
Abstract
Introduction
Population Health and System Science, a longitudinal course at a new medical school in northeast Texas, incorporates case-based learning and experiential field visits during an 18-month pre-clerkship phase. The course integrates content from public and population health, preventive medicine disciplines, and health administration and leadership.
Materials and Methods
A cross-sectional survey assessed student self-reports on achievement of session objectives and introduction to national core curricular, cross-cutting, and systems thinking domains.
Results
Of 36 students, 33 responded. Most rated objectives favorably. Open-ended responses highlighted relevance to future practice and requested more content on biostatistics, epidemiology, health equity, and healthcare economics, financing, and policy.
Discussion
Findings suggest the course effectively introduces key concepts, with opportunities to enhance foundational content in measurement, policy, and financial aspects of healthcare. Future studies should investigate application during required clinical rotations.
Introduction
In modern medical education, health systems science has evolved as a crucial third pillar alongside basic and clinical sciences.1,2 The teaching of population health and health system science (PHSS) competencies early in medical training equips future physicians to navigate and address evolving needs of complex healthcare systems. Population health considerations and delivery system barriers pose unique challenges in rural settings. Many medical schools have struggled determining how best to incorporate this important content into the medical school curriculum. In fact, the 2023 AAMC SCOPE survey included curriculum content areas specific to PHSS, but the 2024 did not, suggesting these competencies remain elusive.
Background
The University of Texas at Tyler Health Science Center (UTTHSC) had its beginnings on the former grounds of the Station Hospital of Camp Fannin, an Infantry Replacement Training Center opened by the U.S. Army during World War II. After the war, it was acquired by the state of Texas and became a tuberculosis sanatorium, subsequently being renamed the East Texas Chest Hospital, operated by the Texas Department of Health. In 1977, it joined the University of Texas System. 3 Over the years, the UTTHSC expanded its clinical care and research missions focused on chest diseases to add legacy accredited graduate medical education programs in family medicine and in occupational medicine (the latter born out of the Center's research in asbestos-related pulmonary diseases). With its longstanding interest in public health, population health, and healthcare administration, UTTHSC added graduate degree programs including a Master of Public Health and a Master of Healthcare Administration. A merger with the main UT Tyler campus in 2021 along with a collaboration with UT Health East Texas health system has culminated in a platform allowing the establishment of a medical school.
The approach to organizing a PHSS course for this new medical school and modern medical curriculum was partly rooted in this history, examining historical and current subject matter expertise as previously outlined in the Introduction and represented in Figure 1. Serendipitously, found in the Social Service archive library of the East Texas Tuberculosis Hospital was a volume entitled Readings in Medical Care by the Committee on Medical Care Teaching of the Association of Teachers of Preventive Medicine. 4 A forward prepared by George Packer Berry, M.D., Dean, Faculty of Medicine, Harvard University, discusses early organized teaching in U.S. medical schools on the topic of Medical Sociology, with the first such medical school program concerned with the structure of medical care taking place in 1945 as a series of special lectures for Harvard medical students, later published in the New England Journal of Medicine. 5

PHSS Specialty Area Year 1 Themes.
Two comments by Dr Berry in 1958 are noted here. First, he comments that educational offerings for future doctors must constantly be adjusted to the changing conditions and needs of society, and that “adequate understanding of the setting of medical care is essential” and that “students must learn about the factors that affect the availability and quality of medical care…The clinical medicine of the future will be indissolubly a part of the future organization of medical service with all the relevant professional activities, facilities, and financing.” 4 Second, he observes that “The practice of presenting to medial students all points of view on sociological problems as they relate to medical care has been continued at Harvard by the Department of Preventive Medicine.” 4 A scan of the contents of the Readings in Medical Care reveals a range of topics relevant to the evolving field of Medical Sociology: the national health picture, adequacy of medical care, the costs of medical care, the medical care team, hospitals (improving service and standards of care), coordination in health and medical service (integrating prevention and cure), care of long-term illness, rural medical care, public medical care, medical care in industry, and medical care insurance.
