
Abstract
Background
In the United States, poisonings account for the highest number of preventable injury deaths and children disproportionately account for the largest number of poisoning exposures. There is limited exposure to toxicology education. We developed and evaluated an asynchronous case-based, interactive, online pediatric toxicology curriculum to augment foundational knowledge and enable pattern recognition in the diagnosis and management of pediatric toxic exposures.
Methods
We developed 12 cases based on cholinergic, anticholinergic, sympathomimetic, sedative-hypnotic, opioid, and serotonergic toxidromes using Rise 360 e-learning application. Participants were recruited from Accreditation Council for Graduate Medical Education-accredited pediatrics, internal medicine–pediatrics, and emergency medicine residencies and pediatric critical care and emergency medicine fellowship programs across the United States. They completed a precurriculum survey including baseline information on their training and prior educational exposure to toxicology as well as a pre- and post-curriculum self-assessment of their comfort level in the recognition, work-up, differential diagnosis, differentiation, and management of a toxic exposure. Participants also completed a 10-question pre- and posttest and provided qualitative feedback on the curriculum.
Results
Of the 238 participants who initially signed up for the course, 152 (64%) completed the pre-curriculum survey and test, and 52 (22%) completed the curriculum, which was available for 6 months. Across all participants, patient encounters were the most common exposure (197, 83%) and an online or web-based curriculum was the least common (11, 5%). Although participants did not have a significant difference in subgroup analysis and test results after completion of the study, collectively study participants demonstrated a significant improvement in comfort across all 5 domains which were assessed.
Conclusion
We developed and evaluated the first pediatric-focused interactive online case-based toxicology curriculum. Self-reported comfort measures on the recognition and management of pediatric toxic exposures improved across various specialties with this curriculum. The curriculum can augment program efforts in improving toxicology education.
Introduction
In the 2023 Annual Report of the American Association of Poison Control Centers’ National Poison Data System, children accounted for 55.66% of the 2 080 659 total poisoning exposures. Children less than 6 years of age account for the majority of the pediatric exposures at 72%. 1 In 2023, 2103 children aged 18 and under died from poisoning exposures. 2 Among adolescents, intentional ingestions are the most common cause of poisoning exposures and are associated with a heightened risk of lethality. 1 This trend is particularly concerning given the rising suicide rates in this age group, with suicide now ranking as the second leading cause of death among children aged 10 to 19. Poisoning exposures have emerged as a significant contributing factor to this growing public health crises.2,3 Poisoning exposures accounted for over $34 billion in combined loss from medical cost and quality of life. 4 Pediatric populations are especially vulnerable as seen after the legalization of cannabis and susceptibility to social media challenges.5–7
Physician-trainees with various backgrounds provide vital care to pediatric patients and their families during the prevention, diagnosis, management, and post acute care treatment of patients with toxic exposures. Importantly, toxicology is a required content domain for pediatric, pediatric emergency medicine, pediatric critical care, and emergency medicine training.8–11 Toxicology education must be robust for physicians providing care to pediatric patients. However, the literature on a standardized pediatric toxicology curriculum for the acute management of patients is limited. 12 Toxicology education has traditionally been emphasized in the training of emergency medicine residents. Patients with poisoning exposures are routinely evaluated and treated in the emergency department.13,14 A prior needs assessment focused on emergency medicine residents demonstrated that less than 50% of the residents surveyed were comfortable with their toxicology education in preparation of their board exams with a significant number reporting discomfort with the identification, treatment, and management of certain toxidromes. Some of the barriers identified included a lack of access to support services including proximity to a poison control center or faculty with toxicology education.15,16
A broad scope of teaching modalities have been used to educate trainees in the management of pediatric poisonings, including simulation-based curriculum to traditional lecture-based modalities and even a virtual toxicology escape room during the COVID-19 pandemic.15,17 Beyond these, the Global Educational Toxicology Project and the Global Education Toxicology Toolkit help to provide innovative teaching modalities for a broader health provider audience in low- and middle-income countries with limited toxicology resource support including poison control centers.17,18 However, given the lack of a published standardized pediatric toxicology curriculum for physician-trainees, we developed and piloted a case-based interactive, self-paced online curriculum to augment foundational knowledge and principles and enable pattern recognition in the diagnosis and appropriate management of pediatric toxic exposures. The aim of this tool is to increase accessibility to toxicology education, ameliorating the limited access to resources such as faculty with toxicology education or proximity to a poison control center.
