
Abstract
Background
Health-Technology-Engineering (HTE) is an interprofessional PhD/MD educational program. All students take the medical school course Introduction to Clinical Medicine (ICM)in order to learn communication, clinical skills, and identify healthcare challenges that could be solved with technologic innovation. This study sought to evaluate HTE-ICM by understanding perceptions between participating disciplines.
Methods
One author (not part of HTE-ICM) conducted five focus groups; interviews were professionally transcribed. Questions were designed to explore motivation, course satisfaction/challenges, and success measures. Transcripts were reviewed separately by two authors and analyzed using grounded theory.
Results
21/63 eligible students (33.3%; 18 MD, 3 PhD) and 9/35 faculty members (26%; 7 HTE, 2 ICM) participated in focus groups. Students were 80.9% male, had an average age of 24.4 years, and 30% self-identified as White/Caucasian. Themes shared by all participants included motivation to collaborate, , satisfaction that the course “opened a window” providing exposure to another profession, and that a success measure is building long-lasting partnerships. Time constraints were the major challenge identified. Additional themes were unique to certain subgroups. Identified opportunities for improvement included (1) peer-mentoring (2) faculty development (3) adjusting student expectations (4) better use of patient encounters to identify problems with engineering solutions.
Conclusions
Qualitative analysis of HTE-ICM identified benefits and opportunities for improvement that can enhance the local experience and guide development of similar programs.
Introduction
The Health-Technology-Engineering (HTE) program at the University of Southern California (USC) was launched in 2011 as a voluntary graduate-level training program for students of both the Keck School of Medicine and Viterbi School of Engineering to learn to collaborate and solve clinical problems by developing medical technologies. 1 The three main curricular elements are a longitudinal team research project, a speaker series featuring experts in innovation and design, and the required medical school course Introduction to Clinical Medicine (ICM). Both MD and PHD-student HTE participants are expected to use ICM to learn communication and clinical exam skills, foster empathy, and identify healthcare challenges by interacting with real patients and a MD faculty mentor in a small group setting. Although an annual evaluation of HTE is administered to participants, it does not specifically address the ICM component, which may offer unique challenges to involved stakeholders.
Nationwide, similar programs have existed since as far back as 1971, when Harvard and the Massachusetts Institute of Technology formed Health Sciences and Technology (HST). 2 However, a lack of a formalized curriculum and high variability between academic centers in facilities, faculty, and research funding make comparisons between such programs’ curriculum and educational successes challenging. For instance, the HST program provides “intense clinical training” to PHD participants, but two published surveys of program graduates focus mainly on ultimate academic successes of participants and not on communication skills or quality of the patient-focused components of training.3,4 Overall, student demand to participate in programs like HST and HTE appears to be increasing. In one example, students without such a local program banded together to form their own student-run biotechnology mentoring incubator (Sling Health, formerly IDEA Labs) that as of 2017 has expanded to six other academic sites. 5 With so many students seeking out specialized medical-engineering experiences in addition to the demands of their primary academic training, we felt that an in-depth evaluation of the HTE program at USC could both improve our local experience and inform national practices.
Therefore, we designed a qualitative study to explore course alignment with the motivations, satisfaction, and goals of all HTE-ICM participants. We included faculty as well as students to provide a comprehensive assessment and thorough evaluation of the existing course experience at all levels. We aimed to use our findings as idea generation to inform future improvements such as faculty development or curriculum redesign.
Methods
Study Design
We conducted a qualitative descriptive study using focus group interviews in order to allow participants to build on or refute each other’s thoughts. All study procedures were approved by the USC IRB (HS-16-00766).
Inclusion, Exclusion
Any student or faculty who was a prior or current participant in the HTE-ICM program was eligible for inclusion. Participants less than 18 years of age were excluded, but this was not applicable to the population. In addition, 2 authors of this study because (M.T. & D.A.) would have been eligible as prior instructors but they were excluded from participation due to their study role.
Subject Recruitment and Enrollment
Student subjects were recruited via email from the pool of HTE-ICM participants since program inception (n=63) on a voluntary basis; participation of students was encouraged by providing food. HTE faculty consisted of instructors who did
Place, Period of Study
Focus groups occurred on the USC campus in a conference room or by web-conference to allow more flexibility in scheduling. Each focus group lasted approximately 1 hour and all focus groups were completed over a 6 month time span.
Study Procedures
Interviews were led by one female author who is not a member of HTE-ICM (A.V.), who holds a PhD in social research methodology. Interview questions centered on themes of motivation, course experience, goals, and specifically addressed if those differed between MD and PhD students [see Supplemental Table 1]. Questions were designed to elucidate the true experience of HTE-ICM, rather than as it was intended or presumed to function. The interview guide included prompts and questions were pilot tested by the authors. Interviews were audio recorded, professionally transcribed (https://www.Rev.com), and transcripts were coded with the aid of computer software (Dedoose). Field notes were recorded by the interviewer and added to the data set.
