
Abstract
Objectives
Few opportunities exist for postgraduate physicians to learn to address racism in their professional practice. We created a virtual, 5-session antiracism course that included the development of a formal action project to address racism at participants’ home institution.
Methods
We delivered this curriculum virtually to 2 cohorts (2021 and 2022) of postgraduate physicians, nationally. The curriculum had 3 educational aims: (1) to increase knowledge on antiracism, (2) to increase comfort and engagement in discussing antiracism at home institutions, and (3) to increase self-efficacy to execute an institution-based project. Theory-informed practice, community building, and project-based learning were used to achieve our educational aims. We analyzed changes in these domains in addressing racism using matched 7-item Likert-scale questions from pre- and post-course surveys and the Wilcoxon signed rank test. We assessed perceptions and impacts of the course with post-course survey items using descriptive statistics.
Results
Forty-three of 50 participants (86%) who completed pre- and post-course surveys were included in the analysis. We found pre–post course increases in mean scores (converted from Likert scales), for all 15 paired questions. For example, we found improvements in understanding the historical context of racism in medical institutions (mean score change: 5.12 [SD 1.00] to 6.42 [SD 0.76], P < .001), comfort in talking to colleagues about racism (5.21 [SD 1.08] to 6.19 [SD 0.70], P < .001), and capacity to address racism in patient care at their home institution (4.51 [SD 1.35] to 5.56 [SD 0.91], P < 0.001). 93% reported the course increased the likelihood of working to address racism at their institution.
Conclusion
This project-based antiracism course for postgraduate learners increased self-reported knowledge of, comfort with, and self-efficacy in addressing racism and was well received by participants.
Introduction
Racism is recognized as a fundamental driver of racial and ethnic inequities in health and healthcare. 1 In recognition of this, many health professional organizations have issued calls for healthcare providers to address racism in medicine.2–7 Medical education can play a key role in supporting antiracism. 8 Antiracism in medicine involves the active practice of naming and confronting racism by changing policies, practices, and norms to achieve racial justice in healthcare. 9
Previous studies have demonstrated that an antiracism curriculum can improve knowledge of, confidence in, and skills in addressing racism in medicine.10,11 While there has recently been an increase in the number of such curricula, most have been designed for students or residents.11–14 Those that have included faculty have been implemented in single academic institutions,15–19 rather than across multiple institutions, including those unaffiliated with academic training programs. Furthermore, these curricula have not included the development of a formal action project to address racism at participants’ home medical institutions or community. However, the use of a formal action project in faculty development courses draws on established adult learning principles and can both lead to greater learner engagement and the ability for learners to apply knowledge and skills from the curriculum directly to their practice. 20 In addition, project-based work can directly facilitate institutional antiracist change by supporting learners in addressing a specific problem at their institution and within their sphere of influence. 20 Finally, designing and implementing a structured project within a curriculum may encourage individuals who are exploring antiracism as a potential new focus area to continue their work after the curriculum has completed. 20
To help address this gap, we piloted a virtual, targeted, multisession antiracism course for postgraduate physicians in which participants develop individual action projects to address racism or the effects of racism on health or healthcare at their home medical institution or in their community.
Methods
Setting and course structure
We have had 2 cohorts take this course, the first February to March 2021, and the second from March to May 2022. The program was run by the Cambridge Health Alliance Center for Health Equity Education and Advocacy (CHEEA). We recruited both physicians who work at academic health centers and those who work in nonacademic community-based settings by sharing the call for applications with the CHEEA listserv and by outreach to a wide variety of health equity leaders across the country who were known to course leadership through various mechanisms. The course leadership additionally developed an inventory of health equity leaders at healthcare systems across the country, finding contact emails through institutional websites, and requested support in the dissemination of application information. We reached out to these leaders to request assistance in disseminating the call for applications for the course. The course was entirely virtual, consisting of a 3-h session every 1 to 2 weeks for a total of 5 sessions. Twenty-five physicians participated in each of the 2 course cohorts for a total of 50 participants. Sessions included a mix of interactive didactic lectures, nonfacilitated small group discussions, and facilitated project-based workshops. The content was designed for individuals who were both motivated and capable of leading racial equity initiatives. At the same time, it was designed to be flexible enough to be useful to participants with varying levels of expertise and different roles within their institutions. The resources needed to implement this program included course directors (2) and faculty (3) for program design, an administrative lead for logistical coordination (1), and an evaluation lead for survey design, implementation, and analysis (1). Existing websites, listserves, and online learning platforms from our center were utilized to execute the course.