Today's textbooks of the emerging discipline of Health Systems Science aim to bridge the gap between basic and clinical science and the potential impact of physicians on patients’ health or on the health of the population. It is interesting that roughly six decades later, as health systems science has become the crucial third pillar of modern medical education, and we refine the competencies, objectives, and topic categories of a national curricular framework, the core and cross-cutting domains continue to bear a striking resemblance – for example, social determinants of health and health disparities; the structures and processes of the health care system (access, financing, quality improvement); societal factors (health policy and advocacy); communication and information technology. 6
Northeast Texans face significant health challenges living in one of the most underserved parts of Texas. 7 To address this, a new University of Texas at Tyler (UT Tyler) School of Medicine (SOM) aims to expand healthcare access for the region's 1.3 million rural residents. One of the school's key strategies to accomplish its community-focused mission is by “educating culturally competent physician leaders who focus on individual wellness, population health, emotional and mental health, as well as physical disease.” 8
Aligned with the medical school mission, a PHSS course was designed for the pre-clerkship curriculum (18 months) that provides an early introduction of public and population health concepts and health system science principles, with special attention to rural settings. The curriculum uses a case-based learning (CBL) approach, with Year 1 involving monthly sessions, and Year 2 offering field visits to rural sites that allow students to observe real-world health system operations and reflect upon application of CBL objectives from Year 1.
PHSS Curriculum Development
The course integrates a spectrum of preventive medicine content and competencies with HSS skills. It helps students achieve fundamental competencies in the Patient Care (PC), Medical Knowledge (MK), Systems-Based Practice (SBP), Practice-Based Learning and Improvement (PBLI), and Healthcare Leadership (Leadership) domains. Medical students will learn about health variables in their patient population(s) and apply the lens of the continuum of prevention. Preventive medicine specialties emphasize health promotion and health protection with a focus on targeted populations sharing common risk factors. These emphases span a range of knowledge and skills, from primary prevention of injury and disease, to secondary prevention involving early detection and intervention, to tertiary prevention of adverse outcomes associated with more advanced medical illness.9,10 The PHSS course focuses on the roles of healthcare administration, leadership, and management (HALM), public health and general preventive medicine (GPM), and occupational and environmental medicine (OEM).
During design of the pre-clerkship curriculum and as part of the accreditation process, medical education program objectives (MEPOs) were developed that were aligned with fundamental competency domains as previously outlined. Several of these MEPOs were adopted directly as session objectives for the PHSS course with many aligned with HALM and the SBP and Leadership competency domains. Additionally, several MK and PC objectives were developed for GPM and OEM, harmonizing with sub-competencies and milestones from the Accreditation Council for Graduate Medical Education (ACGME). 10
In Year 1 of the pre-clerkship SOM curriculum (PHSS IA), subject matter expert faculty engage with students monthly across the three specialty areas, each comprised of four sessions/themes (see Figure 1).
Students are introduced to such topic areas as quality improvement/patient safety in healthcare systems, financing in healthcare, elementary epidemiologic principles/study design, clinical prevention, social/behavioral/rural determinants of community health, and occupational/environmental exposure and risk factors. Students receive formative participation and professionalism feedback from CBL faculty facilitators and are assessed with summative exams. During the first six months of Year 2 (PHSS IB; remainder of pre-clerkship curriculum), students begin with a module on patient-centered care and subsequently participate in monthly experiential activities touching one or more of the three disciplines (GPM, HALM, OEM) and assessed with self-reflective exercises and a group mini-white paper using the general SBAR tool/technique from the Institute for Healthcare Improvement (see SBAR Tool: Situation-Background-Assessment-Recommendation at https://www.ihi.org/resources/tools/sbar-tool-situation-background-assessment-recommendation). 11 SBAR is a framework for potentially communicating the concern to the field site with recommendation(s) for improvement/resolution. Sample rural field visits include a hospital C-suite, federally qualified health center (FQHC), public health office, sawmill, and a family farm.
