
Abstract
This meta-analysis aimed to evaluate the effectiveness of team-based learning in radiology education. Data sources and selection criteria Databases were searched from inception up to August 2019 and included Pubmed, Medline, Embase, China National Knowledge Infrastructure (CNKI), Chinese Wanfang Database, and Chinese VIP. Randomized trials comparing teaching approaches for medical imaging of which provide the outcomes of theoretical scores and/or practical scores were included. Data were extracted independently by two authors and double-checked for accuracy. Outcomes included knowledge scores and practical scores. We pooled data using random-effects meta-analysis. Twelve trials involving 1,371 participants were included. Team-based learning teaching method had positive impacts on theoretical scores compared with the lecture-based learning or traditional teaching method (SMD = 1.07, 95% CI [0.50, 1.63]) and it positively improved skill scores (SMD = 0.68, 95% CI [0.19, 1.17]). Team-based learning could not only improve theoretical and skill scores in medical imaging courses but also encourage students to learn by themselves. Participants believed team-based learning raised their learning interest, team cooperation ability, and interpersonal communication skills. The heterogeneity of the included studies must be noticed and large well-designed and well-conducted trials are urgently needed.
Keywords
Background
The traditional teaching method, known as lecture-based learning, is a teacher-centered and lecture-based pedagogical approach. Medical students have been accustomed to traditional lecture courses, during which all they need to do is listening to the instructor, viewing PowerPoint presentations, and handouts, as well as taking notes. This approach cannot fulfill the educational intentions of medical imaging courses (Hashmi, 2014; Wiener et al., 2009). Therefore, new pedagogical approaches like team-based learning (TBL), problem-based learning (PBL), and case-based learning (CBL) have emerged as supplementary teaching methods.
TBL was defined as an active learning and small group instructional strategy, which provides students with opportunities to apply conceptual knowledge through a series of activities, including individual work, team work, and instant feedback (Parmelee et al., 2012). It was originally developed for small group learning in business courses (Burgess et al., 2014), which can enhance students’ learning motivation, and encourage them to apply knowledge acquired to solve problems (Wiener et al., 2009). Recently, multiple medical schools are experimenting with this new pedagogical approach (Burgess et al., 2014). This approach has drawn great attention for following reasons: permitting a large student-teacher ratio compared with PBL, raising the interest of students for certain courses, and enhancing their ability of teamwork and critical thinking (Reimschisel et al., 2017). In addition, it also provides valuable opportunities and challenges for peer teachers by organizing and directing the class, instead of mere lecturing (Zeng et al., 2017).
The original application of TBL consists of three phases. Firstly, students do preparatory reading before the TBL session by themselves. After reading, students complete an individual readiness assurance test (iRAT) in which basic facts and advanced concepts in the assignment are tested, before the same test in teams of 5 to 7 students (team readiness assurance test, tRAT) is conducted. This test is answered by immediate feedback-assessment technique cards, motivating the students to collaborate until all answers are correct. During the third phase (team application), as the most important phase of TBL, the teams also apply their knowledge to solve clinical problems. The whole process enables students to get immediate feedbacks while explaining and defending their own opinions (Kibble et al., 2016).
Medical imaging is a highly professional subject in which extensive training in identifying specific imaging signs of various diseases is required (So et al., 2017). It is of great difficulty for students to tell the difference between images over a relatively short time period. Essential practice for students to get correct diagnostic method and build scientific analysis ideas cannot be acquired through mere stressing explanations of words. Emphasizing or skipping one or more phases of TBL but do not harm the core elements of TBL (Haidet et al., 2012) is acceptable for simplifying the TBL process in order to adjust to actual teaching situations (Reimschisel et al., 2017). In a systematic review including 14 studies in health education, seven studies showed improved knowledge scores in the TBL group compared with non-TBL group (Fatmi et al., 2013). No studies reported a decrease in scores for the TBL group. Learners’ attitudes toward TBL are generally positive, stressing the significance of active learning style and interaction with their peers (Reimschisel et al., 2017).
Only a few studies focusing on the teaching effectiveness of TBL in medical imaging education are available. None published studies have compared the effectiveness of TBL and lecture-based learning in medical radiology education. This study aimed to displayed the first scoping review and meta-analysis of the effects of TBL in radiology education.
