
Abstract
Interprofessional collaboration (IPC) and interprofessional education (IPE) are two concepts that have gained interest during the last decade, for the positive change they enable, especially in clinical healthcare settings. Despite this surge of attention, there are few studies that systematically analyse interventions aiming at fostering IPC/IPE within clinical teams. Developing additional knowledge around factors that impact the efficiency of similarly targeted interventions can help improve the quality of patient care in clinical settings. To this end, the paper offers a systematic, realist review of the IPC/IPE interventions outlined in the literature, seeking to better understand how the context and mechanisms which shape these interventions interact to produce the desired outcomes (ie, improve IPC). Electronic databases searched were PubMed, PsycINFO, CINAHL and Web of Science. Seventeen articles met the inclusion criteria and were analysed independently by two reviewers following the RAMESES guidelines. The authors propose an explanatory model for the interventions examined and a conceptual framework that can be used as a starting point for the study of effective IPC/IPE interventions within clinical settings. Finally, this realist review highlights discrepancies in the terminology and methodology used to study similar cases, which will need to be systematically tackled by future research to further our understanding of those cases and of key elements of IPC/IPE in clinical working groups.
Keywords
Introduction
Interprofessional collaboration (IPC) is fundamental for good quality healthcare. The concept of IPC was first introduced by the World Health Organisation (WHO) in 1978 as a way to guarantee the effectiveness of primary healthcare. 1 IPC refers to two or more professions working together to achieve common goals and is often used as a means for solving a range of problems and complex issues. 2 Literature suggests that not only IPC increases collaboration, communication and quality of care both among healthcare professionals and patients, but also reduces costs, patient readmissions, length of stay and, consequently, mortality. 3 When healthcare professionals work in a collaborative professional context, there is a better understanding of patient care needs, team decision-making and an increased climate of trust amongst employees.4,5 Institutions that support teamwork and collaboration among their healthcare staff experience a reduction in adverse events. 6 Poor teamwork and poorly integrated care can lead to medical errors and generally diminished quality of patient care. 7
Effective IPC is a concept that has gained interest in both the literature and healthcare policies. Notwithstanding this renewed attention, IPC remains a complex concept often taken for granted by organisations. If the outcomes of IPC are to be achieved, health professionals need to gain and develop certain skills and knowledge, prior to working within IPC contexts. Leadership, mutual respect, coordination, cooperation, shared responsibility and good communication are essential factors of interdisciplinary collaboration. 8 Interprofessional education (IPE) is an effective way to enhance the work of healthcare professionals in IPC. 9 IPE can be defined as instances where “two or more professionals learn with, from and about each other to improve collaboration and the quality of care.” 10 An accomplished interprofessional collaborative healthcare worker is someone with the competency to work efficiently in a team where patient care is dealt through joint intervention among professionals from different disciplines and the patient itself. 11
An increased number of studies report a variety of educational interventions that enhance IPC/IPE in a clinical setting, even though the characteristics of these interventions may strongly differ in terms of duration, framework, protocol and guidelines, to name but a few.12–14 Several realist reviews have also been published in the literature on IPC/IPE regarding reflective practice, 15 cultural safety, 16 young professionals 17 and, predominantly, undergraduate education.17–20 However, there is little evidence in the literature regarding interventions that take place in already-graduated healthcare professionals in their daily clinical environment.
For this reason, the present systemic review focuses on interventions involving mainly graduated healthcare professionals and aims to, firstly, analyse IPC/IPE interventions so far outlined in the literature to summarise their key elements and, secondly, better understand how their contexts and mechanisms produce the desired outcomes, that is, improve and promote IPC and IPE.
Method
A realist synthesis approach in concordance with RAMESES II standards 21 was chosen due to its effectiveness in dealing with complex interventions where multiple interacting components and outcomes are involved. It was originally designed by Pawson et al 22 for complex social interventions to help understand the dissimilarity data that are generated when these social interventions are considered in different contexts to inform policy. A realist study posits that different contexts distinctly affect actions taken within them and responses generated by those actions; it looks to understand causal mechanisms of these responses (in this case, how are positive outcomes regarding IPC/IPE achieved). Thus, this realist review seeks to unfold the connection between the mechanism of the interventions, the context in which they happen, and their outcomes (ie, how the context interacted with the mechanism to deliver a specific outcome). 22 Reporting was in concordance with the RAMESES II reporting standards for realist evaluations 21 (Supplemental Material 1). A protocol for this realist review was registered with The Open Science Framework (available at osf.io/dcp75).
This realist review is part of a larger research project aimed at examining the importance of IPC/IPE in a large hospital setting, where various multi-professional collaborative teams work in different wards within their unique contexts. This new line of research will be conducted by the primary researcher of this paper, involving first-hand data collection on-site, by using observations and semi-structured interviews.
Search Strategy and Study Selection Criteria
Our search strategy combined MeSH terms and free text in the electronic databases PsycINFO, CINAHL, PubMed and Web of Science. There were no date restrictions applied, meaning that our search was expanded to include any records from the first run date of each database (for APA PsycInfo, this goes as far back as 1806). Only records in English were retained, to mount an analysis beyond localised backgrounds. Database searches were conducted again before the final analysis (July 5, 2024). Supplemental Material 2 displays the final search strategy that was used on PubMed; the adjusted strategies concerning the rest of the databases consulted are shown in Supplemental Materials 3 and 4.