Our study aimed to evaluate the degree to which the PHSS course design and content introduced the first class of medical students to many of the topics within the core curricular, cross-cutting, and systems thinking domains as outlined by Gonzalo et al, 2 and to a more comprehensive list of respective content subcategories (referred to in the current research as categories and topics). The core domains include health care structures and processes; health care policy, economics, and management; clinical informatics and health information technology; population and public health; value-based care; and health system improvement. The cross-cutting domains are comprised of leadership and change agency; teamwork and interprofessional education; evidence-based medicine and practice; professionalism and ethics; and scholarship. Systems thinking refers to a “complex web of interdependencies” with “multi-directional cause-effect relationships.” 2
Materials and Methods
Because the students had begun their required clinical experiences, a survey was developed. The survey asked how well each objective introduced students to topics from the national curricular framework 2 mapped to PHSS learning objectives. A 4-point Likert scale was used where 1 = not at all to 4 = extremely well. Additionally, two open-ended prompts were used to have students (1) list up to three items they learned in PHSS that they believed they could apply in future medical practice and (2) list up to three items they wished had been covered in more depth. For these prompts, respondents had the option of marking “I have no suggestions.”
A 4-point Likert-type scale was selected for the quantitative survey given the small number of participants and to prompt a leaning by the respondents as to agreement or disagreement with the statement. While a neutral fifth option is commonplace and permits expressing lack of an opinion or sentiment, a dichotomous response more readily drives adjustment in curriculum content to better meet learning objectives or themes.
On average, the online survey was expected to take less than 30 minutes. The questionnaire had not previously been validated. The survey questions were piloted with PHSS faculty to ensure clarity. The survey was constructed in Qualtrics (Provo, UT, USA), after which two authors reviewed the survey for accuracy and flow. However, the questionnaire was not pilot tested with students prior to administration during the study. The survey tool is available as Appendix A.
The study protocol, survey tool, and informed consent were submitted to, reviewed, and approved by the University of Texas at Tyler Institutional Review Board (IRB). The survey was conducted electronically with written informed consent (approved by the IRB) as part of the web-based administration of the survey. The latter, preceding the survey, provided the student with an explanation of the study and informed consent. Choosing to continue with the questionnaire served as acknowledgment that the participant had reviewed, understood, and willingly chosen to proceed.
All medical students from the Class of 2027 (n = 36) who had successfully completed the coursework for both PHSS IA and IB were invited to participate (inclusion criteria). There were no exclusionary criteria. Approximately three months after course completion in March, 2025, an email invitation explaining the study was sent to the students. The survey was closed approximately two months later (May, 2025).
Two e-mail reminders (approximately two weeks apart) were sent to individuals who had not responded to the initial request for the survey. Due to poor survey response after two e-mail reminders, all eligible students were invited to a free “pizza lunch” where they could use their personal devices to take the survey on-line at the same time. The latter was approved by the UT Tyler IRB. Survey completion occurred following acknowledgement of having read and understood on-line informed consent.
The scaled responses were analyzed for frequency of response to determine the self-reported level of the degree to which achievement of session objectives introduced students to national curricular categories and topics. Due to small numbers, the categories of “Not at All” and “Poor” were combined to calculate an unfavorable rate. Additionally, the open-ended question responses were expected to provide further insight into learned items deemed to be important for future medical practice or items students would like to have been covered in greater depth.