Methods
Course Description
An interactive case-based curriculum was originally designed in Rise 360, an e-learning based platform. Rise 360 is a collaborative authoring web application that can be used to design courses. It provides various layouts and tools to deliver content and test knowledge that easily adapts to various screens for convenience (eg tablets, phones, and computers). 19 The curriculum was focused on the 6 basic toxidromes: sedative-hypnotic, opioid, sympathomimetic, serotonergic, cholinergic, and anticholinergic. The cases, surveys, and tests were developed by a pediatric emergency fellow together with a medical toxicologist who is the medical director of a poison control center. The materials were then reviewed by a pediatric emergency medicine fellowship director. Twelve cases with specific learning goals were subsequently available to participants through the Sharable Content Object Reference Model (SCORM) cloud. Courses with the specific SCORM file coding can be uploaded and distributed to this web application which serves as a learning management system. 20 The cases were designed to be interactive. For each case, a vignette was provided and trainees could input free-text responses to questions or choose from multiple-choice options depending on the question. Additional information such as the differential, test results, and diagnoses were sequentially revealed after participants submitted their response in order to help with the next step of each case. Each case was subsequently followed by a didactic section with virtual flashcards to review a broad differential and with a review sheet focusing on the basics of the management of the toxidrome. The learning pearls were designed to repetitively highlight specific basic principles of toxicology management. The flow of the cases and the didactic section have been included in the Supplemental appendix (Figure S1) and the curriculum can be accessed at this link (https://app.cloud.scorm.com/sc/InvitationConfirmEmail?publicInvitationId=c8dfc0a6-a39a-451f-b732-16f2f4c6a528). Key principles highlighted included the assessment and management of the threatened airway, breathing, circulation, decontamination, skin exposure, the appropriate selection and use of time-sensitive antidotes, and poison control contact information.
Participants and Setting
A pre- and post-evaluation study was performed over a 6-month period between August 2022 and January 2023 to assess the comfort and knowledge of various learners in recognizing and managing a toxic exposure in a pediatric patient. Eligible participants included residents from pediatrics, combined internal medicine–pediatrics, and emergency medicine programs, as well as fellows from pediatric critical care and pediatric emergency medicine programs. These subspecialties were included in the study because of their higher likelihood of managing pediatric poisoning cases in settings such as the emergency department, inpatient units, or the intensive care unit. Participants were identified and recruited via a database of program directors of the Accreditation Council for Graduate Medical Education (ACGME) fellowship and residency programs across the United States. Study recruitment emails were sent out to all program directors to disseminate to their residents and fellows. Subsequently weekly reminder emails were sent out to the participants who initially registered for the curriculum on SCORM cloud to obtain maximum participation. The study window was originally planned for 2 months, but was extended to 6 months to maximize curriculum and survey completion.
Data Collection and Analysis
Study data were collected and managed using Research Electronic Data Capture (REDCap) tools hosted at Johns Hopkins University.21,22 Self-administered pre- and post-curriculum surveys completed by study participants included information on trainee year, specialty, toxicology exposure and their comfort level in the recognition, generation of a differential diagnosis, work-up, and the management of a toxic exposure. The measures of comfort were obtained on a 5-point Likert scale. The surveys were created for this curriculum. Surveys collected information on training background and formal and informal toxicology education opportunities available across the programs to provide a background assessment of available needs. In addition, pre- and posttests including 10 multiple-choice questions each were administered as part of the curriculum. A free-text feedback option was included on the survey form. In addition, pre- and posttests with 10 questions each were accessible via REDCap prior to and after completion of the pediatric toxicology curriculum over the duration of the study. The pre- and post-curriculum surveys and the tests are included in the Supplemental Appendix (S2-S5).