The criteria adopted for inclusion were studies that report any kind of educational or collaborative intervention, the objective of which was to enhance IPC/IPE among healthcare professionals in a medical setting. An intervention can be defined as an action or group of actions purposely implemented to alter a behaviour, procedure, or direction to obtain a different result than the one which would have happened if the action had not taken place. The main objective of an intervention is to improve an existing condition or have a positive impact on a specific scenario. It can be applied in different fields like social services, education and healthcare. 23
A healthcare professional is defined as any individual in the healthcare sector (including patient care, support, and administrative role) who works in a facility where medical care and support are offered to patients. Initially, specific search terms, such as ‘doctor’ and ‘nurse’, were included to describe the professions concerned. However, it was soon established that, as representative of the idea of interdisciplinary collaboration, the overarching term ‘healthcare professionals’ offered a sufficiently large body of evidence to cover the scope of this research, which does not claim to be exhaustive.
No articles were excluded on design, type or methodological grounds. Only studies involving undergraduate or postgraduate students were excluded, as the objective of this research review is to reflect on the context and conditions experienced by healthcare professionals in their daily practice as realistically as possible, addressing the identified research gap, mentioned previously. In addition, studies not promoting the interaction among healthcare professionals to enhance collaborative practice were also excluded. Finally, studies referring to virtual contexts were excluded, as virtual contexts would entail a separate reflection on the frameworks shaping them and an extensive revisiting of the idea of ‘physical contact’ between collaborating professionals, which seemed particularly consequential from the outset. Moreover, given that there were no date restrictions applied to the body of data consulted, including virtual IPC/IPE interventions would most probably create a chronological bias (majority of studies would be dating almost exclusively from the last decade).
We (GBV, CMR) carried out the article selection procedure blindly and independently in accordance with PRISMA guidelines (Preferred Reporting Items for Systematic reviews and Meta-Analyses) 24 following three phases of selection: by title, by abstract and finally a full-text review using the RAYYAN screening tool. 25 At every step, we recorded reasons for exclusion and settled by discussion any difference in criteria. The third researcher (FM) was reached to obtain a consensus if necessary. Figure 1 shows the flow diagram of the study selection.

PRISMA flowchart diagram of search results up to July 2024.
Eligible articles identified through the screening process underwent a quality appraisal. Given the diverse methodologies of the studies, the Mixed Methods Appraisal Tool (MMAT) 26 was selected to guide this evaluation. The qualitative studies included in this review were evaluated using the Critical Appraisal Skills Programme (CASP) Qualitative Checklist. 27
Data extraction, Data Analysis and Synthesis of Findings
To analyse the data from a realist synthesis perspective, 22 we extracted information from the selected articles to identify key components of each intervention (descriptive data resumed in Supplemental Material 5). Next, a data matrix was created focusing on three essential elements of each intervention: context (C), mechanism (M), and outcome (O). We debated and defined the information needed to be collected under each of the three headings (results of this phase of the work presented in Table 1).
Characteristics of the Seventeen Interventions Implemented with Healthcare Professionals, as Derived from the Realist Synthesis Approach up to July 2024.

Context refers to the external factors that can alter the intervention's progression and outcome. To better understand this, we divided those factors into two categories: macro-context and micro-context. Macro-context includes the country and general setting of the intervention, the population that it is addressed to, and the professional framework that supports it. Micro-context refers to the relationship that occurs when healthcare professionals from different disciplines and backgrounds interact with each other to deal with patient care. These interpersonal encounters are a dynamic process where ideas and points of view are shared, to reach a common objective: best patient care.
Mechanism refers to the elements that contribute mechanically or contextually to a particular outcome and in what circumstance. For better understanding, Dalkin et al 28 following the work of Pawson and Tilley 29 divided Mechanism in two categories: Resources which concern all factors introduced in a context that have an impact on someone's reasoning, which, in turn leads to a change in behaviour and to an outcome, and Reasoning which refers to the attitudes, decisions, or ideas that result from the participants’ taking part in the intervention, subsequently fostering behavioural change. 30 So, one aspect of analysis focused on the resources utilised in the intervention and the other on how the reasoning of individuals changes via the implementation of the intervention.
During the analysis of the connections between the C-M-O configurations, the third researcher (FM) was reached once again to obtain consensus if necessary. The analysis is grounded in the several theoretical frameworks underpinning IPC/IPE which highlight the importance of communication, teamwork, shared goals and learning among professionals from different backgrounds.
Results
We originally retrieved a total of 2163 articles, of which 25 (1.1%) were selected for review, following the inclusion criteria. Eight (0.3%) more articles were ultimately excluded (2 involved students only, 3 did not promote IPC/IPE, 2 did not have an intervention, and 1 was a virtual environment). The final 17 (0.7%) articles included in the review revealed 17 completely different interventions (one per article) which were analysed using the realist synthesis method. 22
General Characteristics of the Reviewed Articles
Supplemental Material 5 shows the characteristics of each included article (17 in total), that is, each study's design and objectives, sample groups, frameworks and their respective focuses, with respect to the assessment instruments.31–47 The retained articles were published between 2002 and 2021 and most of them originated from the UK (8).32–34,36,39,41,44,46
Among the studies reviewed, most were qualitative ones (9),33,35,37–39,42–45 only 2 were quantitative46,47; the remaining 6 were of mixed methodology.31,32,34,36,40,41 Overall, 6 of the 17 included articles employed a quasi-experimental design, including 4 mixed methodology studies31,32,40,41 and 2 quantitative studies46–47; no qualitative study used this research approach. All studies used a variety of evaluation techniques, including interviews, surveys of different types (questionnaires/open-ended or rigidly structured), and even observation data. 39 All studies referred to post-implementation evaluations, while 6 also included pre-implementation ones.
