
Abstract
Introduction
There is a growing demand for more thoughtful and holistic healthcare. Whole-person integrative medicine (IM) is cost-effective and clinically effective for enhancing health and well-being. However, existing knowledge gaps in IM among healthcare professionals prevent the application of IM practices in patient care. This project aimed to develop and refine an IM elective to improve health education and learning, thereby enhancing future physicians’ knowledge, skills, and self-care practices.
Methods
Three separate cohorts of third- and fourth-year medical students (n = 18) participated in a four-week immersive IM elective. Weekly and postelective evaluations were used to assess changes in attitudes, behaviors, and self-reported IM knowledge for each cohort. Descriptive analyses were performed, and just-in-time student feedback was used to iteratively refine the IM curriculum.
Results
Students attended at least 85% of class days. Anonymous weekly course evaluation ratings for meeting course expectations, education depth, and usefulness for patient care ranged between 4 and 5 on a Likert scale, with 5 as the most favorable. Postcourse evaluations and the impact of the course on attitudes related to patient care, personal lifestyle, and self-awareness also ranged from 4 to 5. Knowledge scores significantly improved (p < .01), with moderate to large effect sizes (Hedges g's > 0.8).
Conclusions
The implementation of an immersive elective curriculum in IM resulted in high levels of satisfaction, changes in attitudes and behaviors, as well as knowledge scores. Just-in-time feedback and curricular revisions made this curriculum effective for student training. We consider this our first step in integrating IM into the required curriculum for all students, ensuring that, as educators, we close the knowledge gap in IM among future physicians. Empowered with that knowledge, we anticipate them serving their future patients with a more holistic and patient-centered approach.
Introduction
Integrative medicine (IM), also known as Integrative health, 1 is the practice of medicine that incorporates both standard medical and complementary approaches to healthcare, such as natural remedies, mind-body practices, and bodywork. 2 The philosophy underlying IM includes an evidence-informed approach to whole-person care (mental, physical, and spiritual) with importance placed on the relationship-building between the practitioner and the patient in considering all appropriate therapeutic and lifestyle approaches to attain optimal health and healing. 3 In the setting of an alarming increase in the mistrust of healthcare professionals, rising healthcare costs, the burden of chronic disease, and burnout of healthcare providers,4–8 the need for change in our healthcare system to a more patient-centered and holistic approach is imperative.
There is mounting evidence that whole-person integrative healthcare is cost-effective and clinically effective for improving mental and physical health and well-being.1,9,10 However, the wide knowledge gap among healthcare professionals mitigates the implementation of these strategies.11,12 Currently, almost a third of adults and 12% of children use complementary health techniques.13,14 An estimated 59 million individuals aged 4 years and over incurred expenditures for a complementary health approach, resulting in total out-of-pocket costs of $30.2 billion, exceeding those of all primary care providers for the time evaluated. 15 IM therapies in medical care, such as for pain, are associated with effective pain reduction 16 and hundreds of dollars in medical care cost savings per hospital admission. 17 The increasing popularity of complementary approaches among patients suggests a greater need for healthcare professionals with knowledge of the efficacy and safety of IM approaches and the practice skills to provide such care in a patient-centered manner. Despite these facts, almost half of US medical schools (45.4%) do not offer IM education, and only 11.0% have inter-professional instruction with an integrative health provider (a provider trained in complementary therapeutic approaches). 18 Early curriculum guidelines in IM for medical schools were created during 2002 and 2003 by the Education Working Group of the Consortium of Academic Health Centers for Integrative Medicine (CAHCIM) and endorsed by the CAHCIM Steering Committee. 19 In 2010, the CAHCIM assembled a task force from 56 academic health care institutions to create IM fellowship core competencies. 20 Recent updates for IM fellowship competencies were developed through CAHCIM that contain areas such as clinician well-being, health equity, interprofessional collaboration, trauma-informed care, and planetary health. 21 As yet, little research has been published on the impact and effectiveness of teaching IM curricula in the United States and internationally for medical professional students and patient care.22–24 Developing an effective curriculum to train future physicians in IM allows a broader range of low-cost therapeutic strategies, enhances coordination, reduces the fragmentation of care, and attenuates potential negative treatment interactions.