Qualitative analysis of the two open-ended survey items followed the steps of inductive thematic analysis. 12 The two open-ended questions represent inductive methods to explore potential insights and themes generated from the data. This approach was adopted in lieu of deductive methods as no specific pre-existing concepts or theories were postulated for analysis of these qualitative questions. One of the authors initially read the comments carefully. Utilizing Microsoft Copilot, a prompt to follow the 6-step process of Clark and Braun was used for each open-ended question. Specifically, the prompt read: “Use Clark and Braun's approach to thematic analysis for the following open-ended questions by summarizing the list of items based on each question.” Output was then reviewed carefully to ensure the summaries truly reflected the data, editing themes to better reflect the student comments. Afterwards, the summary and raw comments were shared with other authors to read and verify and/or edit the themes.
Results
A total of 33 of 36 (92%) students submitted complete surveys.
Frequencies for scaled responses related to each session objective (GPM, HALM, OEM) can be found in Table 1, as well as frequencies for patient-centered care session and field experience site objectives. Of the 44 individual learning objectives rated, 31 (70%) were rated as well or extremely well. Generally speaking, these fell into broad thematic areas such as:
Health system quality and safety Occupation and environment and their impact on health Health promotion and clinical prevention OEM health protection/regulation/surveillance Health system culture Clinical preventive medicine and social determinants of health Clinical occupational and environmental medicine Field experiences.
Scaled Responses for Student Feedback on Introduction to Categories and Topics From a National Curricular Framework; Using Session Objectives From PHSS Mapped to Categories/Topics Within the Core Curricular, Cross-Cutting, and Systems Thinking Domains (Categories/Topics Are Listed in the Table Parenthetically).

Of those rated poorly by more than 15% of the respondents, the specific topics are listed below:
Teamwork and reflective practice to include quality and patient safety Public health Population health management Communication required in an integrated and coordinated system Health systems principles and concepts; Health care structures and processes; Health care policy, economics, and management Evidence-based medicine and practice Informatics/technology.
Explanations for areas that did not receive favorable feedback may include module sequencing or case selection and development. However, these areas provide an opportunity for further questioning and potential improvement.