More than 50% of the reviewed studies (9) focused on holistically framed interventions, defined here as comprehensive IPC/IPE programmes addressing IPC at the level of organisations or whole teams instead of single, isolated activities. The remaining studies (8)34,37,38,40,41,43,45,46 looked at independent IPC/IPE interventions, either one-off or iterative, including evaluation of IPC everyday settings.
Seven of the interventions/articles31,35,36,42–44,47 analysed were based on one or more conceptual frameworks; social identity theory,31,36 reflective and experimental theory, 31 social impact theory, 35 adult learning theory, 36 contact hypothesis, 36 interprofessional teamwork model, 42 social constructionism, 42 systems theory, 42 solution-focused approach (SFA), 43 collaborative learning approach, 44 social constructivist ontology, 44 Vygotsky's proximal development, 44 and experiential education. 47 The remaining ones32–34,37–41,45,46 were based on different methods and approaches: action research, 32 problem-based approach, 33 multidisciplinary (MDT) team approach, 34 analytic induction, 37 face-to-face communication, 38 interprofessional teamworking, 39 quality improvement collaborative (QIC) methodology, 40 action learning, 41 national quality forum (NQF) 45 and teamworking. 46
General Characteristics of the Reviewed Articles
Context
Macro-context: As previously mentioned, most of the interventions referenced took place in English-speaking countries (15), except for two that were situated in Scandinavian countries.38,42 The general settings of the interventions (12) were mainly based in large hospitals without distinctive differences among the different countries while five interventions were based in local primary care settings.33,40–42,44
Following our inclusion criteria, the target population in our review consisted primarily of professionals involved in healthcare delivery and related services, with one study additionally including patients. 44 Across the included studies, participants comprised medical staff31–34,36–42,44–47 such as physicians, specialist, and consultants; clinical staff including nurses,31–47 pharmacists,33,35,37,41,43,44 physiotherapists,32,38–40,42,44 occupational therapists,32,36–41 physchologists,36,42,44 social workers,36–37,39–43,45 and other allied healthcare professionals31,34,37–40,43,46; support and administrative staff such as managers,32,40,41,44 administrators,40,41 clerks 40 and porters 43 ; and educational and community staff including teachers, 42 researchers, 44 and chaplains.37,45
Micro-context: There was a general agreement within the reviewed articles, that IPC was enhanced when there was an increase of interpersonal time spent in the team. Six of the reviewed studies34,35,38,39,41,45 placed distinctive emphasis on the positive correlation between IPC and interpersonal time. According to them, “the introduction of regular team meetings offered an important meeting point for staff and a positive forum where staff could forge closer working relationships.” 39 It is in fact worth noting that those articles used different methodological approaches (4 qualitative, 2 of mixed methods), which points to a broader validity of the findings; also, that four of those studies reported interventions within large hospital settings.34,38,39,45 Large hospitals manage a relatively heavier workload; therefore, they could be considered as less likely to hold regular face-to-face meetings. In fact, one of the reviewed articles 34 characteristically reported in its final analysis: “Case volume (relating to a large hospitaĺs workload) may not influence the likelihood of holding MDT meetings.” 34
Mechanism
Resources: Through the analysis of the 17 interventions, we identified four resources:
the intervention's structure and characteristics (including target population) its development (including educational content and circumstances) its duration, and finally, aspects connected with its implementation tackling prior preparation and guidance (including conceptual framework).
Structure and characteristics (What is it?) In the pursuit of identifying the characteristics of effective strategies that enhance IPC/IPE, we conducted an analysis of various interventions. These ranged from comprehensive educational programs covering theoretical concepts and methodologies21,23,27,33,34,37 to hands-on clinical simulations.31,47 From the analysis, we could infer that, when the intervention in practice is underpinned by a theoretical foundation, there seems to be a better understanding of the elements that impact the effectiveness of IPC/IPE; this does not seem to be influenced by the setting (large hospitals or primary care local communities).31,35,36,42,44 Interaction-based strategies, such as role-playing, 47 focus groups, 35 small group discussions,31,33,38,44 and interviews,32,34,35 were employed to foster collaboration.
Regarding how similar strategies act on the different individuals, there is evidence to suggest that these are more effective if the volume of the group is kept relatively small, as this allows everyone to have a voice. This was supported by the outcomes of interviews reported in one of the reviewed articles, 33 where participants expressed concern about speaking up in larger groups due to fear of criticism. Groups formed by professionals who are already familiar with each other and distributed evenly among the different professions appear also to constitute factors contributing to positive results. 33 It is noteworthy that newly qualified professionals appear to be less interested in working in IPC/IPE, according to the findings of one of the reviewed articles, 36 which reported a statistically significant difference in evaluation scales between clinicians with more experience and those with less.