Qualitative Statistical Analysis
Two authors (M.T. & D.A.) separately reviewed transcripts using grounded theory to identify themes and codes through an iterative process, with three successive rounds of coding. The first two rounds of initial, focused, and theoretical coding created the codebook and the coders met to discuss themes. In the third round, discrepancies were resolved with the additional two authors (G.T and G. H.) into the final codes and themes. The research paradigm was rooted in objectivity, to identify emerging theories that fit to explain the HTE-ICM experience.
Methods to Enhance Trustworthiness
Thematic saturation was enhanced by conducting additional focus groups (ultimately 5 total sessions occurred; 2 student, 3 faculty) and by member checking. At least 1 PhD student participated in each student group; 1 faculty group contained only HTE instructors.
Study Guidelines
The reporting of this study conforms to the COREQ guidelines 6 [See Supplemental Table 2].
Results
Demographics
Student Demographics
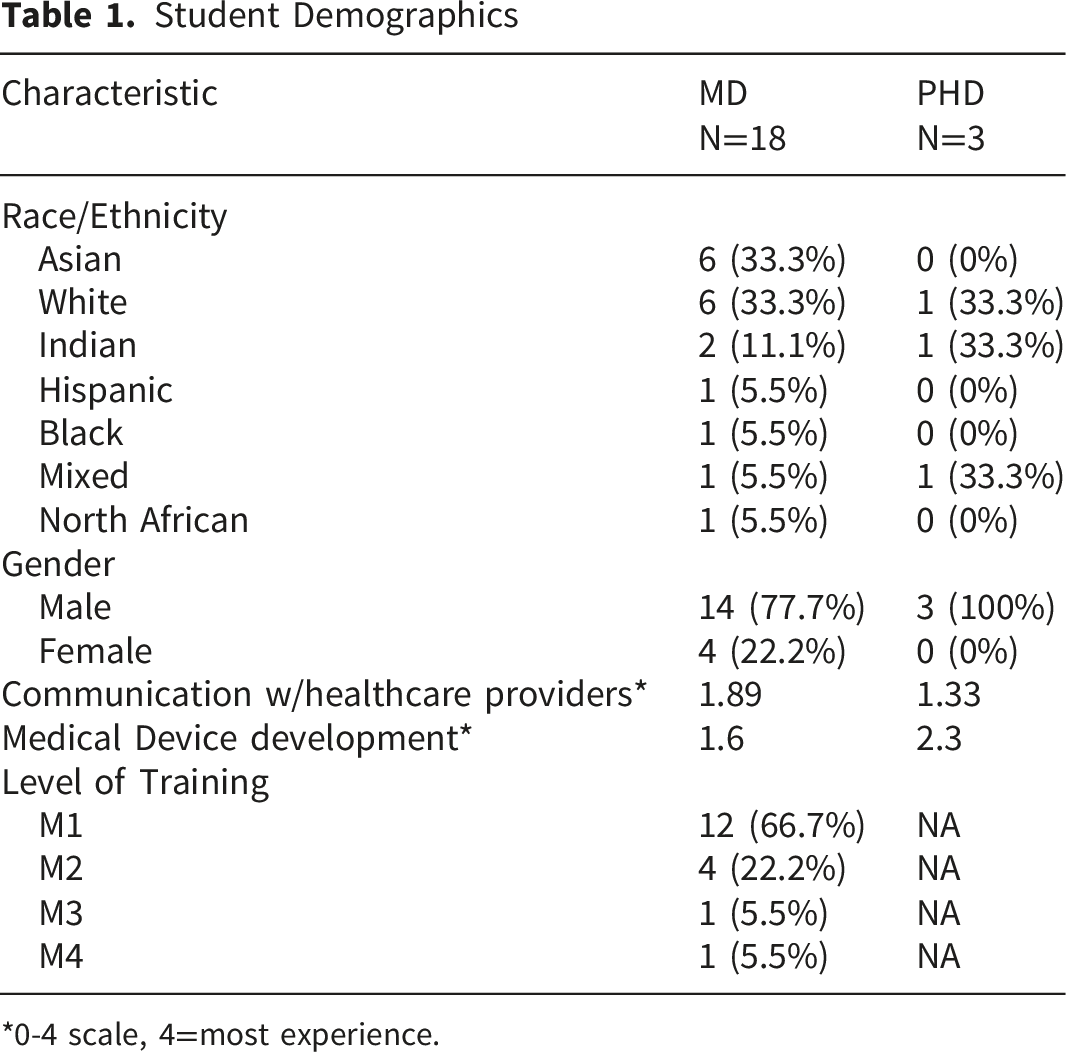
*0-4 scale, 4=most experience.
