
Abstract
OBJECTIVES
While most hospital-based, healthcare professionals are expected to teach and supervise, few receive training in education. We designed, implemented, and evaluated an interprofessional, hospital-based teaching certificate program based on experiential learning and reflective practice for healthcare professionals with little or no formal training in education.
METHODS
Participants attended educational seminars; incorporated new concepts, skills, and behaviors in their teaching; and submitted written reflections. Participants also met with an education coach, received feedback from a trained observer, and observed a “master teacher.” We used descriptive statistics to analyze a survey distributed to the 2017–2019 cohort. We also analyzed written reflections to determine whether participants described a new teaching skill, concept, or behavior, and how they applied these to their teaching.
RESULTS
Survey completion rate was 15/20 (75%). Participants described feeling connected to an educator community, establishing educational alliances with senior educators, and learning teaching strategies from other certificate members outside their own profession. Participants indicated they are more likely to pursue educational innovation, leadership, and scholarship. In the reflections, 88% described incorporating a new concept in their teaching.
CONCLUSION
Participants in an interprofessional teaching certificate program engaged in a curriculum of professional development in education. Graduates of the program reported knowledge gain, behavior change, and establishment of educational alliances and a community of practice.
Introduction
Nearly all hospital-based healthcare professionals supervise and teach others. Some clinical educators pursue intensive training in education through master's degrees, local fellowships, 1 or national longitudinal programs to gain the knowledge, skills, and competencies to teach2,3; however, many of these programs can be costly and time intensive. Many clinical educators only participate in limited professional development through occasional teaching workshops, as there are no universal accreditation standards and assessment methods to certify healthcare professionals as competent teachers. Additionally, few interprofessional programs focus on developing healthcare professionals as educators, even though interprofessional education has recently been recognized as a critical tool to improve practitioners’ teamwork and optimize communication, collaboration, and patient care. 4
To meet these needs at Boston Children's Hospital (BCH), one of the largest pediatric academic medical centers in the United States, we designed, implemented, and evaluated an interprofessional, hospital-based teaching certificate program based on experiential learning and reflective practice. We sought to assess if this hospital-based, interprofessional teaching certificate program would lead to the application of new knowledge into participants’ own teaching practice. We also examined program feasibility, impressions of the program, if participants felt connected to a community of educators, and whether they developed an educational alliance with senior educators.
Methods
In 2016, we designed and launched a 2-year, interprofessional teaching certificate program that includes educational seminars, coaching, and observation experiences. The program is targeted toward healthcare professionals with little or no formal training in health professions’ education and can be completed while maintaining participants’ clinical and teaching schedules. The program jointly accredits physicians, nurses, pharmacists, psychologists, and social workers, and offers a flexible schedule of seminar offerings and activities as well the opportunity to form a community of practice.
Curricular components
Educational seminars
Certificate members participate in 10 interactive, evidence-based, professional development seminars. Six, one-hour seminars focus on core teaching topics identified through a modified Delphi process: adult learning principles, 5 active learning, 6 feedback, 7 critical thinking,8,9 supervision, 10 and instructional design. 11 After each core seminar, participants have 6 weeks to apply a new concept, skill, or behavior gained from the session to their authentic teaching practice. Participants submit written reflections describing their teaching successes and challenges in applying these new concepts, skills, or behaviors. For the remaining 4 seminars, participants choose sessions that meet their learning needs from the hospital's academy of educators’ professional development series. 12 Examples of the academy's seminars include “How to write a narrative evaluation” and “How to establish an inclusive learning environment.”
In these early years of the certificate, all but one of the seminar instructors were physicians; however, as the program has grown, instructors now represent an array of professions, including psychology and nursing. The course directors meet with all seminar instructors prior to each session to orient them to the interprofessional nature of the program, as we found that many educators have limited experience teaching to an interprofessional audience. This includes emphasizing the importance of using varied professions in case examples and using the terms “educator” and “learner” rather than profession-specific terms. We also ask the participants and facilitators to use first names only. We have found this practice levels hierarchy and encourages everyone to participate. Moreover, in order to encourage participants to learn with, from, and about each other, we pre-assign breakout discussion groups with a mix of professions. This prompts participants to problem solve across professions and share their own personal experiences and perspectives.
