
Abstract
Purpose
Physician involvement in healthcare leadership is essential for improving healthcare systems, yet medical students’ interest in future leadership roles is underexplored. This study aimed to examine first- and final-year medical students’ interest in leadership roles.
Methods
In 2021, online questionnaires were distributed to both cohorts, yielding response rates of 94% (109/116) and 87% (95/109), respectively. A mixed-methods approach was employed to examine leadership interest. Free-text responses were first analyzed through inductive content analysis and subsequently, a quantification analysis was performed. Cohort comparisons were conducted to evaluate differences, and age and gender data were collected as background variables.
Results
First-year students exhibited greater optimism, viewing leadership as a natural extension of their careers. Final-year students increasingly prioritized clinical roles, reflecting the influence of physicians’ identity formation and the demands of clinical practice. Final-year students exhibited lower levels of strong interest in leadership and higher levels of disinterest than first-year students. The quantified results aligned with these findings, as 38.5% of first-year students expressed strong interest, compared with 30.5% of final-year students. Conditional interest was higher among first-year students (30.3%) than among final-year students (24.2%), whereas disinterest was higher among final-year students (37.9%) than among first-year students (24.8%). Uncertainty regarding leadership roles was observed in both groups (6.4% of first-year and 7.4% of final-year students).
Conclusions
Differences in leadership interest suggest that increasing clinical responsibilities and physicians’ identity formation may influence students’ interest in leadership roles. Integrating early and longitudinal leadership education into clinical practice—emphasizing its clinical relevance and alignment with physicians’ professional identity—may help sustain interest, support career-aligned leadership decisions, and better prepare future physician leaders.
Introduction
Value of Physician Leadership
The healthcare sector is undergoing continuous transformations, underscoring the essential need for effective leadership. 1 Leaders with clinical backgrounds, particularly physician leaders, are pivotal in successfully navigating these changes. 1 Physician leaders contribute significant value to organizations, as evidenced by various indicators. 2 Initiatives led by physician leaders have been linked to improved patient outcomes and life-saving impacts. 3 Furthermore, healthcare projects are more effectively implemented when led by physicians. 4 Hospitals with a greater proportion of experienced clinical leaders also tend to adopt more management best practices focused on task-oriented outcomes, which is positively correlated with financial performance. 5 Additionally, physician-led accountable care organizations demonstrate superior financial reporting standards and advanced IT capabilities. 6
Physician Leadership
Leadership is understood as a process in which a leader deliberately influences others by directing, organizing, and supporting activities and relationships within a group or organization to accomplish a shared objective.7,8 A leader's role typically includes both leadership and managerial functions. 7 Management entails creating and upholding systems, controls, procedures, policies, and organizational structures. In contrast, leadership centers on building trust and mutual understanding among individuals and is marked by innovation and a drive to initiate change. 9 Some scholars argue that leadership skills are complemented by management, 10 a view supported by Mintzberg's managerial role theory, which identifies leadership as one component within the broader set of managerial responsibilities. 11
Physician leaders commonly hold hybrid roles that combine leadership and managerial responsibilities with clinical practice.12–14 Their work is shaped by complex influences, including ongoing system-level changes and external pressures, while ensuring that healthcare organizations fulfill their professional obligations. 15 Therefore, physician leaders play a key role in overseeing medical services, safeguarding the quality of care, and connecting administrative policies with clinical practices.16–18
Challenges in Physician Leadership
New graduates are poorly prepared to fill leadership roles, as they often lack leadership-specific communication skills. 19 Chief residents have identified a lack of leadership, management, communication, role clarification, and professional status as pitfalls that interfere with success in resident leadership roles. 20 Primary care physicians often view themselves as uniquely suited for leadership roles but face obstacles such as inadequate leadership education. 21 Physician leaders frequently experience identity conflicts, sometimes prioritizing their role as physicians over that of leaders. 22 This conflict can hinder their ability to implement initiatives that empower their teams, ultimately affecting team effectiveness. 23 These challenges are often rooted in the strong occupational identity of physician leaders, which is closely tied to their professional status and autonomy. 23
Interest in Physician Leadership
Research on medical students’ perceptions of physician leadership is both limited and controversial. 24 A review study indicated that many medical students display limited enthusiasm for leadership positions. 25 Similarly, resident physicians have shown little inclination toward formal leadership roles, viewing them as potential threats to their professional identity as practicing physicians. 26 On the other hand, some studies suggest that while medical students may be receptive to leadership responsibilities within clinical teams, they exhibit less enthusiasm for managerial positions. 25 Other research highlights the complexity of perspectives on leadership among medical trainees, emphasizing differences across specialties and their broad acceptance of leadership roles. 27 Furthermore, a recent study found that medical students’ perceptions of how physicians should be led remain consistent throughout their education. 28