Motivation
We identified key motivating factors for participation in HTE-ICM that were either primarily endorsed by one group or shared between multiple groups (see Figure 1). Motivating factors for HTE-ICM participation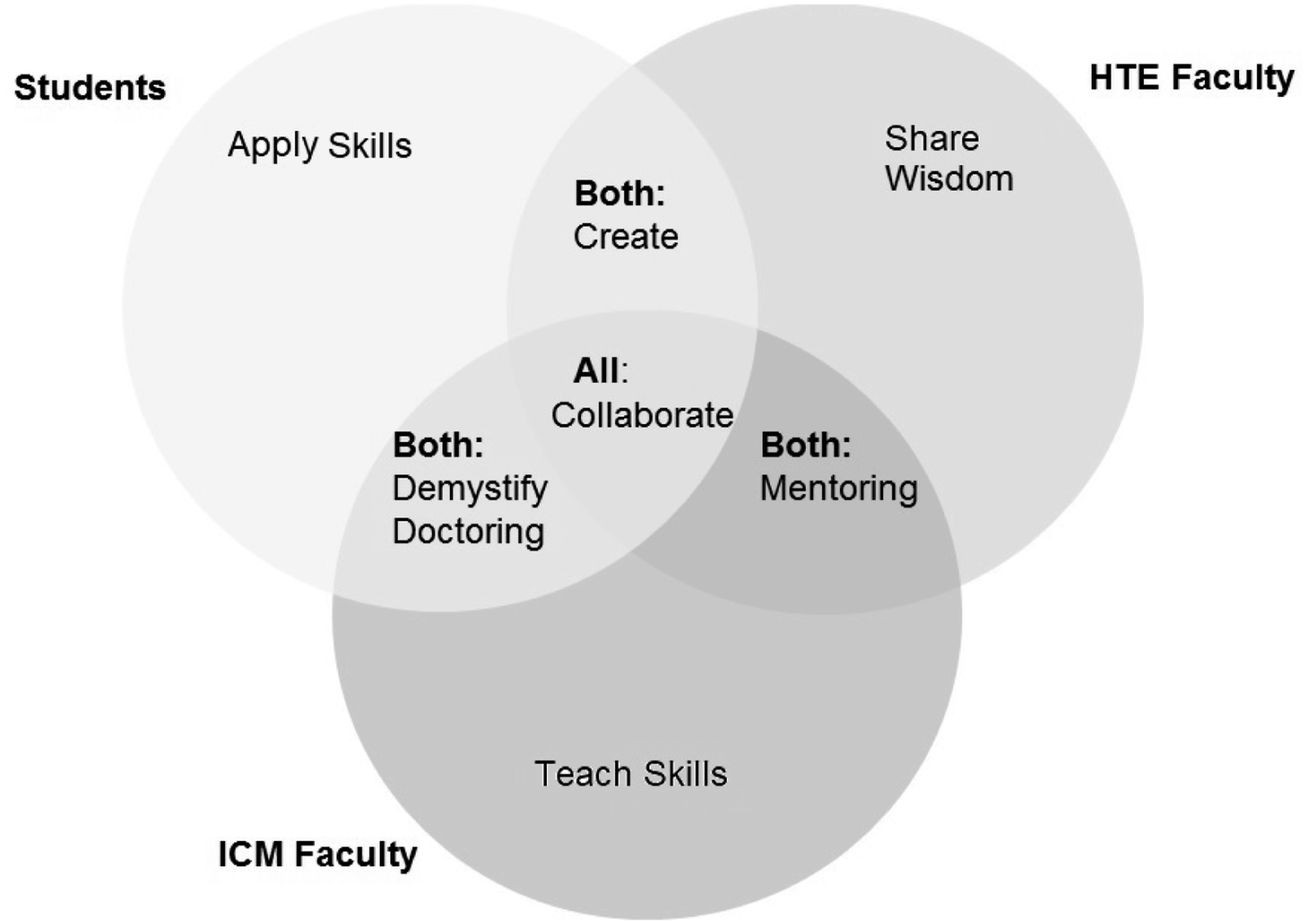
• MD Student: “…to stay in touch with aspects of curriculum and academics that I had in undergrad so having an economics background for example I wanted to try to apply that in a new environment and basically see what was possible outside of the classroom.”
A motivating factor that students shared with their HTE faculty was the desire to create (or learn to eventually create) medical-technology products. • PhD Student: “…so you have both the medical access and then engineering talent being present for the ultimate project and goal of the course, which is…your device.” • HTE Faculty: “…bringing together the folks who can build solutions and…the folks who and help articulate the problems, and…construct a business opportunity out of that to actually improve healthcare.”
On the clinical side, since ICM is often the first experience medical students have interacting with patients in real clinical settings, the motivation for student and clinical faculty participation was to “demystify doctoring” and explore what physicians do and how they practice their craft. • PhD Student: “I think there's a lot of, I guess, misunderstanding about medicine, especially if you haven't experienced it yourself. I guess it's kind of a way for PHD's to at least have some idea of what it's like.” • ICM Faculty: “allowing the PhD students, from the engineering perspective, to interact with real patients, to get a sense of what's happening with the patients. And then also to see what's involved in the daily workflow of a physician. So they not only get to see what their medical student colleagues are doing, but also what do physicians...how do nurses interact? By having exposure directly to kind of hands-on clinical care, the engineers are...they have this exposure to where patients are being taken care of and they can see all of the technological issues and kind of have more of a real clinical experience”
• HTE faculty: “Because I…ran a private practice, I could bring that experience to share with the students in terms of how decision making occurs on a physician’s part to use a product or not.” • ICM faculty: “…[students] may need a little bit of refocusing to remember that what they’re learning in ICM is…for clinical care and doctor/patient relationship, and I think that’s probably the job and focus of the instructors, and particularly the instructors who choose to teach HTE. So maybe not get off on the tangent of ‘Oh, this is all just to help me create a new product or something bioengineering”
• MD Student: “…so we could learn early what it’s like to collaborate with people who have different educational backgrounds. I think because we’re all young and we’re all fairly close to the beginning of a graduate experience that it should be easy or seamless but it turns out that we have a lot of differences” • HTE faculty: “bringing the two disciplines together and really teaching them how to work together, because neither one of them in their respective disciplines are taught very strong collaboration skills” • ICM faculty: “I don’t have that engineering background, it makes me wonder, ‘Wow, I wonder what somebody else who has a technological background would say [about this clinical experience]…would they totally geek out and have this higher level conversation about what they could innovate from here?’”.
