
Abstract
OBJECTIVES
Driven by innovations in healthcare, observation medicine (OM) is expanding as a medical specialty. Despite exponential growth, education on OM remains underemphasized in the internal medicine (IM) residency programs. We assessed the impact of an educational intervention pairing didactic and experiential learning with an interdepartmental approach on IM residents’ confidence, knowledge, and attitudes when providing observation care to patients with neuro-cardiovascular diseases in the hospital setting.
METHODS
Our multifaceted intervention incorporated OM’s principles and practice in a flipped classroom with the team-, case-, lecture- and evidence-based learning model. Kirkpatrick’s evaluation model was used to assess the educational intervention’s effectiveness according to the first three levels, ie, reaction, learning, and behavior, using quantitative surveys. The surveys were completed pre-intervention, and immediately upon completion of the educational intervention.
RESULTS
Of 55 eligible residents, 55 (100%) participated in this intervention. Fifty (90%) completed the pre-intervention survey, and 21 (38%) completed the immediate post-intervention survey. Kirkpatrick’s evaluation framework showed that the intervention had a positive impact on residents’ motivational reaction (attention, relevance, confidence, and satisfaction [ARCS], M = 3.8, SD = 0.87), their knowledge of common observation diagnoses (pre = 49%, post = 63%), particularly on cardiac diagnostic workup and approach to patients with transient neurological symptoms (P < .05), and their behavior and self-assessment of core competency domains (pre-mean = 2.69, post-mean = 3.18, P < .001).
CONCLUSIONS
Our multimodal intervention provides a framework for a structured OM educational experience that can be incorporated into residency training, even without a formal observation unit rotation. The analysis also offers literary data on the current state of OM education in an IM residency program and supports the need to expand OM's educational resources to counteract the growth in hospital observation services. Future research should include an analysis of residents’ knowledge and skills from a longitudinal OM experience and advancing the results to residency programs where observation care is as applicable as ours.
Keywords
Introduction
The art of observing patients is an ancient and critical one. Hippocrates, the father of medicine, emphasized the value of physicians’ observation skills by stating, “Leave nothing to chance, overlook nothing: combine contradictory observations and allow enough time. A great part, I believe, of the art is to be able to observe.” 1 His writings on medical practice observations, assembled in the Hippocratic corpus, laid the foundation of modern medicine. More than two millennia later, observation care remains an essential element of the philosophy of doctoring and patient care. The Centers for Medicare and Medicaid Services defines observation care as “a specific, well-defined set of clinically appropriate services, which include ongoing assessment, reassessment, and short-term treatment; before a decision regarding further inpatient hospital management or discharge can be finalized.” 2 Observation medicine (OM), therefore, encompasses the knowledge and skill needed to observe selected patients and actively manage them beyond the emergency department (ED), typically up to 24 hours.3,4
The emergence of OM as a medical specialty parallels the growth of emergency medicine (EM).5,6 The American College of Emergency Physicians, in its policy statement, reported that “observation of appropriate ED patients in a dedicated ED observation area, instead of a general inpatient bed or an acute care ED bed, is a ‘best practice’ that requires commitment of staff and hospital resources.” 7 Observation units (OUs) increase patient satisfaction and safety, provide high-quality and efficient patient care, and improve financial performance for both EDs and the hospitals in which they operate. 8 Given such, the percentage of hospitals in the United States with an OU has increased from 19% in a 2003 national survey 9 to 44.6% per the 2016 National Hospital Ambulatory Medical Care Survey Data. 10 Simultaneously, the usage of hospital observation services has grown drastically in the last decade, affecting the number and percentage of patients admitted with observation status. 11 The accelerating use of observation services appears to be increasing across the age spectrum, and the magnitude of these changes raises concern that observation is becoming a surrogate for inpatient admission. 12 This paradigm shift is likely a result of evolving healthcare systems, emerging payer policies, and hospitals’ continuous efforts to improve patient flow in the ED, reduce inpatient admissions, and avoid readmission penalties. 13