Need for Leadership Education
There is a widely recognized need for standardized leadership education to instill leadership skills early in undergraduate medical curricula.19,27 However, leadership training is often absent from medical school curricula, 29 and existing programs vary significantly, with few aligning seamlessly with established competency frameworks.30,31 Empirical evidence on the successful integration of leadership studies into medical education is scarce globally. 31 This lack of professional consensus on the scope of medical leadership and its optimal pedagogical approach impedes the effective integration of leadership education into medical curricula.30,31
Professional Identity Formation
Professional identity formation in medical students is a complex and multifaceted process shaped by the interaction of clinical and non-clinical experiences, contextual demands, and environmental influences with students’ personal values and beliefs. 32 This process unfolds through ongoing cycles of integrating and re-evaluating professional values and behaviors within an existing sense of self and may be impeded when insufficient or inappropriate support turns developmental influences into obstacles. 32 As a non-linear and evolving phenomenon, professional identity formation involves negotiating tensions between personal and professional domains, while institutional strategies—such as mentorship, guided reflection, and supportive learning environments—play a central role in facilitating the alignment of personal and professional identities over time, ultimately contributing to improved practice at individual, institutional, and societal levels. 32 Hence, organizational support plays a vital role in fostering leadership development. 27 Genuine leadership experiences, backed by trainers and institutions, benefit trainees and offer opportunities for meaningful service improvement. 27
Research Gap to Fill
As physician involvement in healthcare leadership is essential for improving healthcare systems, medical students’ interest in future leadership roles is underexplored. To address this research gap, it is essential to explore medical students’ perceptions of leadership throughout their education. This study examines and compares the perceptions of first- and final-year medical students toward future leadership roles. To the authors’ knowledge, no previous study has explored this topic in such detail. The findings are expected to offer universal insights for leadership education in medical curricula.
Study Objectives
To evaluate interest levels in pursuing physician leadership roles in the future among first-year and final-year medical students. To analyze differences in attitudes towards leadership roles between first- and final-year medical students.
The Context of the Study
Undergraduate medical education in Finland lasts 6 years and comprises 360 ECTS credits. 33 The first 2 years focus on preclinical studies. This is followed by a 4-year clinical phase in hospitals and health centers, providing students with exposure to a range of medical specialties. 34 A distinctive feature of Finnish medical education is the longstanding practice that allows medical students, after 4 years of training, to temporarily assume formal doctor positions in specialized care units or health center wards, under the written supervision of an assigned healthcare professional. 35
Conceptual Framework
This study was exploratory in nature and employed an inductive mixed-methods approach. Therefore, no single leadership theory guided the data analysis. Instead, participants’ responses formed the basis for category development. Existing literature on physician leadership and professional identity formation served as a conceptual framework to support the interpretation and discussion of findings in relation to leadership education within medical curriculum.
Methods
In 2021, invitation emails containing online questionnaires, detailed instructions, and study objectives were sent to all to of the first- and final (sixth)-year medical students at the University of Oulu, Finland. Given the total class sizes (116 first-year and 109 final-year medical students), we invited all students to participate, ensuring adequate representation, which yielded high response rates of 94% (109/116) and 87% (95/109), respectively. The recruitment for this study took place between September 10 and September 19, 2021, for first-year medical students, and between October 28 and November 4, 2021, for final-year medical students. Final-year medical students were assumed to have a basic understanding of physician leadership, owing to their exposure to leadership and management concepts throughout their medical curriculum, with which first-year students were not yet familiar. The entire survey included several questions on students’ perspectives on physician leadership, but not all these questions were analyzed in the present study, as some had been published previously. The questions were intentionally analyzed in separate studies to allow a focused examination of each item, to provide a more in-depth discussion of each phenomenon, and to link the findings meaningfully to the relevant literature. The specific survey question used here was “Would you be interested in working as a physician leader in the future?” This single open-ended qualitative question was chosen to elicit a broad range of responses not limited by narrowly defined topics. The responses were saved digitally and coded for analysis, producing seven A4 pages (Calibri, 12 pt, single spacing). An English-translated version of the original Finnish survey is provided in Appendix 1.
