnotes
Acknowledgments
We would like to thank the children and their families who participated in this research, as well as the research staff who contributed to the coding of gestures and collection of data.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was supported by the Intramural Program of the National Institute of Mental Health of the National Institutes of Health, ZIA MH002868, (Study NCT01339767, 11-M-0144), as well as the University of Utah Study Design and Biostatistics Center, with funding in part from the National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health, through Grant 8UL1TR000105 (formerly UL1RR025764).
Supplemental Material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.