Given the current expansion of observation services and proliferation of OUs, it is becoming crucial for resident physicians to get exposed to the OM principles and practice, including observation-specific medical decision-making, risk stratification, disposition decision-making, cost-effective care, utilization management, and clinical quality metrics, for a well-rounded residency experience. However, despite recognizing the importance of OM education and training for healthcare providers, there is a significant gap between the need and the current state of OM training in residency programs. A 2002 national survey found OM underrepresentation in EM residency programs, with only 9.8% of programs requiring their residents to have a mandatory OM experience during training; of those without an OM requirement, only a quarter of programs offered an observation elective. 14 The study also found that merely 11.3% of faculty had OM experience as residents, verifying residents and faculty development opportunities. 14 The advent of hospital medicine has expanded the clinical horizon and created opportunities for internists and hospitalists to provide clinical care to patients requiring hospital observation care. 15 The Society of Hospital Medicine (SHM) estimated that in 2012, hospitalists provided observation care to 59% of Medicare patients. In the SHM white paper, the lack of training and clarity around the observation rules was reported as one of hospitalists’ concerns regarding OM. 16 This lack of formal education and training in OM can lead to knowledge gaps and inconsistent practice among residents and hospitalists, potentially compromising patient safety and quality of care. Internal medicine (IM) residents are essential members of the hospital medicine workforce, yet less is known about the state of OM education in the IM residency programs; one can only assume that it is similar to the EM residency programs. Additionally, despite an undeniable need to expand OM's educational resources and experience to counterbalance the increase in hospital observation services, OM education is lagging in the curricula for residents and faculty development. While observation care grows and unfolds, it becomes critical for IM residents to acquire OM knowledge and experience during residency training.
The IM residents at our institution have a geographic and inpatient unit-based rounding structure, limiting their care delivery to observation patients on the floors and in the hospitalist-run observation unit. A 2-week observation unit rotation is available to the postgraduate year (PGY)-1 IM residents; however, the effectiveness of this rotation has yet to be studied. To further expand the OM's educational resources within the IM residency program, we implemented a multifaceted educational intervention pairing didactic and experiential learning to expose our residents to OM principles and practice, including observation-specific medical decision-making for patients presenting with low-intermediate risk chest pain and transient neurological symptoms in a multidisciplinary and interdepartmental setting. In addition, a quasi-experimental study evaluated the educational intervention's impact on residents’ confidence, knowledge, and attitudes toward hospital observation care. Specifically, the study sought to answer the following research question: What is the relationship between the OM-specific educational intervention and IM residents’ confidence, knowledge, and attitudes when providing observation care to patients with neuro-cardiovascular diseases in the hospital setting?
The proposed research aims to address a critical gap in knowledge, contribute to the current state of OM education, address the need for OM training in residency programs, and provide the framework for a structured OM educational experience that can be incorporated into IM resident education and didactics, even without a formal OU rotation. This can ultimately contribute to enhancing the quality of care delivered to patients in the observation setting and inform best practices for resident training.
Methods
Study design, setting, and participants
We conducted a quasi-experimental study of a single group with a pretest–posttest measurement of the educational intervention within the IM residency training program at the University of Massachusetts Medical School—Baystate Medical Center in August 2021. Convenience sampling was used among IM and Medicine-Pediatric (MP) residents on the medicine service (n = 55) for the eligible participants. Residents at all training levels eligible to attend the weekly academic half-day (AHD) were required to participate in this educational intervention and study. All residents off-site, off-service, on night shifts, on vacations, and off from work didn’t receive the intervention and were excluded from the study. Therefore, sample size calculation and power analysis were not conducted. Our Institutional Review Board (IRB) deemed this project and “proposed activity does not constitute human subject research as defined by federal regulations. As such, an IRB review is not required” (IRB reference # BH-21-053). Pre- and post-intervention, residents were contacted electronically to consent for participation in web-based online surveys; completion of surveys was presumed as implied consent of participation, participation in the surveys was optional and voluntary, and aggregate responses were collected anonymously and remained confidential (Supplemental File: Participant recruitment email).
Educational intervention
We designed a multifaceted intervention integrating principles of observation care in flipped classrooms with team-, case-, lecture- and evidence-based learning (FC-TCLEBL) 17 to blend residents’ asynchronous, self-paced learning with synchronous instruction. This model attempted to address the needs of diverse groups of residents with heterogeneous learning goals and varied clinical experiences by creating an active, engaging, and stimulating learning environment. Content selection for the asynchronous self-study material, synchronous didactic sessions, and team-case-based learning sessions in this educational intervention was based on the recommendations from the observation unit faculty and focused on the common observation diagnoses cared for at our institution. The breakdowns of the didactic content with various elements are highlighted below (Table 1).
