
Abstract
Background
The ability to provide informed consent (IC) is a critical component of patient autonomy. Medical training programs have recognized the importance of training physicians to become skilled in obtaining IC, but few have reported curricula that address IC separately from broader ethical principles. This review aims to consolidate current methodologies and outcomes regarding medical education on informed consent.
Methods
Adhering to PRISMA-ScR guidelines, studies were obtained from PubMed and MedEdPORTAL that focused on evaluating the need for informed consent education and on assessing strategies to teach informed consent. Educational programs or assessments that focused broadly on medical ethics without a specific focus on the teaching of informed consent were excluded.
Results
Of 142 abstracted articles, 59 were included for analysis. 34 were categorized as needs-assessments, while 25 were interventions. Across various medical and surgical specialties and training levels, there is a need for more robust education on informed consent. No standard process for training medical learners about this topic exists currently. Of the interventions examined, both didactic curricula and simulation-based modalities demonstrated efficacy in improving knowledge and comfort levels with IC.
Conclusions
This review summarized both studies on needs assessments of IC education in medical training and on interventions to improve trainees’ skills in obtaining IC. Though obtaining IC is a critical clinical skill for nearly all clinicians, there is no consensus method to teach IC, satisfaction with current IC education is low, and debate exists on whether IC can ever be entrusted to trainees. These important gaps in IC education suggest a need to develop a structured, systematic approach to providing IC education in order to assure competency in this essential skill for patient safety and trainee wellness.
Introduction
Informed consent is based on 4 core principles of biomedical ethics: autonomy, beneficence, nonmaleficence, and justice.1–3 Personal autonomy is defined as self-rule that is free from both controlling interference by others and from limitations that prevent meaningful choice. 1 Informed consent for medical care or a surgical procedure takes into account all of these principles; it requires that the patient has the medical decision-making capacity to understand and make a decision, receives information they can understand about the indications, risks, benefits, and alternatives of a proposed intervention, and that they act voluntarily. 4
The ability to obtain informed consent is a critical component of patient autonomy in modern healthcare. 5 Virtually all clinicians obtain informed consent as part of their routine practice.5,6 This clinical skill involves providing the patient with a reasonably comprehensive review of the rationale, risks, benefits, alternatives, and nuances involved in a medical decision, so that the patient may make an informed choice. The clinician needs to confirm that the patient has understood the information and is making a decision without undue outside influence; only then can the decision be acted upon.6,7 Informed consent is becoming increasingly pertinent to modern healthcare as the medical field expands its range of services into increasingly complex territories, such as reproductive medicine and medical genetics, and, in response, patients and medical societies alike emphasize the importance of shared decision-making.8–11 Thus, the ability to obtain and document informed consent is a critical and necessary physician skill to honor a patient's right to autonomy, a foundational medical ethics principle. 12
A physician must undergo special training to become skilled in obtaining comprehensive informed consent (IC) from patients. The Association of American Medical Colleges (AAMC) has made obtaining IC part of its core entrustable professional activities (EPAs) for entering residency. 13 Outside of the world of medical education, a physician's ability to obtain IC is also under legal scrutiny. The tort of negligence, a prominent legal theory, notes that it is a civil wrong when a foreseeable risk is not communicated and so implies that physicians are obligated to communicate “all facts necessary to form the basis of an intelligent consent by the patient to proposed treatment.”14,15 The medicolegal complexities of IC continue to grow as more novel and advanced therapeutics are introduced to medical care and legal cases arise challenging our previous understanding of sufficient informed consent.16–18 Despite the recognition from medical education professional societies that IC is a foundational skill for clinical practice and the backdrop of growing legal ramifications to improper IC, existing curricula on this topic are generally a small part of preclinical ethics didactics and may not be readily applicable to the variety of clinical situations trainees face.19–21
Other authors have recognized this issue and have worked to synthesize current literature on IC education. For example, reviews exist that have identified key components of IC for surgical procedures, pointed out gaps in resident IC competencies, and devised a schema for improving IC education for surgical residents.6,12,22 However, a broad review of the literature, irrespective of clinical specialty, has not been completed. This review aims to consolidate current literature of medical education on informed consent, ranging from medical students to physicians of various specialties, including those from international programs. Our goals are to understand the successes and failures of current IC education and to identify the components of all reported medical IC curricula. This is the first step in creating a reliable methodology for teaching medical professionals to obtain comprehensive informed consent.