Our team at the University of Miami (UM) Miller School of Medicine (MSOM), Osher Center for Integrative Health in the Department of Family Medicine and Community Health, sought to fill a gap in education at the MSOM to address this challenge. A 4-week elective for medical students was developed and implemented using an iterative refinement strategy. 25 Content for the elective was drawn from the CAHCIM core competencies, the American College of Lifestyle Medicine's Six Pillars of Lifestyle Medicine, 26 and the course instructor team's own experiences across academic, clinical, and wellness sectors. Moreover, students were exposed to direct experiences of evidence-based IM modalities that focus on lifestyle behaviors shown to promote health and well-being. In designing the elective, we considered several key concepts of an IM approach: lifelong learning and curiosity, the healthcare provider's personal health behaviors, collaboration among the healthcare team, health equity, and an active learning model. In addition, to prepare the students as leaders and change agents in healthcare, we offered opportunities to foster leadership in education and advocacy with IM projects and oral presentations.
The overarching aim of this project was to implement and iteratively refine an IM elective curriculum to enhance the knowledge base, skill set, and self-care of future physicians and respond to the growing demand for more thoughtful and holistic medical care.
Methods
IRB Approval, Consent, and Assessments
The University of Miami Institutional Review Board (IRB) approved this implementation feasibility project on January 18, 2023. The study adheres to the guidelines of the Declaration of Helsinki. The research staff emailed a brief description of the study to the students enrolled in the elective. If students indicated they were interested in learning more, the research staff further described the project to them individually and obtained verbal consent. The reporting of this study conforms to Standards for Quality Improvement Reporting Excellence in Education (SQUIRE-EDU) guidelines 27 (see supplement materials for the SQUIRE-EDU checklist).
Design Overview
Medical students in the third and fourth year (MS3 and MS4) enrolled at the University of Miami MSOM are required to take 18 elective credits on topics that are not covered in the standard curriculum. The Medical Education Curriculum Committee approved the syllabus for a 4-week elective course on Integrative Medicine (IM) in 2022. The course was based at the Osher Center for Integrative Health, within the Department of Family Medicine and Community Health. Clinical experiences took place in IM practitioner clinics across the University of Miami medical campus, including the Osher Center patient care rooms, as well as at the Veterans Healthcare System. Lectures and IM experiences occurred in the Osher Center classroom or outdoors on the medical campus.
The Integrative Medicine course was developed by a core team composed of University of Miami School of Medicine instructors with extensive experience teaching topics in integrative medicine. The team included the course director (KK), who was the Osher Center Medical Director, a physician fellowship-trained graduate of the University of Arizona Center for Integrative Medicine; the Osher Center Assistant Director, an integrative health physical therapist (TG); an Ayurvedic doctor/Acupuncturist (AD); and the Osher Center integrative health Research Director (LSR). The team carefully considered the curricular design elements and made decisions by team consensus, based on educational expertise and just-in-time learner feedback. The instructor team conducted weekly evaluations of the curriculum for all three cohorts and learner feedback was used to iteratively improve the curriculum.
As part of the elective design, interprofessional guest educators were selected through a criteria-driven process prioritizing clinical credibility, expertise, teaching effectiveness, scholarly contributions, and alignment with evidence-based integrative practices. Educators included other faculty from the UM academic medical center, members of the Osher Collaborative (a group of 11 academic medical centers across the USA and in Stockholm), and external experts with demonstrated success in specific IM modalities. This approach reflects the principle that the quality and impact of teaching are primarily determined by the caliber of the instructors and their ability to teach techniques, taking into account evidence-based practice and empirical outcomes.
