
Abstract
Background:
Medical undergraduates should be prepared to recognize life threating critical conditions. Undergraduate medical curriculum development to incorporate more critical care education is an essential requirement. Problem Based Learning curriculum has a potential advantage in providing more focused critical care education to medical undergraduate.
Objectives:
We aimed to evaluate the final year medical students’ knowledge and confidence in key critical care concepts in Problem Based Learning (PBL) curriculum compared to those in Traditional (Lecture) Based Learning curriculum. We also aimed to evaluate undergraduate’s level of satisfaction with the exposure to critical care education during medical education and training.
Materials and methods:
This is a cross-sectional anonymous self-administered survey questionnaire completed by two groups of final-year medical students (PBL and TBL) from three Saudi medical schools to assess the degree of undergraduate exposure to critical care and their knowledge of key critical care assessment parameters.
Results:
The responses of 279 final year medical students was analyzed (70% response rate). The majority (53%) was male and the mean age 23.9 ± 1.4 years. Only 13% of students felt confident to manage hypovolemic shock and 15% could recognize the signs of a threatened airway. One third of the students (29%) correctly identified the critical level of lactic acid in shock and less than 2% of the sample responded correctly to all the questions related to the formal assessment of critically ill patients. Lectures were the main source of information in acute care. More than two-thirds (46%) of the sample indicated that they received tuition in critical care, however the total duration spent in a critical care rotation or teaching was 1 day or less. The medical students, who completed their training with a Problem-Based Learning curriculum, had a higher knowledge base and were more confident in many critical care concepts. Only 6.5% choose critical care as their likely future career.
Conclusion:
Medical undergraduates in PBL have an overall better knowledge on key concepts and assessment tools applicable to evaluating and managing critically ill patients compared to students in TBL. However the gap in knowledge and confidence in assessing ill patients in both groups is evident. Critical care was not chosen as a preferred future career in all surveyed students. There is a need for institutional support and endorsement of undergraduate critical care exposure and education in Saudi Universities both to better prepare medical students for their imminent post-graduates exposure to ill patients and to help in closing the gap in critical care physicians through promoting the specialty.
Introduction
A medical school curriculum is ideally designed to support the development of medical students, such that they achieve sufficient knowledge as well as clinical and professional skills to assume appropriate responsibility after graduation. 1 Graduates should be adequately prepared to recognize life-threating signs at an early stage and to have the basic knowledge and concepts to manage critical conditions.2,3 A significant percentage of adverse events in hospitals are attributed to less experienced physicians. 4 In a 9-month randomized clinical trial performed at an inpatient general medical service of a large academic medical center, the medical error rate was 107.6 per 1000 patient-days in resident-led rounds. 5 Rapidly deteriorating sick patients either were not evaluated or were evaluated but not timeously due to the failure to recognize serious signs and symptoms. 6
Early exposure to critical care management principles would improve the knowledge base, confidence, and competency of junior physicians during the critical transitional period to postgraduate training. During this transitional period, newly graduated physicians are usually the first responders for the assessment and treatment of an acutely ill patient.7-14
According to literature, focused undergraduate exposure to critical care and the management of acutely ill patients is either non-existing or inadequate despite the evidence of its benefits.15,16 In a survey conducted in Irish medical schools, most student placements in critical care was 5 days or less with no procedural training. 17 Teaching intensive care was compulsory in only 31% to 56% of medical schools with 1 week of clinical exposure.15,16 None of the Saudi Medical Schools currently has mandatory Critical Care Medicine as a separate undergraduate educational block within the curriculum. A few medical schools have an elective or mandatory critical care course, usually embedded in the anesthesia block. Most of the exposure to critical care medicine occurs during medical and surgery blocks with limited insight or assessment in the quantity and quality of critical care.