Strengths
When queried about HTE-ICM course experience, respondents endorsed several core strengths of the program, although different groups often identified different positive aspects (see Figure 2). Strengths of HTE-ICM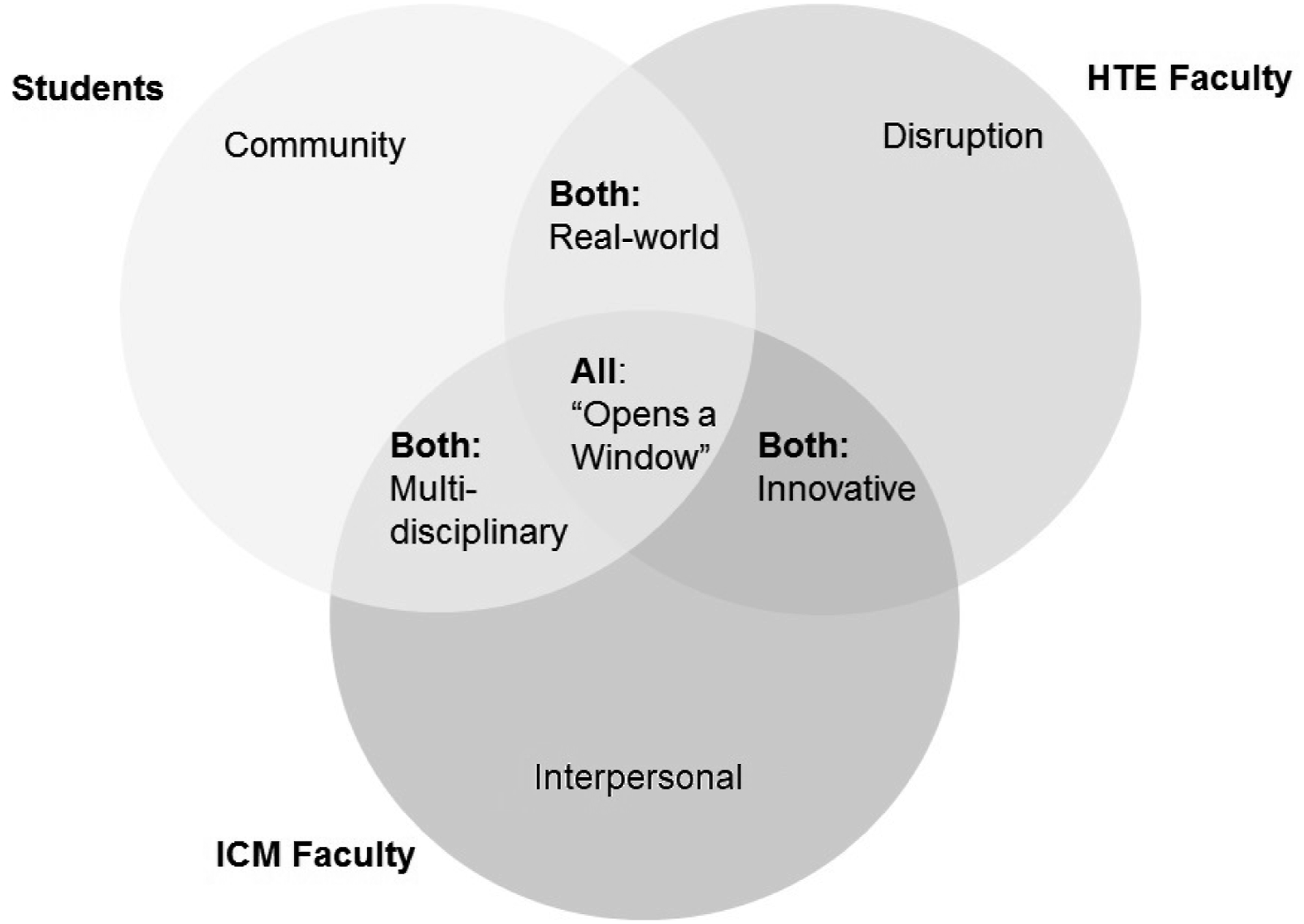
• MD Student: “not every team’s successful and there’s a lot of frustration between teams, but…we are all pretty fine in ICM, versus some other ICMs that are very dysfunctional. I think it’s because of the increased number of interactions we have.” PhD Student: “Yeah, it brings us together.”