Curricular Design
To cater to varied learning styles and facilitate active learning, which fosters engagement and a deeper understanding of the materials, a variety of teaching strategies and techniques were implemented, including lectures, immersive experiences, patient case-based discussions, shadowing of IM clinicians, and independent study. 28 Pre-readings were selected prior to each lesson based on course objectives. Students chose projects related to IM topics for independent study and group presentations. Clinician instructors discussed patient care strategies, including active listening and self-reflection, to enhance their understanding of patient care. Learners were asked to practice a self-selected IM strategy for their personal health care to experience the challenges of implementing health behavior changes. The content and instructional approaches were refined based on feedback from each cohort of students.
Learning objectives were based on the CAHCIM core competencies, the American College of Lifestyle Medicine's Six Pillars of Lifestyle Medicine (nutrition, physical activity, stress management, restorative sleep, social connection, and avoidance of risky substances), 26 and the core instructor team's experience across academic, clinical, and wellness sectors. Didactic, experiential, and reflective learning objectives were then aligned with weekly themes and the overarching principles of integrative health. After each round of the elective, the instruction team assessed student achievement in meeting the course objectives.
Course Content
The month-long curriculum was divided into weekly themes to encompass domains of health addressed by IM. The weekly themes were planetary health and connection, nutrition, mind-body, and the 4 Rs of Restoration, Rejuvenation, Resilience, and Renewal. Table 1 outlines the weekly themes, and the topics and activities covered. The unit themes were used as a guide to learning not only the content but the philosophies behind IM and whole person health (consideration of mind, body, and connections with the outer world).
Weekly Themes, Curricular Topics and Activities in the Four-Week IM Elective.

Every morning began with a different meditation. The daily curriculum content included in-person lectures, videos from leading experts, readings, discussions, and direct experiences of nature, yoga, acupuncture, qigong, nutrition and herb focused cooking classes, body work, exercise, music therapy, guided imagery, and energy practices. Each week consisted of approximately 6‒8 h of lectures, videos, and discussions, 3 h of experiential activities, and 3 h of clinical applications, including history taking, faculty-led case studies, and student presentations of case studies. Clinical experience occurred 3 afternoons per week for 2–3 h each, where students interacted with patients in clinic settings. Each Friday, students presented as a small group on an integrative health research topic, there was a group discussion reflecting on the week's activities, and a weekly course evaluation. A final project was presented at the end of the elective in groups of three, describing the students’ visions for the future of medicine and healthcare.
Assessments
To understand the impact of the course on the learners and the educational program, quantitative and qualitative data were collected iteratively. Demographic factors were assessed, including age, sex, year of medical school, race, and ethnicity. Using a 5-point Likert Scale (0 as least favorable and 5 as most favorable), participants completed weekly assessments on whether the unit met expectations, the acceptability of the unit's educational depth, and the usefulness of the material in patient care. While five-point Likert scales are most common, we chose a six-point scale, which can be easier to interpret as negative or positive and avoids neutral answers.29,30
Open-ended questions were also used to query the strengths of the course and to understand how the preceding week's unit could be improved. Additionally, an overall evaluation of the course was obtained at the end of the 4-week elective. The weekly and postelective evaluations were collected anonymously (without personally identifiable information) from paper surveys, and data were entered using Research Electronic Data Capture (REDCap) hosted at the University of Miami School of Medicine, a metadata-driven workflow and methodology process that comprises translational research informatics support.31,32 Participants completed surveys assessing pre- and postknowledge competencies via links distributed through REDCap. The course faculty met weekly and at the end of each 4-week elective to review the evaluation data and adjust the curriculum.
Following each round of the elective, the achievement of the course objectives was assessed by examining their alignment with the curriculum and from student feedback. Each student was also evaluated by the instructors for course objective achievement during the final grading period.