In 1960 a new teaching method in undergraduate medical education was presented for the first time at McMaster University in Canada. 18 Compared to the traditional Lecture Based Learning (LBL) curriculum where students get knowledge predominantly from lectures, Problem Based Learning (PBL) curriculum utilizes a preset clinical scenarios and problems from which students work their way through to resolve. Students apprise the problem critically, generate ideas and acquire knowledge, and skills to manage the presented clinical scenarios.19-22 As compared to TBL, problem based learning has number of proposed advantages like better learning motivation and knowledge retention and increases in-depth learning.23-25 PBL however is more time consuming. 26 Studies that compare the two methods based learning however did not always demonstrate superiority of PBL on students’ knowledge.24,27-34
The current study aims to evaluate the final year medical students’ knowledge and confidence in key critical care concepts in Problem Based Learning (PBL) curriculum compared to those in Traditional (Lecture) Based Learning curriculum. We also aimed to evaluate undergraduate’s level of satisfaction with the exposure to critical care education during medical education and training.
Materials and Methods
The study is a cross-sectional survey for final year medical students at three Saudi Universities using an anonymous self-administered questionnaire. The survey was conducted during the first and second semester of the final medical year. Group A students have a traditional Lecture-Based Learning (LBL) curriculum spanning 5 years while group B students have an integrated Problem-Based Learning (PBL) curriculum spanning over same period. Both curricula incorporating academic and clinical phases.
The questionnaire consisted of 5 sections. The first section covers participant’s demographic information. The second section is dedicated on exploring time spent in education on critical care (ICU rotations, formal ICU lectures, clinical scenarios on critical care, self-learning time in ICU including e learning) while in medical school. Participants are also asked if they think they had adequate training and resources to identify critically ill patients including teaching and training on physiological track and trigger system (eg, early warning scores indicating that the patient is sick) and if they are satisfied with both time and content of the education.
The third section explore the participant knowledge on the most useful physiological observations for identifying the sick patient (Blood pressure, Temperature, Respiratory rate, Level of consciousness, SpO2 saturation, Heart rate, Urine output, Blood glucose level). All of them should be selected. In this section the participant is also asked about most common clinical signs and assessments in understanding and investigating critical illness (General appearance, Breathing patterns, Airway patency, Circulation adequacy, Pulse volume and rate, Signs of a threatened airway, Glasgow Coma Scale, Pupillary reaction, Blood glucose measurement, Abdominal girth measurement, Finger clubbing, Lower limb edema). Participant will choose to agree, be neutral or disagree that those are useful parameters to assess critically ill patients. The last 3 parameters are considered less useful as critical clinical signs. Participants are then asked about typical ICU monitoring parameters, frequency of monitoring in ICU, and patients nursing ratio.
The fourth section of the questioner assess medical student’s previous exposure and ability of to perform ICU some skills like nasal airway/suctioning, using O2 therapy devices, interpretation of ABG, techniques for establishing an airway and for mask ventilation, assessment of body perfusion, and GCS assessment. They are also asked if they are comfortable in assessing and managing a patient with hypovolemic shock or pulmonary edema.
Section 5 of the questioner address the formal assessment of critically ill patients (intubation thresholds, critical systolic blood pressure, GCS threshold for intubation, critical oxygen saturation, normal capillary refill time, the bedside management principles of hypovolemic shock, critical lactic acid levels, features of sever sepsis and essential bedside approach, tissue hypoperfusion features, critical urine output, initial ABC in management of sick patients). Multiple choices are given and participant will choose the correct answers to those standard questions.
The questioner was developed by a group of ICU consultant from 2 university hospitals who are involved in academic teaching and both undergraduate and post graduate training. The main skeleton was adopted from previous similar questioners while individual questions contents are developed by the study team. Ideal and correct responses were also established by study team. Student’s competency is the subjective comfort of the student in knowing and performing the skills.
The study objectives were explained to the participants. Agreeing to complete the questioner is considered as an informed consent to participate in this study. The study was approved by the Institutional Review Board of King Abdullah International Medical Research Center.
Statistical analysis
Standard descriptive statistics were done. Categorical variables are presented as frequency and percentage with continuous variables as mean ± standard deviation. Categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate. All tests were two-tailed and significance was accepted at a P-value <.05. Statistical testing was performed using SPSS for Windows (version 20.0; IBM, Armonk, NY, USA).
Sample size analysis calculations
To detect a difference of at least 15% in proportion of the correct answer in any of the knowledge questions between the two groups (PBL vs traditional) at 5% level of significance and to achieve a power of 80%, the required sample size was 183 from each group with a total of 366. To accommodate for a 20% non-response rate, the total number of questionnaires to be distributed was around 400.