Methods
Study Design: PRISMA-ScR
This review aims to investigate how effectively informed consent is taught to medical professionals and which methodologies are currently used. To address both arms of our question, we sought out studies that reported on educational curricula on obtaining IC and studies that assessed the adequacy of current informed consent training. In consideration of the mixed methodologies of the studies included with the majority not reporting statistical analyses, we utilized thematic analysis to produce our results. 23 Outcomes examined were performance and confidence in obtaining informed consent, as well as feasibility of different curricula and methods. This review was conducted according to Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.
Eligibility Criteria
Studies were eligible for initial inclusion if they: (1) focused on education and/or assessment methods of any level medical trainee or physician in their ability to obtain informed consent and (2) targeted our broad population of interest, including medical students, residents, physicians, and residency program directors. Studies were included if they were published between January 1, 1990, and December 12, 2024.
Studies were ineligible for inclusion if they were not written in English or were review articles. Articles on other allied professionals, like nursing or social work, were excluded. We also excluded articles on educational programs or assessments that focused more broadly on medical ethics if they did not evaluate the needs of informed consent education specifically or evaluate their curriculum specifically on informed consent knowledge or skill as an outcome (Figure 1).

PRISMA Flowsheet.
Information Sources
Studies were obtained from PubMed, MedEdPORTAL, Education Source, and ERIC, using search terms “informed consent education,” “medical education informed consent,” “resident education informed consent,” “informed consent education in residency,” and “education in informed consent.” No quotations were used in searches. A fully reproducible search strategy is available in Supplementary Table 1. The references of included articles were reviewed for articles that did not appear in our searches, and any eligible studies were added to the list of articles for further review. Authors SC, CM, CG, AB, and YEX independently identified eligible studies by assessing title and abstract and sought consensus for any discrepancies at regular group meetings. Studies deemed relevant for inclusion were read in full by either SC, CM, CG, AB, or YEX, and a summary was shared with all authors. All reviewers then discussed each article summary to achieve consensus on the studies included in the final analysis.
Data Abstraction
All authors contributed to data abstraction. The following data were extracted after full text review: (1) Article title, (2) Citation, (3) Journal, (4) Educational tool or survey used, (5) Goal of study, (6) Study population, (7) Results, (8) Author's comments, (9) Study limitations. Collective practice with the data abstraction allowed for adequate standardization. The articles were divided between team members and monthly meetings were held to discuss salient findings, track progress, and address any concerns.
Analysis and Synthesis
All authors convened to analyze the included articles and synthesize our results. Each included article was categorized into 2 groups: (1) Needs Assessment and (2) Intervention. Articles in Group 1 were labeled according to subject training level and country of origin. Articles in Group 2 were labeled according to subject training level, country of origin, type of intervention, and method of intervention evaluation, if applicable. Two authors (YEX and CG) independently evaluated the quality of each included study using the standard medical education research study quality instrument (MERSQI) tool; disagreements were resolved by a third author (SC). 24 We additionally examined trends in study number and study quality (based on MERSQI scores) over time with descriptive statistics. Finally, a list of abbreviations was compiled (Supplementary Table 2).
Results
After abstract screening, a total of 142 articles were identified for full-text review, 59 of which were included for analysis. Reasons for exclusion of the remaining articles are outlined in Figure 1. Results are structured according to the PRISMA-ScR criteria.