In terms of professions, the review analysis unveiled that nurses seem to have more positive attitudes towards the benefits of IPC/IPE than doctors. This was highlighted in one of the focus groups discussions 38 which explored differences in expectations and experiences when working in a collaborative environment involving the coordination of the different healthcare professionals that provide care to a single patient.38,40 Having said that, workload and individual interest are contextual aspects that can affect the initial positive attitude expressed by nurses. 38
When it comes to collaborating with patients with the objective of gaining further insight into IPC/IPE, the analysis found that the learning process seems to be more ambitious and difficult to work with but ultimately with positive outcomes. 44 Interview findings revealed both patients and healthcare workers felt that the presence of patients initially hindered the flow of communication. However, once this barrier was overcome, the patients’ input was considered valued and unique. 44
Workshops were also used as strategies which delved into essential aspects like speaking up, 47 leadership initiatives,45,47 work roles,33–35,40,44 workplace environment, 44 problem solving,37,39,42,44 action planning, 35 self-reflection,32,36 conflict resolution,39,40 adaptation to change,41,42,44,45 trust,39,40,47 interaction process, 37 building core communication and relationship skills45,47 and a competency-based approach. 42 Additionally, seminars, 37 presentations36,40 and case discussions31,33,34,36,37 also played a paramount role in IPC, along with team meetings held on a daily, 38 weekly, 39 or monthly basis,37,45,46 emphasising face-to-face communication34,35,38,44,45 and closer physical proximity.34,39 During the implementation of these strategies, the facilitator, who serves as a contextual anchor, appears to play a critical role in guiding the process and creating a relaxed atmosphere,33,46 as highlighted in interview responses. One interviewee stated: “I think the first few where we weren’t 100% how it was going to go, you need someone to facilitate it to get you all talking about the right things and in the right manner.” 33 Other key elements include the use of case-base-learning strategies and case group discussions, which seem to elicit a positive response by engaging them in real-world contexts, ultimately enhancing collaboration and interaction.33–36,44,46
Development of the intervention (How does it work?) The interventions analysed revealed the methods by which these were facilitated to new learners. We unveiled distinct strategies, including self-reflection,32,36 opening monologues that promoted uncovering thoughts and feelings, 47 conversation and listening skills that employed communication tools,31,40,44,47 debriefing sessions that followed up with questions and interaction,37,47 ice-breakers such as didactic lectures and group discussions,31,33,38,42,44 and the incorporation of staff huddles and one-to-one meetings.31,40 There was a common dynamic pattern in all of these strategies which was the repeated engagement of the individuals through a variety of approaches in an attempt to enhance collaborative skills for better and more efficient patient care.
The thematic content on which the above-mentioned methods are based appears to play a key role in enhancing IPC/IPE. This content is actively influenced by each organisation, its local context, and the behaviours of the participants. To be effective, as some of the interviewees pointed out, the content should be engaging, relevant to the community's needs,33,36,40 and supported by management so that participants can apply in practice. 40 Some participants mentioned they were unable to follow the program due to the content being too challenging and technical. 36 Regular feedback from participants helps to adjust both the message and its delivery to better meet their needs.31,34–36 Factors such as resource shortages and lack of time can directly impact the success of the intervention.31,41
Duration of the intervention: The structure and duration of the intervention varied considerably; most of the articles referred to interventions lasting from 3 to 12 months. Two out of the 17 referred to interventions spanning 2 years38,42 and there was also one case in which the article referred to a permanent, ongoing intervention. 45 In terms of the structure of the duration, the intervention was usually divided using distinct strategies. Again, there was diversity between cases and not all of them provided detailed information; from 3 h to 512 h was the mean duration of the interventions divided into an average of 6 to 10 sessions. Through the analysis of the reviewed articles, we could not identify any common pattern between the duration of the intervention and its structure. However, once more, the analysis did reveal that interventions involving regular meetings have a positive effect on education, communication and stress management for both patients and healthcare workers, as highlighted by the themes that emerged from interviews in the reviewed articles.34,41 In one of the studies in particular, 34 regular meetings were reported to help eliminate barriers and foster more fluid communication between junior and more experienced staff.
Other aspects concerning implementation (guidance and prior preparation). Additionally, we examined whether manuals, which guarantee the accuracy of the intervention's design existed or not; in 50% of the cases involved in our analysis, this turned out to be the case. Also, we looked at whether previous training to implement the intervention had been implemented or not; this was negative in all cases (Table 1).
Regarding the conceptual framework of the interventions analysed, 7 (41.1%)31,35,36,42–44,47 were based on 13 different conceptual frameworks, as previously mentioned. Seven of those 13 frameworks (social identity theory,31,36 social impact theory, 35 social constructionism, 42 social constructivist ontology, 44 Vygotsky's proximal development, 44 collaborative learning approach 44 and interprofessional team model) 42 shared a constructivist foundation where meaning and knowledge arise from social engagement and interaction with others. They underpin learning as an active, socially embedded process. 48 One particular conceptual framework 44 referenced Vygotsky's concept of the Zone of Proximal Development (ZPD), 49 which posits that every individual has an initial zone of development and with guidance and collaboration from others, they can expand their knowledge. A peer or experienced instructor can help broaden an individual's competencies, introduce new ways of thinking, and thereby enlarge the individual's initial zone of development. 49 The remaining six conceptual frameworks (reflective and experimental theory, 31 adult learning theory, 36 contact hypothesis, 36 systems theory, 42 SFA 43 and experiential education) 47 also maintained a constructivist perspective, emphasising learning through reflection, experience and these being context-dependent.50,51 The importance of a theoretical framework supporting the intervention should be examined in direct relation to the existence of manuals and any other preparatory material training the participants with respect to the intervention's components.