A mixed-methods approach was employed to address the research question from multiple perspectives, with inductive content analysis and quantification applied to both datasets, and the results were subsequently compared. 36 First, qualitative responses from both student groups were analyzed separately via inductive content analysis, 37 providing a description of the phenomenon and possibility to connect findings to broader contexts and the existing literature. 37 The analysis followed a three-phase process: first, the data were read repeatedly for familiarity, with key phrases highlighted and coded to reflect levels of leadership interest (interested / not interested). Next, the open codes were consolidated into broader categories on the basis of their similarities (interested / not interested /conditional). Finally, these categories were refined into higher order themes representing varying levels of students’ leadership interest. To examine differences in leadership interest throughout medical education, data from both groups were compared. Relevant participant excerpts were cited, labeled with participant numbers, and distinguished as first-year (F) or final-year (S) students. The citation selection process maintained respondents’ anonymity, with any citations that could potentially compromise anonymity modified or excluded without affecting the analysis or results. 37 The results were subsequently organized and presented systematically in a tabular format (Table 1).
Main Themes and Results from the Inductive Content Analysis of Medical Students' Responses Regarding Interest in Leadership Roles, with Illustrative Citations and a Comparison between Cohorts.

Source: Authors' own work.
Statistical Analysis
Following the inductive content analysis, a quantification analysis was performed on both datasets. Quantification, referring to the “numerical translation, transformation, or conversion of qualitative data,” is an integral component of mixed-methods research. 38 (p208) As such, in quantification, the data are calculated based on how many participants express the same thing. 39 In this study, this involved calculating the number of participants expressing each level of leadership interest (Table 2), presented as absolute values (n) and percentages (%). This allowed for a direct comparison of leadership interest levels between the two groups. Quantification provides an additional perspective on qualitative data interpretation, 40 facilitating a more robust and nuanced discussion41,42 and strengthening the study's triangulation and reliability. 37 Triangulation was further reinforced through cross-group comparisons, offering a comprehensive view of leadership interest in different steps of medical education. Comparable findings validated the conclusions from both groups, whereas differences provided opportunities for a deeper exploration of context and meaning. 43 All eligible first- and final-year medical students at the institution (n = 116 and n = 109, respectively) were invited to participate. Formal sample size calculations were not performed due to the exploratory nature of the study; however, the high response rates (94% and 87%) ensured that the sample was broadly representative of each cohort. Because of the relatively small number of participants in each leadership interest category, advanced statistical analyses were not performed. The results were subsequently organized and presented systematically in a tabular format (Table 2).