Method
Search Strategy
We systematically searched the databases, including PubMed, Medline, Embase, China National Knowledge Infrastructure (CNKI), Chinese Wanfang Database, and Chinese VIP information database and the date last searched is 15 August 2019. Following the procedure in Figure 1, we retrieved the studies from inception up to August 2019 with no language limits. The following key words and heading terms were used: “(TBL OR team-based learning) AND ((medical imaging) OR radiology or MRI OR CT OR Echo OR ultrasound).” Articles matching the criteria were retrieved for further data extraction and quality assessment. All articles were selected by manual operation.
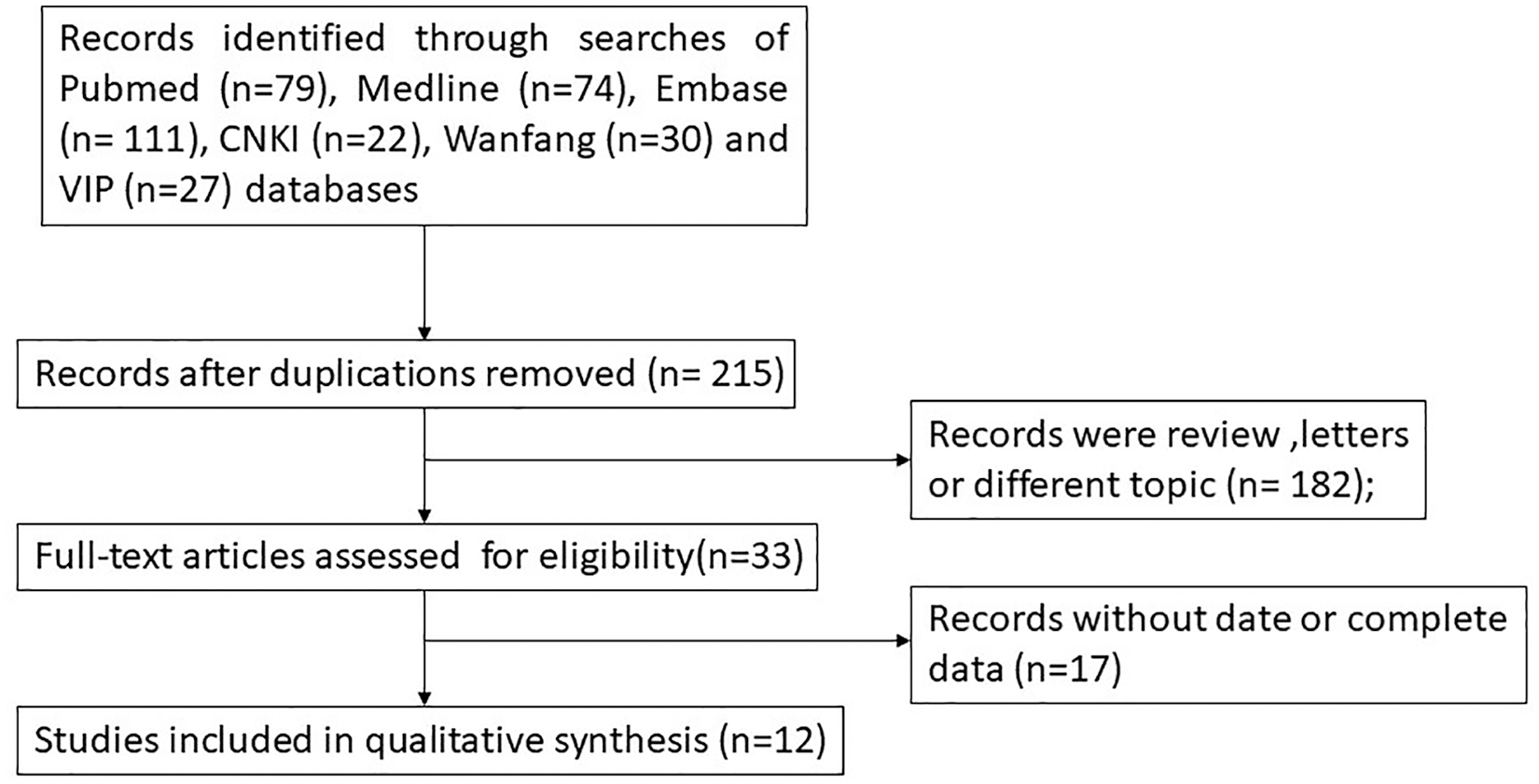
Flowchart of selection process of the included studies.