Results
Of the 400 questionnaires distributed, 279 were completed, resulting in a response rate of 70%. There was more students in traditional lecture-based learning curriculum (57.7% vs 42.3%) and more participant from the first semester of the final year (59% vs 41%). The mean age of the combined group was 23.9 ± 1.4 years and just more than half (53%) were male (Table 1).
Demographic characteristics of the participants (N = 279).

More than two-thirds of the sample (62%) stated that they received some form of teaching in critical care. Regarding the total duration spent in critical care rotations or teaching, the majority (74%) indicated 1 day or less (Table 1). Formal lectures accounted for approximately 50% of the education and workshops 18%. When asked to evaluate the adequacy of the education to be able to identify a critically ill patient, 79% indicated not receiving adequate teaching (Table 1). A small proportion (<2%) was satisfied with their theoretical and clinical exposure and 4.3% were satisfied with the content of the education regarding critically ill patients.
In terms of routine aspects of care for critically ill patients, less than 10% knew or was exposed to the use of O2 therapy devices and airway suctioning, 13% felt competent to apply the principles of hypovolemic shock management, and 15% would recognize the signs of a threatened airway (Table 2). The sample was knowledgeable about useful physiological observations and clinical signs in critical illness such as blood pressure, level of consciousness, the Glasgow Coma Scale, and oxygen saturation (Table 3). Features like lower limb edema, finger clubbing, and abnormal abdominal girth were considered as signs of critical illness by participants (Table 4). Only 29% could identify the critical level of lactic acid in shock and 13% knew that tachypnea could be an early sign of critical illness.
Competency with basic tools frequently used in daily intensive care practice.
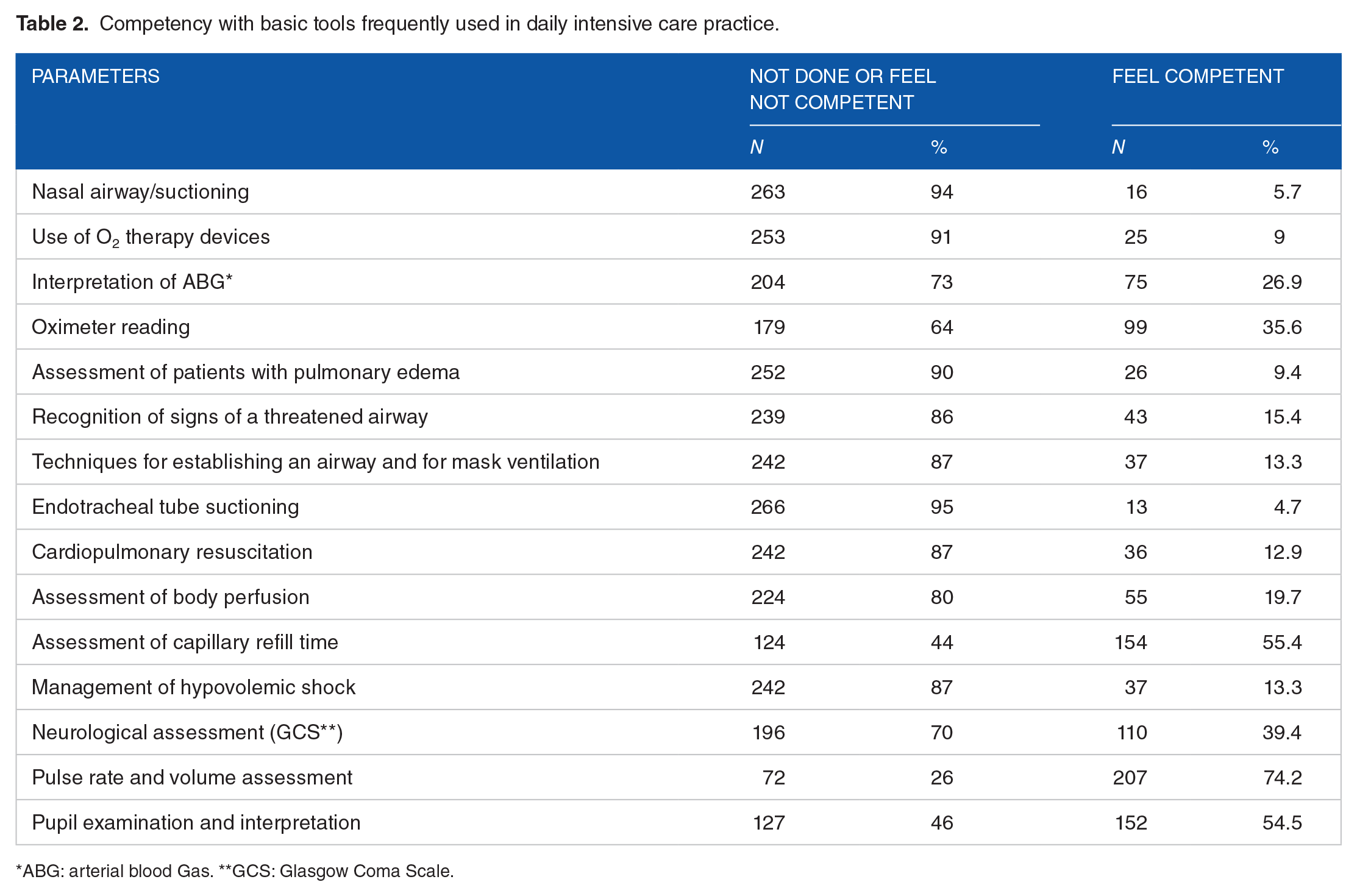
ABG: arterial blood Gas. **GCS: Glasgow Coma Scale.
Most useful physiological observations for identifying the sick patient.

Most common clinical signs and assessments in understanding and investigating critical illness.

A small proportion (1.8%) correctly responded to all 15 questions related to the formal assessment of critically ill patients. The mean score of correct responses was 6.78 (SD ±2.29) and the mean average score, out of 100, for all the questions regarding the formal assessment of critically ill patients was 45.2 (SD ±15.3).
There were significantly more participant from first semester in the BPL group while more participant in the second semester were from TBL group (P = .04). When asked if they have exposure to critical care lectures, workshops, and rotations in ICU, students in PBL group were significantly more affirmative on all (P < .001). E-learning contributes to around 4% of critical care information only in both groups. Time spent in ICU was not significantly different between