Statistical Methods
Descriptive quantitative analyses included means and standard deviations for weekly evaluations and postelective evaluations, as well as pre- versus postpaired t-tests for changes in self-reported competencies in IM, calculating Hedges’ g's to determine effect sizes. Analyses with missing data used list-wise deletion. Qualitative information was gathered through weekly evaluations of each unit, where participants were asked to write a few sentences about the strengths of the unit and suggest ways it could be improved. Two of the authors (LSR and KK) systematically reviewed the textual data to identify patterns, themes, and insights that could improve the curriculum. After becoming familiar with the data, a codebook was created. Four a priori codes were identified based on the weekly topic, and sub-codes were categorized as strengths and areas needing improvement. Segmented data were extracted into matrices in Microsoft Excel for each week, and common themes were identified.
Results
Three rounds of the elective were piloted with a total of 18 students (February 2023, October 2023, and March 2024) at the University of Miami Osher Center for Integrative Health. The initial cohort consisted of three students, the second cohort comprised seven students, and the third cohort consisted of eight students. The participants met five days a week for approximately 40 h over 4 weeks. The feasibility of implementing the elective was demonstrated, as students attended at least 85% of class days. The most common reasons for missing classes were illness and residency interviews. All students who began the elective completed it. The average age of the participants was 26 (SD = 1.46); 89% were white, 22% were Hispanic, 89% were female, and most (89%) were in their fourth year, with only two students in their third year of medical school.
Weekly unit evaluation survey ratings from Cohorts 1‒3 were between 4 and 5 on the Likert scale for meeting expectations, education depth, and usefulness for patient care (Table 2). Of the three cohorts, up to four weekly evaluations were missing due to residency interviews. Postelective evaluation and impact ratings also had scores between 4 and 5 (averages, standard deviations) for meeting course expectations (4.92, 0.28), teaching methods (4.85, 0.37), learning resources (4.85, 0.55), understanding basic principles of IM (4.92, 0.28), approaches to patient care (4.92, 0.28), desire to work with IM providers (4.84, 0.37), and effects on personal lifestyle (4.61, 0.55).
Weekly Course Evaluations From Learners in the IM Elective.

Significant improvements in knowledge scores related to IM topics were found from the beginning to the end of the elective (p < .01) (Table 3). Students completed the competency assessments both before and after the elective, and all knowledge improvements showed moderate to large effect sizes.
Changes in Pre and Postelective Knowledge Scores in the IM Elective.

Iterative Curricular Improvements
Improvements were made to each iteration of the IM elective based on student feedback on the strengths and suggested areas for improvement. Table 4 details learner feedback and the changes made to the curriculum as a result. Student feedback on the curriculum fell into categories that included experiential IM activities, the learning environment, and patient-focused activities, which led to the implementation of curriculum changes for the next cohort of students. Students suggested areas for improvement, including a desire for more interactive experiences, such as those involving plants and herbs, as well as hypnosis. Also suggested were shorter lectures, and increased discussions on unfamiliar topics to stretch comfort levels, more time for self-exploration of IM topics, and more lectures on IM research topics. Students also stated that they wanted more patient practice cases and role-playing, as well as more clinic time. In response, we made curriculum changes such as adding a hypnosis interactive activity with a physician who emphasized the “power of words” in clinical practice, and a visit to an herb farm. There was also an increased focus on evidence-based IM practices, which were provided with each lecture. More time was allocated for self-exploration of IM topics and partnered projects. Patient interviews were introduced in the first week of the elective to provide a foundation for whole-patient-based IM care, and additional role-playing activities were provided for topics such as nutrition counseling and nutrition treatment plans. Patient care experiences with IM practitioners increased to several times per week.
Strengths, Areas for Improvement and Resultant Curricular Changes in the Integrative Health Elective Based on Three Cohorts of Medical Student Feedback.

The students gave a lot of positive feedback on the strengths of the elective. Notably, learner comments included “feel more ready to counsel patients about lifestyle” and “stretched my comfort levels.” Strengths noted were group activities such as qigong, acupuncture, yoga, cooking with herbs, and shopping in a food desert. Strengths also stated were the breadth of lectures, discussions on patients’ emotional/social backgrounds, the students’ futures as physicians, and the future of healthcare. Additional strengths included collaborative projects and presentations, demonstrations of patient intakes and practicing patient intakes on one another, and shadowing IM practitioners, such as a functional medicine physician, acupuncturist, physical therapist, and VA IM practitioners.