Curriculum development
Our curricular development was informed by the Multimodal Model for Online Education developed by Picciano. 21 Picciano's model consists of 7 components: content, self-paced/independent study, social/emotional support, reflection, dialectic/questioning, collaboration, and evaluation. 21 In addition to this model, other teaching approaches also influenced course development including antiracist pedagogy, 22 engaged pedagogy, 23 and critical race theory. 24 It was also influenced by both constructivism25–27 and adult learning theory. Constructivist theory highlights the significance of the learner's interaction with the material, proposing that learning objectives are achieved through “constructing” knowledge rather than merely “acquiring” it. This approach supports using content that fosters active engagement and problem-solving over rote memorization. Effective adult education relies on several key principles: adult learners should feel that their learning has immediate practical value, address issues that impact them directly, and enhance their skills and abilities. Additionally, adult education is most successful when learners have the autonomy to control their learning process and engage in a collaborative, respectful, and informal learning environment. The curriculum framework was also influenced by the work of Kolb, focusing on interactive holistic processes grounded in experience.28,29 The curriculum was intentionally broad, with content at the beginning of the program that was foundational with progression to more advanced content and theory-based learning by the end of the course. The program was intended for learners of varying levels of expertise in this area, with a belief in the value of developing a community of practice comprising learners at different stages of expertise. We created the course content through iterative discussions among clinical faculty with expertise in teaching healthcare providers about racism in medicine, social justice, social medicine, and community organizing and through a review of literature about these concepts and how they have been taught. While this specific curriculum was not piloted prior to implementation, it grew out of pedagogy developed in prior courses taught by our center. All sessions were facilitated by the 2 course directors. These course directors, along with 3 additional faculty, facilitated small group discussions and workshops. Each of the 5 of these faculty had extensive experience and training in antiracism and health equity education.
Based on our overall goal of better preparing providers to actively reduce the effects of racism in professional practice, we defined 3 educational aims of the course: (1) to increase knowledge of racism's impacts on the practice of medicine; (2) to increase comfort with and capacity to engage in antiracism conversations at one's home institution; and (3) to increase a sense of self-efficacy to engage in strategic, project-based antiracism work at one's home institution. Each aim had underlying learning domains and underpinning theories that guided curriculum development and implementation which are detailed in (Table 1). We describe each learning domain in greater detail below.
Structure of course sessions.