Inclusion Criteria and Exclusion Criteria
The selected studies should follow these criteria, including TBL teaching method used in the medical imaging courses and compared with the traditional or lecture-based learning teaching, as randomized controlled studies. Studies that displayed no complete examination results, reviews and letters were excluded. Inclusion criteria are as follows: Participants: medical students and trainee doctors in the Medical colleges and the teaching hospitals; Intervention: using TBL (team-based learning) in medical imaging related medical course teaching; Comparator: using traditional teaching or lecture-based learning or CBL (case-based learning); Outcomes: theoretical scores and skill scores of medical imaging course; Study design: randomized controlled studies.
Data Extraction Method and Quality Assessment
Screening was completed by three reviewers independently under the same inclusion criteria. Data was then extracted and cross-checked. Information including author name, publication year, study type, sample size (total and control), medical imaging course’s name and type, participant characteristics, intervention, comparator, and scores was extracted. Quality assessments of the selected studies were evaluated with the risk of bias table according to the Cochrane Collaboration by Review Manager 5.3 (Cochrane Collaboration, Copenhagen, Denmark).
Statistical Analysis
The extracted data was analyzed using Review Manager version 5.3 (Cochrane Collaboration, Copenhagen, Denmark). Since the outcome measure (examination score) of efficacy was a continuous one, the standardized mean difference (SMD) with 95% confidence interval (CI) was applied to determine the efficacy of the TBL model for medical imaging course teaching. Forest plots were drawn to show the point estimations of each study. The homogeneity of this included study was based on the Q statistic and I2 statistic. In this study, I2 value of >50% or p-value of <.05 were assumed to be statistically significant. When moderate to high homogeneity was improved, a random-effects model was used to combine the SMD with 95% CI. If not, a fixed-effects model was used. Funnel plots and Begg’s tests were applied to assessed the degree of publication bias with STATA 12.0 software.
Result
Search Results
In this study, a total of 343 relevant studies were initially found, and Figure 1 is the flow chart of the article selection process. The potentially eligible studies were identified following the search strategy described above from related databases. After removing the duplications, we found 215 relevant articles at the beginning. After the title-abstract screening, 182 studies were excluded, for being reviews or letters, or on different topics. Seventeen studies were excluded because of their incomplete data. Finally, a total of 12 studies were included in this meta-analysis, all of which were published in Chinese.
Study Characteristic and Study Quality
The characteristics of the included studies are shown in Table 1. They were all published in Chinese between 2014 and 2019, and extracted from Chinese National Knowledge Infrastructure (Chinese database), Wanfang Data (Chinese database), and VIP Information (Chinese database). The effectiveness of TBL on Medical radiology teaching compared with the traditional teaching were evaluated by the theoretical scores and/or skill scores. A total of 1,371 participants (697 in test group and 692 in control group) were included. Our study comparted subjects into two grades: freshmen and sophomores in the lower grade, and elder students as well as trainee doctors in the higher grade. Five studies were carried out within the lower grade (Bai & Yang, 2019; Jia et al., 2017; Luan et al., 2014; Pan et al., 2017; Zhao et al., 2019), and seven studies were carried out within the higher grade (Gu et al., 2019; Li et al., 2017; Pan et al., 2016; Wang, 2016; Wu et al., 2014; Zhang, Qiu, et al., 2018; Zhu & Wang, 2016).
Main Characteristics Extracted From the Included Studies.

Note. TBL = team-based learning; LBL = lecture-based learning; CBL = case-based learning; Lower grade = freshmen and sophomores in the lower grade; Higher grade = elder students as well as trainee doctors; Theory = course to learn theories, Practice = course to practice with theory.
The risk of bias assessment of the 12 included studies is shown in Figure 2 including the aspects of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcomes assessment, incomplete outcome data, selective reporting, and other bias.

Summary of each methodological quality item presented as percentages across all included studies.