Discussion
Despite mounting evidence suggesting the safety and efficacy of many integrative health approaches there is a substantial knowledge gap among health professionals about IM.16,33,34 While there are some efforts to provide IM education at the medical school level, many institutions lack such programs, and among those that do, the content and depth of training vary. 35 Moreover, there has been little research on IM curriculum implementation. To address this need, the elective was created and evaluated to provide preliminary information on the feasibility and acceptability of the course as an immersive experience into many facets of IM, expanding student clinical skills while emphasizing the importance of self-exploration and self-care. Importantly, IM education may facilitate the use of IM in the healthcare system, leading to more equitable access. 36
According to student feedback and confirmation of prior studies, the multimodal learning model proved to be an effective strategy for teaching as evident by improvements in knowledge self-assessments and positive evaluations. Teaching methods included lectures, discussions, independent research topics, observed physician-led integrative health histories and physicals and performance of simulated patient assignments using a family member or friend. Students were also required to choose an aspect of their own lives that needed greater attention, such as diet, exercise, or sleep. It was anticipated that they would cultivate an appreciation for the commitment and work required by patients to establish daily habits that support their well-being. Students reflected on how the information from the course could be integrated into a broader landscape of patient care. The students’ final assignment was to design the future of healthcare with the intention of stimulating a path for the students as future leaders towards building innovative and more effective medical models for the future.
The project had several limitations, including a lack of student diversity and a small sample size. It is unknown whether a more diverse and larger group of students would provide the same positive feedback or suggest additional improvements to the curriculum. The one-month duration of the elective limits the opportunity for medical students to observe the long-term impact of IM interventions. However, the month-long rotation exceeds the typical two-week IM elective, which often lacks immersive clinical experiences.
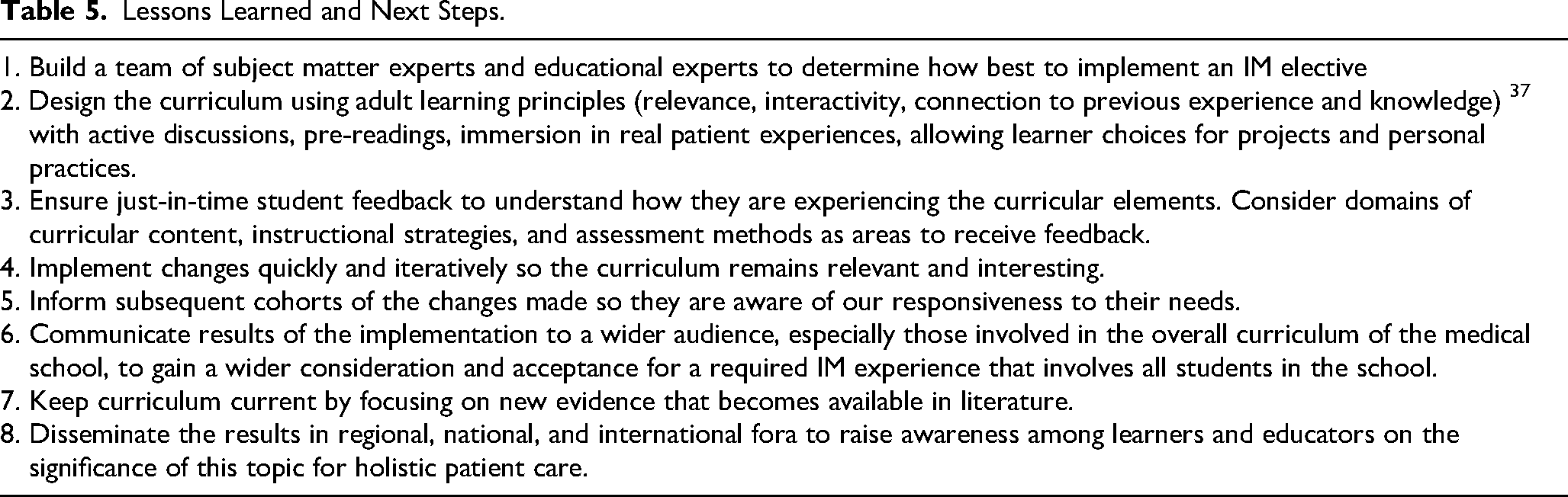
A plan is in place to integrate the IM elective into our school's required curriculum on flourishing and wellness across all four years of medical school, which may stimulate an interest in an expanded model of care among medical school graduates. With dissemination across national platforms, there is a distinct possibility that other schools will consider adopting or adapting such approaches to integrate learner wellness and integrative medicine practices throughout the entire medical school curriculum. Based on the experiences with the three pilot cohorts for the IM elective, various early lessons were learned that may be helpful for other health professions schools as they contemplate including IM into their existing curricula (see Table 5 for Lessons Learned and Next Steps). As IM training becomes more widely prevalent among medical schools, integration of such training and practices into other training phases including graduate and continuing medical education as well as other health professions training programs such as nursing, physical therapy, and others, has the potential to truly impact patient-centered evidence-based integrative and holistic model of patient care focused on patient interests. With such expanded training, the future of healthcare will be in the hands of IM-trained medical professionals who can utilize both standard medical and complementary approaches to enhance the health and well-being of all patients.