Need Assessments
Study Participants
Needs assessment studies totaled to 34 articles (Table 1).13–45 Needs assessments were intended to query medical students,25–27 residents,25,28–53 fellows, 54 or attending physicians and medical school faculty,34,35,39,41–46,52,55,56 regarding self-perceptions of their knowledge, skill, and education related to informed consent. The majority of studies investigated a wide range of medical student and resident training levels.25,28–37,39,40,42,43,53 Fewer studies specifically investigated postgraduate year 1 residents38,51,57 or students in their final year of medical school.26,27,50,57 A small number of studies presented surveys of the most diverse population of trainee levels as they investigated IC training among medical students, residents, fellows, advanced practice providers, and attendings.44,45,58 A minority of studies specifically investigated various program directors’ educational models on informed consent and their perception on how well their programs taught informed consent to their trainees.37,54,59 One study investigated physicians’ understanding of informed consent and their performance in obtaining consent by providing questionnaires to patients to assess their understanding of the risks involved in their respective procedures. 52
Summary of Studies Assessing the Need for Informed Consent Education.

NR = not reported; PGY = postgraduate year; SP = standardized patient; OSCE = objective structured clinical exam.
Location of Studies
Nearly half of the studies were conducted in the USA, with Australia (4),33,42,47,52 Canada (3),26,37,39 Ireland (2),48,51 Japan (1), 53 Kashmir (1), 55 Malaysia (1), 55 Netherlands (1), 46 New Zealand (1), 26 Nigeria (1), 40 Pakistan (1), 34 Saudi Arabia (1), 31 Uganda (1) 44 , and the UK (1) 49 representing the rest.
Study Design
Surveys were the main assessment tool that were utilized in the reviewed studies.25,28,29,31–36,40–42,47–49,53–56,58 These surveys investigated the participant's knowledge, education, experience, challenges, confidence, and comfort related to informed consent. Two studies assessed the status of ethics training in current residents by surveying program directors.37,59 A small minority of studies used multiple choice questionaries.46,51 Three studies utilized Objective Structured Clinical Exam (OSCE) and/or standardized patient (SP) encounter on obtaining informed consent.38,50,57 Two studies had an ethical dilemma essay completed by the participants.26,27 One study gave questionnaires to patients and conducted interviews with medical staff, 52 and 2 articles included information from chart reviews of prior completed informed consents.39,43 Other studies utilized a combination of different assessment methods, including surveys, written exam, and OSCE scores, 37 questionnaires, interviews, and chart reviews, 44 and interviews and focus groups. 45
Outcomes
While all studies underscored the importance of informed consent training, the majority of trainees learned informed consent process through direct observation.25,28,35,36,51 Trainees were unsure of all the risks to procedures while obtaining informed consent and did not have a structured way to assess decision-making capacity.28,31,32,36,37,40,46,47,51,58 Some trainees noted no formal training in neither medical school nor residency.25,30,33,34,40,47,53