Reasoning
In our research analysis, we identified several crucial reasoning aspects. These encompassed fostering ease in interprofessional communication by reducing barriers,33,37,43 understanding professionals’ roles which enhanced team collaboration,32,38,40,44,45 establishing new cultural norms,40,47 empowering each team member to acquire knowledge,31,33,35–37,40 feeling valued 46 and contributing to the team's final goal,35,38,46 altering communication behaviours to create a climate of trust,39,40,47 openness, 41 empathy and compassion within the team, 45 and improving team conflict resolution methods.39,40 For example in one of the reviewed articles, 33 several interviewees appreciated the knowledge sharing, stating: “Everyone has really good habits in different areas, and everyone has their own strengths, and it's nice sharing those,” and “It makes you tackle areas which I probably wouldn’t have done otherwise.”
The effectiveness of these crucial reasoning aspects was also interrelated with their local context. Individuals tended to act more proactively towards members of different professions when pre-existing informal relationships were already in place, 33 and when their professions 39 and autonomy 36 were respected. However, individuals are less inclined to collaborate with others if acting alone or if they are perceived merely as representatives of their profession. 31
Outcomes
From the 17 interventions analysed in our research study emerged three different layers of outcomes. The first level corresponds to the changes triggered by having the interventions implemented to enhance IPC such as the employment of extra staff. This included increased presence of consultants in the clinic fostering more engaging dialogues. 39 In addition, decision-making processes saw greater participation from healthcare workers,37,39 while leadership initiatives within the department were initiated and expanded.45,47 Routine morning huddles, 47 regular seminars, 37 case discussions,31,33,34,36,37 and extra one-to-one meetings enhanced cross-professional interaction.37,46 The introduction of simulation cases,31,47 reflective journaling,31,35,36 and didactic lectures31,42 promoted learning experiences.
The second layer of outcomes relates to participants’ personal perceptions and reflections on the intervention they were involved in. These subjective opinions appeared during the interviews and follow-up workshops. Outcomes included an overall improvement in teamwork climate 46 with knowledge sharing,33,37 a reduction of staff stress 34 through peer support,34,38 a deeper understanding of responsibilities and practice's roles34,46 and behaviours,36,44,47 feeling respected 38 and empowered to take decisions 37 and leading roles 47 for greater patient care. In addition, there was a reduction in feelings of isolation 33 by fostering a sense of group membership,40,46 with greater enthusiasm, excitement, motivation, and interest in the work, ultimately contributing to personal growth. 40
The third layer of outcomes focuses on the clinical benefits that emerged from the implementation of the interventions. Notable outcomes include a patient-centred approach 38 with enhanced patient care,34,37,40 patient safety, 41 team climate,46,47 patient management, 32 and closer physical proximity of staff to patients34,39 leading to a more comprehensive care plan.32,35 In addition, a decrease in hospital readmissions, 32 length of stay 32 and staff sickness. 39
Even though the various layers of outcomes mentioned above highlight the importance and success of IPC/IPE interventions, they are influenced by the context in which they occur. Factors such as organisational cultures, 38 personal interests, 38 incentives, 33 motivation, 32 financial implications, 33 organisational support, 37 among others, can affect individual and group behaviours, leading to changes in the collaborative environment occurring at different speeds. 38 As highlighted by some participants (nurses) in the interviews, doctors were criticised for not completing the MDT pathways correctly, which led to communication breakdowns. 32
Discussion
Through the realist review, we analysed 17 articles which described different interventions with the aim of promoting any form of IPC/IPE among different healthcare workers and with the ultimate objective of improving patient care. This data analysis facilitated the creation of an explanatory model (Figure 2) concerning all interventions, which provides insight into the relation between the context of the intervention, its mechanism of action (including the theoretical framework on which it is based), and the desired outcomes. Identifying common ground or patterns in the implementation of the IPC/IPE intervention to achieve specific outcomes is of paramount importance for healthcare workers who would like to either create a new intervention or adopt an existing one to improve patient care.