Didactic content of the observation medicine educational intervention.

Asynchronous pre-class flipped classroom
The self-study material in the intervention consisted of pre-class reading articles and two concept videos. One of the authors (RS) created the videos18,19 on the lumen5 platform, 25 5 minutes each, elaborating the basic principles of OM, including introduction to hospital observation services, appropriate observation patient selection, utilization management, and clinical quality metrics. The pre-reading articles included clinical practice guidelines and reading materials on low-risk chest pain, cardiac stress testing, syncope, and transient ischemic attack.20–24 The high-yield content within the pre-reading articles was assigned to the residents based on their PGY level of training but was open to discussion with others when working on case studies (Supplemental File: Appendix A). The workshop's outline and learning objectives were shared with the residents beforehand, and the self-study material was uploaded on the IM residency OneDrive account one week before the in-class sessions. Residents were expected to review the pre-class material beforehand to process and reflect on new concepts and increase their knowledge base before the classroom sessions.
Synchronous classroom instruction
Synchronous learning was conducted as a workshop during residents’ AHD and utilized the team-, case-, lecture- and evidence-based learning multimodal approach. The workshop was 4-hour long and was split into four 1-hour long workshop sessions and case studies, as elaborated below (Supplemental Files: Appendices B–E).
Session 1: observation medicine 101—introduction to hospital observation services
This educational session provided an introduction to the fundamental concepts of OM and observation care. This session was facilitated by the observation unit faculty and delivered as a didactic presentation with the aid of PowerPoint.
Session 2: utilization management—right level of care
This educational session provided an introduction to utilization management (UM), elaborating on its role as an evidence-based, clinical support group for physicians. The UM champion in the hospital medicine department delivered this session as a didactic presentation with the aid of PowerPoint.
Sessions 3 and 4: team-case-based learning—approach to patients with chest pain and transient neurological symptoms
During the second half of the workshop, residents collaboratively worked on four case studies in eight small groups. Each case started with a clinical vignette prompting a series of follow-up questions regarding the case study. These sessions were facilitated by the resident team leaders of the small groups, chief medical residents, and subspecialists from the departments of cardiology and neurology. The facilitators also received the facilitator guide with answers to the questions before the start of sessions. These sessions allowed residents to apply theory to practice by applying knowledge to the cases, using critical thinking, team-building skills, and inquiry-based learning methods.
Outcomes
Kirkpatrick’s evaluation model was applied to objectively measure the effectiveness of the educational intervention in a hierarchical process incorporating three levels, ie, reaction, learning, and behavior. 26 Given the novel nature of this multifaceted intervention, Kirkpatrick’s model was preferred because of the process simplicity, manageable evaluation criteria, and lack of necessity to collect learners’ previous performance; most importantly, to gain an understanding of this educational initiative’s efficacy and strategies to improve specific components in the future.
Kirkpatrick's evaluation model
Level I—assessment of motivational reaction
John Keller’s Instructional Materials Motivation Survey (IMMS) was used as a framework to assess level 1 of the framework and residents’ motivational reaction to the program, by measuring the four constructs of attention, relevance, confidence, and satisfaction. 27 The questions pertaining to the reaction portion of Kirkpatrick's model were adapted from a validated 12-item Reduced Instructional Materials Motivation Survey (RIMMS) with a 5-point Likert scale (1 = not true; through 5 = very true) questionnaire 28 and were administered immediately after completion of the workshop (Supplemental File: Appendix F).
Level II—assessment of learning
The learning portion was assessed using a 10-item multiple-choice questionnaire (adapted with permission from NEJM knowledge +), 29 incorporating common OM diagnosis, ie, risk stratification of chest pain, cardiac stress testing, diagnostic workup of palpitations, syncope, and transient neurological symptoms. The questionnaire was administered before and after the completion of the educational intervention (Supplemental File: Appendix G).