One study using OSCEs demonstrated that the majority of interns showed moderate proficiency in obtaining informed consent, with a need for improvements in communication skills. 50 Another OSCE structured around informed consent completed by 258 incoming pediatric interns resulted in only 8 informed consents filled accurately. 38 Similar findings were shown in a retrospective chart review, where only 2% of 270 of surgical patients had accurate and completed informed consents. 39 Even with dedicated ethics modules within residency curricula, Padela et al noted there was no association between having a dedicated ethics module and informed consent knowledge scores. 41
Surveys noted that residents had greater confidence in obtaining informed consent as they progressed through residency training.28,32,34,35 When adequate training was conducted (eg boot camp, didactic session), residents were found to write significantly more detailed informed consents for simple surgical procedures (eg cholecystectomies). 43 Notably, studies showed that trainees perceptions of their knowledge and skill in informed consent did not always align with their reported practice.33,40,42,44
Attendings were noted to be knowledgeable in informed consent elements and completed surgical informed consent documentation more thoroughly than their resident counterparts. 46 However, Williams et al found the opposite; surgical residents performed better than attendings in documenting informed consent discussions in the outpatient clinical setting. 39 White et al examined how attending surgeons learned IC and found that 86% of sampled attending surgeons learned IC through observation of another attending; furthermore, surgeons in this group who reported learning by observing were more likely to teach by having residents observe them, as well. 56
Multiple studies identified that a large proportion of physicians in postgraduate training had little prior training in IC. About half of the respondents in the study by Anderson et al never received training on how to obtain informed consent in medical school. 25 As for residency curricula, the majority of training programs studied only spent between 0 and 10 h per year on ethics education,37,59 and none of the residency program that were studied had a consistent approach to teaching or evaluating informed consent skills. 37 The majority of queried fellowship directors “rated their programs as ‘strong’ or ‘very strong’ in preparing trainees to obtain informed consent; however, 28% of these fellowship programs reported having no formal curricula on obtaining informed consent. 54
Only 1 study evaluated the efficacy of the IC process for educating patients on the procedures they received and found that patients had poor understanding of their disease, the intervention options, and possible complications of the procedures after completing the IC process with a clinician. 52
Overall, these needs assessment studies underscored a crucial need to have formalized training in obtaining informed consent early in residency.28–38,40,41,43–47,50,53,54,58,59 Surveys noted residents requested more education to help them address difficult topics in informed consent (eg obtaining informed refusal, or handling patients with compromised decisional capacity).29,40
Interventional Studies
Study Participants
Overall, 25 articles reported on educational methods for IC. Interventional methods studied were aimed at educating mostly residents57,60–73 and/or medical students.65,68,74–81 Of the 14 resident-targeted interventions, 9 addressed first-year residents,57,60–62,67,69–71,73 4 covered multiple levels of resident trainees,60,66,72,82 and 5 did not specify postgraduate year(s) targeted.62–64,66,68