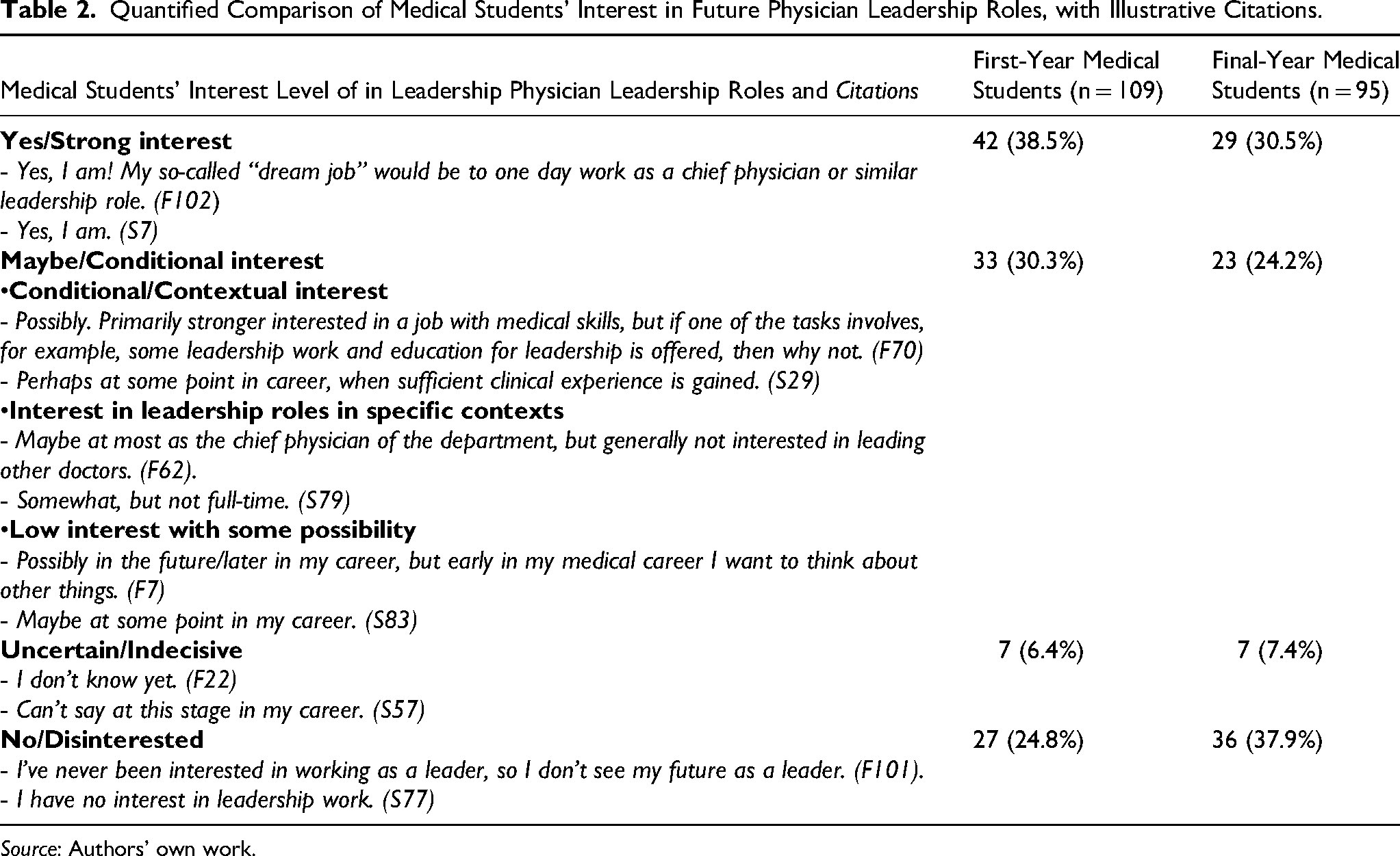
Quantified Comparison of Medical Students' Interest in Future Physician Leadership Roles, with Illustrative Citations.
Source: Authors' own work.
The reliability and validity of the study were reinforced through several measures. The sampling approach ensured robust representation of the target population by inviting all first- and final-year medical students from the 2021 cohorts to participate. A survey methodology was selected for its efficiency in gathering comprehensive data within a short timeframe. 44 Before deployment, the survey underwent pretesting by the authors to evaluate the clarity and relevance of the items and identify potential ambiguities or challenges in interpretation. This feedback process helped ensure the questionnaire's relevance, clarity, and comprehensibility for the study population.37,44 All the authors, who represented different academic backgrounds, independently reviewed the data, cross-checked interpretations, and discussed the results until a consensus was reached, thereby enhancing triangulation and reliability. 37
Ethics Statement
This study complies with both national and international ethical standards for non-medical research involving human participants, aligning with the guidelines established by the Finnish National Board on Research Integrity (TENK, 2019) and the European Union's data protection regulations. 45 In accordance with Finnish law and ethical guidelines, the study did not require approval from an ethics committee. Authorization was granted by the Faculty of Medicine under current policies, and a statement from the Ethics Committee of Human Sciences at the University of Oulu is provided in Appendix 2. The data are available from the authors upon reasonable request. The students received explicit instructions outlining the study objectives, voluntary participation, confidentiality, and anonymity assurances, with the right to withdraw at any time. Informed consent for participation and data usage was acquired from all participants. Data analysis was performed without the use of personal identifiers, and no incentives were offered for participation.
Results
Among 116 first-year medical students, 94% (n = 109) participated in the survey, with the majority (n = 94/81.0%) being under the age of 25. Among the 109 final-year medical students surveyed, 87% (n = 95) participated, most of whom (n = 86/81.1%) were within the 25-30 age range (Table 3).
Background Variables of the Respondents.

Source: Authors' own work.
Through inductive content analysis, several themes emerged regarding interest in leadership roles. First-year medical students demonstrated strong interest, potential interest, uncertainty, and disinterest in leadership, whereas final-year students exhibited strong interest, conditional interest, and disinterest in leadership roles. Compared with first-year students, final-year students also provided more definitive responses regarding their interest in leadership roles (Table 1).