However, one student did note that they sometimes felt confined by the close-knit community when it came to working on longitudinal projects and research: • MD Student: “What if…I had somebody in undergrad that I’m thinking about doing something with or I have other connections….I don’t want the journey to necessarily be alone, I like the community that HTE creates, I just don’t think necessarily it has to be where I’m definitely going to work with somebody in HTE.”
Both students and ICM faculty generally felt the multi-disciplinary nature of the course was a strength of the ICM experience, but (as later described) it could also be a challenge. The positive aspects largely centered around getting to see different styles of approaching the same problems, as well as unexpected ideas that may spring from encountered clinical scenarios. • MD Faculty: “Yeah and someone else was talking about a pacemaker, and there was a lot of discussion about the pacemaker…‘How big is the pacemaker? And how long is the battery life? And how does it get designed?’ And so there was this whole focus that I felt like, this is probably a more advanced discussion or a different discussion that many other groups would have about a pacemaker”
Students and their HTE faculty praised the aspects of the course that were less academic and more “real-world” which included both interacting with industry experts or the actual hands-on work of trying to develop their own ideas and products. • MD Student: “I think from my perspective the most valuable thing that we’ve learned is experiences like where we can come and meet with people in industry or we had someone from [a business] come and talk to us” • PhD Student: “the most learning is coming from the trial and error, it’s coming from the actually doing”
• MD Faculty: “I enjoyed being able to take the discussion to the next level…whether it’s related to patients and how to interact with patients, to even talking about ‘What did you notice from a project potential?’…So they’re always thinking from an innovative perspective, and that was refreshing.” • HTE Faculty: “The health tech space is changing so rapidly these days that it’s mind boggling to people in the industry…Now as a school, if you’re just looking at the curriculum to be able to help students reach that transition, I think it’s going to be extremely hard. If you have a set of external people come in…[that’s] wonderful to insert the knowledge and the perspective from a practical world into the academic exercise.”
Clinical faculty were the only group to show appreciation for how the course provides training in developing interpersonal skills, and that ICM instructors really focus on communication skills and empathy when part of HTE-ICM. • ICM Faculty: “I think probably in HTE we’re skewed. There's probably a higher likelihood that there's going to be more difficulty with the patient/physician interaction, but I think that because it's already somewhat known that engineers may have more difficulty, or medical students with a heavy engineering interest or background, that maybe the instructors focus on that.”