Level III—assessment of behavior
Lastly, behavior was evaluated using a self-assessment proficiency survey incorporating the six core competencies outlined by the Accreditation Council for Graduate Medical Education (ACGME), including patient care, medical knowledge, interpersonal and communication skills, professionalism, practice-based learning and improvement, and system-based practice, with specific sub-competencies and milestones relevant to the practice of OM. 30 The instrument is a 17-item questionnaire with a five-point Likert scale ranging from proficiency levels: (1) fundamental awareness (basic knowledge), (2) novice (limited experience), (3) intermediate (practical application), (4) advanced (applied theory), and (5) expert (recognized authority). 31 A panel of writing experts established the questionnaire's content validity, and internal consistency was calculated by Cronbach's Alpha. The value for Cronbach's Alpha for the survey was α = 0.94. The survey was administered before and after completing the educational intervention (Supplemental File: Appendix H).
Statistical analysis
The surveys were disseminated online using Qualtrics survey software (Qualtrics, Provo, UT, USA). 32 Statistical analysis was performed using IBM Statistical Package for the Social Sciences Statistics for Windows, Version 29.0.0.0 (241). 33 Data were analyzed using descriptive and inferential statistics (paired t-test and Fischer's exact tests). The significance was assessed at a 5% level of significance (P < .05) with a 95% confidence interval.
Results
An anonymized survey was administered to assess residents’ learning and behavior pre-intervention, and reaction, learning, and behavior post-implementation of the educational intervention. The Qualtrics survey was split into three categories that helped guide the study's objectives using Kirkpatrick’s Evaluation Model. The surveys were distributed to 55 residents, and 50 responses (90%) were received pre-intervention and 21 responses (38%) were received post-intervention (Supplemental Files: Appendices F, G, and H)
Assessment of motivational reaction
Kirkpatrick's evaluation of motivational reaction, based on the 12-item RIMMS scale, included specific questions regarding the educational intervention, both related to the pre-class asynchronous flipped classroom and synchronous classroom instruction. The participants’ overall thoughts on the instructional components of attention, relevance, confidence, and satisfaction were positive (M = 3.8) (Table 2). Regarding specific aspects of the educational intervention, the usefulness of the content was the highest-ranking aspect (M = 4.14), followed by the organization and style of the content (M = 4.13). The lowest-ranking aspect was the ability to maintain attention (M = 3.50).
Kirkpatrick's level I—assessment of motivational reaction.

Assessment of learning
Pre-intervention, the baseline average scores were lowest in the question categories related to the diagnostic work-up for neurocardiogenic syncope, palpitations, and management of transient ischemic symptoms. Post-intervention, the average knowledge scores increased from pre-intervention (49%) to post-intervention (60%). However, statistical significance (P < .05) across the groups was only noted in the questions about the cardiac diagnostic workup and approach to patients with transient neurological symptoms (Figure 1).

Kirkpatrick’s level II—assessment of learning.
Assessment of behavior
The mean competency score increased from 2.69 pre-intervention to 3.18 post-intervention (P < .001). Within the specific ACGME core competencies, statistical significance was noted in the domains of medical knowledge (P = .006), practice-based learning and improvement (P = .04), and system-based practice (P = .005). In comparison, patient care (P = .06), professionalism (P = .32), and interpersonal and communication skills (P = .40) showed no significant difference across the groups (Table 3).
Kirkpatrick's level III—self-assessment of ACGME core competencies.