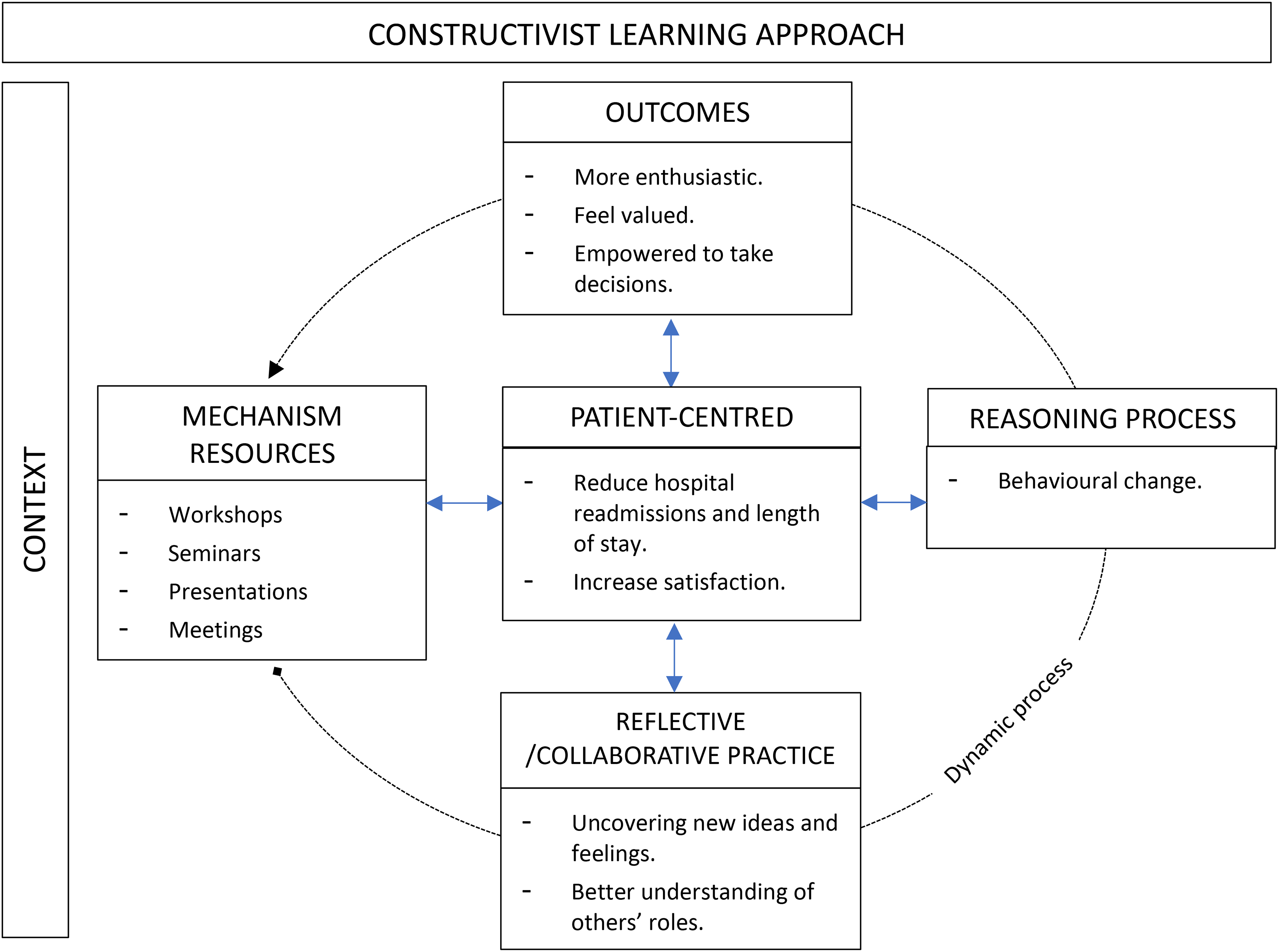
The explanatory model derived from the scrutiny of context-mechanism-outcome composition in the different IPC/IPE interventions up to July 2024.
It has been found that the learning theory of constructivism can serve as a foundational framework based on the principles of social collaboration. 52 It emphasises real-world meaningful contexts and builds on prior knowledge through reflective techniques, which are central to the interventions analysed. 53 Constructivism views learning as a dynamic, flexible process that promotes individual exploration and growth. 53 As such, it provides an effective analytical lens for understanding the different interventions addressed in this realist review, responding to each one's unique framework. It can similarly be considered as a key part of IPC/IPE enhancement processes, as it can help learners to deepen their understanding of those processes.
Social Collaboration
A critical element derived from the data analysis is the interrelationship among the different healthcare workers with the objective of learning from each other so that the collaborative practice runs more efficiently towards delivering high patient quality of care. Literature suggests that education by itself seems not to be sufficient for behavioural change but interventions that focus on a repetitive engagement of the participants seem to make a difference.54,55 This repetitive engagement was reflected in the various methods used during the “Development of the intervention (How does it work?”), with a common dynamic pattern observed in the reviewed articles, aiming to repeatedly engage individuals through a range of approaches.