Effects of TBL on Theoretical Scores
The theoretical scores were evaluated via multiple-choice questions, gap fillings, and essay questions to test students’ mastery in theoretical knowledge. Improvements in theoretical scores via TBL teaching was reported in all of the 12 studies included compared with LBL, CBL and traditional teaching, involving 1,371 medical students and trainee doctors (TBL group = 679, control group = 692). As is shown in Figure 3, there is a high degree of heterogeneity across the included studies (I2 = 95%, p < .00001). We used random-effects model for this part of analysis. The result showed a significant difference in theoretical scores (SMD = 1.07, 95% CI [0.05, 1.63] in favor of TBL. To further understand the effectiveness of TBL on different participants, we divided them into two subgroups, including the higher grade subgroup (elder students and trainee doctors) (Gu et al., 2019; Li et al., 2017; Pan et al., 2016; Wang et al., 2014; Wu et al., 2014; Zhang, Qiu et al., 2018; Zhu & Wang, 2016) and the lower grade subgroup (freshmen and sophomores) (Bai & Yang, 2019; Jia et al., 2017; Luan et al., 2014; Pan et al., 2017; Wang et al., 2014; Zhao et al., 2019; Zhu et al., 2017). The statistically significant differences were detected in both of the subgroups, the higher-grade subgroup (SMD = 0.63, 95% CI [0.28, 0.97] and the lower grade subgroup (SMD = 1.74, 95% CI [0.47, 3.02]).

Forest plot for the effects of TBL on knowledge scores compared with the traditional teaching or lecture-based learning. TBL = team-based learning.
Effectiveness of TBL on Skill Scores
The skill scores were evaluated by film reading, medical record writing, and cases diagnosis to test students’ clinical skills. Effectiveness of TBL teaching compared to LBL, CBL, or traditional teaching in improving skill scores were reported in 9 of the 12 studies included, involving 1157 medical students and trainee doctors (TBL group = 579, control group = 578), As it is shown in the Figure 4, there is a high degree of heterogeneity across the included studies (I2 = 93%, p < .00001). Random-effects model was used to combine the SMD in this part of analysis. The results showed significant differences in skill scores (SMD = 0.68, 95% CI [0.19, 1.17]) in favor of TBL. To further understand the effectiveness of TBL on different participants, we divided them into two subgroups, including the higher-grade subgroup (elder students and trainee doctors) (Gu et al., 2019; Li et al., 2017; Pan et al., 2016; Wang, 2016; Wu et al., 2014) and the lower grade subgroup (freshmen and sophomores) (Bai & Yang, 2019; Jia et al., 2017; Luan et al., 2014; Pan et al., 2017). Statistically significant differences were shown in the lower grade subgroups (SMD = 0.85, 95% CI [0.05, 1.64], but no statistically significant difference was shown in the higher grade subgroup (SMD = 0.56, 95% CI [−0.21, 1.33].

Forest plot for the effects of TBL on skill scores compared with the traditional teaching or lecture-based learning. TBL = team-based learning.
Sensitivity Analysis and Publication Bias
Sensitivity analyses were performed to evaluate the stability of the results. Begg’s funnel plots of the SMD against the standard error of SMD suggested no substantial asymmetries in theoretical scores (Figure 5(a)) and skill scores analysis (Figure 5(b)). Egger’s regression test also showed no evidence of publication bias in theoretical scores (t = 0.33, p = .748) and skill scores analysis (t = 1.01, p = .344)

Funnel plot of the included studies for publication bias. (a)Evaluation of knowledge scores, divided into higher grade (elder students and trainee doctors) subgroup and lower grade (freshmen and sophomores) subgroup. (b) Evaluation of skill scores, divided into higher-grade subgroup and lower-grade subgroup.
Discussion
Recently, many new teaching methods like PBL, TBL have emerged. It is of great importance for teachers to find out which pedagogical approach should be used in different scenarios (Burgess et al., 2017; Dolmans et al., 2015). Since medical imaging teaching is divided into theoretical courses and practical courses, both of great significance for improving students’ theoretical knowledge and practical skills (Zhang, Xu et al., 2018) and there are few published articles focused on the effectiveness of TBL method in medical radiology. We designed this scoping review and meta-analysis in order to evaluate whether TBL is a better pedagogical approach compared to LBL in medical radiology courses. Considering the social constructivism and active learning of TBL, this article proposes a assumptions that TBL may have greater performance than lecture-based learning on Chinese radiology education.
