
Abstract
Introduction
Case-based learning (CBL) is a newer modality of teaching healthcare. In order to evaluate how CBL is currently used, a literature search and review was completed.
Methods
A literature search was completed using an OVID© database using PubMed as the data source, 1946-8/1/2015. Key words used were “Case-based learning” and “medical education”, and 360 articles were retrieved. Of these, 70 articles were selected to review for location, human health care related fields of study, number of students, topics, delivery methods, and student level.
Results
All major continents had studies on CBL. Education levels were 64% undergraduate and 34% graduate. Medicine was the most frequently represented field, with articles on nursing, occupational therapy, allied health, child development and dentistry. Mean number of students per study was 214 (7–3105). The top 3 most common methods of delivery were live presentation in 49%, followed by computer or web-based in 20% followed by mixed modalities in 19%. The top 3 outcome evaluations were: survey of participants, knowledge test, and test plus survey, with practice outcomes less frequent. Selected studies were reviewed in greater detail, highlighting advantages and disadvantages of CBL, comparisons to Problem-based learning, variety of fields in healthcare, variety in student experience, curriculum implementation, and finally impact on patient care.
Conclusions
CBL is a teaching tool used in a variety of medical fields using human cases to impart relevance and aid in connecting theory to practice. The impact of CBL can reach from simple knowledge gains to changing patient care outcomes.
Introduction
Medical and health care-related education is currently changing. Since the advent of adult education, educators have realized that learners need to see the relevance and be actively engaged in the topic under study.
1
Traditionally, students in health care went to lectures and then transitioned into patient care as a type of
There is not a set definition for CBL. An excellent definition has been proposed by Thistlewaite et al in a review article. In their 2012 paper, a CBL definition is “The goal of CBL is to prepare students for clinical practice, through the use of authentic clinical cases. It links theory to practice, through the application of knowledge to the cases, using inquiry-based learning methods”. 3
Others have defined CBL by comparing CBL to a similar yet distinct clinical integration teaching method, problem-based learning (PBL). PBL sessions typically used one patient and had very little direction to the discussion of the case. The learning occurred as the case unfolded, with students having little advance preparation and often researching during the case. Srinivasan et al compared CBL with PBL
4
and noted that in PBL the student had little advance preparation and very little guidance during the case discussion. However, in CBL, both the student and faculty prepare in advance, and there is guidance to the discussion so that important learning points are covered. In a survey of students and faculty after a United States medical school switched from PBL to CBL, students reported that they enjoyed CBL better because there were fewer
CBL is currently used in multiple health-care settings around the world. In order to evaluate what is now considered CBL, current uses of CBL, and evaluation strategies of CBL-based curricular elements, a literature review was completed.
This review will focus on human health-related applications of CBL-type learning. A summary of articles reviewed is presented with respect to fields of study, delivery options for CBL, locations of study, outcomes measurement if any, number of learners, and level of learner's education. These findings will be discussed. The rest of this review will focus on expanding on the article summary by describing in more detail the publications that reported on CBL. The review is organized into definitions of CBL, comparison of CBL with PBL, and the advantages of using CBL. The review will also examine the utility and usage of CBL with respect to various fields and levels of learner, as well as the methods of implementation of CBL in curricula. Finally, the impact of CBL training on patient and health-care outcomes will be reviewed. One wonders with the proliferation of articles that have CBL in the title, whether or not there has been literature defining exactly what CBL is, how it is used, and whether or not there are any advantages to using CBL over other teaching strategies. The rationale for completing this review is to assess CBL as a discrete mode of transmitting medical and related fields of knowledge. A systematic review of how CBL is accomplished, including successes and failures in reports of CBL in real curricula, would aid other teachers of medical knowledge in the future. Examining the current use of CBL would improve the current methodology of CBL. Therefore, the aims of this review are to discover how widespread the use of CBL is globally, identify current definitions of CBL, compare CBL with PBL, review educational levels of learners, compare methods of implementation of CBL in curricula, and review CBL reports on outcomes of learning.
Methods
A literature search was completed using an OVID© database search with PubMed as the database, 1946 to August 1, 2015. The search key words were “Case Based Learning, Medical Education”. Investigational Review Board declined to review this project as there were no human subjects involved and this was an article review. A total of 360 articles were retrieved. Articles were excluded for the following reasons: unable to find complete article on the search engine OVID, unable to find English language translation, article did not really describe CBL, article was not medically or health related, or article did not describe human beings. Articles that originated in another language but had English language translation were included.