We hypothesized that if trainees had easy access to a pediatric toxicology curriculum, their self-reported ability to recognize and manage common toxic exposures in children after completion of the curriculum would improve. The primary outcome was to determine whether test scores improved significantly after completion of the curriculum. The secondary outcome was to assess whether learners demonstrated a statistically significant improvement in self-reported comfort with recognizing a toxic exposure, generating differentials, differentiating toxidromes, developing a work-up and a toxidrome-specific management plan for the 6 basic toxidromes.
Statistical Analysis
Data were first examined for completeness and duplicates, and incomplete surveys were excluded from analysis. All data, including demographic information, pre- and posttest results, and comfort levels were summarized with descriptive statistics including frequencies and percentages. Normally distributed data were summarized using means and standard deviations whereas non-normally distributed data were described using medians and interquartile ranges. Wilcoxon rank sum and paired t-tests were respectively utilized to determine any significant difference between pre- and posttests in the independent samples of participants who completed both tests and for the matched results of the individual participants who completed both tests. Perceived comfort level and test performance were compared by training program year and type and summarized with a Kruskal–Wallis test. A Bonferroni correction was applied, such that only results with P-values <.0038 (13 tests divided by 0.05) were considered to be statistically significant. We conducted a posthoc power analysis for our primary outcome, with a 2-sided alpha of .05 and 80% power.
Additionally, participants were given the opportunity to provide free-text feedback after completion of the curriculum. The free-text responses were not qualitatively analyzed as part of the study design. However, the common themes are summarized in the Supplemental Appendix (S6). This education study was considered exempt after IRB review by the Johns Hopkins University Institutional Review Board and was funded by a Johns Hopkins Medical Alumni grant.
Results
The curriculum was sent out to all ACGME-accredited pediatrics, internal medicine–pediatrics, emergency medicine residencies and pediatric emergency medicine and pediatric critical care fellowships in the United States. A total of 238 participants initially registered for the curriculum, 152 (64%) completed the precurriculum surveys, 117 (49%) completed the precurriculum test, 52 (22%) completed the post-curriculum survey, and 47 (19.7%) completed the post-curriculum test, as indicated in Figure 1. Pediatric critical care fellows and pediatric emergency medicine participants predominated in the study as demonstrated in Figure 2 with the following distribution of participants: pediatrics (29, 19%), internal medicine–pediatrics (5, 3.4%), emergency medicine (15, 9.8%), pediatric critical care (40, 26.3%), pediatric emergency medicine (60, 39.5%), and other (3, 2%). Patient encounters were the most common exposure (83%) to toxicology education, followed by a didactic lecture from the training program (61%) and self-directed learning (51%) while an online or web-based curriculum was the least common (5%) across all study participants as indicated in Figure 3 and again in Figure 4 by specialty.

Study flowchart.

Distribution of study participants by specialty training with pediatrics (Peds), combined internal medicine–pediatrics (IM/Peds), emergency medicine (EM), pediatric critical care medicine (PCCM), pediatric emergency medicine (PEM), and other.

Distribution of educational modalities across all specialties.
