
Abstract
OBJECTIVE
Anatomy, a foundational preclinical course in medical education, is crucial for students. However, a comprehensive comparison of case-based learning (CBL) and lecture-based learning (LBL) in anatomy instruction is lacking. This study investigates the effectiveness of CBL and LBL methods in a lower limb anatomy course, evaluating medical students' satisfaction, attitudes, knowledge, and skills.
METHOD
This prospective cohort comparison study was conducted over three academic years, using a hybrid instructional approach to accommodate COVID-19 protocols. Six groups of undergraduate medical students (n = 466) were randomly assigned to either CBL (n = 231) or LBL (n = 235). Both groups had the same curriculum, learning objectives, and instructor. The LBL group received lectures, while the CBL group engaged with clinical cases and radiographic images, followed by interaction and knowledge application. Questionnaires were used to collect data on student demographics, satisfaction, and attitudes, and learning progress was assessed through tests. Data were analyzed using SPSS 22 with t-tests, Wilcoxon tests, and Pearson's correlation coefficient (≤ .05).
RESULTS
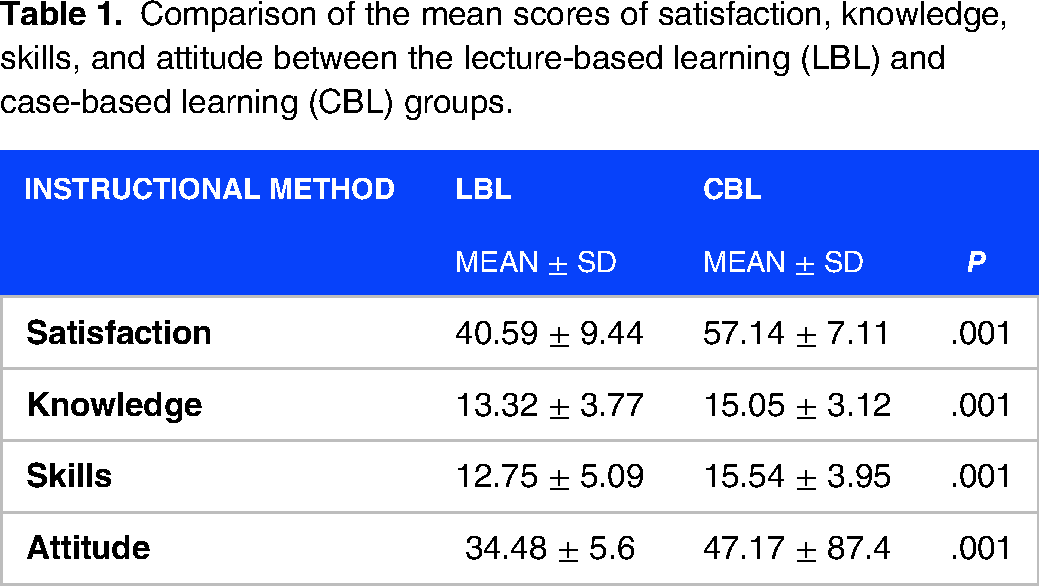
Compared to the LBL group, the CBL group demonstrated significantly higher levels of knowledge (15.05 ± 3.12 vs. 13.32 ± 3.77; P < .001) and skills (15.54 ± 3.95 vs. 12.75 ± 5.09; P < .001). Students in the CBL group also reported significantly greater satisfaction (P < .001) and a more positive attitude toward the learning method (42.78 ± 8.01 vs. 34.7 ± 35.64; P < .001).
CONCLUSION
CBL significantly enhances knowledge, skills, satisfaction, and attitudes of first-year medical students learning lower limb anatomy. This makes CBL an effective instructional method for anatomy courses.