After excluding the articles as described, 70 of these articles were selected to review for location of study, description of CBL used, human health care-related fields of study, number of students if available, topics of study, method of delivery, and level of student (eg, graduate or undergraduate). Students were considered undergraduate if they were considered undergraduate in their field. For example, medical students were considered undergraduate, because they would still have to undergo more training to become fully able to practice. If the student was in the terminal degree, then that was considered a study of graduate students. For example, nutrition students were listed as graduate students. CBL encounters for both residents and independent practitioners who were in their final training prior to practice were listed as graduates. Residents were listed under graduate medical education. If a group had already graduated, they were listed as graduates. For example, MDs who participated in a continuing medical education (CME)-type CBL were listed as graduate type of student. Articles that did not list the total number of students were included, as one of the purposes of this review was to discover how widespread the use of CBL was globally, and what types of students and types of delivery were used. By including descriptive articles that were not specific, the global use of CBL could attempt to be assessed. Including locations of studies would then help decide whether CBL was isolated from the Western countries or has it truly spread around the world.
In order to review how CBL was used, in addition to where it was used, the method of delivery was assessed. Method of delivery refers to how the total educational content was delivered. Articles were reviewed for description of exactly how material was imparted to learners. Since many authors described their learning methods in detail, an attempt was undertaken to classify these methods. Method of delivery was classified as follows: live was considered a live presentation of the case, this could be a description, a patient, or a simulated patient. Computer or web based meant that the case and content were web based. Mixed modalities meant that more than two modalities were used during presentation. For example, if an article described assigned reading, lectures, small group discussions, a live case-based session, and patient interactions, then that article would be described as mixed modalities.
Method of evaluation of the educational intervention was also reviewed. The multiple ways in which the interventions were evaluated varied. A survey of how the learners viewed the intervention was frequent. Tests of knowledge gained were frequent, and these ranged from written, to oral, to Observed Skills Clinical Examination (OSCE). Another way by which CBL intervention knowledge was evaluated was review of practice behavior in clinicians. These multiple ways to evaluate the introduction of CBL into a curriculum are summarized in a table.
Results are presented in simple frequencies and percentages. SPSS (Statistical Program for the Social Sciences, IBM) version 22 was used for analysis.
Results
All continuously inhabited continents had studies on CBL (Fig. 1). North America is represented with the most with 54.9% of articles, followed by Europe (25.4%) and Asia, including India, Australia, and New Zealand (15.5%). South America had 2.8% and Africa had 1%.5–75
Level of education was undergraduation in 45 (64%) articles and graduation in 24 (34%) articles, with one article having both levels. One study with both faculty and residents was considered as a type of graduate education. The types of fields of study varied (Fig. 2). The most represented field was medicine including traditional Chinese medicine, with articles also on nursing, occupational therapy, allied health, child development, and dentistry. The number of students ranged from 7 to 3105 and the mean number of students was 214. One study reported on the use of teams of critical care personnel, in which it was mentioned that there were three persons per team usually. Thus, the number of students was multiplied: 40 teams x 3 = 120 in total. The total number of students were 9884 from the 46 papers that explicitly stated the number of students.
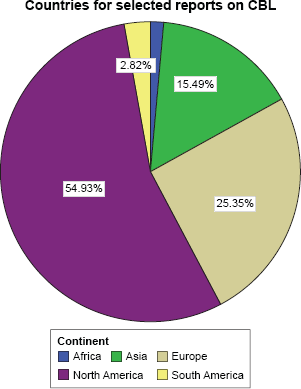
CBL use worldwide.

Fields of study.
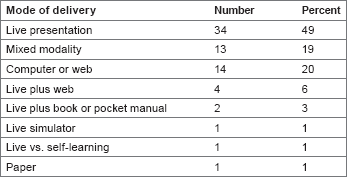
Mode of delivery of CBL.