Location of Studies
Most (93%) interventional studies were conducted in the United States. Canada was also represented.64,83
Procedure or Skill Evaluated
Most of the interventions aimed to educate trainees in procedural specialties or focused on obtaining IC for procedures. These included transfusion, surgery, emergency procedures, interventional radiology procedures, or a combination of procedures.60–65,67,71–74,83 A smaller proportion were neurology or psychiatry-based, often involving decision-making capacity77,79,80,82, or centered around pediatric cases68,69, or devoted to obtaining consent for general anesthesia 70 or chemotherapy. 78
Methods
Most educational interventions reported utilizing multimodal education programs featuring some combination of didactics (traditional classroom-based lectures on IC), small group discussions (case-based discussions among peers), standardized patient or simulated encounters where trainees role-played obtaining IC, individually reviewing sample cases on obtaining IC, and/or self-study of the principles and practice of obtaining IC (Table 2).
Summary of Studies About Informed Consent Curricula.
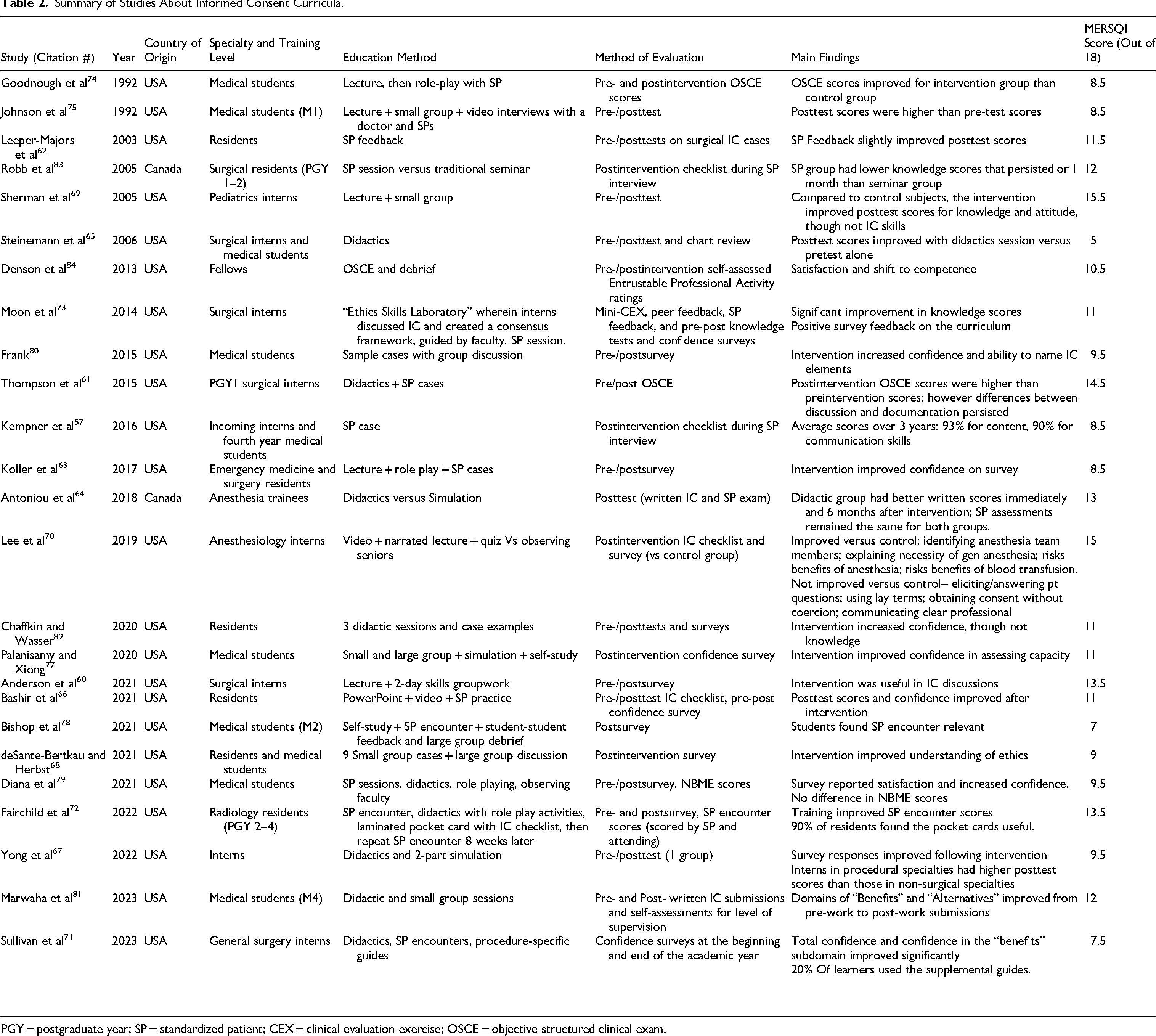
PGY = postgraduate year; SP = standardized patient; CEX = clinical evaluation exercise; OSCE = objective structured clinical exam.
Though all studies described their intervention and the impact of their curricula as a whole, only a handful of studies specifically examined the effects of any tool in isolation. Leeper-Majors et al looked at the impact of adding SP feedback to their video-based didactic lesson 62 ; Antoniou et al compared didactic teaching versus a SP session 64 ; Lee et al compared IC-gathering performance among students who either watched a lecture or observed faculty obtaining consent 70 ; both Steinemann et al 65 and Chaffkin and Walker 82 studied the impact of didactic sessions on knowledge regarding IC; Palanisamy and Xiong conducted a 4-day, small group-based, role-playing exercise 77 ; Frank conducted group-discussion of IC-focused sample cases 80 ; and Denson et al used an OSCE and an accompanying debrief session. 84 Fairchild et al also provided laminated pocket cards with an IC checklist for residents to use throughout the study period. 72 Four studies utilized real-time feedback as a teaching tool, either from SPs or other students.57,62,73,78
There were also a variety of strategies used to evaluate the effects of the educational intervention. A smaller number of studies investigated the effects of their educational intervention on OSCE scores.61,74 Many evaluated interventions via postintervention written assessments,62,64–66,69,73,80,81,83,85 which in most cases assessed knowledge of the components of informed consent.69,80 Surveys of trainee confidence in obtaining IC and/or satisfaction with the educational tool were also commonly used to evaluate the intervention.63,66,67,71,73,77–80,84 Sullivan et al included levels of attending confidence in trainees’ ability to obtain IC before and after the intervention. 71 Most studies only conducted short-term evaluation of their interventions. Three studies extended this with postintervention tests 1 month, 83 2 months, 72 or 6 months 64 after the initial educational intervention.