the two groups. When students were asked if they think they had adequate training in identifying critically ill patients, 23% of the PBL groups versus 19% of TBL were affirmative (P .38). Medical students in TBL were more likely to choose critical care as a future career (P < .001). The overall numbers who choose critical care was so low in both groups however.
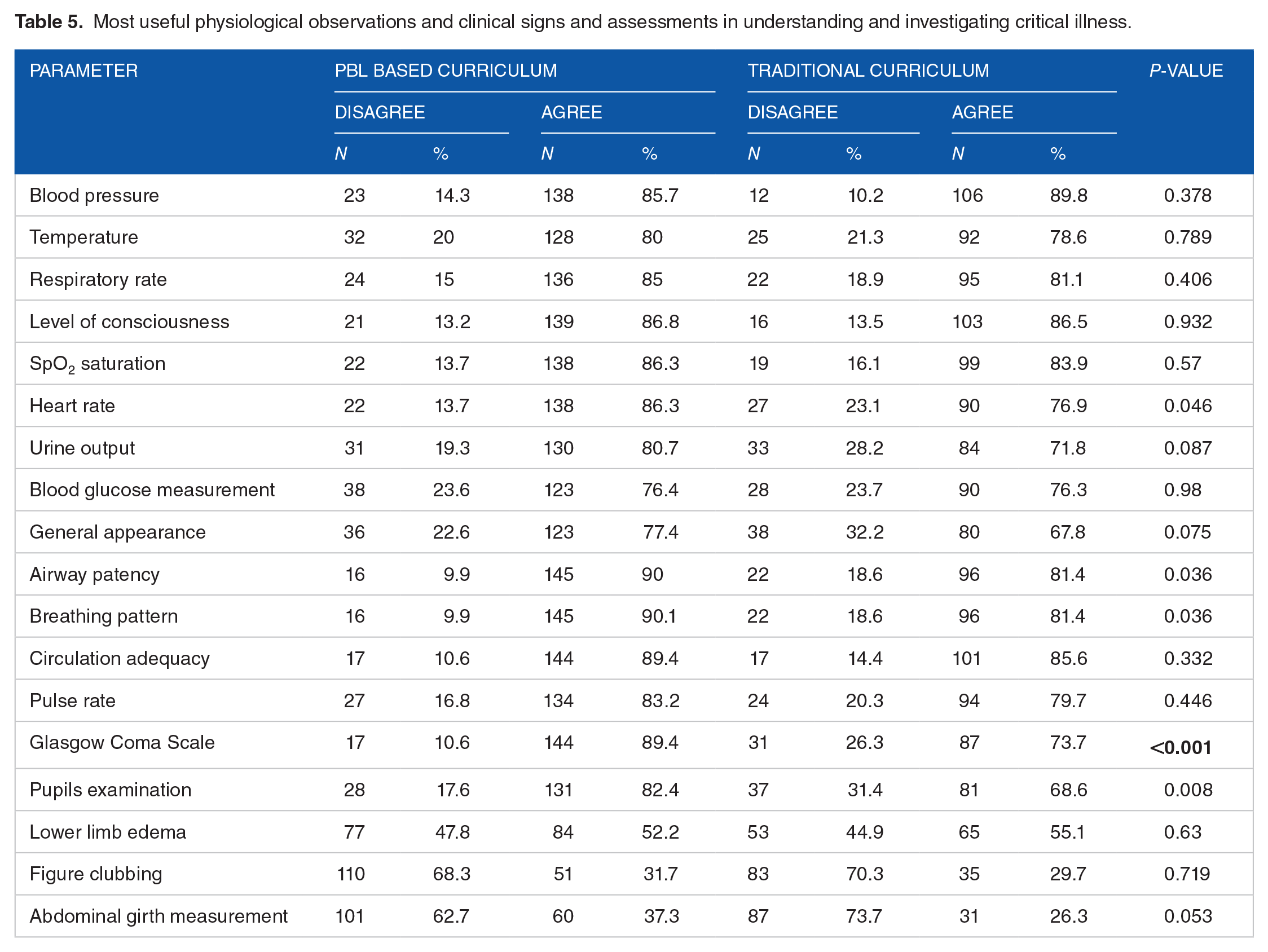
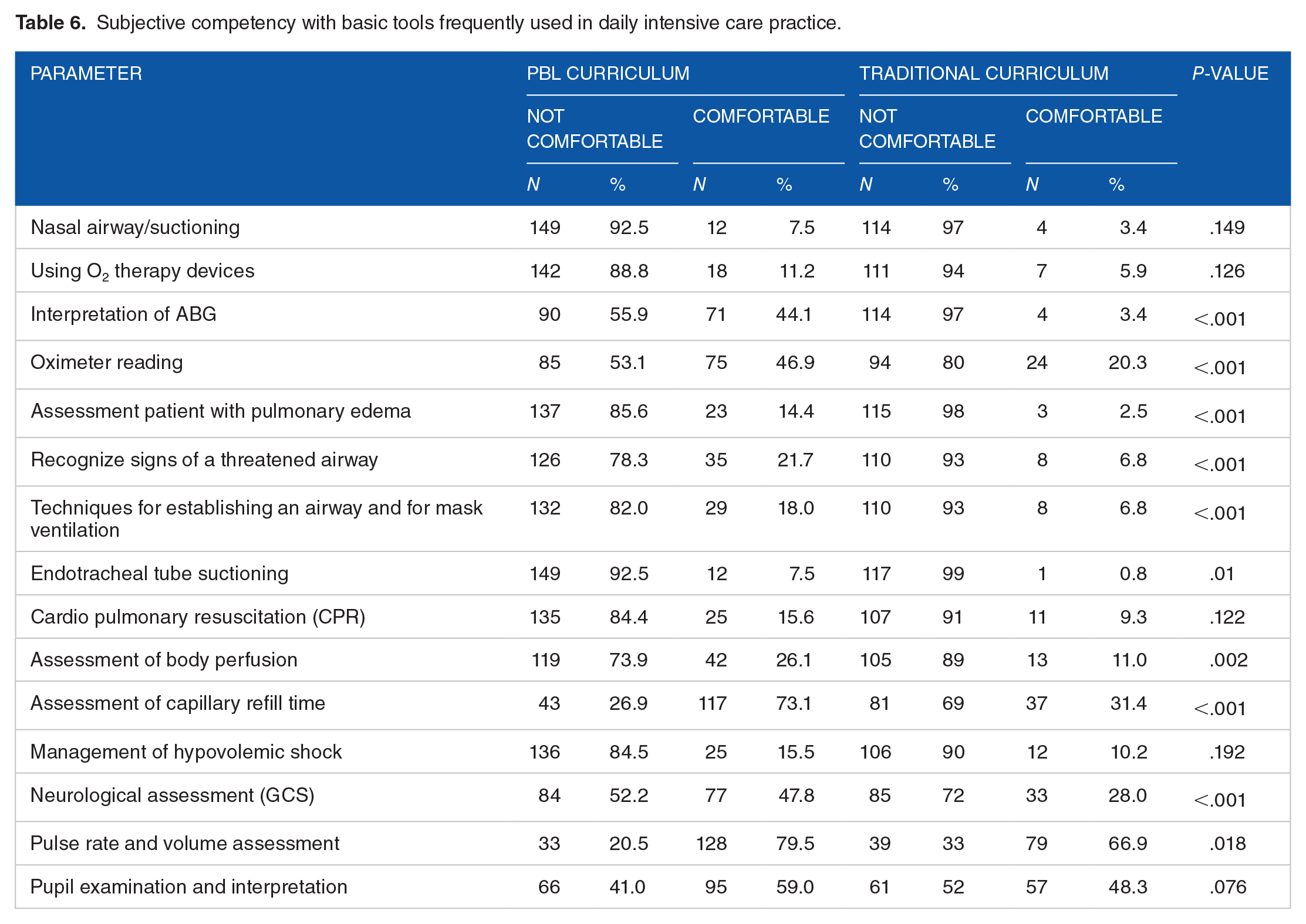
PBL Group were able to identify more high alert clinical signs and assessment tools in critically ill patients (Table 5), felt more competent with basic tools frequently used in daily intensive care practice (Table 6) and more participant responded correctly to key aspects of the assessment and management of critically ill patients (Table 7).
Most useful physiological observations and clinical signs and assessments in understanding and investigating critical illness.
Subjective competency with basic tools frequently used in daily intensive care practice.
Formal assessment questions of critically ill patients (correct answer).

The proportion of the sample who chose critical care as a career had significantly less correct responses than the group who chose other specialties (mean score: 32.6 vs 46.1; P-value <.001). Critical care was chosen by only 6.2% of the sample with 12% choosing emergency medicine (ER) and 55% other specialties. PBL group was less likely to choose critical care as a future career as compared to students in traditional curriculum (Table 4). Participants who received education in critical care were more likely to choose ER as a specialty, rather than critical care (P-value <.001). The time spent in the ICU and the duration of ICU related education and training had no impact on choosing critical care as a career.
Discussion
Medical graduates starting their residency have the responsibility as first-responders in the care of patients, including acutely ill patients. To increase patient safety, the new graduates should be equipped with the necessary knowledge and skills to detect critically ill patients early and initiate appropriate management plans. Adequate and efficient undergraduate education in managing acute illness and recognizing patients with potentially life threating conditions will translate to a better performance during this period of physicians training. 10
The current study highlights the deficiency in critical care exposure in the undergraduate education and training. Confidence in the management of basic critical care concepts such as shock management is low. Similar to other studies, the majority of the participants indicated that their exposure to critical care should be improved (only 4% were satisfied with theoretical/clinical exposure and content of critical care in our cohort).15,35-37 Though the PBL curriculum provided more exposure to critical care core principles and a higher overall confidence level, a short duration, non-horizontal approach, and absence of formal assessment were also highlighted.