Methods of delivery also varied (Fig. 3). The most common method of delivery was live presentation (49%), followed by computer or web based (20%) and then mixed modalities (19%). Method of evaluation or outcomes was studied (Fig. 4). Survey (36%), test (17%), and test plus survey (16%) were the top three methods of evaluation of a CBL learning session. Lesser in frequency was review of practice behavior (9%), test plus OSCE (9%), and others. Review of practice behavior could include reviewing prescription writing, or in one case reviewing the number of adverse drug events reported spontaneously in Portugal. 65
Discussion and Review
CBL is used worldwide. There was a large variety of fields of medicine. The numbers reported included a wide range of number of learners. Some studies were descriptive, and it was hard to know exactly how many students were involved. This problem was noted in another recent review. 3 CBL was used in various educational levels, from undergraduate to graduate. The number of students ranged from very small studies of 7 students to over 3000 students. The media used to deliver a CBL session varied, from several live forms to paper and pencil or internet-based media. The outcomes measurement to review if CBL sessions were successful ranged from surveys of participants to knowledge tests to measures of patient outcomes. In order to further analyze the worldwide use of CBL, the articles are reviewed below in more detail.
Definition of CBL
CBL has been used in medical fields since at least 1912, when it was used by Dr. James Lorrain Smith while teaching pathology in 1912 at the University of Edinburgh.63,68 Thistlewaite et al 3 pointed out in a recent review of CBL that “There is no international consensus as to the definition of case-based learning (CBL) though it is contrasted to problem based learning (PBL) in terms of structure. We conclude that CBL is a form of inquiry based learning and fits on the continuum between structured and guided learning.” They offer a definition of CBL: “The goal of CBL is to prepare students for clinical practice, through the use of authentic clinical cases. It links theory to practice, through the application of knowledge to the cases, using inquiry-based learning methods.” 3

Method of evaluation.
Another pathology article from Africa, describing a course in laboratory medicine for mixed graduate medical education (residents) and CME for clinicians, defines CBL: “Case-based learning is structured so that trainees explore clinically relevant topics using open-ended questions with well-defined goals.”
7
The
A modern definition of CBL is that CBL is a form of learning, which involves a clinical case, a problem or question to be solved, and a stated set of learning objectives with a measured outcome. Included in this definition is that some, but not all, of the information is presented prior to or during the learning intervention, and some of the information is discovered during the problem solving or question answering. The learner acquires some of the learning objectives during the CBL session, whether it is live, web based, or on paper. In contrast, if all of the information were given prior or during the session, without the need for inquiry, then the session would just be a lecture or reading.
Comparison of CBL and PBL
CBL is not the first and only method of inquiry-based education. PBL is similar, with distinct differences (Fig. 5). In many papers, CBL is compared and contrasted with PBL in order to define CBL better. PBL is also centered around a clinical case. Often the objectives are less clearly defined at the outset of the learning session, and learning occurs in the course of solving the problem. There is a teacher, but the teacher is less intrusive with the guidance than in CBL. One comparison of CBL to PBL was described in an article on Turkish dental school education: “… CBL is effective for students who have already acquired foundational knowledge, whereas PBL invites the student to learn foundational knowledge as part of researching the clinical case.” Study, of postgraduate education in an American Obstetrics and Gynecology residency, describes CBL as “CBL is a variant of PBL and involves a case vignette that is designed to reflect the educational objectives of a particular topic.”
54
In an overview of CBL and PBL in a dental education article from the United States, the authors note that the main focus of PBL is on the cases and CBL is more flexible in its use of clinical material.
16
The authors quote Donner and Bickley,
70
stating that PBL is “… a form of education in which information is mastered in the same context in which it will be used … PBL is seen as a student-driven process in which the student sets the pace, and the role of the teacher becomes one of guide, facilitator, and resource … (p294).” The authors note that where PBL has the student as the
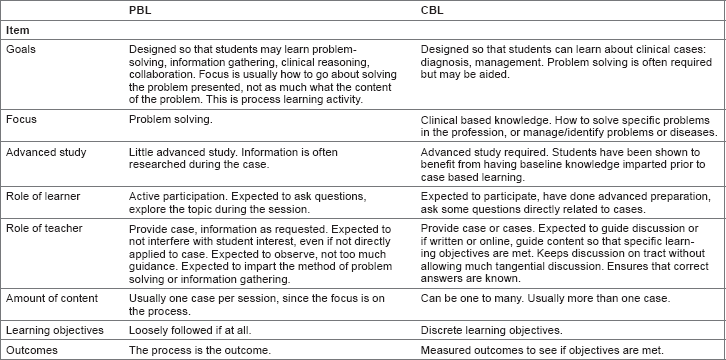
Differences in CBL and PBL.