• PhD Student: “[Without HTE-ICM] I think the PhD students, or anyone that’s outside of medical school, would have a much harder time accessing the things that medical students have access to, or even seeing the world of the medical student” “I’m taking the ICM course…we share that in common…I get to see a window into the other things that medical students are doing. There are research opportunities for medical students to see what PhD students are doing. It’s really a very good split in the middle.” • HTE Faculty: “Increasingly, our students in biomedical engineering have essentially no contact with disease or hospitals [since] the day they were born…That lack of experience makes it extremely difficult for them to have any instincts for our technology. It actually gets used in healthcare, which is essential for product design.” “Yeah, absolutely I would second that. I think I'd also, just to build on that, I think understanding the culture and the thought process, both of those groups, it's critical for each other. In a sense, it’s a bit like musicians and instrument makers understanding each other’s craft and ultimately things blow out better when that happens.” • MD Student: “I mean multidisciplinary teams, it’s not about me becoming a chemical engineer and being able to do their work, it’s about me being able to see their strengths and weaknesses, work with them, respect them…so I just need a glimpse into their life, a glimpse to what they bring to the team and to know what I can go to them for. And then we’re on the same page. But I don’t need to learn their craft. So it’s like, that’s where ICM is a little bit weird.”
Success Measures
When prompted to discuss how success of this course could be measured, a variety of different themes were identified (Figure 3). Measuring success of HTE-ICM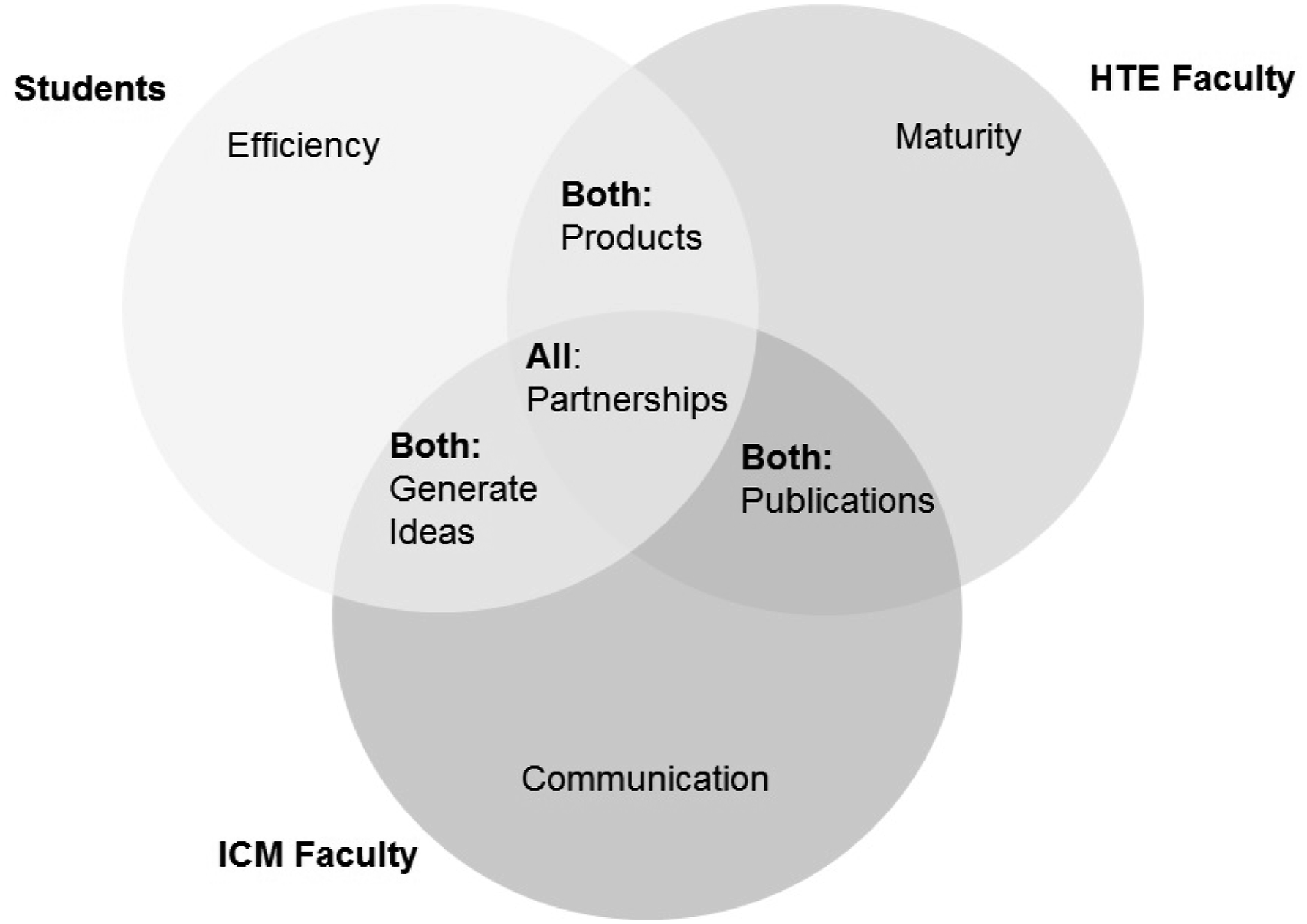
• MD Student: “I think simply, if you just asked us at the end of the program, ‘Do you feel like your time was used wisely or wasted?’ I think that's successful.” • HTE faculty: For me, that's a leading metric to say how many companies have come out of this program. What are the exits? How many of them got bought out by a bigger company?
• HTE faculty: “Well, maybe… just like a complete business case for why their project or venture should go forward. Why does it make sense? To be able to hit sort of all the major points and to have an appreciation of what it would take to make this thing a commercial success and not to have gaping holes in their presentation.” • ICM Faculty: “to feel like they're also getting something from engaging in a conversation with engineering students…as they're interviewing patients so that they can actually take the discussions to the next level.”
• ICM Faculty: “Do they feel like they now have the network of graduates they could draw upon, do they have instructors that they've met, that they have the connection to USC going forward that they...for future business or innovation they may reach back to.… has there been kind of a creation of an alumni feeling around HTE?”
Challenges and Solutions
Challenges and Proposed Solutions
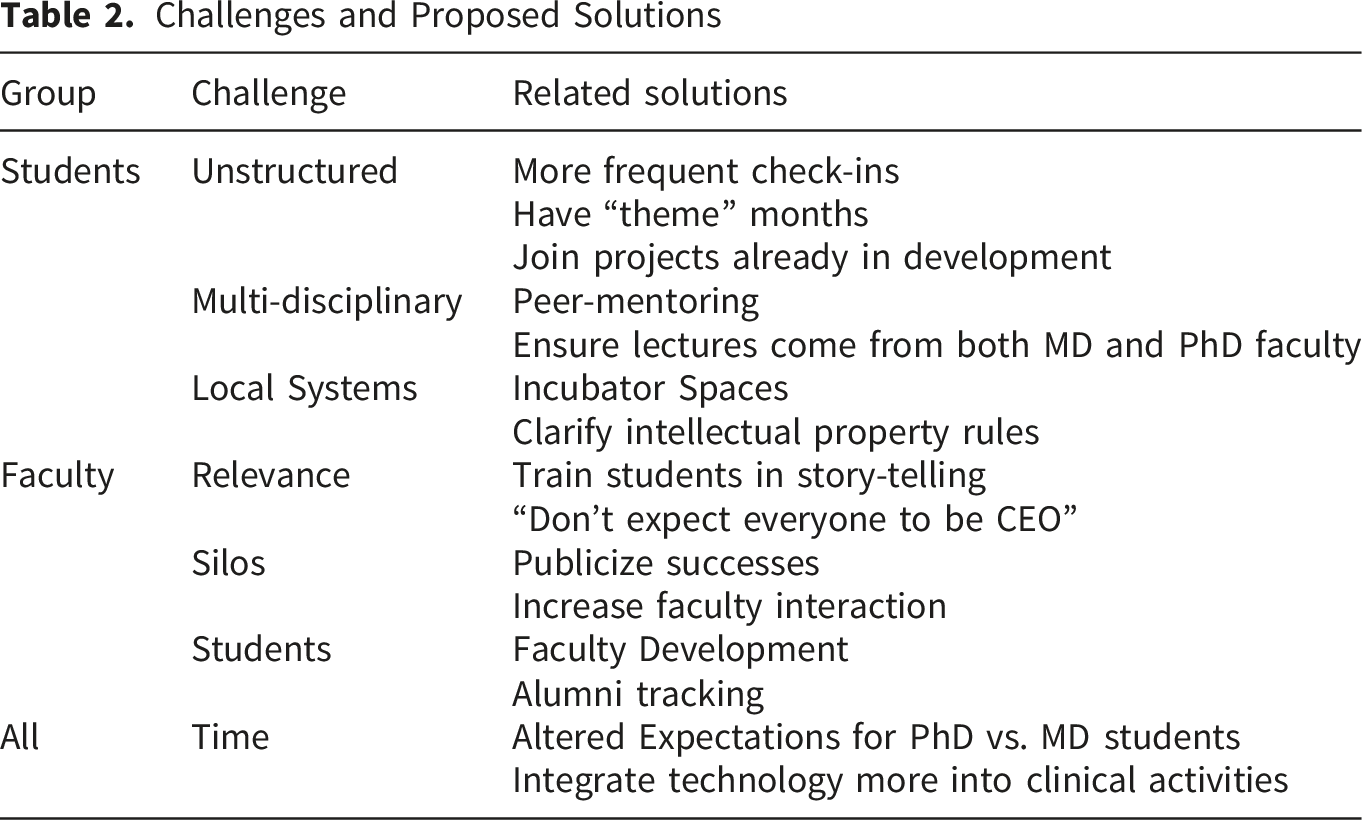
• MD Student: “we need a little more structure, but structure that lets us create, you know what I mean?”
Students liked collaborating and building community with multi-disciplinary colleagues, but also found that competing interests made the course confusing. • MD Student: “So I think the issue is...not everybody's on the same baseline. So then you have to dabble in a little bit of everything…if everybody’s an engineer, you already got your basics covered…needs finding would be a lot more efficient. But here, we have to do a lot of catching up, I feel like.”
Local systems issues were also identified, many around either the physical layout of campus and a lack of shared working space, or regulatory issues related to building products that could become companies within an educational institution.