Many first-year students perceived leadership as a natural extension of their career paths, aspiring to positions such as chief physician and demonstrating a strong personal affinity for leadership roles. These aspirations were often grounded in prior leadership experiences before entering medical school, with students regarding leadership as an integral component of their future professional identity (eg, “Yes, I am; I have worked as a supervisor for several years” (F49)). In both groups, some students expressed a preference for context-specific leadership roles or part-time leadership positions and indicated greater interest if supported by appropriate leadership education.
A minority of students in both groups was uncertain about their interest in leadership, often remarking that it was premature to make a definitive career decision. Disinterest in leadership roles was more prevalent among final-year students than among first-year students. Many in the final-year cohort prioritized direct patient care, regarding leadership responsibilities as a potential distraction from clinical work. While interest in leadership was conditional for some final-year students, others had clarified their views, often conceiving of leadership more as collaborative engagement within clinical teams rather than as hierarchical authority. A summary of the main themes and results from the inductive content analysis of first-year and final-year medical students’ responses regarding interest in leadership roles, including a comparison between the cohorts, is presented in Table 1.
In the quantification, among first-year students, 38.5% expressed strong interest in leadership roles, whereas 30.5% of final-year students expressed strong interest. Conditional interest was slightly greater among first-year students (30.3%) than among final-year students (24.2%). Notably, disinterest in leadership roles was higher among final-year students (37.9%) compared with first-year students (24.8%). Persistent uncertainty about leadership aspirations was similar, with 6.4% of first-year and 7.4% of final-year students undecided. A comparative summary of the quantified responses from first-year and final-year medical students to the question “Would you be interested in working as a physician leader in the future?” is presented in Table 2.
In comparison, the results of both the inductive content analysis and the quantification analysis show that first-year students demonstrated greater enthusiasm for leadership roles, whereas final-year students were more reserved, often citing the challenges of leadership responsibilities and a preference for clinical work. Additionally, final-year students provided more definitive answers regarding their interest in leadership roles compared with first-year students. In both cohorts, conditional, contextual, or potential interest, or uncertainty regarding leadership, was observed, suggesting that clinical experience tends to solidify students’ positions into either interest or disinterest.
Discussion
This study aimed to examine first- and final-year medical students’ interest in becoming physician leaders, with a focus on how these interests differ across stages of medical education. The results reveal differences in leadership interest between first- and final-year medical students. The following sections discuss these findings in more detail, and in relation to existing literature and consider the implications for leadership education within medical curricula.
Interest in Leadership
While both groups included students who expressed strong interest in leadership roles, many first-year students viewed leadership as a natural progression in their careers, aspiring to roles such as chief physician and considering their previous leadership experiences to be central to their professional identity. This contrasts with most earlier studies, which reported limited enthusiasm for leadership among medical students, 25 although some research conducted a decade ago suggested that medical students may be more receptive to leadership education than previously assumed. 46
The persistence of conditional interest among final-year students implies that while some students solidify their views on leadership, others remain ambivalent, possibly influenced by their evolving professional and clinical experiences. They also viewed leadership more as collaborative involvement within clinical teams rather than as occupying a hierarchical role. This finding aligns with prior studies indicating that while medical students may be receptive to team leadership, they are less inclined toward formal leadership positions. 25 Some students expressed an interest in leadership within specific contexts, such as serving as heads of departments or undertaking part-time leadership roles, without aspiring to assume full-time leadership positions. This conditional interest may reflect a preference for tailored leadership opportunities or more targeted training. Targeted leadership development programs during medical education could also sustain interest in leadership and support students’ aspirations and preparedness for future leadership roles. Exposure to varied leadership models—including team-based, clinical, and administrative roles 47 —as well as opportunities for interdisciplinary collaboration, 48 may help undecided students identify pathways that align with their professional goals. Furthermore, previous studies indicate that leadership education can be effectively integrated into medical curricula through a combination of didactic coursework, experiential learning, mentorship programs, 48 and online modules embedded within longitudinal programs such as the Physician Leadership Certificate. 49
Disinterest in Leadership
Disinterest in leadership roles was greater among final-year students compared to first-year students. Many final-year students viewed leadership responsibilities as a potential distraction from clinical duties, which may be due to the fact that, in Finland, final-year medical students are permitted, under certain conditions, to work temporarily as doctors in formal physician vacancies, whereas first-year students are not. 35 This reluctance may also reflect broader cultural issues in medical education, where leadership roles are frequently regarded as administrative distractions from patient care. 26 This trend also aligns with studies showing that increased clinical exposure often redirects attention from leadership to direct patient care. 50 As graduation approaches, students may prioritize securing clinical roles and refining medical skills over leadership aspirations. Consequently, this prioritization may reduce the appeal of leadership duties, potentially “handicapping their developing leadership skills.” 50