According to D’Amour et al, 56 collaboration is based on two components: the development of a collective activity that deals with the complexity of participants’ needs, and the development of a team dynamic that integrates each person's point of view while enabling mutual understanding, trust and respect between all people involved. Regular feedback from participants, as revealed in our analysis can help adjust both the thematic content and its delivery to better meet their needs.31,34–36 Interestingly, our analysis also revealed that doctors and newly qualified professionals were criticised in several of the reviewed articles as participating in IPC/IPE interventions less effectively than other healthcare professionals, such as nurses.32,36,38 One reason for this, as noted by Hall 57 could be that doctors are trained to focus primarily on a patient's well-being rather than coordinating with healthcare professionals from different disciplines (ie, nurses, nurse assistants, pharmacists, physiotherapists). In contrast, nurses focus more on the patient's overall well-being, including the patient's subjective perception of it, through high-quality care, which requires building a more cohesive team dynamic. Regarding newly qualified professionals’ poor interest in IPC/IPE, 36 as noted also by Tunstall-Pedoe et al, 58 this could be due to their limited experience, which does not immediately allow them to appreciate the importance and benefits of collaborative work. This is why the WHO has advocated for the introduction of IPC/IPE at the undergraduate level. 59
‘Dialogue’ is a key component within the constructivist learning approach. 53 According to the National Coalition for Dialogue and Deliberation, 60 contemporary in-group dialogue performance is an activity designed to make participants engage together with the aim of exploring disharmonic social concerns, collaborative activity, decision-making and conflict resolution. The aim behind this engagement is to enhance relationships, empower individuals, offer a voice in shaping public policies, and promote learning. 61 Despite the diversity in the strategies used across the reviewed articles, dialogue (regarding activities and aims) was consistently found to be a fundamental dimension in all 17 interventions. However, dialogue also comes with challenges, as highlighted in our analysis. When patients were involved, the learning process became more ambitious and difficult to manage, yet ultimately resulted in positive outcomes. 44 These findings are consistent with those of other authors.62,63
Real-world Meaningful Contexts
Learning that takes place within communities of practice is based on social activities framed against a specific context, in this instance, the healthcare environment. Two main things thus occur: (i) learning is closely determined by the context and (ii) interaction between individuals induces learning.64,65 Both elements are also present in a constructivist learning approach as previously reported.52,53
Through the analysis of the reviewed articles, we could infer that context (i) plays a critical part in shaping the planning, application, and effectiveness of an intervention. The design of the intervention which should be adapted to the local context,33,36,40 could be influenced by factors such as time,35,37,39–43 available resources, 33 organisational frameworks, 35 the target community,31,43 as well as the engagement and support of both participating individuals32,33,36,38,39,41,45 and leadership. The success of an intervention is closely aligned with the social interactions (ii) that occur during its implementation.34,38 These interactions, while not exclusively, are influenced by factors such as (a) the size and distribution of healthcare professionals within different groups, (b) the thematic content on which the strategies are based, and (c) the task of a facilitator.
As noted by Wakeling et al, 66 larger groups, particularly those with 10 or more members, where professionals are unfamiliar with one another or unevenly distributed across different professions, can hinder individual engagement, trust-building, and dialogue. 33 Regarding thematic content, it should be appealing and aligned with participants’ needs, as revealed in our analysis.33,36,40 Strategies such as case-based-learning and group discussions have been shown to enhance positive responses by engaging participants with real-world contexts.33–36,44,46 The facilitator also emerged as a crucial factor33,44,46 in ensuring the effectiveness of interventions. They are instrumental in adjusting the content to meet participants’ needs and creating a relaxed environment where professionals from diverse backgrounds can collaborate and agree on common goals to improve patient care, aligning with the findings of O’Halloran et al. 67 It is worth noting that this crucial role of the facilitator finds parallels with Vygotsky's ZPD theory, which suggests that with guidance and collaboration from an experienced instructor, people can expand their knowledge. 49 Vygotsky's conceptual framework was utilised in one of the reviewed articles 44 and aligns closely with the core principles of constructivism. 53
In addition, the review analysis revealed that the “Macro-context” did not seem to have an impact on the design, implementation, or effectiveness of the various interventions. Despite interventions taking place in different countries, languages, and settings (such as large hospitals vs primary care, or distinct wards, such as Early Pregnancy Assessment, Orthogeriatric, or Palliative), these factors did not seem to affect the positive outcomes of the interventions, as long as other crucial parameters, such as the ones mentioned before were observed. On the other hand, one of the reviewed articles 34 pointed to the fact that a heavier workload in larger hospitals did not seem to hinder regular face-to-face meetings, reinforcing the idea that the “Micro-context” understood principally as social interaction is more consequential than the “Macro-context.”
In line with what has been observed regarding the “Macro-context,” it is worth noting that four of the reviewed articles31,36,42,44 which used the same conceptual frameworks (social identity theory31,36 and social constructivism),42,44 obtained similar outcomes, such as improved teamwork,31,36 enhanced professional competencies, 42 and a better understanding of one another's roles, 44 despite being conducted in different countries (USA, 31 UK36,44 and Finland), 42 employing varied methodological approaches (mixed methodology31,36 and qualitative research),42,44 strategies (clinician training, 31 case discussion, 36 role-play 42 and group discussion) 44 and intervention durations (4 months, 36 6 months, 31 1 year, 44 2 years). 42
The need for an intervention manual, available in only five (29.4%) of the articles,34,35,40,46,47 or for prior training, in turn lacking in all of them, was not confirmed as the existence of either of these two parameters did not seem to affect the outcome of the interventions.