• ICM Faculty: “…it would be nice to be able to engage the clinical faculty and make sure people...the faculty are involved in HTE and also have the opportunity to see what the students are doing on the other side, too outside of the clinical realm.”
• PhD Student: “I guess a key difference here is with a PhD it’s kind of flexible timeline…that flexibility allows you to do some of these classes outside of your own discipline.” • MD Student: “Prior to neuro block ICM was kind of this novel, unique thing. During the neuro block, it was just one of eight different things I had to do…it quickly turns from fun to more cumbersome.”
Faculty similarly were aware of the competing demands for student time and that although the specific tasks and deliverables were different, both MD and PhD students suffered because of it. This was exemplified by the following focus group discussion: • HTE faculty: “I’d say that probably the med students…it’s a greater challenge for them simply because the medical program is [a defined] length and probably a bit more intense whereas you’re a grad student or a ‘gradual’ student, you’ve got the option to stretch things out a little bit” • HTE Faculty: “I hope that’s true but there’s another unfortunate experience…which is that the PhD students are under so much pressure to focus on their thesis research and pressure from their advisors…they’re being discouraged from joining the program.” • HTE Faculty: “…I completely agree…Where does that maniacal focus come in and that sort of lack of a more holistic approach to the research? Clearly, having that…clinical exposure and that real-world exposure, you think would lead to better science and better insights in the long run.”
Interestingly, one participant’s response to this discussion was to put some of the blame for this phenomenon on faculty themselves: • HTE Faculty: “We had a similar history and challenge with PhD students….it was very clear that…they [faculty] were very protective of the students as being their employee essentially…also they are defensive because they’re maybe in a more basic role and they’re not really sure what this [HTE] is bringing value to the lab or whether they want somebody to bring value that they [faculty] don’t have. That could be a bit threatening to their leadership really.”
Conversely, a faculty participant in another focus group felt that students themselves could overcome the time constraints with self-motivation: • HTE Faculty: “I have the HTE student that is coming to mind that I actually work with. I mean she is stellar. She’s just often calling me saying, ‘Do you have anything more?’ So, I think it depends on the individual too.”
Almost all participants agreed on solutions, which would be to alter the schedule and utilize some of the clinical or lecture time more overtly to work on product ideas and development: • ICM Faculty: “I don’t know exactly how to do this, but one might be to revisit the schedule and make sure [it] really optimizes their participation in ICM and their participation in the HTE certificate stuff so there’s not a lot of competing interests time-wise.” • MD Student: “I was pitched this program like, ‘We’re going to create stuff. We’re going to do all this cool stuff.’ I don’t really know what we’re doing. Are we supposed to be working on projects on our own? It would be really cool if instead of having these presenters we have this class time to develop our ideas.”