Many final-year students expressed a preference for direct patient care. Given that medical students’ professional identity formation is a multifaceted process influenced by both clinical and non-clinical experiences, as well as by personal values and beliefs, 32 the increasing demands of clinical practice and the formation of physicians’ identity during medical education may lead to an emphasis on patient care over administrative or leadership responsibilities. As a result, students may perceive their primary identity as clinicians rather than as leaders, prioritizing hands-on practice over leadership. This observation aligns with previous research suggesting that medical students envision themselves primarily as clinicians rather than leaders, experiencing identity conflicts that lead them to prioritize their professional identity as physicians. 22 Professional identity thus influences behaviors and experiences, 51 affecting identity development within social contexts. 52
The difference in leadership attitudes between first- and final-year medical students can also be understood through role socialization, wherein students adopt the norms and values of their chosen profession. 53 In the medical profession, this often involves prioritizing clinical excellence over administrative or leadership roles. A shared feeling of unity within a professional community 52 may have further influenced the results. Additionally, increased clinical exposure likely heightens awareness of the complexities involved in healthcare leadership, prompting more cautious attitudes toward leadership roles. This aligns with prior research showing limited enthusiasm among medical students and residents for pursuing leadership positions, 25 which are often perceived as threats to their clinical identity. 26
Furthermore, diverse clinical experiences can profoundly shape students’ career aspirations and leadership perceptions. Although not explicitly observed in the present study, previous research has demonstrated that exposure to incivility—a prevalent phenomenon in medical training—can adversely affect students’ professional identity by undermining self-esteem, confidence, and their sense of belonging. Such experiences may contribute to disidentification with the clinical environment, resulting in feelings of ineffectiveness, voicelessness, and powerlessness,54,55 thereby diminishing students’ capacity to envision themselves as future physician leaders and discouraging the development of aspirations toward leadership roles.
Uncertainty in Leadership
A small proportion of the students in both groups expressed persistent uncertainty about their interest in leadership roles. This may suggest that some students do not develop a clear stance on leadership even as they advance through medical school. Professional identity forms through ongoing integration of values and behaviors within the self and may be impeded when insufficient or inappropriate support transforms developmental influences into barriers. 32 Consequently, such uncertainty may arise from limited exposure to leadership opportunities or an incomplete understanding of the importance of integrating leadership roles with clinical practice. 56
Many students indicated that it was too early in their careers to make a definitive career choice, reflecting the general ambiguity common during early medical education, where the focus remains on clinical competencies with little emphasis on leadership development. As professional identity formation is a dynamic process shaped by the navigation of personal–professional tensions and supported by institutional strategies, ultimately enhancing practice across individual, institutional, and societal levels, 32 early recognition of the vital role that physician leaders play in healthcare organizations1,2 could cultivate positive attitudes toward leadership among medical students. Furthermore, early leadership education has the potential to foster authentic leadership traits, strengthen professional identity and engagement, and ultimately improve patient care and healthcare outcomes. 57
Practical Implications for Leadership Education in Medical Curricula
Physician leaders play essential roles in healthcare organizations.1,2 However, our study demonstrated that, compared to first-year medical students, final-year medical students exhibited lower levels of strong interest in leadership and higher levels of disinterest. Furthermore, while first-year students demonstrated greater enthusiasm for leadership roles, final-year students expressed challenges associated with leadership responsibilities and a preference for clinical work. Previous research has found no significant differences in medical leadership competencies—such as “demonstrating personal quality,” “working with others,” “managing services,” “setting direction,” and “improving services”—across academic year, gender, or academic performance. 58 In this context, our findings both align with previous literature emphasizing the importance of introducing leadership training early in medical education 49 and highlight the growing need to enhance leadership education within medical curricula.59,60 The findings also point to the importance for flexibility in leadership education. Accordingly, embedding leadership development within clinical practice, rather than presenting it as a separate domain, may help avoid overcrowding the undergraduate curriculum while reconciling differing perspectives and engage students who might otherwise avoid administrative roles. Providing optional leadership tracks, mentorship opportunities, and exposure to diverse leadership experiences could support students in gradually developing confidence and leadership competencies. 48 In addition, early exposure to leadership training or shadowing experiences may help students more effectively evaluate whether leadership aligns with their career aspirations.