Thematic analysis of the two open-ended survey items can be found in Table 2. Alignment of themes with current health systems science (HSS) literature was determined based upon a comparison of findings with representative curricular content in core, cross-cutting, and linking domains. 2 Thematic categories such as health disparities, social determinants of health (SDOH), healthcare systems/policy/insurance, interprofessional collaboration and communication, public health and data literacy, and policy and systems thinking suggested strong concordance with the HSS literature.
Open-Ended Survey Items for Student Feedback on Introduction to Categories and Topics From a National Curricular Framework.
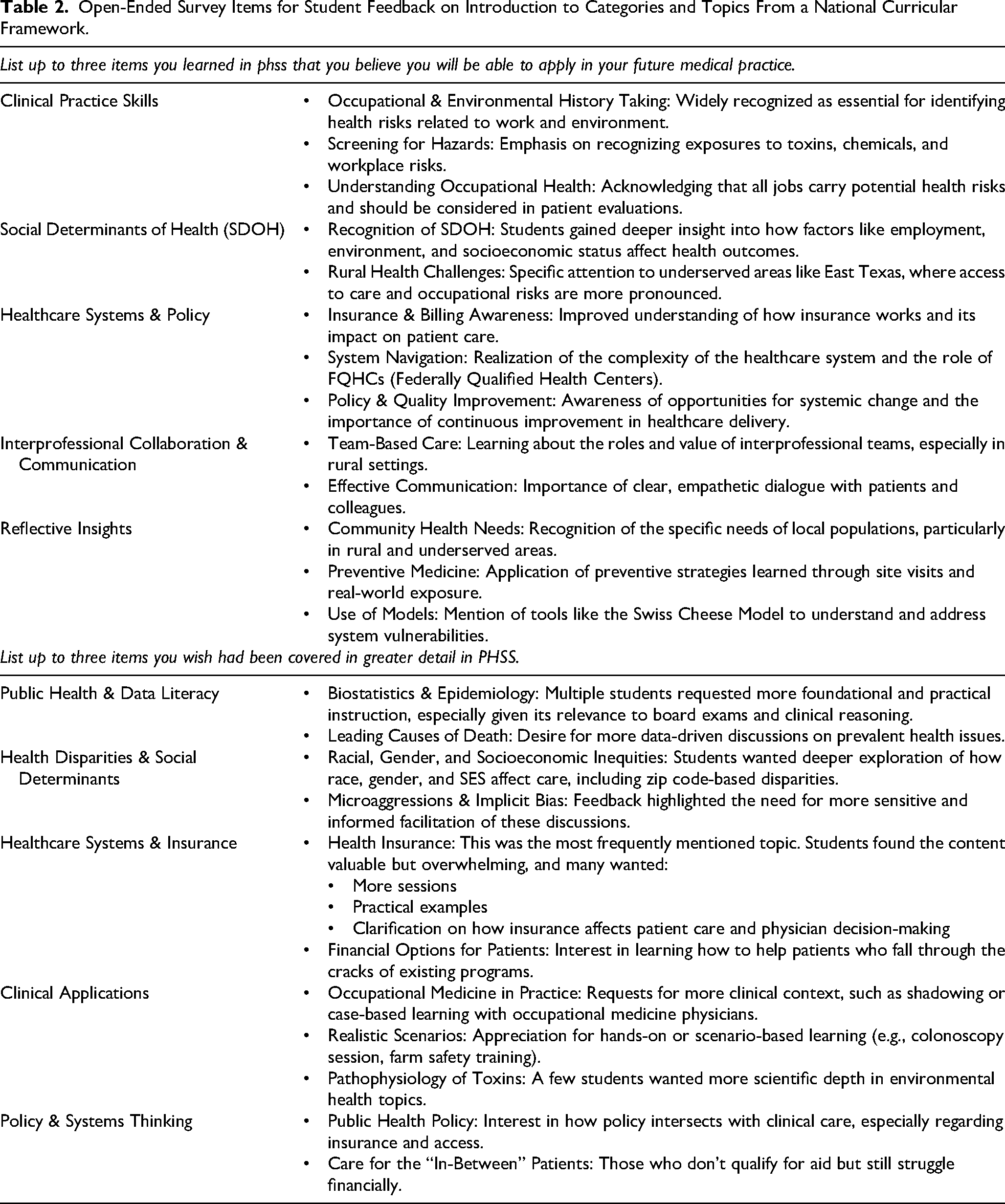
In response to the open-ended item of application to future medical practice, 6/36 answered “I have no suggestions.” For the item “wish covered in greater detail in PHSS,” 10/36 answered “I have no suggestions.” In both instances, this was felt to indicate a notable portion of students either felt content with the experience or had no additional feedback to offer.
Discussion
The School of Medicine at UT Tyler chose to capitalize on its rich history, experience, and available resources in the disciplines of Preventive Medicine (GPM, HALM, and OEM) in order to pilot a curriculum for its PHSS course that would allow early career medical students to accomplish medical education program objectives and introduce students to the many topic categories of a modern national curricular framework. 2
The theoretical underpinnings for using a self-report survey (both quantitative and qualitative) in evaluating the effectiveness of competency-based medical education is rooted in constructivist theory. The students constitute one of several essential sources of feedback, serving as self-directed learners and actively building or constructing their knowledge. This has been an embedded principle in this pre-clerkship phase PHSS course where a case-based approach has been adopted to achieve learning objectives.
Data collected from the scaled survey questions in this study represent a cross-sectional view of the success of that effort. While the data clearly demonstrate favorable student feedback for most session objectives, it is worth noting where more than 50% of respondents scored in the “Extremely Well” category. These included the utility of medical screenings and the importance of early disease detection (52%) as related to population health management (core domain) and evidence-based medicine and practice (cross-cutting domain); recognizing health challenges characterizing the Northeast Texas community at 55% (as related to determinants of health); and describe the special needs of an aging workforce on a working family farm at 52% (as related to healthcare disparities and vulnerable patient populations). The field experiences overall appeared particularly well received.