Introduction
Competency-based medical education (CBME) is an outcomes-based approach to designing, implementing, and evaluating educational programs and assessing learners across the continuum that utilizes competencies or observable abilities. 1 CBME aims to ensure that all learners achieve the desired patient-centered outcomes during their training and emphasizes the development of cognitive, psychomotor, and affective skills essential for future clinicians. Additionally, CBME incorporates newer teaching and learning methods, such as small group teaching and role-playing, which can enhance the learning experience for students. 2
A competency-based curriculum emphasizes what learners are expected to do rather than primarily focusing on what they are expected to know. 3 Such a curriculum is learner-centered and adaptive to the changing needs of students, teachers, and society. Several methods have been developed to promote active and compelling interactive learning. Three commonly utilized methods include problem-based learning (PBL), case-based learning (CBL), and team-based learning (TBL). Although CBL was first described in 1912 by Lorrain Smith at the University of Edinburgh and adopted by Harvard Business School in the 1920s, its instructional use in health and medicine became commonplace in the 1990s. 3
CBL attempts to link basic scientific understanding (commonly delivered via lectures) to future clinical practice. Students are typically expected to complete readings or assignments before the CBL session, and learning objectives are communicated before the session begins. 4 Students use higher-order cognition to assess their understanding of the concepts by debating a clinical case associated with the lesson. 1
Anatomical science is the cornerstone of medicine and surgery, utilized by physicians daily to analyze radiographic images, interpret exam results, and communicate with other medical professionals. Therefore, teaching anatomy is crucial for medical students. 3 Additionally, clinically oriented anatomy education has been proposed as an effective strategy in anatomy curricula; however, studies on the effectiveness of the CBL instructional method in anatomy education are limited, and most studies have measured students’ perceptions rather than their knowledge levels. 4 Consequently, this study aimed to design, implement, and evaluate CBL to improve undergraduate medical students’ satisfaction, attitude, knowledge, and skills in the anatomy course.
Methods
This prospective cohort comparison study was performed at the Hamadan University of Medical Sciences, Hamadan, Iran, over three spring semesters in three consecutive academic years (the second semester of 2020, the first and second semesters of 2021, and the first and second semesters of 2022). In 2020, the study began during the second academic semester, which runs from March to June each year in Iran. To address potential COVID-19 contact restrictions, the instructional methods were delivered through a hybrid approach, combining in-person sessions with online components to ensure adherence to health protocols.
After the course was presented in both groups, student satisfaction and attitudes regarding the instructional method, and their knowledge and skills, were measured. The Ethics Committee of Hamadan University of Medical Sciences (IR.UMSHA.REC.1399.423) approved the study protocol, and each participant provided informed consent before enrollment. The article is presented in accordance with the Guideline for Reporting Evidence-based practice Educational interventions and Teaching (GREET) checklist (Supplementary 1). 5
Study population
The study population consisted of all undergraduate medical students enrolled in the lower limb anatomy course during the study period. Each academic year in the second semester included 2 classes of undergraduate medical students. Thus, by lottery, one class was assigned to the interventional group receiving CBL, while the other class served as the control group receiving LBL. The inclusion criterion was medical students in their first year of medical school, while the exclusion criterion was students who had not passed this course before.
Sample size
The sample size was estimated to be 185 people based on the formula for comparing the ratio of response to treatment in three groups and its parameters, specifically a 99% confidence coefficient (1−α) and a 99% test power (1−β). The values of μ1 and μ2 were selected from the study by Anwar Alhazmi et al. 5

Finally, 466 students from 6 groups of 77 to 78 participants (CBL= 231 vs. LBL= 235) participated in this study.
Study design
The study design incorporated several measures to moderate potential confounding factors. The course curriculum features, including the content, learning objectives, and duration, were identical between the CBL and LBL groups, as both cohorts were enrolled in the same lower limb anatomy course. Additionally, the same instructor taught both groups, controlling for potential instructor effects. Each year, the comparability of the 2 class populations was assured by examining the students’ characteristics, such as gender, age, and prior academic performance, using the Chi-squared test and t-test as appropriate. These statistical analyses revealed no statistically significant differences between the CBL and LBL groups on any examined student characteristics (all P > .05). This indicates that the random assignment procedure successfully created comparable class populations at baseline across these key demographic and academic factors. Furthermore, the CBL and LBL groups students were housed in separate dormitories, which helped minimize the risk of contamination bias.
The lower limb anatomy course was a 2-unit course held for 4h per week during the semester, including 8 theory and 4 practical sessions. The course content covered the osteology of the lower limb, the anterior compartment of the thigh, the medial compartment of the thigh and gluteal region, the posterior compartment of the thigh and popliteal region, the posterior compartment of the leg, the anterior and lateral compartments of the leg and foot, and the lower limb joints.
The learning objectives were for students to be able to describe the muscle compartments of the lower limb, detail their attachments, actions, innervation, and blood supply, recognize clinical presentations of lower limb movement abnormalities, and formulate appropriate diagnoses.
Intervention
LBL group
Before the session, the LBL group students were assigned 7 to 8 small groups for practical sessions. In an orientation session, they were all informed about the teaching process. All the students in the LBL group received traditional didactic lectures on the lower limbs anatomy course for the entire 8-week semester. Each lecture session lasted 2h, for a total of 16 lecture hours. The instructor covered both normal anatomy and provided examples of pathologies and radiograph. In the practical sessions, which were 2h long and held weekly, the teacher used moulages, cadavers, and relevant radiographic images related to the session's anatomical content to teach the material, and the students examined the learned content in assigned small groups of 7 to 8 students. The students were advised to read the relevant chapter from Gray's Anatomy for Students before the class (Figure 1a).