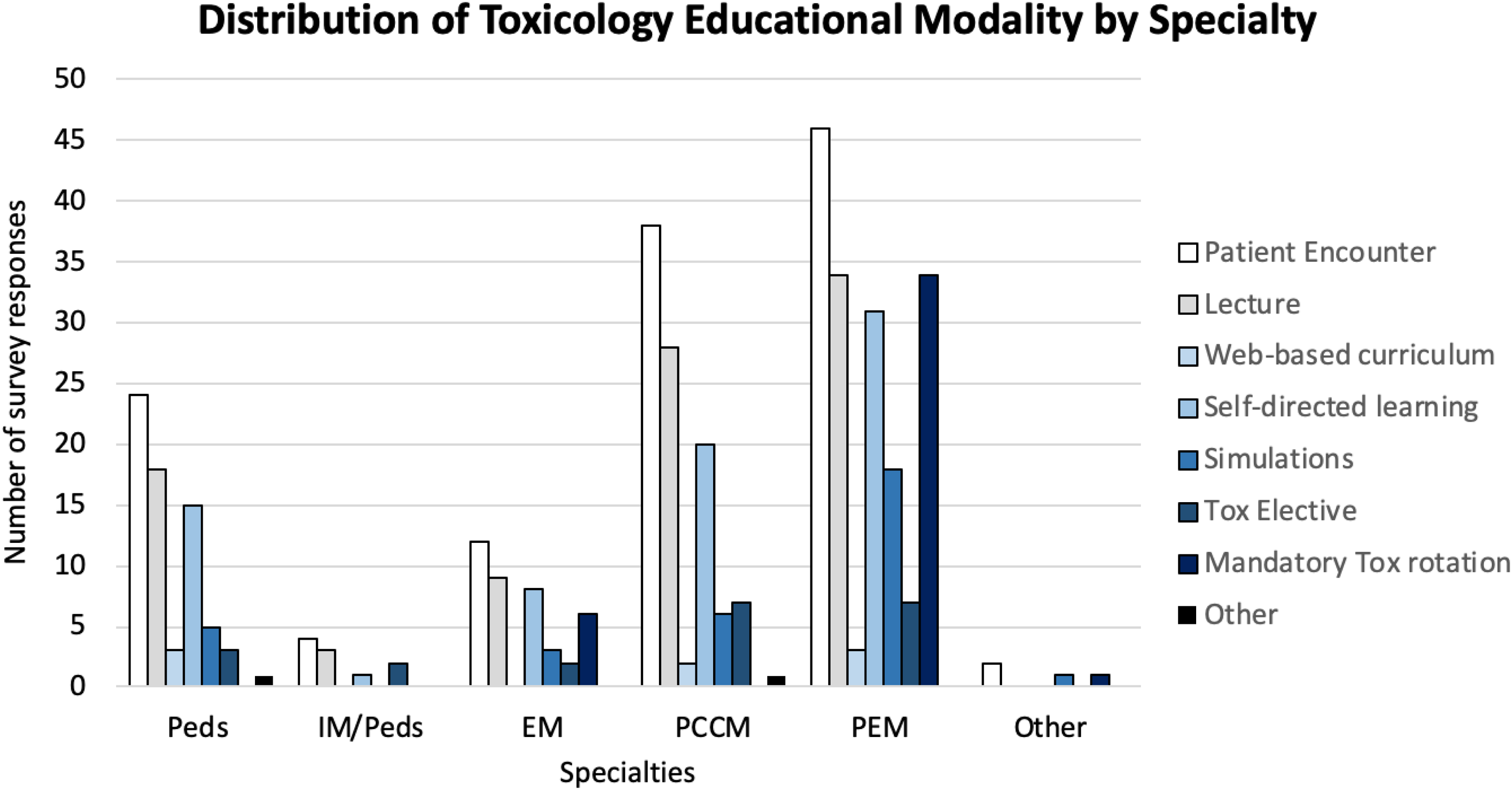
Distribution of educational modalities by specialty training: pediatrics (Peds), combined internal medicine–pediatrics (IM/Peds), emergency medicine (EM), pediatric critical care medicine (PCCM), pediatric emergency medicine (PEM), and other.
After completion of this study, survey participants reported statistically significant positive change in their perceived comfort level in the recognition of a toxic exposure, the ability to generate a differential, differentiate toxidromes, and develop a general work up as well as a toxidrome-specific management plan (Table 1). There was no statistically significant change in test performance as shown in Table 1. In a paired t-test limited to participants that completed both surveys (n = 23), the difference in total scores prior to and after completion of the study was not statistically significant. Our posthoc power analysis for n = 23 pairs found that we had 80% power to detect a change in test scores of ±1.4, far higher than our observed change of −0.35, for which we only had 10.8% power.
Pre- and Post-curriculum Comfort Domains and Test for Study Population.