On the unfavorable side, two areas had unfavorable ratings at 20% or higher including describe the structure, purpose and finance of health care (21%, related to economics) and evaluate the validity of information and apply statistical and quantitative understanding to the interpretation of data (24%, related to public health).
The open-ended survey question pertaining to applicability to future medical practice identified several themes identified by students that appeared to be aligned with the broad disciplines of GPM (deeper insights into SDOH and rural health challenges), HALM (enhanced understanding of how insurance works and its impact on patient care, complexities of healthcare system financing and navigation, and opportunities for quality improvement), and OEM (hazard recognition). Student responses suggested that the field experiences provided insights to roles of various healthcare team members, effective communication, rural and underserved needs, and prevention strategies. Finally, there were themes indicating a desire for more detailed instruction on topics such as biostatistics and epidemiology; exploration of racial, gender, and socioeconomic inequities; health insurance; and policy intersection with healthcare.
This study relies heavily on a set of ACGME competency domains (as previously outlined) that now transcend graduate and undergraduate medical education. However, while the training of medical and health professionals in the U.S. and other countries has shifted to competency-based education, there is no single or uniform core components framework or taxonomy for these broad domains, much less sub-competencies or MEPOs.13,14 This study emphasizes the SBP, PBLI, and Leadership domains essential to medical students for synthesizing, consolidating, and applying knowledge and skills to population health and health systems operations (in the pre-clerkship phase). This pilot study demonstrates how student learners perceive their success in meeting learning objectives and themes readily linked to a national curriculum consensus framework. Equally importantly, areas rated poorly represent opportunities for enhancement.
While similar competencies may be expected in other international models, it is clear that the domain taxonomy may differ and there is not an exact cross-walk with ACGME or the national curricular PHSS framework. For example, the Royal College of Physicians and Surgeons of Canada CanMEDS framework focuses on physician competencies in comparable areas of Medical Expert, Communicator, Leader, and Professional (see https://www.royalcollege.ca/en/standards-and-accreditation/canmeds.html). Alternatively, the World Health Organization (WHO) Global Competency and Outcomes Framework for Universal Health Coverage (UHC) advances improvements in health and progress towards UHC “through aligning health worker education approaches with population health needs and health system demands” (see https://www.who.int/publications/i/item/9789240034662).
A particular strength of this study resides with its very high response and completion rates (all questions answered). Another strength is that it adds to the scholarly discourse on how best to train future physicians for the realities of modern healthcare systems. The authors believe the study sets a good example of successful integration of health systems science in medical education, while providing additional credibility by using a standardized framework to assess the domains.
This pilot curriculum could be replicated in the pre-clerkship phase of other medical schools using a model containing the three preventive specialty areas (GPM, HALM, OEM) and embedding competencies such as social determinants of health, the structures and processes of the health care system (access, financing, quality improvement), societal factors (health policy and advocacy), and communication. However, challenges may include a lack of understanding for these disciplines, sufficient faculty expertise which spans a multitude of areas, and adequate as well as sustainable time and space in the pre-clerkship calendar. Travel costs to rural field experience sites may also prove to be a barrier. Nonetheless, the course overall has received very favorable feedback.
Limitations included using a cross-sectional and descriptive design, student self-ratings, administration of an unvalidated and non-piloted survey tool, and non-generalizability. Moreover, pertaining to analysis of the two open-ended questions, and despite a very high response/completion rate (33/36 or 92%), it is difficult to state that data saturation has been reached, further limiting the generalizability of the qualitative portion of this survey. The convenience nature of this sample is a principal contributor to this limitation as to whether sufficient qualitative data have been collected or analyzed. 15 The notion of saturation as applied to qualitative research has come into question, making this arguable as a true limitation. Nonetheless, the pilot nature of this work offers an opportunity for further investigation. Future study of the impact of the coursework should involve exploring application of the material during the required clinical rotations.