One-on-one experiences
Each participant engages in 3 individualized learning experiences with structured reflection, debriefing, and coaching. First, senior educators, trained in peer observation, observe the participants teach and provide individualized feedback. 13 Second, participants observe a senior “master” teacher lead a clinical teaching session and then debrief the observation. 14 These experiences occur in the participants’ own teaching venues (eg, operating room, simulation center, classroom) to ensure maximum educational impact. Third, participants meet with an educational coach at least 3 times over the course of the program to discuss their teaching challenges and career goals. We conducted in-person training for a selected, interprofessional group of senior educators at BCH, who would serve as the coaches. The senior educators were selected because of their membership in the BCH Academy for Teaching and Education Innovation and Scholarship, their years of teaching experience, and their participation in an intensive health professions education program such as a fellowship or master's degree. The coach training was led by a Harvard Medical School and Harvard TH Chan School of Public Health associate professor with expertise in faculty mentoring and coaching. The structured guide used for the one-on-one coaching meetings was adapted from Palamara et al's professional development coaching program. 15 We stress interprofessional learning in our Master Teacher Observations, Peer Observations, and Coaching experiences, and often pair participants from one profession with senior educators from other professions.
Conceptual framework
Experiential learning benefits healthcare professional educators as it values the practice of professional skills in real life contexts, can be used to design learning strategies for constructing knowledge, and promotes competencies for professional practice.16,17 We used Kolb's Experiential Learning Theory to develop the curriculum. 18 Kolb's experiential components include: participation in case-based seminars and teaching observations (concrete experiences); reflection on these activities (reflective observation); incorporating relevant learning, including master teacher observation, into a new plan for teaching (abstract conceptualization); coaching to help certificate members interpret and understand why teaching experiences were or were not successful (abstract conceptualization); and integration of educational concepts, skills, and behaviors into own teaching practice (active experimentation). We designed the program to be interprofessional so that diverse healthcare professionals could discuss common teaching challenges, learn how varied professions apply educational principles in different contexts, share best teaching practices across professions, and engage in an educator community of practice.
Evaluation
We performed a cross-sectional survey of the 2017–2019 teaching certificate cohort, distributed following their completion of the program. Participant professions included 10 physicians (50%), 6 nurses (30%), 1 dentist (5%), 1 pharmacist (5%), 1 occupational therapist (5%), and 1 radiologic technologist (5%). The survey (supplemental document A) was designed by experts in medical education (ASW and LRN) and included questions about the program's impact on perceived: behavior change, connection with a community of educators, development of an educational alliance (meaning participants were able to identify someone in the program who demonstrated trust in their ability to achieve their teaching development goals 19 ), interprofessionalism, and overall impressions. Although there were no published surveys with validity evidence in our target population that we were able to identify when designing our survey, we utilized available literature to inform the development of our survey questions.19–23 We also used Kirkpatrick's 4 Levels of Training Evaluation to construct the questions, with a particular emphasis on Level 2 (learning): the degree to which participants acquire the intended knowledge, skills, attitude, confidence, and commitment based on their participation in the training; and Level 3(behavior): the degree to which participants apply what they learned during training to their teaching practices. 24 The survey was pilot tested using cognitive interviewing with 2 prior certificate members, leading to minor wording adjustment.
In addition to the survey, 3 independent reviewers (ASW, KH, LN) rated participants’ reflections for 4 core seminars to determine: (a) whether participants were able to describe a new teaching skill, concept, or behavior taught during the seminar, and (b) whether they applied this new knowledge to their teaching practice after the seminar. At least 2 reviewers independently rated each reflection using a structured scoring rubric and resolved discrepancies through discussion. Reflections from 2 of the 6 core seminars were excluded from the analysis as they required a different submission format (eg, lesson plan). Exemplar responses were identified, and permission was obtained to include these excerpts in a publication. The Boston Children's Hospital institutional review board determined the protocol to be exempt from the requirements of 45 CFR 46 (BCH protocol number IRB-POOO24756). A consent process was included in the survey (supplemental document A) and included the following clause: “This is an anonymous survey (names will not be collected) and completion of this survey is entirely voluntary. The results of this survey may be published, using only aggregate, anonymous data (anything that is identifiable, will not be included). If you are concerned about publication of the data and do not wish to participate, simply do not fill it out.” Additionally, we obtained verbal consent from the participants whose excerpts were included in Table 1.
Samples of participants’ reflections describing how they incorporated a new teaching concept, skill, or behavior into their teaching.