Two studies highlight the advantages and disadvantages of CBL compared with PBL. Both studies report on major curriculum shifts at three major medical schools. The first study, published in 2005, reported on the performance outcomes during the third-year clerkship rotations at Southern Illinois University (SIU).
19
At SIU, during the 1994–2002 school years, there was both a standard (STND) and PBL learning tract offered for the preclinical years, years 1–2. During the PBL tract, basics of medicine were taught in small group tutoring sessions using PBL modules and standardized patients. In addition, there was a weekly live clinical session. The two tracts were compared over all those years with respect to United States Medical Licensing Exam© (USMLE) test performance on Steps 1 and 2, and also overall grades and subcategories on the six third-year clerkships. So the two tracks had differing years 1–2 and the same year 3. Results noted that the PBL track had more women and older students, so these variables were set out as covariates analyzing other scores. Comparing the PBL versus STND tracks, USMLE scores were statistically equal over the years 1994–2002. PBL was 204.90 ± 21.05 and STND was 205.09 ± 23.07 (
The difficulties in using PBL were associated with changes in other medical schools. Two medical schools in the United States, namely, University of California, Los Angeles, and University of California, Davis, changed from a PBL method to a CBL method for teaching a course entitled
Advantages of CBL and deeper learning
Another touted advantage of CBL is
Another attempt to measure deeper learning was reported from a dental school in Turkey.
8
The authors compared a CBL course with an older LBL course from the previous year by using “SOLO” taxonomy, developed by Biggs and Collis.
73
SOLO taxonomy rates the learning outcomes from prestructural through extended abstract. For example, in unistructural, the second item of SOLO, items could be “define”, “identify”, or “do a simple procedure”, whereas in the “extended abstract” level, the items are “evaluate”, “predict”, “generalize”, “create”, “reflect”, or “hypothesize” in higher mental order tasks.
8
A post-test was used to measure the responses on the test. The test questions were assigned to SOLO categories. In the first three categories of SOLO taxonomy questions, there was no statistical difference in scores between LBL and CBL groups. In the last two or higher categories of questions based on SOLO taxonomy, there was a statistically significant increase in the scores for relational and extended types of questions for the CBL group (
Two other studies discussed the levels of thinking and preparation for practice. One study compared students in interdisciplinary (ID) versus single-discipline students (SD; clinical anatomy) in a Graduate School for Health Sciences in Missouri, U.S. The two groups had slightly different cases. The ID group had complex ID cases and answered multiple choice questions about the cases. The SD group had cases in their discipline and answered multiple choice cases around the case. The assessment tool was the Watson-Glaser Critical Thinking Appraisal. The mean scores of both groups were not statistically different. However, ID students who scored below the median on the pretest scored significantly higher on the posttest. While this study set out to compare the differences in SD vs ID teaching using CBL, it also compared the effects of an ID course on critical thinking and it appears to be synergistic with improving scores for students who started below the median on testing. This is important in education programs, because while mean scores may not rise, if less students are scoring lower, then less students will fail the course and have to repeat.
The second paper that attempted to measure higher learning outcomes queried dental school graduates who had completed a CBL course during their dental school training. 22 The survey was designed to assess the CBL curriculum with respect to actual job requirements of practicing dentists. The graduates spanned 16 years, from 1990 to 2006, and the survey was conducted in 2007–2008. The response rate was 41%. The findings were that the CBL course was associated with positive correlations in “research competence”, “interdisciplinary thinking”, “practical dental skills”, “team work”, and “independent learning/working”. Other items including “problem-solving skills”, “psycho-social competence”, and “business competence” were not scored as highly with respondents. This article measured self-reported competencies and not the competencies as assessed by independent observers. However, it does attempt to link CBL with the actual practice with which it was attempting to teach, which is one of the generally accepted benefits of CBL.
In summary, CBL is defined as an inquiry structured learning experience utilizing live or simulated patient cases to solve, or examine a clinical problem, with the guidance of a teacher and stated learning objectives. Advantages of using CBL include more focusing on learning objectives compared with PBL, flexibility on the use of the case, and ability to induce a deeper level of learning by inducing more critical thinking skills.