Conclusions
The design of the longitudinal PHSS course at UT Tyler SOM uses a case-based learning approach to drive self-directed learning of population health and health systems science principles in the three preventive domains of GPM, HALM, and OEM. This conforms to the general learning approach for other block foundational science courses allowing the students to grow comfortable with consistent teaching and evaluation methods. The model also relied upon a team-based teaching approach spanning several faculty and disciplines, relying upon subject matter expertise and resources for instruction and facilitation. This pilot survey of the first class of medical students completing PHSS IA and IB generally suggested favorable self-reported achievement of session objectives and introduction to core, cross-cutting, and linking domain topic areas in a national curricular framework. Students made repeated requests for more content/time spent on financial/economic matters in healthcare as well as epidemiologic and biostatistical/measurement principles, two areas that have already undergone expansion in the second medical school class.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205251395290 - Supplemental material for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework
Supplemental material, sj-pdf-1-mde-10.1177_23821205251395290 for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework by Jeffrey Levin, Gary Beck Dallaghan, Chaynee Atwood, Vanessa Casanova, Cynthia Ball, Theresa Byrd, Emmanuel Elueze, Michael Kennedy, Dalia Nessim, Peter Pendergrass and Yordanos Tiruneh in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205251395290 - Supplemental material for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework
Supplemental material, sj-pdf-2-mde-10.1177_23821205251395290 for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework by Jeffrey Levin, Gary Beck Dallaghan, Chaynee Atwood, Vanessa Casanova, Cynthia Ball, Theresa Byrd, Emmanuel Elueze, Michael Kennedy, Dalia Nessim, Peter Pendergrass and Yordanos Tiruneh in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-3-mde-10.1177_23821205251395290 - Supplemental material for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework
Supplemental material, sj-pdf-3-mde-10.1177_23821205251395290 for Population Health and Systems Science: Medical Student Feedback on a Novel Approach That Follows a National Curricular Framework by Jeffrey Levin, Gary Beck Dallaghan, Chaynee Atwood, Vanessa Casanova, Cynthia Ball, Theresa Byrd, Emmanuel Elueze, Michael Kennedy, Dalia Nessim, Peter Pendergrass and Yordanos Tiruneh in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
The authors wish to acknowledge the encouragement and support of several individuals – Drs. Kathleen Jones and Gerald Ledlow, Ms. Kerrie Anne Ambort-Clark, and Drs. Sue Cox, Daniel Griffin, David Rice, Crystal Bryce, Elza Mylona, David Elkowitz, and Brigham Willis. The authors also wish to acknowledge the generous support of the TLL Temple Foundation on behalf of the students at the University of Texas at Tyler School of Medicine for operations and transportation associated with PHSS (experiential field site visits).
ORCID iDs
Ethical Considerations and Consent to Participate
The Institutional Review Board at the University of Texas at Tyler operating under Federal Wide Assurance Numbers: 00003494, 00006044, and 00009775 approved our protocol (2024-264), consent for online survey, and data collection tool (survey) on 01/09/2025. Respondents acknowledged reading and understanding informed consent prior to proceeding with completion of the on-line survey.
Authors’ Contributions
Jeffrey Levin and Gary Beck Dallaghan contributed to protocol and survey design, data collection and analysis, and manuscript preparation. Chaynee Atwood contributed to survey preparation, coordination, and data collection and manuscript review. Vanessa Casanova, Cynthia Ball, Theresa Byrd, Emmanuel Elueze, Michael Kennedy, Dalia Nessim, Peter Pendergrass, and Yordanos Tiruneh contributed to survey and manuscript review.
Funding
The authors received financial support for the research, authorship, and/or publication of this article. Funding for the free “pizza lunch” for eligible students to complete the survey (as outlined in Materials and Methods and approved by the UT Tyler IRB) was supported by the TLL Temple Foundation (see Acknowledgments).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.