Building on Prior Knowledge and Reflective Techniques
Building on prior knowledge and self-reflection techniques are a fundamental part of the constructivist learning approach because they support the creation of an individualised and meaningful learning experience. 53 Associating new pieces of knowledge to information learners already possess through deep reflecting thinking triggers cognitive activity, encouraging individuals to actively take part in the integration of new knowledge while consolidating the familiar one. 53 Through the analysis of the reviewed articles, we could not identify any common pattern between the duration of the intervention and the structure of it. However, the analysis did reveal that IPC/IPE was enhanced when teams increased their interpersonal time together, either by increasing the frequency of regular meetings or extending the duration of each encounter.34,35,38,39,41,45 This additional face-to-face contact time appeared to be closely linked to improved understanding and trust-building among healthcare workers. 52 It also provided opportunities for participants to actively construct meaning and integrate new insights into their prior knowledge, making the learning process more effective and valuable. 53 Strategies that were found in our review analysis to strengthen this process were: role-playing, 47 focus groups, 35 small group discussions,31,33,38,44 problem solving,37,39,42,44 action planning, 35 self-reflection,32,36 conflict resolution,39,40 building core communication45,47 and adaption to change.41,42,44,45 Even though the activities varied substantially among them, the core element was to engage participants in an active, self-driven learning process taking into consideration local needs. That being said, factors such as resources, time constraints, workload, personal interests and motivation need to be considered within the context, as they can significantly influence participants’ active engagement.31,38,41
Explanatory model
The scrutiny of the context, mechanism and outcomes (CMO) composition gives an indication that the physical aspect that comes with each intervention and its characteristics produces an emotional, psychological and social effect on the multiple dimensions of the participants that increases simultaneously the effectiveness of the mechanism of the intervention. This dynamic relationship is divided into different stages which are interrelated and happen under the umbrella of a specific context and a conceptual framework; the mechanism resources enhance the creation of ideas and attitudes within the community that then lead to a behavioural change in the individuals (Reasoning). In turn, this change leads to an emotional sensation of fulfilment and personal enrichment when improving patient care (Outcomes). This continuous data of patient and staff feedback closes the dynamic cycle process by making the mechanism improve and be more effective. Figure 2 shows the explanatory model created from the 17 CMO interventions.
Strengths, Limitations and Future Research
The strength of this study is that through a realist synthesis approach, it has managed to analyse, integrate and find common ground from a wide range of data originating from diverse backgrounds, methodologies, outcome evaluation techniques, and conceptual frameworks. At the same time, the same diversity of the analysed articles highlights the need for further research to compare and validate the findings.
Another important limitation of our research is the discrepancy found among the different articles reviewed when it comes to the standardisation of the IPC/IPE concept, taking into account that different definitions and terminologies have been widely used to convey similar meaning. Concepts like interprofessional (IP) learning, IP team working, IP practice, IP care, continuing IP education, team working, multi-professional meetings, multi-professional education, multidisciplinary team learning, multidisciplinary team collaboration, interdisciplinary interactions, interdisciplinary team training, transdisciplinary teamwork, collaborative multidisciplinary care teams were used indistinctively in the literature concerned by our research, without a clear consensus regarding their definitions, competencies and limitations. Further research is needed to identify the causes of this discrepancy and clearer guidelines should be in place for researchers to follow. For this same reason, our findings constitute a valued addition to the current knowledge in this field since, on the one hand, we managed to uncover this limitation in current terminology and, on the other, we managed to achieve clear conclusive outcomes, despite it.
A final limitation we encountered relates to the outcomes of the articles reviewed. The participants in the different studies may not represent realistic scenarios in many other professional settings experienced by healthcare professionals, as those selected for the intervention were chosen on their prior willingness, availability, and interest in IPC and/or IPE. Therefore, the positive outcomes obtained in each article may not be entirely attributable to the success of the interventions. In addition, in most of the articles (64.7%),31–35,38–40,43,45,47 there were only a small number of respondents (less than 50%) to the intervention follow-up interviews and/or focus groups.
Conclusion
This systematic realist review has produced an in-depth evaluation of all the interventions described up to date that enhance IPE/IPC among healthcare professionals with the ultimate goal of improving patient care. Despite this being a hot topic in the current literature, the number and design of the interventions remain small and diverse. The explanatory model obtained from the analysis in this review should be of considerable help to future clinicians who decide to implement an already-described intervention or create a new one in their workplace.
At the same time, as the concepts of IPE and IPC continue to develop, this review will be useful to future research, when it comes to a clear definition of the aims, design of the interventions (context-mechanism-outcomes), participation and measurement of results. There is a need for further research that considers the limitations described here and investigates in depth the complex dynamics among healthcare professionals with the ultimate goal of improving the delivery of patient care.
Supplemental Material
sj-docx-1-mde-10.1177_23821205261425325 - Supplemental material for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review
Supplemental material, sj-docx-1-mde-10.1177_23821205261425325 for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review by Gerard Balague-Viladrich, Frederico Matos and Cristina Monforte-Royo in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205261425325 - Supplemental material for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review
Supplemental material, sj-docx-2-mde-10.1177_23821205261425325 for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review by Gerard Balague-Viladrich, Frederico Matos and Cristina Monforte-Royo in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205261425325 - Supplemental material for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review
Supplemental material, sj-docx-3-mde-10.1177_23821205261425325 for Interprofessional Collaboration and Interprofessional Education Interventions in Clinical Healthcare Settings: A Realist Review by Gerard Balague-Viladrich, Frederico Matos and Cristina Monforte-Royo in Journal of Medical Education and Curricular Development
Footnotes
Ethical Considerations
This article does not contain any studies with human or animal participants.
Consent to Participate
Not applicable.
Consent to Publication
Not applicable.
Author Contributions
GBV conceived the study as part of doctoral research, led the study design, conducted the literature search, performed the article selection process, and drafted the manuscript.
FM contributed to study design, discussed selection of relevant articles, provided methodological guidance and critically reviewed the manuscript.
CMR contributed to the conception and study design in a supervisory capacity, independently conducted article selection, contributed to interpretation of findings, and critically revised the manuscript.
All authors reviewed and approved the final version of the manuscript and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data available from the corresponding author upon reasonable request
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.