Uses of CBL with respect to various fields and various levels in health-care training
CBL is used to impart knowledge in various fields in health care and various fields of medicine. The findings in this review showed that articles demonstrated the use of CBL in medicine,2,4–7,9,10,12–14,18–21,24–26,30,33,34,36,37,39–44,46,48–62,64–67 dentistry,8,15,16,22,23,28 pharmacology,11,27,29,35,45,63 occupational and physical therapy, 31 nursing,5,21,38,47,51 allied health fields, 32 and child development. 17
Eighteen fields of medicine were seen in this review, from internal medicine and surgery to palliative medicine and critical care (Fig. 2, “fields of study”). Several articles highlight ID care or interprofessional care. A 2011 article in critical care medicine demonstrated the utility of both simulators and CBL on behaviors in critical situations of critical care teams of physicians and nurses. 5 Palliative care 21 and primary care51,59 articles also reported on using a CBL course for learning with physicians and nurses. An article from the United Arab Emirates discussed how CBL better prepared participants for critical situations as well as basic primary care. 59
CBL is also used in various levels, including undergraduate education in the professions, graduate education, and postgraduate education. One field that uses CBL for all levels is surgery. Several articles describe surgical undergraduate medical education. One article describes using a paper and pencil plus live review sessions on improving student knowledge as tested by a standardized test in surgery. 6 Another paper from Germany describes initiation of a CBL curriculum for medical students and lists the pitfalls in establishing this curriculum. 26 A third undergraduate paper in a medical school course in surgery describes utilizing CBL and a more structured curriculum to aid in knowledge gains. A study utilizing both surgical simulators for laparoscopic procedural skills and CBL for clinical knowledge and reasoning demonstrates learning enhancement using CBL in surgical residents, or graduate surgical training. 20 In this study, scores in both procedural ratings during surgery for residents and also knowledge scores when presented with complications from surgery both rated higher in the CBL-enhanced course. Graduate use of CBL in surgery is frequent. CME courses are taught in trauma, which features lectures, skill stations, and simulation-based CBL. 74 Advanced Trauma Life Support (ATLS) certification is required for all surgeons who practice in a designated trauma center in the United States. 74 In addition, the American College of Surgeons publishes a self-assessment course entitled “SESAP” or Surgical Education and Self-Assessment Program, which is a web or CD-ROM course that is largely case based, with commentaries. 75 These two courses are widely available and are constantly revised to reflect new advances in patient care research. The use of CBL programs was employed in undergraduate and graduate including postgraduate fields in this review.
Use of CBL in rural and underserved areas
One practical use of CBL is to use CBL to enhance knowledge in rural or underserved areas. An excellent example of CBL is the Project Extension for Community Healthcare Outcomes (ECHO) program in Arizona and Utah states, United States.10,12 This program was based on the Project ECHO program initially devised at the University of New Mexico Health Sciences Center in 2003. 10 In Arizona and Utah, the CDC helped fund a program to teach primary care providers and also provide access to specialist to treat hepatitis C virus (HCV)-infected patients. The primary aim was to increase treatment, as new drugs have become available, which are highly effective in treating HCV. The program works by recruiting primary care physician to participate. An initial teaching session is held on site at the health-care clinic in the rural or underserved area. Then, the provider teams are asked to participate in “tele ECHO” clinics in which participants present cases and have experts in HCV treatment comment. There are also educational sessions. Ninety providers participated, with 66% or 73% being primary care providers in rural or community health centers and not at universities. Over one and a half years, 280 patients were enrolled with 46.1% starting treatment. Other patients were likely not able to be treated, as their laboratory values indicated advanced liver disease. The percentage starting treatment was more than twice as many as expected to receive treatment prior to the project, based on historical controls. In addition to showing how CBL can impact rural medical care, this study is an example of learning assessment measured in patient outcomes.