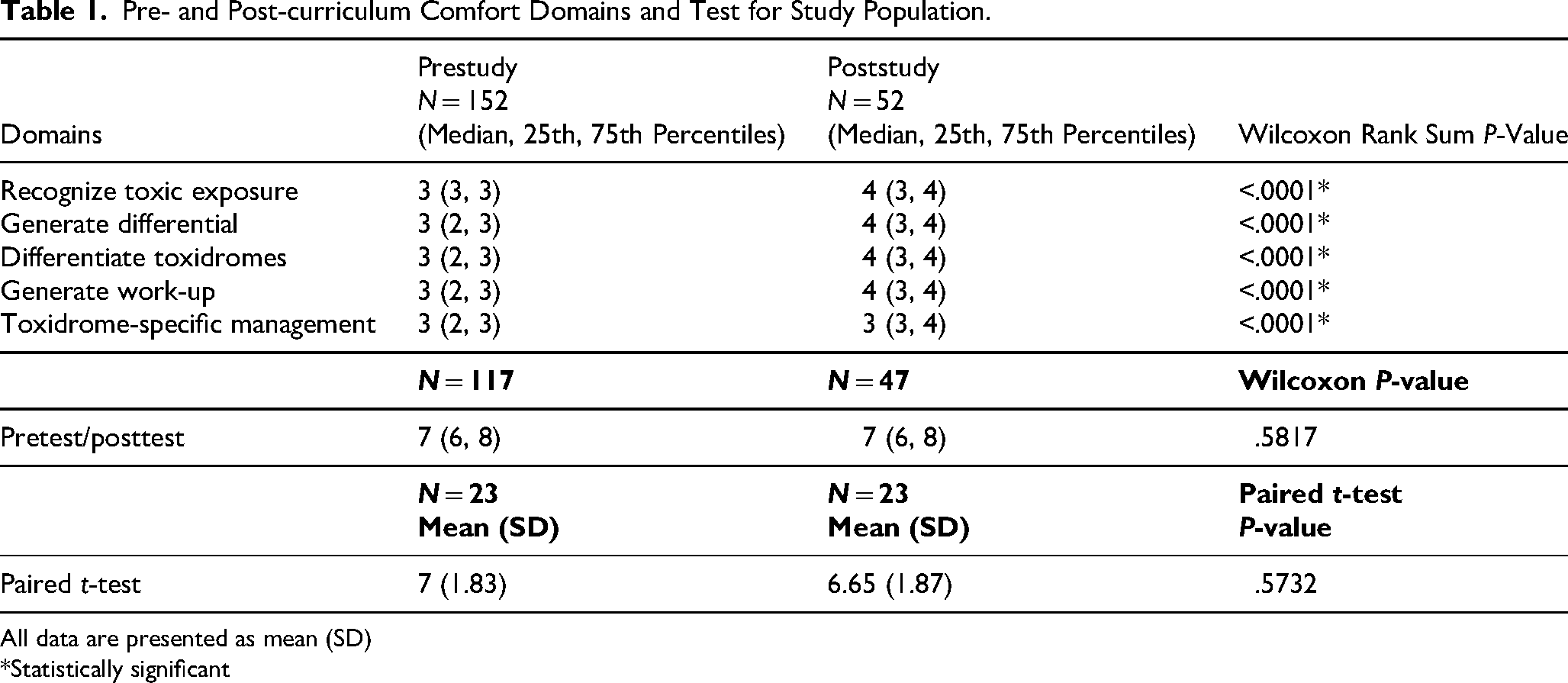
All data are presented as mean (SD)
*Statistically significant
As expected, trainees above their third year of postgraduate training year (PGY) reported the highest comfort level prior to completion of the curriculum. There was a statistically significant difference in perceived comfort across all domains and in precurriculum test performance prior to completion of the curriculum across the trainee groups but the difference across domains did not increase consistently by the PGY group. There was no significant change in test performance after completion of the curriculum as demonstrated in Table 2.
Pre- and Post-curriculum Comfort Level Across Domains and Test Performance by Postgraduate Year (PGY).

All data are presented as mean (SD)
*Statistically significant
Pediatric residency trainees had the lowest perceived level of comfort across all survey questions while trainees in combined internal medicine–pediatrics programs generally had the highest level of perceived comfort across the majority of domains. While pretest scores were statistically significantly different across programs, there was no statistically significant difference across the different subspecialty groups after completion of the curriculum, as illustrated in Table 3. Across all domains, trainees demonstrated a statistically significant difference in their perceived comfort prior to completion of the curriculum. However, there was no statistically significant difference in perceived comfort in any domain across the emergency medicine, pediatric critical care medicine, pediatric emergency medicine, and pediatric groups after completion of the curriculum. However, there was insufficient data to demonstrate a meaningful difference between subspecialty groups.