Sequence of educational activities for the LBL (a) and CBL (b) groups.
CBL group
Collaborating with an orthopedic specialist, the course instructor designed 10 clinical cases augmented by authentic radiograph of orthopedic patients with broken legs and deformities. These cases were to be covered over 8 weekly sessions to address all the essential educational objectives of the lower limb anatomy curriculum. The CBL items were reviewed and refined by members of the Anatomy Group at the Medical School to ensure they adequately addressed any potential deficiencies in the curriculum. The students in the intervention group were assigned to small groups of 7 to 8 learners and received an orientation on the CBL teaching approach prior to the start of the course. This orientation was intended to familiarize the students with the CBL format and prepare them for the interactive nature of the sessions. The students were advised to read the relevant chapter from Gray's Anatomy for Students before the class.
Each weekly 2h session (totaling 16h) began with introducing a clinical case relevant to the session's anatomical topic. This initial case presentation was followed by a lecture from the instructor covering the key anatomical features, including muscle origins, insertions, innervation, and function. After the introductory lecture, the students were asked to examine the presented case and the corresponding radiograph and identify the critical anatomical features discussed. This active learning component allowed the students to apply their knowledge and engage more deeply with the material. Finally, the instructor provided a 30-min follow-up lecture that revisited the clinical case, highlighting the relevant anatomical findings and tying them back to the educational objectives of the session. This helped solidify the students’ anatomical knowledge of real-world clinical scenarios. The students then worked in their small groups to identify the affected muscle, nerve, and function and propose a solution to the clinical problem. The instructor subsequently provided the correct diagnosis and appropriate treatment approaches, critiquing the students’ proposed solutions. Additional clinical cases were presented, and the student groups similarly analyzed them. Similar to the first case that described at beginning the class, the teacher reviewed it after the students examined it. As an assignment, each group of students was required to design 3 new clinical cases per session that aligned with the session's learning objectives (Figure 1b). The students submitted these case studies using the learning management system (Navid®).
In the practical sessions (2h weekly sessions), along with the moulage and cadaver, the students were provided with relevant radiographic images related to the session's anatomical content. The student groups were asked to analyze these images, identifying the visible vital features such as tissue types, muscles, vessels, and pathological findings (Figure 1).
Research tools
Four separate questionnaires were used for data collection, and all students answered the questionnaires. The details of these instruments were as follows:
Demographic data form: This form collected students’ information, such as age, marital status, place of residence, and grade point average (GPA) from the last semester. It was developed based on the demographic data form by Safari et al.
6
Student's Satisfaction Questionnaire: The “Student Satisfaction with Instructional Method Scale” is a self-administered questionnaire consisting of 18 questions scored on a 5-point Likert scale (from “very low= 0” to “very high= 4”). Some examples of its questions are as follows: “To what extent did the instructional method help to solve controversial issues in the classroom?,” “To what extent did the assignments motivate you to learn more?,” and “To what extent did the instructional method increase learning retention after the classroom?”. Both instructional methods were completed at the end of the course. Ten experts in medical education reviewed this questionnaire to determine its validity. The content validity ratio and index were .73 and .88, respectively. Additionally, to quantitatively determine the face validity, the impact score of 3.81, the intraclass correlation coefficient of .75, and the reliability coefficient (using Cronbach's alpha method) of .86 were calculated. Student's Attitude Questionnaire: This self-administered questionnaire contains 12 questions scored on a 5-point Likert scale (from “totally disagree= 0” to “totally agree= 4” for questions 1-10). The last 2 questions have a negative proposition (from “totally disagree= 4” to “totally agree= 0” for the last 2 questions). Some examples of its questions are as follows: “This instructional method leads to a better understanding of the subject,” “This instructional method has made me responsible,” and “This instructional method is an enjoyable way to learn in physical therapy.” Both instructional methods were completed at the end of the course. Ten experts in medical education reviewed this questionnaire to determine its validity. The content validity ratio and index were .78 and .85, respectively. Additionally, an impact score of 3.85, an intraclass correlation coefficient of .88, and a reliability coefficient using Cronbach's alpha method of .9 were calculated to assess the face validity quantitatively. Summative learning test: An electronic test (20 marks) with multiple-choice questions based on course plan objectives assessed students’ knowledge level after 2 LBL and CBL training courses. Additionally, a 20-point paper test using an objective structured practical examination (OSPE) was conducted to evaluate students’ diagnostic skills level after the same training courses. An expert panel confirmed the content validity of these instruments, and their reliability was established through test-retest, where McNemar's test showed no significant differences.