A second CBL project was used in the United Arab Emirates to train rural practitioner's vital aspects of primary and emergency care using a CBL project. 60 The learners were able to provide feedback to the teachers as to the topics needed. This demonstrates the potential for interaction between teachers and learners using CBL, as it is a practical way to teach active practitioners. A third demonstration of using CBL in rural areas is in a report on teaching laboratory medicine in Africa. 7 In Sub-Saharan Africa, there is low trust in laboratory medicine services due in part to lower the quality of laboratories. This problem directly impacts patient care. Multiple international agencies are assisting the clinical laboratories in Sub-Saharan Africa in order to improve the quality of service. According to this report, the quality problem has led to decreased trust in laboratory medicine in the region. The course, given at Addis Ababa University in Ethiopia, was initiated to provide knowledge and also increase trust in laboratory medicine. The participants were 21 residents (graduate medical education), 3 faculty members, and 4 laboratory workers. The course was structured with both lectures and cases. Students were given homework for the differing cases. The assessments were both knowledge gains and also surveys of satisfaction for the course. Ratings on the survey were by ratings on a Likert scale of 1 (least valuable) to 5 (most valuable). Regarding the methods of delivery, the CBL sessions were rated highest with 85% of learners rating them as most valuable. In all, 81% rated case discussions as most valuable. Lectures received the most valuable rating by 65%. On the 12 question pre-/posttest, the mean score rose and also the number of questions answered correctly by the majority of learners. 7 These reports from three continents demonstrate that CBL is a practical way to impart knowledge in a diverse range of topics to clinicians who may be remote from a medical university.
Delivery of CBL: implementation and media
As illustrated in the above examples of use of CBL in rural settings, CBL use is varied as to the delivery method and implementation. Several articles demonstrate the importance of preparation for use in CBL. As many practitioners and students in all fields likely have more experience with LBL, participating in a course with CBL requires a different strategy and mindset in order to reach learning objectives. Preparation of both students and teachers in a CBL format is also very important for success. Two studies highlight the preparation and implementation of CBL: one not as successful as the other. In a qualitative study of introducing a new CBL format series to undergraduate medical students based in Sweden, the authors found that preparation of both students and faculty was likely inadequate for complete success. This study, held at the Karolinska Institutet, described the implementation of a CBL format for learning surgery during a semester course. All LBL classes were replaced with CBL sessions. The authors noted that at this time, there were organizational obstacles to starting a CBL course: lack of time and funds for faculty training. As such, faculty training was delayed and decreased. The study was a survey of five students and five faculty, who were picked from larger pools. There was a lot of criticism by students that the CBL needed more structure, or that the faculty often turned the CBL session more into a lecture session. The faculty described problems with getting the students to engage, and also with the lack of preparation for teaching in that format. Still, the overall impression was that CBL could increase interactive learning for this level of student. 26 This study demonstrates how lack of adequate preparation can impact a CBL experience for both faculty and students.
Another article demonstrated the differences in student motivation for autonomous learning, which was different, depending on how CBL was introduced. In a study of child development students in Sweden, there were four group methods to compare how students learned, depending on how CBL was introduced. The four groups were as follows: (1) LLL or all lecture, (2) CCCC or all CBL, (3) LCLC in which lecture and CBL were alternated in each session after the introduction, and (4) LLCC, in which there were three sessions with all lectures, two mixed lecture plus CBL, and two CBL only lectures to finish. There was a knowledge pretest and post-test to assess what the authors call
Use of CBL to impact patients and measurement of results
As described earlier, the Kirkland model of learning and assessment of outcomes includes assessment of the results of the training as its final method of assessing an intervention. In other words, how did the training impact patient care or its surrogate marker? Four recent studies illustrated how CBL can impact patient care.10,12,40,54,69 The first, already described, is the Project ECHO for HCV treatment, which resulted in 46.1% of patients in the areas affected being started on treatment, and a large proportion of those treated being started on the newer antivirals. The second study was a study on practices by primary care physicians on treating diabetic patients. In this study, 122 primary care physicians (Family and Internal Medicine) at 18 sites were divided into three groups to enhance diabetes care. Group A received surveys and no intervention and served as a control group; group B received Internet-based software with three cases in a virtual patient encounter. The cases had simulated time and could include laboratory and medication orders and follow-up visits. After the cases, the physicians received feedback in the form of what an expert would do. Group C received the same CBL as group B with the addition of 60 minutes of verbal feedback and instruction from a physician opinion leader. The authors were able to obtain clinical data for the results. The results were that group B had a significant decline in hemoglobin A1C measures, the most common means of assessing glucose control over time in diabetics, while groups A and C did not. Groups B and C had a significant decline in prescribing metformin in patients with contraindications also. This demonstrates favorable clinical results using a CBL intervention. 40 The third was a study to institute chlamydia screening in offices. While the intervention did not globally increase chlamydia screening, the impact was that there was less of a decay on chlamydia screening in the intervention groups. 54 The last study demonstrated a CBL study in Portugal, which demonstrated an increase in reporting of adverse drug events after a CBL intervention in a study population of over 4000 physicians. 69 These four articles describe the use of CBL to impart medical knowledge and the use of patient outcomes to assess that learned knowledge. This is the ultimate test of learning for health-care practitioners: knowledge that improves patient care.