Pre- and Post-curriculum Comfort Level Across Domains and Test Performance by Specialty.
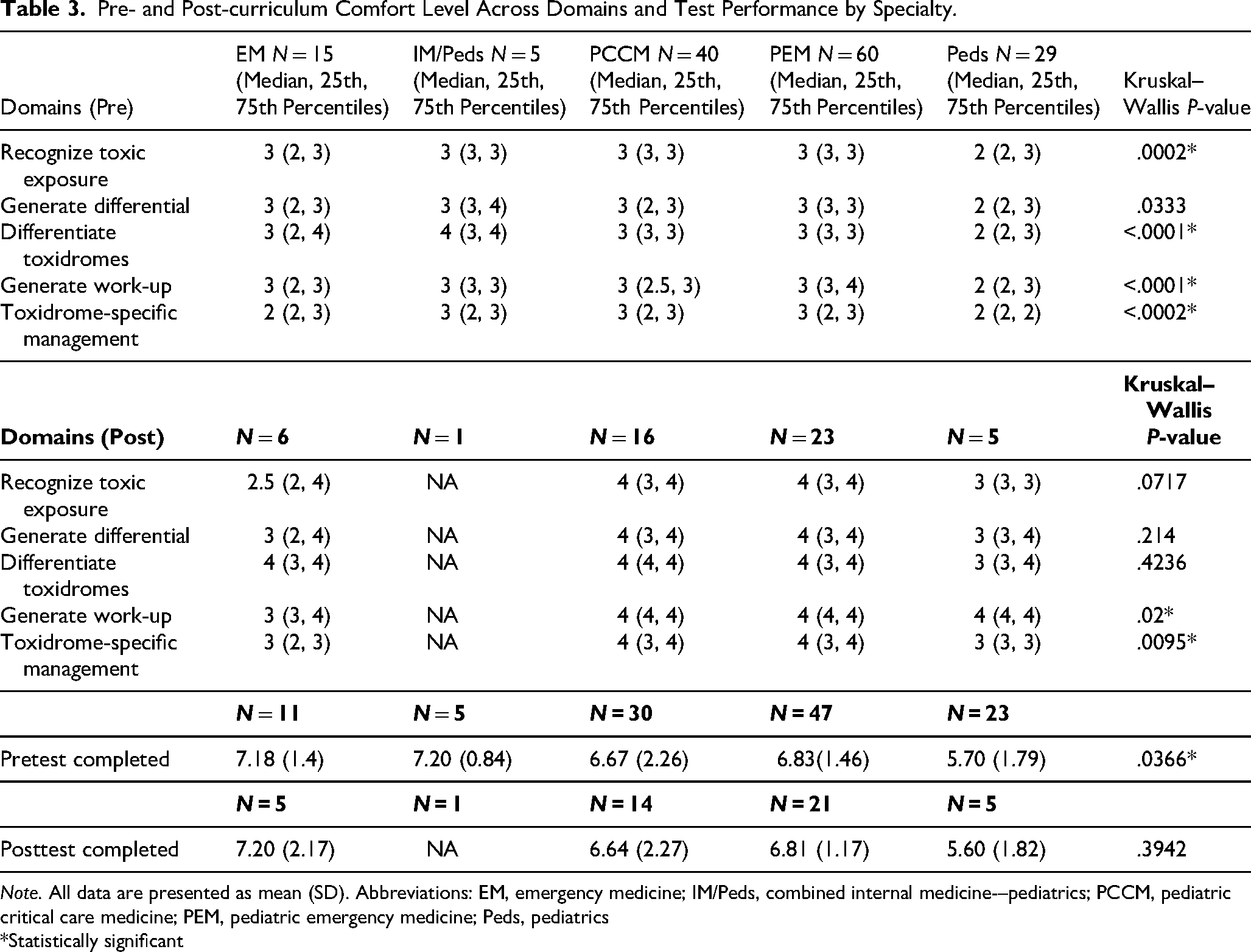
Note. All data are presented as mean (SD). Abbreviations: EM, emergency medicine; IM/Peds, combined internal medicine-–pediatrics; PCCM, pediatric critical care medicine; PEM, pediatric emergency medicine; Peds, pediatrics
*Statistically significant
Participants provided additional free-text feedback on the pediatric toxicology curriculum. The feedback was categorized into 5 main themes. First, participants found the free-text responses had to be specific and recommended using less free-text answers or to opt for primarily multiple-choice answers for the course. In addition, they recommended incorporating more cases such as “beta blockers, calcium channel blockers, other toxic exposures, salicylates, iron and acetaminophen” or nontoxicological cases and increasing the complexity of the cases. The third category focused on highlighting abnormal findings and incorporating more discussion on toxicology management.