Statistical analysis
All statistical analyses were performed using SPSS version 22 (SPSS Inc., Chicago, IL, USA), and the results were reported as mean ± standard deviation (SD) for quantitative variables and as percentages for qualitative variables. Changes in quantitative variables after educational interventions were measured using the paired t-test or the Wilcoxon test. The associations between quantitative variables were assessed using Pearson's correlation coefficient. P of .05 or less were considered statistically significant.
Results
Demographic findings
The mean (SD) age of participants in the CBL and LBL groups was 22.64 (±1.92) and 22.73 (±3.61) years, respectively. The mean total score of final exams in the preceding semester was 15.48 (±0.82) in the CBL group and 15.37 (±1.32) in the LBL group (the highest possible mean total score is 20). Most students in the CBL (96.10%) and LBL (96.59%) groups were single. Additionally, 35.36% of the CBL group and 64.68% of the LBL group stayed in university dormitory facilities. No significant difference (P >. 05) was found regarding the features above between the 2 groups.
Satisfaction
Although the students’ satisfaction level with the instructional methods was high in both groups, the CBL group (57.14 ± 7.11) was significantly more satisfied than the LBL group (40.59 ± 9.44) (P = .001; Table 1).
Comparison of the mean scores of satisfaction, knowledge, skills, and attitude between the lecture-based learning (LBL) and case-based learning (CBL) groups.
Some satisfaction questionnaire items, including “To what extent did the instructional method increase learning retention after the classroom?,” “To what extent did the instructional method lead to better and deeper learning of the content?,” and “To what extent did the instructional method increase the level of communication and interaction between the teacher and the students in the class?” indicated a high level of satisfaction with the CBL instructional method (70%). In contrast, the satisfaction percentage for the LBL method based on the items from the satisfaction questionnaire was below 30% (Table 2).
Comparison of satisfaction levels after case-based learning (CBL) and lecture-based learning (LBL) methods.

Knowledge
After 2 training courses using the LBL and CBL instructional methods, the final knowledge scores of the students after the CBL method were significantly higher than those after the LBL method for anatomical and clinical questions (P <.001) (Table 1).
Diagnostic skills
After 2 training courses using the LBL and CBL instructional methods, students scored significantly higher in their diagnostic skills, as evidenced by OSPE, after the CBL method compared to the LBL method (P <.001) (Table 1).
Attitude
The attitude scores of students toward the instructional methods were high in both groups; however, the CBL group (42.78 ± 8.01) scored significantly higher than the LBL group (34.73 ± 5.64) (P <.001) (Table 1).
In the CBL group, the attitude scores for several items on the attitude questionnaire, including “This method is valuable for better learning concepts,” “This method leads to a better understanding of the issue,” “This method is useful for upgrading skills,” “This method created effective communication with other students,” “This method enhanced the relationship between students and the teacher,” and “This method is a way to enjoy learning anatomy,” were over 50%. In comparison, the attitude scores for the LBL method were <30% (Table 3).
Comparison of attitude levels after case-based learning (CBL) and lecture-based learning (LBL) methods.

Discussion
This study examined the effectiveness of CBL and LBL teaching methods in a lower limb anatomy course on medical students’ satisfaction, attitudes, knowledge, and skills. In general, students had positive perceptions of CBL. As a result, CBL has the potential to enhance critical thinking abilities, student performance, and learning efficiency in medical education. Regarding the role of general practitioners in the health system of Iranian society, the Ministry of Health and Medical Education of Iran has published a document outlining the minimum capabilities necessary for the influential role of general practitioners in the health system. 7 According to this document, medical education could benefit from CBL in several ways. Studies have indicated that students who complete more cases typically receive higher grades for each case. Additionally, CBL is highly beneficial in creating more productive interactions between educators and learners and advancing students’ capacity for independent study, theory application, and self-learning.8,9
The traditional lecture- and teacher-centered teaching method is still among the most common instructional methods in medical schools in many countries. 8 However, this instructional method does not provide an active and problem-solving learning experience to improve undergraduate medical students’ clinical knowledge and skills. The key to effective teaching is inclusive, active participation in learning. 10 CBL is fundamentally rooted in cooperative learning to prepare students for clinical practice using real clinical cases; however, there is no international agreement on the definition of the CBL instructional method. 11 In this pedagogical approach, teachers play an essential role and are no longer merely transmitters of knowledge. In other words, teachers facilitate students’ deep learning by emphasizing high cognitive abilities and effective learning strategies, guiding them toward an active presence in education with high engagement and satisfaction. 12
CBL can help shape the curriculum by exposing students to real-world circumstances they might encounter in their future employment as healthcare professionals. By examining and resolving these cases, students can acquire critical thinking, problem-solving, and decision-making abilities that are crucial for their professional development.13,14
The results of the present study showed that the CBL method increased satisfaction, created a positive attitude, and improved undergraduate medical students’ knowledge and skill levels in the lower-extremity anatomy course.