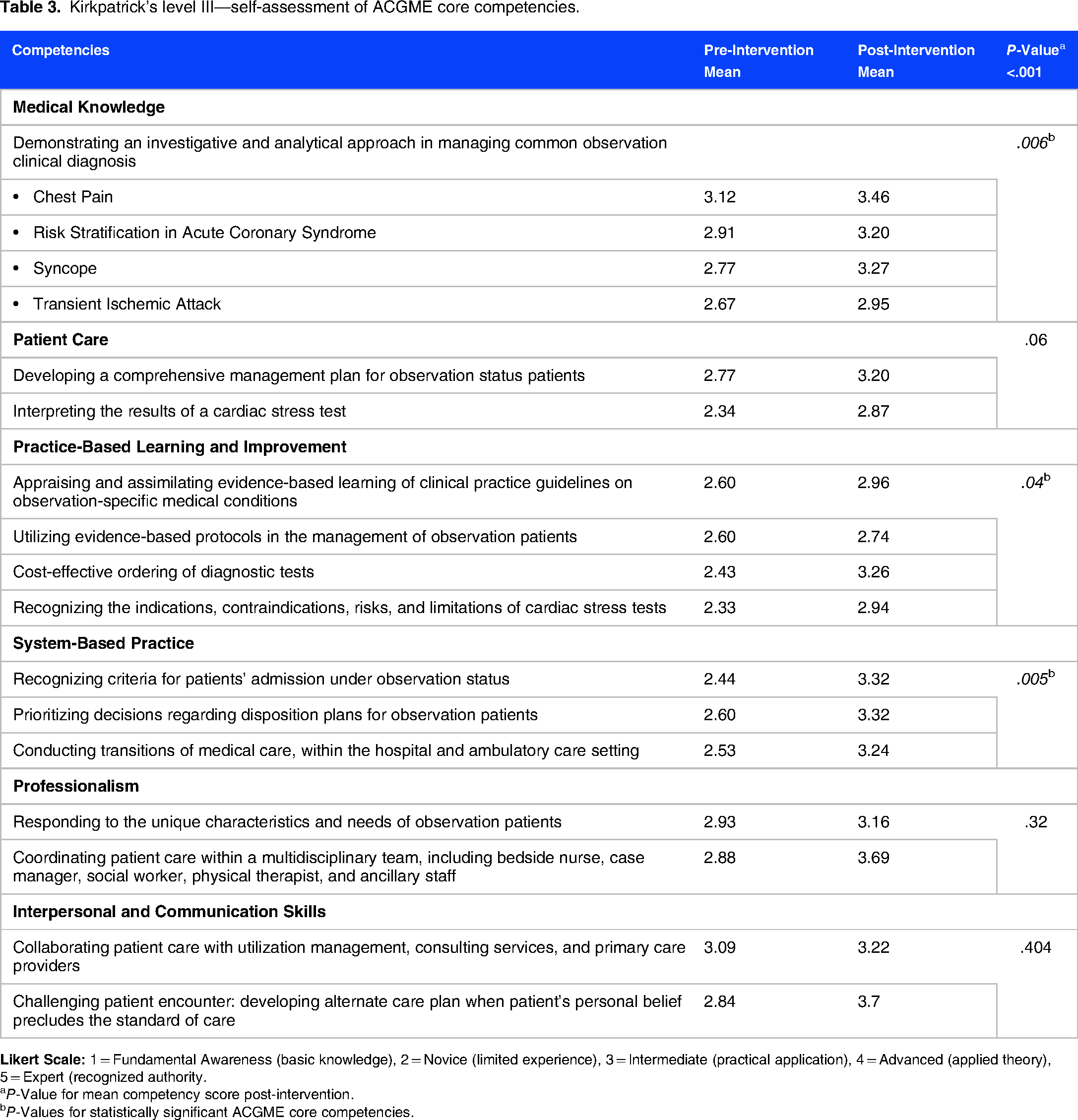
aP-Value for mean competency score post-intervention.
bP-Values for statistically significant ACGME core competencies.
Discussion
This study demonstrates that a multifaceted educational intervention model integrating flipped classrooms with team-, case-, lecture- and evidence-based learning (FC-TCLEBL) meaningfully impacts residents’ confidence, knowledge, and attitudes while providing observation care in a hospital setting to patients with neuro-cardiovascular diseases in an IM residency program. Additionally, this study reinforces the necessity for research in the arena, adds to the limited body of literature related to OM education during IM residency training, and highlights the importance of ongoing OM education and training for healthcare professionals in this emerging field of medicine. The FC-TCLEBL model extends the work by Ding et al, 17 previously demonstrated to be an effective approach in developing critical reasoning, problem-solving, and teamwork in ophthalmology teaching in an undergraduate medical education program. To our knowledge, ours is the first to utilize the multimodal FC-TCLEBL model for OM education in a graduate medical education (GME) program. Our study has thus contributed to the emerging body of evidence across GME specialties supporting the effectiveness of curricula pairing didactic and experiential learning with an interdepartmental approach.