Discussion
This qualitative focus-group exploration of an interprofessional education (IPE) program between medicine and engineering at one institution found that a clinical course (HTE-ICM) offered benefits such as “opening a window” between two different fields of study but challenges such as increased time demands on already busy schedules. A strength of the study is that it included insights from about one-third of the total eligible past and present students and faculty course participants. HTE-ICM is one of many such combined design-oriented medical educational programs that have been launched worldwide.5,7,8 While IPE is recommended 9 to cultivate collaboration in health professions and enhance patient care, no conclusive evidence exists that such collaborations are effective. 10 Although some themes identified are unique to this program, many can be applied broadly to help others in planning, development, modification, and evaluation of similar courses.
Participants were motivated to participate in HTE-ICM because they wanted to collaborate with people involved in other disciplines. However, clinical (ICM) faculty did not necessarily join the program because they wanted to build med-tech products or start companies, rather they wanted to show students the real world of being a doctor and teach communication and clinical skills. HTE faculty also joined the program to mentor but often envisioned becoming part of the students’ product development groups. It was interesting that no participants discussed financial reasons for joining the program, although securing funding or creating companies that were “bought out by a bigger company” were mentioned by a few participants as success measures.
All participants viewed strength of the course as an “exposure” program that shared elements of culture without requiring full integration (e.g. medical students were not planning to get a PhD). Therefore, requiring PhD students to join onto a regular medical student class (ICM) may give them too much time in the clinical setting – at first useful but as medical students learn medical jargon they too much surpass their PhD colleagues level of understanding and the class has diminishing returns. Whether immersion or exposure is more effective as a methodology for IPE remains subject to debate 11 and our study seems to support exposure. Many of the strengths of HTE-ICM would likely be maintained with shorter or more directed clinical exposures for PhD members. Similarly, the medical students may benefit from shorter health-technology-engineering experiences with clear goals and objectives, as opposed to expansive lectures from successful entrepreneurs that cover many topics.
Literature reviews of IPE programs have previously identified administrative support, programmatic infrastructure, experienced faculty, and acknowledgement of student efforts as key factors to assure success. 12 Our study supports these elements and suggests that if an IPE program includes engineering, it would also benefit from enhancing relevance and focusing teaching efforts on “real-world” applicable skills acquisition to make best use of time.
This study had several limitations. 80% of the student participants were male, which approximates the gender breakdown reported in other studies of similar programs. 13 However, viewpoints of why women would/wouldn’t be motivated to participate may be under-represented. As in any qualitative study, proposed solutions to identified challenges are limited to the perceptions of the participants and may not actually lead to improvement if implemented. Selection bias may be present as our sample was composed of those who responded to email solicitation, and we did not collect information about non-participants. In addition, this is a single center study and the wide variability in similar courses at other institutions may limit generalizability. After conclusion of this study but unrelated to the results, the HTE program was ended, although similar design-oriented courses and programs continue to be offered at USC.
Conclusion
Groups of student and faculty participants in a health-technology-engineering interprofessional education course that included a robust longitudinal clinical patient encounter experience identified strengths and opportunities for improvement. The general motivation for participation was to encourage collaboration. Challenges primarily centered around time constraints. Success measures aside from viable product production could be identified. This data may support the widespread value of such courses; limited exposure to core concepts of health-technology product design could be offered to all medical students and patient care experiences to more graduate students. Varying the required levels of immersion/exposure based on the student’s primary degree track could optimize cross-disciplinary IPE programs.
Supplemental Material
Supplemental material - Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation
Supplemental Material for Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation by Margaret Trost, Anne Vo, Denizhan Akan, Gregory Harlan and George Tolomiczenko in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation
Supplemental Material for Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation by Margaret Trost, Anne Vo, Denizhan Akan, Gregory Harlan and George Tolomiczenko in Journal of Medical Education and Curricular Development.
Supplemental Material
Supplemental material - Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation
Supplemental Material for Clinical Experience in a Medicine-Engineering Interprofessional Education Program: A Qualitative Evaluation by Margaret Trost, Anne Vo, Denizhan Akan, Gregory Harlan and George Tolomiczenko in Journal of Medical Education and Curricular Development.
Footnotes
Acknowledgement
We would like to acknowledge Nadine Afari for her assistance in coordinating the focus groups.
Ethical Considerations
Ethical approval to conduct this study was granted by the University of Southern California Health Sciences Campus Institutional Review Board (IRB) HS-16-00766.
Consent to Participate
The study was determined exempt from full consent, assent was obtained and an information sheet provided to participants.
Author Contributions
Dr. Trost co-conceived and conducted the study, analyzed the data, and wrote and edited the manuscript. Dr. Vo conducted the focus groups, collected and analyzed the data, and critically revised the manuscript. Dr. Akan co-conceived and conducted the study, analyzed the data, and critically revised the manuscript. Dr. Harlan contributed to the study design, provided project mentorship, and critically revised the manuscript. Dr. Tolomiczenko contributed to the study design, provided project mentorship, and critically revised the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.