Outcomes
Among the studies that investigated the effects of their educational intervention on OSCE scores, Goodnough et al found that OSCE scores were higher for medical students who participated in a lecture and small group simulated patient session than those who did not. 74 Similarly, Thompson et al found that surgical interns scored higher on their post-didactics and SP cases OSCE than preintervention, though they also noted that differences remained between what the surgical interns discussed in the SP encounter and what they documented. 61 Fairchild et al found significant improvement in OSCE scores after their intervention of readings, a lecture, and a pocket-card IC checklist. 72
For studies that evaluated interventions via postintervention written assessments, interventions that led to improved postintervention scores were didactics and lectures,64,65,69,75,81 group discussions,69,75,80,81,83 sample videos or role-plays with physicians,66,69,75 and SP simulations.62,66,73,75 Postintervention scores in study groups were compared to preintervention scores in the same study group62,65,66,69,75,77,82 or with scores from a control group.64,66
For studies that surveyed trainee confidence in obtaining IC and/or satisfaction with the educational tool, interventions that resulted in improved confidence and/or satisfaction were mostly multimodal, encompassing a combination of a lecture and a role-play scenario (including SP cases),63,66,67,71,72,77–79 or a lecture with either a small group project, skills groupwork, or case examples.67,82 Confidence was also improved with unimodal approaches, such as OSCE, small group simulation, or sample case discussion.77,80,84 Interestingly, 1 study evaluated the efficacy of its OSCE with self-reported EPA ratings, although ratings were not published. 84
Among studies that utilized feedback as an instructional tool, one found that residents who received SP feedback on their IC skills had a greater improvement in pre- to postintervention scores than a control group that received an instructional video alone. 62 Bishop et al did not evaluate whether feedback impacted skills, but when surveyed, the students did report the exercise as useful; Bishop et al also suggested that the exercise may be improved with the addition of feedback from clinical faculty. 78
For studies that followed outcomes over extended periods of time, Robb et al found that the residents provided training on IC through SP had lower knowledge scores when assessed 1 month following the intervention than residents who only received the traditional seminar on IC. 83 Fairchild et al found that improvement in OSCE scores persisted 2 months after their intervention of readings, a lecture, and a pocket-card IC checklist. 72 At the end of the academic year, the attendings in the study by Sullivan et al rated their confidence in surgical interns’ IC abilities similarly to the beginning of the year prior to the simulation-based intervention. 71 Antoniou et al found that, although both didactic and simulation groups had significant immediate postintervention improvements in IC documentation compared to baseline, only the didactics group had persistently elevated scores 6 weeks postintervention. 64
Trends in Study Quantity and Quality
The number of studies identified focusing on informed consent education has increased over time, with 4 studies from the 1990s, 10 studies from the 2000s, 25 from the 2010s, and 19 from 2020 to 2024. MERSQI scores of needs assessment studies were on average lower than those of intervention studies (8.6 vs 10.6). The quality of needs assessment studies remained relatively stable over time; the MERSQI score average was 8.5 for studies from the 1990s, 7.8 for studies from the 2000s, 8.9 for studies from the 2010s, and 8.5 for studies from the 2020s. On the other hand, the quality of intervention studies on average improved from the 1990s to the 2000s and have remained at a higher level of quality since then; the MERSQI score average was 8.5 for studies from the 1990s, 11 for studies from the 2000s, 11.3 for studies from the 2010s, and 10.4 for studies from the 2020s (Tables 1 and 2).