Sangam et al 15 conducted an interventional cross-over study that demonstrated that the CBL instructional method increased the average difference in scores between presession and postsession tests, as well as the average difference in scores between the postsession tests and retention tests in the CBL group compared to the LBL group. However, unlike our study, the 2 instructional methods, CBL and LBL, were examined in only a few lessons during a course.
Vedi and Dulloo 16 conducted a nonrandomized interventional study that assessed undergraduate medical students from 2 consecutive batches and concluded that, compared to the traditional method, students in the CBL group obtained higher scores and had a more positive attitude toward the teaching approach. However, unlike their study, we implemented both instructional methods face-to-face. 16
Blewett and Kisamore in their prospective cohort study, demonstrated that using the CBL instructional method in teaching microbiology increased students’ performance on case-based exam questions. Additionally, students found this helpful method for preparing for exam questions and reviewing the course material. 17
In contrast to our findings, Chao et al observed no significant difference in medical students’ knowledge in Geriatrics and Home Medical Care clerkship courses between traditional instructional methods and the CBL method. This lack of difference may be due to implementing the CBL method on a virtual platform. This educational method requires interaction between the teacher and the student to advance the educational cases, and such interaction cannot be effectively established in virtual environments.18,19
Understanding the benefits of CBL can integrate it into the existing anatomy curriculum. Additionally, it is recommended that the CBL instructional method be promoted in various fields and stages of the basic sciences of medical education, enabling students to acquire the necessary skills to succeed in the clinical course.
Limitations and strengths
This study was conducted in a single institute and during a specific course. Students’ enthusiasm for the new teaching-learning method may have increased the scores favoring the CBL method; therefore, its impact on long-term behavior change should be assessed. Additionally, the CBL group may have been more positive in their ratings, knowing they enjoyed implementing a new learning format. While the CBL and LBL students were in distinct dormitories, this alone may not have eliminated the risk of contamination bias. Future studies should consider implementing more comprehensive monitoring and restriction protocols to isolate the treatment conditions to the greatest extent possible. However, some strengths of this study include the large sample size, the existence of a control group, and the implementation and evaluation of a new educational method over 2 consecutive years.
Conclusions
The present study led to the development, implementation, and evaluation of a CBL instructional method for medical students at the University of Medical Sciences in Iran for the first time. The CBL instructional method improved medical students’ satisfaction, attitudes, knowledge, and skills of lower-extremity anatomy; thus, it is more effective than the LBL method.
Supplemental Material
sj-docx-1-mde-10.1177_23821205251317942 - Supplemental material for Design, Implementation, and Evaluation of Case-Based Learning Aimed at Improving Undergraduate Medical Students’ Satisfaction, Attitude, Knowledge, and Skills in the Anatomy Course: An Interventional Study
Supplemental material, sj-docx-1-mde-10.1177_23821205251317942 for Design, Implementation, and Evaluation of Case-Based Learning Aimed at Improving Undergraduate Medical Students’ Satisfaction, Attitude, Knowledge, and Skills in the Anatomy Course: An Interventional Study by Amir Mohammad Salehi, Mahdi Ramezani, Elham Khanlarzadeh, Mahnaz Khatiban, Mohammad Ahmadian and Zohreh Alizadeh in Journal of Medical Education and Curricular Development
Footnotes
Author contributions
MR was involved in the study's conception and design, and the intervention was performed. EK and ZA analyzed the data. MK made significant contributions to the writing of the manuscript. AS made significant contributions to the writing of the manuscript. MA and AS contributed to refining the clarity, coherence, and overall quality of the manuscript through detailed editing and revisions. All authors participated in participant assessments and data acquisition, were involved in revising and approving the manuscript, and read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declare that they have no conflicts of interest regarding the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially supported by the Hamadan University of Medical Sciences (9904312720).
Availability of data and materials
The datasets used and/or analyzed during the current study are available at the request of the corresponding author (Mahdi Ramezani: m.ramezani@umsha.ac.ir).
Ethics approval and consent to participate
The Ethics Committee of Hamadan University of Medical Sciences approved the protocol of this study (IR.UMSHA.REC.1399.423). The research was conducted by the Declaration of Helsinki, and informed consent was obtained from all participants.
Consent for publication
Each participant gave informed consent before enrollment.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.