Strengths, Limitations, and Future Research
A strength of this study is its mixed-methods approach, 61 which uses high response rate data from both first-year (94%, 109/116) and final-year (87%, 95/109) medical students. The use of inductive content analysis allowed themes to emerge naturally from participants’ responses, providing valuable qualitative insights into leadership interest. Additionally, we presented a clear, reproducible method for the quantification of qualitative data. However, as the data were drawn from only one university, the results may not be fully generalizable to medical students at different stages, locations, or institutions. Cohorts may differ in optimism or perspectives, and generational shifts, along with the impact of the COVID-19 pandemic, may have influenced the results. The cross-sectional design also precludes observation of changes within the same cohort over time. Future studies could address this by exploring perceptions longitudinally as students’ progress through medical school, thereby providing more comprehensive insights. The inductive content analysis of open-ended responses may introduce subjectivity, as interpretive biases could affect categorization. 43 In Finland, final-year medical students are permitted to work temporarily as formal physicians under certain conditions, while first-year students are not, 35 which may have influenced the conceptualization of the physician leader, as it was not explicitly defined. In-depth interviews or focus groups could further enrich the data by revealing motivations and concerns that shape students’ leadership interest. Although the foundations of medical curricula are similar worldwide, results may vary between medical schools with integrated leadership pathways or between countries with different healthcare governance models. Consequently, contextual factors may influence the transferability and/or generalizability of the findings. 62 Finally, converting qualitative data into frequency counts may dilute the nuances of respondents’ experiences. 63 Future studies should evaluate the effectiveness of various leadership development programs within medical curricula.
Conclusion
This study highlights different perspectives on leadership interest among medical students as they advance through their education. First-year students demonstrated greater optimism and enthusiasm for leadership, often viewing it as a natural extension of their careers. In contrast, final-year students increasingly prioritized clinical responsibilities, reflecting the influence of physicians’ identity development and the demands of clinical practice. Compared to first-year medical students, final-year medical students exhibited lower levels of strong interest in leadership and higher levels of disinterest. Although medicine must remain the central focus of the medical curriculum, the essential role of physician leaders in healthcare organizations highlights the need to enhance leadership education within medical curricula. Integrating early and longitudinal leadership education into clinical practice—emphasizing its clinical relevance and alignment with physicians’ identity—rather than treating leadership as a separate domain, may help sustain interest, enable students to assess whether formal leadership roles align with their career aspirations, and better equip future physician leaders.
Footnotes
Acknowledgments
The authors wish to thank the medical students at the University of Oulu for their participation in the study.
Ethical Considerations
This study follows national and international ethics standards for non-medical research with human participants, adhering to guidelines set forth by the Finnish National Board on Research Integrity (TENK, 2019) and the data protection regulations of the European Union. According to Finnish law and ethical guidelines, the study did not require clearance from an ethics committee. Permission for the study was granted by the Faculty of Medicine in accordance with current policies. The statement from the Ethics Committee of Human Sciences at the University of Oulu is available in Appendix.
Consent to Participate and Publication
The students received written explicit instructions outlining study objectives, participation voluntariness, confidentiality, and anonymity assurances, with the right to withdraw at any time. Written consent for participation, data use to publish was obtained from all participants, with data analysis conducted without personal identifiers, and no incentives were provided for participation.
Author Contributions
All authors have made substantial contributions to the conception and design of the work, as well as to the acquisition, analysis, and interpretation of data. All authors have also significantly contributed to drafting the work and critically revising it for important intellectual content. Each author has given final approval for the version to be published and has agreed to be accountable for all aspects of the work, ensuring that questions related to the accuracy and integrity of any part of the work are appropriately investigated and resolved.
SHT contributed in study design, data analysis and interpretation, manuscript drafting and revision, final approval of the version to be published. TT contributed in study design, data collection, analysis and interpretation, manuscript drafting and revision, final approval of the version to be published. PK contributed in study design, data analysis and interpretation, manuscript drafting and revision, final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data is available from the authors upon reasonable request. No material from other sources has been used.