The impact of undergraduate PBL curriculum on critical care has been explored predominantly in nursing schools. A significant improvement in critical thinking, evaluating and deduction of confronted problem, and overall metacognitive analytic skills in nurses with problem based learning as compared to lecture based learning.21,38-40 Some studies however could not show same positive effect despite higher overall student’s satisfaction with PBL approach in communication and motivation. 41 Effect of PBL approach in education was evaluated in a group of Medical student in public health. 42 Students in PBL has significantly better performance in exams and were gave their teacher in PBL higher scores compared to traditional based learning teachers. Similarly PBL was associated with higher learning and recalling scores in medical students taking pediatric gastroenterology courses. 43
Simulation based learning in critical care for undergraduate medical students in comparison to PBL is superior for acquisition of critical assessment and management skills. 44 In a randomized controlled comparison, medical students were educated on 2 acute medical problems, dyspnea, and abdominal pain crisis. Utilizing assessment checklist scores, students educated by SBL were able to approach the medical scenarios better than those educated with PBL.
Many critical care societies and organizations endorsed the incorporation of critical care education as a distinct block in medical school curricula.45-48 The critical care specialty is unique in providing not only clinical diversity but also in providing clear, measurable cognitive, and procedural learning outcomes. Critical care units are ideal environments for the framing of communication skills, professionalism, and systems-based practices, such as triage and bundles. 17 These skills constitute the pillars of many patient safety initiatives taught to postgraduates.
Despite the evident benefits of dedicated education in this discipline, critical care is still inconsistently taught to undergraduate medical students globally.15,16 In a survey conducted in Irish medical schools, most student placements in critical care were for less than 5 days with no procedural training. 17 In addition, a survey of intensive care education in English-speaking medical schools, intensive care education was compulsory in only 31%, and in a more recent survey of Australian and New Zealand medical schools, mandatory teaching of critical care was offered by 56% of medical schools. However, the duration of such teaching in the curricula was less than 1 week in the majority of the schools.15,16
The current model in undergraduate acute/critical care education is typically dispersed and non-core focused teaching.15,49 There is a need for an organized curriculum model that includes clear learning objectives, a mixture of bedside, classroom, and eLearning activities, procedural skills training, enriched evaluation of teaching and teaching methods, and a formal process of student assessment. 17 The majority of the current sample (78%) considered their critical care exposure inadequate. There was a low level of competency in the application of basic critical care principles, such as hypovolemic shock and threatened airway management. The overall knowledge of key elements regarding the assessment of critically ill patients was low.
The current undergraduate medical student exposures to critical care in the majority of 28 Saudi universities are limited to elective rotations. Some universities have mandatory courses during the anesthesia block with a maximum of 2 weeks. A more structured approach with a core critical care curriculum spread over the last 2 or 3 years of medical school is required. Both the horizontal and vertical structure of such a curriculum block would provide opportunities for simultaneous parallel exposure to many sub-specialties. The students would have a good opportunity to integrate their basic, clinical, theoretical, and bedside training and experience the procedural domains associated with many diseases. According to literature, undergraduate medical students have expressed interest and declared a need for more exposure to critical care medicine.37,50 In a survey of third-year medical students, 91% indicated that critical care should be a core component of the medical school curriculum. 51 Early exposure to critical care as a distinct discipline, in the form of an organized curriculum may also encourage students to choose critical care as a career and increase the current low interest in this crucial specialty.50,52 Improving the undergraduate knowledge base and competencies is imperative to patient safety. Barriers such as a full curriculum, insufficient staffing, and a lack of funding should be resolved for the sake of optimum patient safety. 53
Another potential advantage of formal undergraduate critical care teaching in medical schools is the increase in the quantity of critical care consultants in the future through promoting the specialty early in the career path. In the USA, it is estimated that the demand for critical care medicine will continue to grow rapidly, with the supply remaining near constant, causing a shortfall of specialist hours equal to 22% of the demand by 2020 and 35% by 2030. 54 In Saudi Arabia, there are only 43 critical care consultants for the 458 tertiary critical care beds in the central region with a lower ratio in other regions. 55
The current study has multiple laminations. The small sample size and the geographical limitations make generalization of the results to other medical schools very difficult. The relatively high non response rate (30%) is another limitation. We could not include more students as the year was completed. We also did not include an objective competency measure. Future inclusion of objective measures to evaluate competency in critical care skills is essential.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have critically reviewed and approved the final draft and are responsible for the content and similarity index of the manuscript.