Discussion
Our study reviewed both studies on needs assessments of informed consent education in medical training and on interventions to improve the education of informed consent. Our results demonstrated that across different medical specialties and different training levels and for at least the past 30 years, there has been a need highlighted in the literature for more robust education on informed consent. In addition, we found that despite an increased interest in informed consent education over time, as demonstrated by an increase in the number of studies and an increase in attention to study quality, there remains no standard process for training medical learners about this topic. Of the interventions examined, we found that didactic curricula, small group discussions, and simulation-based curricula were most frequently adopted and shown to be effective in improving trainees’ competence in obtaining IC. Specifically, these 3 modalities all demonstrated efficacy in improving learners’ knowledge of the relevant ethical principles and components of IC, their clinical skills in obtaining IC, and comfort level with performing this skill. However, it is unclear whether these interventions lead to sustained improvements in trainees’ skills. Only 3 studies evaluated whether improvements in IC knowledge and skills were sustained over time and had mixed results with some suggesting persistent improvement after 1–2 months, while another found no difference in skills after 1 year. More research on the retention of learned skills with these interventions would help clarify this matter. Our results also found a paucity of data on how assessing decision-making capacity is taught, despite it being a crucial component of obtaining informed consent.
Integration
Previous reviews of informed consent education have focused on how IC is obtained in surgical specialties or for specific procedural interventions.6,11,16 Our review broadens the scope and provides a wider view of informed consent education across specialties and training levels. Our findings align with previous reviews and support the conclusion that more robust informed consent education is needed in medical education. Trainees often report learning to obtain informed consent through direct observation of more senior team members, but note insufficient formal education on this topic. Trainees’ performance of this critical healthcare skill also often shows deficiencies. Though results suggest that comfort and knowledge in obtaining informed consent improve with more years of training, it is alarming to see that not all studies find that attending physicians are better at obtaining and documenting appropriate informed consent when compared to their trainees.
It is also worth noting that despite the many studies on teaching informed consent, there remains a debate in the literature on whether obtaining IC should be a core EPA. 86 White et al raised the concern that because surgical attendings often do not entrust the obtaining of IC to residents regardless of resident competency in the matter, IC may not be entrustable at all. 86 These findings suggest that there may be additional barriers to a standardized and effective approach to teaching and entrusting IC beyond the lack of consistent and robust curricula on IC. Though our study did not address these concerns, our review collated the large amount of work that has already been done globally to assess and improve our education on informed consent to medical trainees. Our findings illustrate that there is little standardization of methods and timing of IC education, but that we have the necessary foundational elements to create a meaningful and measurable IC curriculum for medical trainees. We suspect that the creation of such a curriculum will increase attendings’ comfort with entrusting IC to trainees and productively contribute to this debate on IC as an EPA.
Implications
Given these findings, we call for medical educators across all specialties to examine how informed consent is taught in their respective programs. Obtaining informed consent is a foundational skill for all clinicians to practice ethically, and the inadequate training and limited confidence and skill learners report having in this area have immediate and significant implications for the quality of care they will provide for their patients. The ability for patients to give informed consent is core to their autonomy in healthcare, and the nuances around how to obtain consent appropriately are critical for all patients, but especially true for special populations, including children, the elderly, those with cognitive impairments, and those with mental health disorders.87,88 These vulnerable populations necessitate a higher level of rigor in ensuring that adequate informed consent has been obtained and that standards specific to their population have been adhered to. For example, in children, informed consent should additionally involve the child's participation, as developmentally appropriate, and assent from the child, when possible, though formal consent will be given by their legal guardian. 89 As for those with cognitive impairments or severe mental illness, a more rigorous assessment of decision-making capacity is imperative, as well as familiarity with the process of identifying and utilizing legal medical decision-making proxies and advanced directives.90–92 This suggests that medical educators may need to develop longitudinal curricula where obtaining IC from adults without cognitive impairments is taught first and then more advanced training on informed consent in special populations is presented afterwards to build on previous learning. Appropriately obtaining and documenting informed consent is also increasingly important due to the heightened legal scrutiny over this element of healthcare, adding another layer of relevance to learners as they prepare for independent practice. 93
As such, there needs to be more research done on this topic, especially studies comparing the efficacy of different interventions to improve the skill of obtaining informed consent and studies exploring ways to encourage long-term retention of these skills. We also need to develop standard processes to evaluate how well learners obtain informed consent to facilitate the tracking of their progress across training years. Ultimately, we need to develop a structured method and curriculum to teach and assess trainees’ competency in this area, including capacity assessments as part of informed consent. Based on the findings of this study, we have created an outline of suggested curricula for medical students and residents (Tables 3 and 4). Further development and application of such curricula will meaningfully improve our trainees’ ability to provide care, and thus also the care that our patients receive, by developing more robust educational systems around the core skill of obtaining informed consent.