Results
All 20 cohort members graduated from the program. Survey completion rate was 15/20 (75%). Participants’ perceptions of the program's impact are summarized in Table 2. The majority of participants (87%) reported feeling connected to a community of educators. Ten respondents (67%) also reported establishing an educational alliance with someone from the program, including with their educational coach (7/10, 70%), their master teacher (6/10, 60%), their peer observer (3/10, 30%), a fellow teaching certificate member (2/10, 20%), and a teaching certificate program director (2/10, 20%). Participants reported the program helped them further understand their teaching roles and the roles others play on an interprofessional clinical team. Furthermore, the majority of participants (87%) reported learning teaching strategies or approaches from certificate members outside of their own profession; 73% indicated that they are more likely to pursue educational innovation, leadership, and scholarship as a result of the program. All participants would recommend the program to a colleague.
Teaching certificate participants perceptions of the impact of the BCH program.
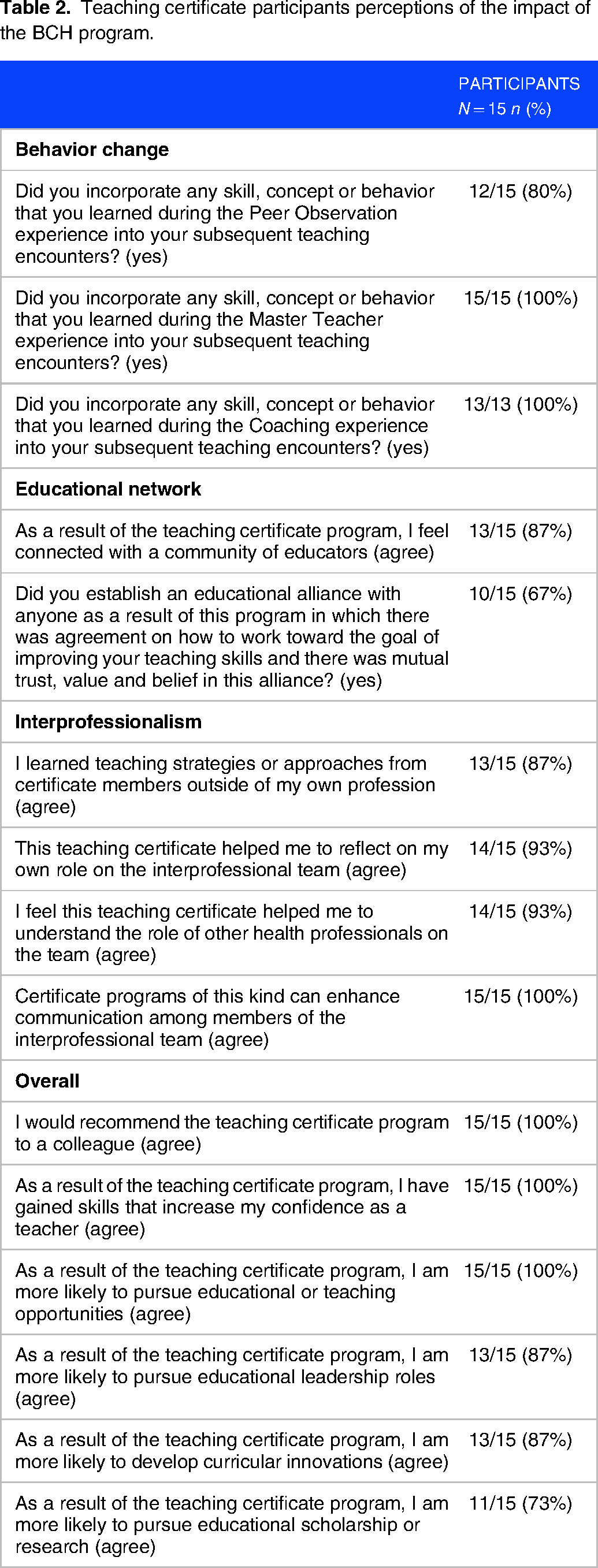
The majority of participants reported incorporating a skill, concept, or behavior they learned during the peer observation (80%), master teacher (100%), and coaching sessions (100%) into their subsequent teaching encounters. Additionally, in their reflections, participants described changes in their teaching practice. Of the 78 reflections that were submitted and scored by the research team, 78 (100%) described a new teaching concept, skill, or behavior gained from the seminar, and 69 (88%) additionally described applying this new knowledge to their teaching. Excerpts of participants’ reflections on applying a new teaching concept, skill, or behavior to their teaching for each of the four seminars are listed in Table 1.