Lessons Learned and Next Steps.
Conclusion
Although there is evidence that whole-person integrative medicine is effective for enhancing health and well-being, there are knowledge gaps in IM among healthcare professionals that prevent the application of IM practices in patient care. Moreover, there is a lack of literature on the effectiveness of curricula used in existing medical school courses. The aim of this project was to develop and refine an IM elective to improve future physicians’ knowledge, skills, and self-care practices. Just-in-time feedback and curricular revisions appeared effective for student training and scalable to other medical schools. Further research is needed to develop, evaluate, and enhance IM curricula that incorporate greater student diversity and larger sample sizes. This is a first step toward integrating IM into the required curriculum for all students at UM, ensuring that we close the knowledge gap in IM among future physicians. Empowered with that knowledge, we anticipate them serving their future patients with a more holistic and patient-centered approach.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251389390 - Supplemental material for Implementing a Curriculum to Advance Integrative Medicine Education for Medical Students: Early Lessons and Next Steps
Supplemental material, sj-docx-1-mde-10.1177_23821205251389390 for Implementing a Curriculum to Advance Integrative Medicine Education for Medical Students: Early Lessons and Next Steps by Karen Koffler, Kassandra M. Bosire, Teresa Glynn, Latha Chandran, Anisha Durve, Edward Robert Schwartz, Joan St. Onge and Laura Redwine in Journal of Medical Education and Curricular Development
Supplemental Material
sj-pdf-2-mde-10.1177_23821205251389390 - Supplemental material for Implementing a Curriculum to Advance Integrative Medicine Education for Medical Students: Early Lessons and Next Steps
Supplemental material, sj-pdf-2-mde-10.1177_23821205251389390 for Implementing a Curriculum to Advance Integrative Medicine Education for Medical Students: Early Lessons and Next Steps by Karen Koffler, Kassandra M. Bosire, Teresa Glynn, Latha Chandran, Anisha Durve, Edward Robert Schwartz, Joan St. Onge and Laura Redwine in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We thank Emily Del Rio who as the Osher Center for Integrative Health project manager played a major role in organizing the course.
Ethical Considerations
The IRB Ethics Review Committee at the University of Miami approved our surveys (approval: 20221345) on 1/18/2023.
Consent to Participate
Respondents gave written consent for review and signature before starting the surveys.
Authors’ Contributions
All authors made a significant contribution to the concept, design, acquisition, analysis and or interpretation of data. All authors were involved in drafting or revising the article critically for important intellectual content. All authors approved the final version of the article for publication and agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bernard Osher Foundation Endowment.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.