Lastly, the feedback was categorized as either positive or miscellaneous. A participant liked the “repetitive case-based learning with summaries” and another trainee reported enjoying the “case-based scenario and progression from developing differential and management plan.” Some of the miscellaneous suggestions included adding mnemonics as part of the learning tools, decreasing the repetitive nature of the curriculum, and incorporating videos. No qualitative analysis was performed for the free-text responses. However, the responses were summarized and are included in the Supplemental appendix (S6).
Discussion
We describe our experience with the dissemination and assessment of the first interactive pediatric-focused online toxicology curriculum across multiple trainee programs. The overall goal of this study was to provide a tool to increase the exposure of both residents and fellows who take care of children to be able to promptly recognize and manage toxic exposures. Our specific aims with the curriculum were to improve pattern recognition for potential toxic exposures using clinical signs and symptoms and the physical exam including vital signs and to reiterate basic management principles including supportive care and antidotal therapy. Although participants did not have a significant difference in subgroup analysis and test results after completion of the study, collectively study participants demonstrated a significant improvement in comfort across all 5 domains which were assessed.
Trainees have limited opportunities for toxicology education. Previous work in this field has largely focused on the toxicology education of emergency medicine residents.3,16 Across all the programs that were surveyed in this study, emergency medicine residents were the most likely to have access to more formalized toxicology education. Yet, Ebersole and colleagues demonstrated that many emergency medicine residents were not comfortable with their toxicology experience. 23 Our baseline data revealed a significant gap in training across pediatrics, combined internal medicine–pediatrics, pediatric critical care, and pediatric emergency medicine programs. Although participants reported that patient encounters were their most frequent educational opportunity, Mittiga and colleagues have shown even at a high-volume center, pediatric residents’ encounters with acutely poisoned patients did not meet the ACGME requirements. 24 Especially with an online or web-based program cited as the least available modality for education, this curriculum meets a need by circumventing some of the barriers to toxicology education. It can also be adaptively delivered to best suit programmatic needs (eg asynchronously on a toxicology rotation or as an independent study resource).
There was no statistically significant difference in test performance across the PGY group after completion of the 10-question tests. We hypothesized that the number of questions were not sufficient to discriminate in test performance. Boyd demonstrated that the introduction of a standardized toxicology curriculum helped to improve the toxicology scores for emergency medicine residents on their in-training exams, a surrogate marker for board exam performance. However, the curriculum included in Boyd's study included “one-on-one case-based teaching with a board-certified toxicologist, taking toxicology consultation call” and assessing both adult and pediatric patients with toxic exposures in the outpatient clinic, emergency department, floor, and intensive care unit. 25 Many of those opportunities are ideal for learning but as demonstrated by the precurriculum survey were not easily accessible to majority of trainees.
As expected, trainee comfort across the different surveyed domains positively correlated with advancing years in their training. Even still, this study demonstrated a statistically significant improvement in comfort level across the surveyed domains across all years of training and across specific specialty training programs. Altogether, this indicates that the available pre- and posttest questions could be expanded in number and made more discriminatory to better assess comprehension of foundational principles and retention of toxidrome-specific information. Although trainees’ perceived comfort does not necessarily translate to competence, the improvement in their perceived comfort suggests that having standardized curriculum can improve familiarity and provide a foundation for a subject matter that can appear esoteric and limited primarily to the expertise of toxicologists.