This study showed that TBL was superior to LBL by improving both theoretical and skill scores. Our results have accumulated the findings of recent TBL studies in Chinese medical imaging education including CT, MRI, and ultrasonic. Participants’ theoretical and skill scores have improved in favor of TBL. In addition, theoretical scores and skill scores of lower-grade (freshmen and sophomores) (Bai & Yang, 2019; Jia et al., 2017; Luan et al., 2014; Pan et al., 2017; ) subgroup are significantly inferior compared to the higher-grade (elder students and trainee doctors) subgroup. The reason why the lower-grade students get more benefits reflected in the theoretical scores from transition in teaching approach is that they have relatively less basic knowledge of anatomy and pathology compared to senior students. It’s of little difficulty to improve their ability from beginner level to being able to pass the exam, but it takes much more time to raise their scores from 70 to 100. Besides, the elevation in theoretical scores is higher than that in skill scores. TBL encourages students to apply their knowledge to solve practical problems whereas LBL makes students rely passively on acceptance of knowledge.
There were no statistically significant differences in the higher-grade (elder students and trainee doctors) subgroup when it comes to skill scores. In this study approach, the students are required to search database, read materials, think independently and work as a team, so it is beneficial for freshmen and sophomores to enhance their theoretical capabilities. The ability of film reading, medical record writing and cases diagnosis requires experience and clinical practice in abundance, so their skill scores showed no significant improvement. There are other possible reasons for this inconsistent result. The TBL is a novelty for most of lower-grade (freshmen and sophomores) Chinese medical students, so their learning interests can be more easily and strongly inspired by the PBL teaching method which doesn’t appeal much for high-grade students.
All the studies included were from a Chinese context. As we know, medical training in China comparing with US models were significantly different. Chinese medical students were younger because they starting right after high school, while American graduates need join in the National Resident Matching Program (NRMP) (or the Match) to get a chance of 4 years’ residency program and pass all the medical licensing examination after the program (Gong, 2014). The heterogeneity of population may lead to variation in the effect of TBL. As an active learning and small group instructional strategy, TBL requires students to be more proactive. However, Chinese students tend to be more conservative under their own cultural background than western countries. Cultural factors which may influence the acceptance of TBL.
Despite many advantages of TBL described above, problems still exist in Chinese TBL radiology education. Firstly, some students find it hard to get accustomed to TBL and may doubt its efficacy (Kek et al., 2019). Secondly, the pre-class preparation of TBL is time-consuming and laborious (Remington et al., 2017) and the preparatory work may limit potential knowledge acquisition and overall impact of the TBL (Volerman & Poeppelman, 2019). Thirdly, it may be problematic to effectively organize discussions and allocate time during lectures (Wu et al., 2014). Excessive class size and limited class time cannot enable every students to voice their opinions (Luan et al., 2014). What’s more, team work may raise problems in scores and learning attitude (Carrasco et al., 2019). Although 81% of students said that they had to prepare before TBL class and believed they had to contribute to the learning of their team, only 52% believed that they were accountable for the team learning (Kazory & Zaidi, 2018). Their final results are basically the same, which will cause some students to feel unfair. However, TBL is demonstrably better than LBL despite these perceived barriers.
There are still many limitations of our study. A shortage of report on large-scale studies on the effects of LBL in radiology education around the world is an enormous drawback. The standards on scores and levels of radiology education vary significantly among different medical schools in China. Some schools may focus mainly on final examination while others lay more emphasis on the learning process. Standardized questionnaires need to be developed to quantitatively evaluate the motivation of students including the students’ learning interests, clinical thinking and communication abilities, serving as feedbacks to teachers. The experimental and control groups were always divided basing on classes rather than individual students, so it is difficult for investigators and participants to implement double blinding method. As a result, the selection bias and performance bias were unavoidable. Lastly, this study not characterize the fidelity of TBL implementation in the included studies.
Conclusion
The result shows that TBL teaching method is superior to traditional LBL teaching method in improving theoretical scores and skill scores in medical imaging courses in most cases, but improvement in practical skills was not significant in the higher grade (elder students and trainee doctors) subgroup. Most of the studies included provided subjective questionnaire surveys on students’ satisfaction to and effectiveness of the courses, and the results showed that participants believed TBL improved their learning interest, team cooperation abilities and interpersonal communication skills. However, the heterogeneity among the studies should be taken into consideration. With regard to the limitations described above, more standardized and better-designed researches are needed in this field.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed the ICMJE uniform disclosure form at ![]() and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
and declare: no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study did not require any ethical approval as the data used have been published previously, and they are already in the public domain.
Patient Consent
Consent is not required when conducting a systematic review.
Data Sharing Statement
Extracted data are available upon request to the corresponding author.