OM is one of the rapidly growing medical sub-specialties, yet an underemphasized area within the curriculum of the residency training and IM residency programs. Therefore, when creating the educational content for this intervention, we focused on educating residents on the principles and practice of OM, including focused patient care goals, utilization management, cost-effective care, clinical quality metrics, and observation-specific medical decision-making. The main challenge foreseen with this project's implementation was integrating OM's principles and practice into the culture of residency training and clinical practice, which required residents’ buy-in, engagement, and satisfaction. Therefore, along with our focus on the learning outcomes, understanding residents’ attitudes and beliefs towards observation patients and OM education was considered imperative to add educational value to this project. Thus, we used Kirkpatrick's model of evaluation to assess the effectiveness of the educational intervention at three levels: (1) the residents’ reaction and perception to the educational experience, (2) the residents’ cognitive development, learning outcomes, and attainment of knowledge and skills after the intervention, and (3) the residents’ change in behavior and application of content learned during the intervention.
As noted in the results section, residents’ motivational reaction to the program using the attention, relevance, confidence, and satisfaction (ARCS) model27,28 was encouraging. All residents found the content valuable and relevant, felt satisfied and confident upon completion of the intervention, but had difficulty maintaining attention. Challenges with attention could be attributed to the cognitive load from the didactic and case-based sessions and could be avoided by breaking down the content into multiple, short, and focused sessions. Regarding the knowledge assessment, we achieved statistical significance on questions pertaining to cardiac diagnostic workup and approach to patients with transient neurological symptoms, which could be attributed to specific case studies on the diagnostic and therapeutic approach to patients with low-risk cardiac and neurological conditions followed by subspecialists’ input to clarify any misconceptions and facts regarding those clinical diagnoses. The baseline knowledge scores were lowest in the questions on the diagnostic workup of neurocardiogenic syncope; post-intervention, despite the positive trend, statistical significance wasn’t achieved, highlighting the need for continuing education on this topic in the classroom and patient care setting. Lastly, residents’ self-perception of ability in the six areas of ACGME core competencies was also noted to be statistically significant (P < .001). All areas of competence were reported to have a positive trend. But statistical significance was noted in the domains of medical knowledge, practice-based learning and improvement, and system-based practice (SBP). 30 Since principles of observation care align well with the competency and sub-competencies of SBP, a structured OM curriculum could enable the integration of SBP in residency training and contribute to improving the quality and safety of patient care. Exposure to a structured OM educational experience would also train residents to prioritize decisions regarding disposition plans for observation patients, deliver cost-effective and high-value care through the conscious ordering of diagnostic tests, and help acquire knowledge and skills needed to conduct effective medical care transitions within the hospital and outpatient setting.
Feasibility
Our IM residency program provides a weekly protected 4-hour educational experience for the residents, known as academic-half-day. Therefore, creating a structured educational experience during that dedicated time was logistically convenient. Without a protected educational time, programs may have challenges finding an alternative medium to dedicate time for team-based learning. However, the importance of OM education during IM residency education may justify the displacement of traditional lecture-based instruction for this multifaceted educational model. Alternatively, programs can consider breaking down the sessions into a series or creating a longitudinal educational experience. However, the creation of online videos and the implementation of four workshop sessions can be a daunting task, as it requires coordinating multiple team members with variable clinical and administrative responsibilities, ie, observation unit faculty, utilization management champions, hospital medicine faculty, cardiologist, and neurologist, for a well-rounded learning experience. In addition, finding faculty members and stakeholders invested in resident education can be challenging for a few programs, particularly those without an observation unit or dedicated faculty.