Outline of Proposed Medical Student Curriculum on Informed Consent.

Outline of Proposed Resident Curriculum on Informed Consent.

Limitations
Our review had multiple limitations. The quality of the studies available for analysis was limited by study design. The bulk of the needs assessment studies were surveys, and there were no randomized control trials among the studies of interventions. End points were often assessed without previously validated tools, and generally only descriptive statistics were provided. The majority of the studies on interventions also did not assess learners’ performance in obtaining informed consent from patients; thus, we could not draw conclusions on whether the studied interventions would significantly improve patient outcomes. These limitations are reflected in the moderate MERSQI scores that most of the included studies received, with the average score being 9.5 of a maximum 18. Our study was also limited by the variability in the endpoints examined in the studies, thus making it more challenging to compile results and preventing us from completing more statistical analyses on the data.
Conclusion
Obtaining informed consent is a critical aspect of upholding patient autonomy and is of growing legal relevance. Despite these realities, our review found that across specialties and training levels, informed consent education has lacked robust, standardized curricula for at least the past thirty years. Didactic, small-group, and simulation-based methods all improve trainees’ knowledge, skills, and comfort with IC, but evidence on long-term retention of this skill is limited and mixed, warranting further study. It is paramount that the medical education community develop longitudinal and structured IC curricula, as well as standardized methods to assess IC competency. To this end, we have proposed a framework for evidence-based IC education, spanning undergraduate and graduate training. Ultimately, advancing IC training will enhance the medical profession's ability to deliver ethical, patient-centered care, and our review provides concrete next steps toward this important goal.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251384380 - Supplemental material for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review
Supplemental material, sj-docx-1-mde-10.1177_23821205251384380 for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review by Sophia Chryssofos, Cynthia Glickman, Cyrus Mowdawalla, Amanda Burden and Yingcheng Elaine Xu in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251384380 - Supplemental material for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review
Supplemental material, sj-docx-2-mde-10.1177_23821205251384380 for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review by Sophia Chryssofos, Cynthia Glickman, Cyrus Mowdawalla, Amanda Burden and Yingcheng Elaine Xu in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251384380 - Supplemental material for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review
Supplemental material, sj-docx-3-mde-10.1177_23821205251384380 for Current Practices, Limitations, and Recommendations for Informed Consent Education in Medical Students and Physicians: A Scoping Review by Sophia Chryssofos, Cynthia Glickman, Cyrus Mowdawalla, Amanda Burden and Yingcheng Elaine Xu in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgments
We would like to express our gratitude to Dr. Douglas Coursin, MD and Dr. Katherine K. McMackin, MD, MS for their guidance and advice during the drafting of this manuscript.
Ethical Approval
Ethical approval for this work was not required because it is nonhuman subjects research.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
All authors contributed to the literature search and analysis of identified articles. SC, CM, CG, and YEX drafted the manuscript. YEX and CG assessed the quality of all included studies and completed revisions of the manuscript. AB provided guidance on the drafting of the manuscript and subsequent revisions. YEX, CG, and AB conceived the project. YEX supervised the project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.