Limitations of this Review
This review was an attempt to classify a term,
Conclusions
CBL is a tool that involves matching clinical cases in health care-related fields to a body of knowledge in that field, in order to improve clinical performance, attitudes, or teamwork. This type of learning has been shown to enhance clinical knowledge, improve teamwork, improve clinical skills, improve practice behavior, and improve patient outcomes. CBL advantages include providing relevance to the adult learner, allowing the teacher more input into the direction of learning, and inducing learning on a deeper level. Learners or students in health care-related fields will one day need to interact with patients, and so education that relates to patient is particularly relevant. Relevance is an important concept in adult education. CBL was found to be used in all continents. Even limiting the search to English and English translations, articles were found on all continuously inhabited continents. This finding demonstrates that the use of CBL is not isolated to Western countries, but is used worldwide. In addition, based on the number and variety of fields of medicine and health care reported, CBL is used across multiple fields.
In reviewing the worldwide use of CBL, several constants became apparent. One is that this involves a case as a stimulant for learning. The second is that advance preparation of the learner is necessary. The third is that a set of learning objectives must be adhered to. A comparison with PBL across several articles revealed that most teachers who use CBL, in contrast to PBL, need to get through a list of learning objectives, and in so doing, must provide enhanced guidance to the learning session. That adherence to learning objectives was evident in most articles. There were varied methods of delivery, depending on the learning situation. That is one of the practical aspects of learning sessions termed case-based learning or CBL. The teachers used cases within their realm of teaching and adapted a CBL approach to their situation; for example, live CBL might be used with medical students, video cases might be used with practitioners. CBL differs from PBL in that it can cover a larger amount of topics because of the stated learning objectives, and guidance from the teacher or facilitator who does not allow unguided tangents, which may delay covering the stated objectives. Contrasting CBL with CBL, in PBL, the focus is on the process of learning as much as the topic, whereas in CBL, the learning objectives are stated at the outset, and both learners and teachers try to adhere to these. Because there are stated objectives at the outset of the learning experience in CBL, these objectives can be tested to see if they are met. These tests of knowledge were explored as methods of evaluation, which varied.
The methods of evaluation ran the range of Kirkpatrick's hierarchy of learning. One of the important aspects of CBL which was explored was that perhaps CBL could induce learning on a deeper level. And so going up the hierarchy of learning, some evaluations were simple surveys of the learners/and or the teachers on how they liked the CBL intervention. Some were tests of knowledge or skills learned. A few studies evaluated practice behavior; that is, going beyond knowledge learned into what behaviors that knowledge induced. The last hierarchy was how the knowledge learned from CBL affected actual patients: a few studies revealed that patient outcomes were affected positively from CBL. Thus, published studies of CBL spanned the hierarchy of learning, from opinions of the activity to actual patients affected by the learning of practitioners.
In summary, CBL was found to be practiced worldwide, by various practitioners, in various fields. CBL delivery was found to be varied to the situation. Methods of evaluation for CBL included all the steps on Kirkpatrick's hierarchy of learning and demonstrated that CBL could be shown conclusively to produce deeper learning.
To repeat the definition included earlier in this review, CBL is a form of learning that involves a clinical case, a problem or question requiring student thought, a set of learning objectives, information given prior and during the learning intervention, and a measured outcome.
CBL imparts relevance to medical and related curricula, is shown to tie theory to practice, and induce deeper learning. CBL is practical and efficient as a mode of teaching for adult learners. CBL is certain to become part of every medical and health profession's curriculum.
Author Contributions
Conceived the concepts: SFM. Analyzed the data: SFM. Wrote the first draft of the manuscript: SFM. Made critical revisions: SFM. The author reviewed and approved of the final manuscript.