Limitations
Certain limitations of this study are worth considering. This is a single-center and a single cohort study, which could limit generalizability. Our research on the FC-TCLEBL model’s feasibility on GME is only based on results from a single group. Since we didn't recruit a control group, it is hard to conclude if the positive impact on residents’ knowledge, attitude, and behavior was related to the OM intervention or specifically to the multimodal FC-TCLEBL model. The content selection for this educational intervention focused on the common observation diagnoses managed at our institution, ie, the approach to low-intermediate risk chest pain and transient neurological symptoms, limiting the generalizability of findings to other organ systems. Further research is needed to compare the effects of traditional lecture-based instruction with the FC-TCLEBL model and expand the educational content to include observation diagnoses seen at other institutions. Additionally, we utilized the convenience sampling method by extending this intervention to all IM and MP residents eligible to attend weekly AHD and didn’t conduct sample size calculation and power analysis for this study. As a result, all residents off-site, off-service, on night shifts, on vacations, and off from work were excluded from the study; potentially leading to sampling bias. Despite achieving satisfactory results, our post-intervention survey completion rate was low. We were unable to provide a protected time for the completion of post-intervention surveys. Since participation in the surveys was optional, most residents opted out of it upon completing the educational intervention. This could be remediated by splitting the educational program into a series of brief, focused sessions to allow everyone to participate and account for the cognitive load and fatigue during the intervention and survey completion. Our questionnaires utilized closed-ended questions to keep the research quantitative and outcome-oriented and simplify data analysis. However, providing an opportunity for an unstructured, open-text format instead of defined response categories might have created room for authentic, unexpected feedback and offered more information on the process. The competency survey, created by the study's authors, was validated at our institution; but not pilot-tested along with the questionnaire for assessment of learning, and delivered directly pre- and post-intervention. Lastly, due to the limited time available for the intervention, we could not assess the intervention’s impact on the last level of evaluation in Kirkpatrick’s model, ie, evaluating results. Therefore, a longitudinal OM educational experience might be warranted to assess the intervention's long-term impact on resident physicians’ performance during clinical practice and organizational and patient care outcomes.
Conclusions
Overall, this study provides a framework for a structured OM educational experience that can be incorporated into IM resident education and didactics, even without a formal observation unit rotation. As observation services continue to expand and observation units open, it becomes critical for IM residents to acquire OM knowledge and experience during residency training. However, residents’ education in OM is lagging behind the rapid growth in observation services. Our study and analysis also offer literary data supporting the need to expand OM's educational resources and experience to counterbalance the increase in hospital observation services. Specifically, implementing a structured, multimodal educational intervention pairing didactic and experiential learning with an interdepartmental approach into a GME program was well-received by the IM residents, who perceived improvement in their knowledge and competence postintervention. Future research should include an external analysis of residents’ acquisition of knowledge and skills and formal evaluation from the faculty, comparison of FC-TCLEBL with traditional modes of instruction, expansion of educational content to include observation diagnoses seen at other institutions and advancement of the results to residency programs in our institution where OM is as applicable as ours, ie, Emergency Medicine residency program. Integration of OM education in residency programs can be a cultural change for many but a step in the progressive and right direction for all. When Hippocrates stated this in 410 BC, “A great part, I believe, of the art is to be able to observe,” little did he know that his approach to medicine is going to be a long-lasting one, cherished by many generations to come.
Supplemental Material
sj-doc-1-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-1-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-docx-2-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-3-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-3-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-4-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-4-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-5-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-5-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-6-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-6-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-7-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-7-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Supplemental Material
sj-doc-8-mde-10.1177_23821205231183220 - Supplemental material for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study
Supplemental material, sj-doc-8-mde-10.1177_23821205231183220 for Impact of an Observation Medicine Educational Intervention on Residents’ Confidence, Knowledge, and Attitudes: A Quasi-Experimental Study by Riffat Sabir, Muhammad Umar, Venkatrao Medarametla and Aseesh Sreedhrala in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
Riffat Sabir, MD, MEHP, FACP would like to thank Toni Ungaretti, PhD, other faculty, and fellows at the Master of Education in the Health Professions program at Johns Hopkins University School of Education for their guidance and support in the development of this scholarly project. The authors would also like to thank Reham Shabaan, DO, MS, FHM, for providing us with this protected educational time during residents’ academic half-day.
Author Contributions
All authors contributed to study design, questionnaire development and administration, data collection and analysis and in writing and revision of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was reviewed by the Baystate Health Institutional Review Board (IRB), Springfield, MA. The proposed activity was deemed not to constitute human subjects research as defined by federal regulations. As such, an IRB review was not required (IRB reference # BH-21-053).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent was obtained electronically prior to participation, and completion of surveys was presumed as consent of participation. Aggregate responses were collected anonymously and remained confidential.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.