Discussion
This 2-year teaching certificate program, grounded in experiential learning, reflection, and personalized coaching and observation, offers continuing professional development by building foundational skills for educators. Participants reflected on and reported integrating new knowledge, skills, and behavior into their educational practice. Furthermore, participants noted that participating in the program enabled development of educational alliances with senior educators.
There are few teaching certificate programs noted in the literature and most are geared toward a single specialty or health profession.25,26 However, interprofessional education supports members of different healthcare professions to learn interactively together as members of a community of practice, with the goals of improving interprofessional collaboration and professionalization of their roles as educators.27,28 Communities of practice emerged from the understanding that such a community is “a persistent, sustaining social network of individuals who share and develop an overlapping knowledge base, set of beliefs, values, history and experiences focused on a common practice and/or mutual enterprise.” 29 A community of practice particular to health professions’ education emerged from social learning theories that propose learning is a social activity that takes place in communities, heavily influenced by history and culture. 30 By joining a community of practice of interprofessional educators, we aimed to have teaching certificate members connect with like-minded individuals, thereby increasing their understanding of their teaching roles and their personal commitment to those roles. 30 Accordingly, participants in this certificate program reported that they were able to learn from educators in other healthcare professions and better understood the roles of other members of an interprofessional team. Moreover, when the program was initially launched, nearly all the seminar instructors were physicians. As the program has grown, we have intentionally included instructors from other professions, including psychology and nursing, to co-lead the seminars. In addition, we now have educators from different professions support the program as coaches, master teachers, and peer observers. The diversity of educators, including those from physical/occupational therapy, social work, psychology, and nursing, enables us to cater to the wide range of learner experiences in the program. We believe that this model exemplifies interprofessional collaboration and effective teaching practices.
Busy clinicians, across professions and clinical care settings, need access to longitudinal professional development opportunities focused on teaching, beyond occasional workshops. 31 Literature reviews of health professions education highlight the positive impact of longitudinal professional development in advancing educational leadership, scholarship, and networking. 32 Other fellowship and master's programs are often expensive or require scaling back or restricting clinical or teaching activities to complete the training. The teaching certificate's 2-year structure allows participants to complete activities alongside their clinical duties and regular teaching responsibilities. The feasibility of the certificate program for busy clinicians is corroborated by its 100% completion rate. This structure also allows the program to be accessible for novice healthcare professionals who have no experience in education, yet are expected to immediately assume teaching roles. Since this study, in the setting of the COVID-19 pandemic, we have transitioned the seminars to an online format, which enables asynchronous learning and increased accessibility.
Limitations of the study include reliance on participants’ self-report of behavior changes, lack of a fully validated survey instrument, the potential for a non-response bias, a small sample size, and lack of a control group. Additionally, participants were not asked to identify their professions in the survey; we were therefore unable to analyze the differential impact of the program by profession. Furthermore, the program requires administrative resources that may not be available at other institutions. Future study should include objective outcomes such as student ratings or observed structured teaching encounters 33 and a qualitative thematic analysis of reflections.
Conclusion
A hospital-based, interprofessional teaching certificate program, developed using experiential learning theory and reflective practice, is feasible, leads to reported behavior change, and fosters educational alliances and a community of educators. Recognizing the impact of this program, we aim to scale our program locally, with the goal to require teaching certificate participation for all new healthcare professional educators. We encourage other academic medical centers to implement teaching certificate programs to ensure that those who educate future healthcare professionals meet teaching standards as well as professional and interprofessional competencies.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231205433 - Supplemental material for Beyond the Workshop: Results From a Longitudinal, Interprofessional Teaching Certificate Program
Supplemental material, sj-docx-1-mde-10.1177_23821205231205433 for Beyond the Workshop: Results From a Longitudinal, Interprofessional Teaching Certificate Program by Ariel S Winn, Kathleen Huth, Alan M Leichtner and Lori R Newman in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors would like to thank the participants of this program and the healthcare professionals who taught seminars and served as coaches, peer observers, and master teachers. Additionally, they would like to acknowledge the administrative support of Angela Lam, Rosalyn Pofcher, and Joseph Fournier.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.