Limitations
This study had several limitations. Our conclusions are limited by the small sample size of study participants and lower response rates which may not be representative of the broader experiences of all trainees across the different surveyed specialties across ACGME-accredited programs in the United States. Study recruitment emails were sent out to all program directors to disseminate to their residents and fellows. Efforts were made to obtain maximum participation by sending out weekly reminder emails to the participants who initially registered for the curriculum on SCORM cloud. In addition, the study was extended from 2 to 6 months to allow for curriculum completion.
We did not achieve the sample size required by our a priori power analysis (n = 385) which was a limitation of the study. Despite the positive feedback that we received on the curriculum, only 23 participants who completed the curriculum submitted both the pre- and post-completion survey responses as well as the pre- and posttests. As a result, the study was underpowered and we did not find statistically significant results in test performance after completion of the curriculum, as evidenced by our paired t-tests and by extension in our subgroup analysis by PGY and subspecialty. Depending on the available resources within a specific program, the curriculum may be a redundant tool for some trainees. However, our study aligns with prior study findings demonstrating a dearth of dedicated toxicologic educational resources for trainees in residency and by extension, fellowship. 15 A study with a larger number of participants is needed to further investigate changes in test performance from this curriculum.
Furthermore, the pre- and post-curriculum surveys were specifically created for this study to align with the research aims. However, as a limitation, they were not previously validated. Although we had statistically significant changes across our domains, it may not have accurately captured learners’ perceptions of their comfort in the recognition and management of pediatric toxic exposures and any subsequent improvements after completion of the curriculum.
The content of the curriculum was focused on the 6 basic toxidromes in order to initially build a tool with a succinct amount of information thereby increasing the odds of completion by trainees. However, the potential toxic exposures for children far exceed the basic toxidromes and epidemiology of pediatric toxic exposures continues to evolve. Therefore, this curriculum can serve as a foundation to build additional cases and more complex toxidrome presentations. In addition, the cases can be reviewed by a broader group of toxicologists and nontoxicology cases can be included for improved fidelity of the curriculum.
Lastly, this study did not focus on user experience with the e-learning platform but the qualitative feedback provided by trainees can be adapted to make the interactive course more user-friendly. For example, trainees had commented on the issue of fine discrimination of their free-text answers by the software. In future iterations of this curriculum, trainees will be given multiple-choice options.
Conclusion
We demonstrated an improvement in trainee comfort with the recognition and management of pediatric toxic exposures with an online, asynchronous pediatric-focused toxicology curriculum. We identified opportunities to better assess knowledge retention and improve on the content included in the curriculum as well as the functionality of an e-learning platform to continue to engage learners. This will help to ameliorate some of the barriers in obtaining robust toxicology education and ultimately serve to provide medical care for a vulnerable population.
Supplemental Material
sj-png-1-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-png-1-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-2-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-3-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-4-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-5-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-5-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-6-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-6-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-7-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-docx-7-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-8-mde-10.1177_23821205251411213 - Supplemental material for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum
Supplemental material, sj-pdf-8-mde-10.1177_23821205251411213 for Assessment of an Interactive Online Asynchronous Pediatric-Focused Toxicology Curriculum by Roselyn Appenteng, Thuy Ngo, Lisa Yanek and Rebecca Bruccoleri in Journal of Medical Education and Curricular Development
Footnotes
Author Note
The first author completed this research at The Johns Hopkins University School of Medicine but is currently affiliated with Emory University School of Medicine.
Ethical Considerations
This study was approved by the Johns Hopkins School of Medicine Institutional Review Board (Approval no. IRB00311895) on June 2nd, 2022.
Consent to Participate
This study was approved as exempt. Participants consented to participate in this study by opting in to complete the curriculum and associated surveys and participant information submitted in the surveys were de-identified.
Author Contributions
Roselyn Appenteng, Rebecca Bruccoleri, and Thuy Ngo, were responsible for conceptualization and methodology. Roselyn Appenteng, was responsible for the investigation. Roselyn Appenteng, Rebecca Bruccoleri, and Lisa Yanek, were involved in the formal analysis of this paper. All authors were involved in the preparation, review, and editing of this manuscript
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Johns Hopkins Medical Alumni grant.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.