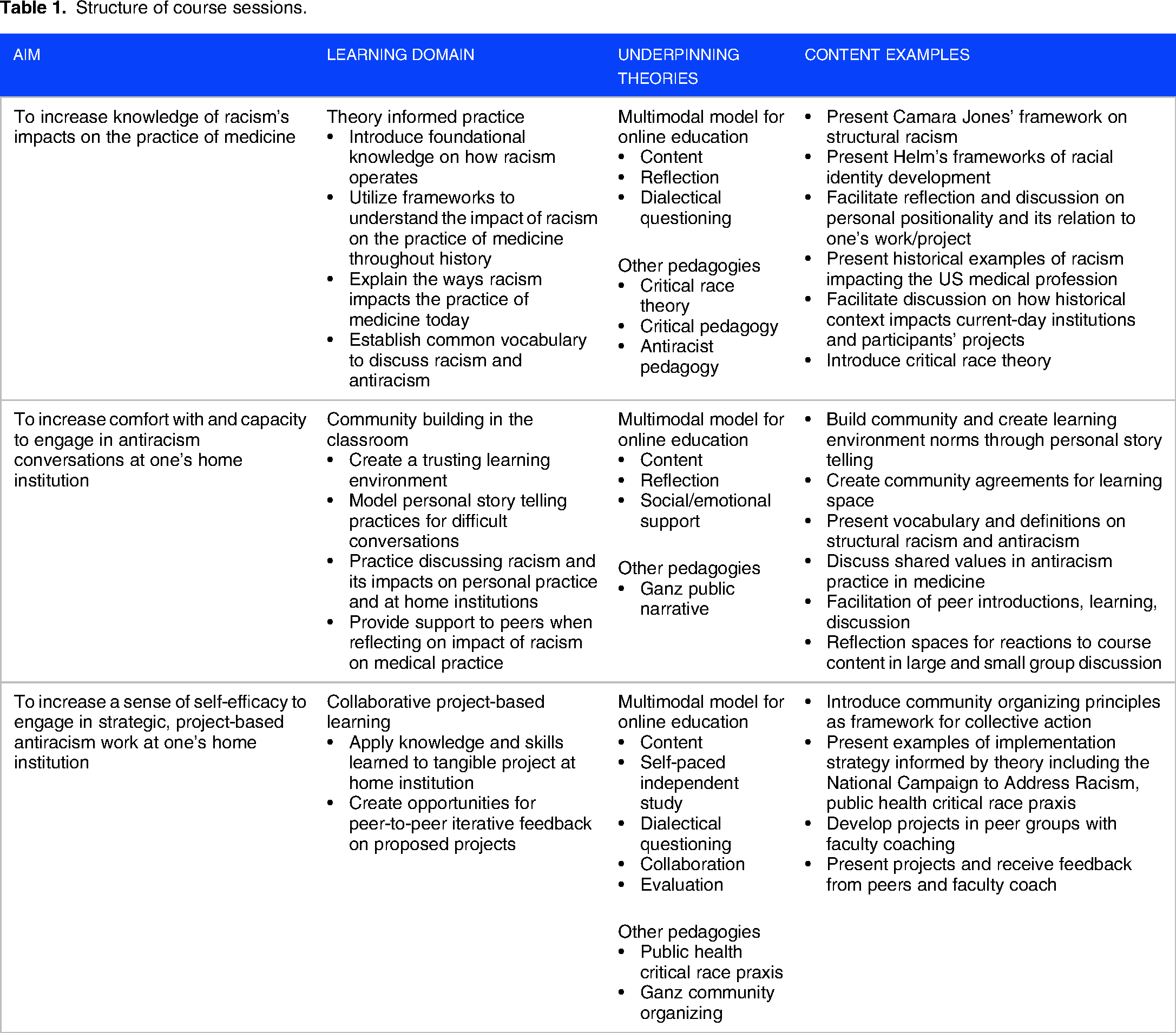
Domain 1: Theory-informed practice
Our course content challenged participants to engage in praxis—a mode of reflecting on theory to inform antiracism practice. We presented Dr Camara Jones’ frameworks on structural racism 30 and Helm's model of racial identity development. 31 We used these theories to reflect on the history of how racism has shaped medicine within the United States and how racism impacts personal racial identity development and communication around racial issues. We also discussed how theory can be applied to action within healthcare institutions by introducing several social change frameworks, including community organizing principles, 32 the National Campaign to Address Racism, 30 and Public Health Critical Race Praxis. 24 Content related to this domain was engaged with in large group didactic sessions, followed by small group breakout discussion sessions.
Domain 2: Community-building in the classroom
Community building was a critical learning domain that was employed not only to achieve a trusting, nonhierarchical, egalitarian learning environment, but also to model the conditions conducive to having productive conversations about racism. Consistent with community organizing pedagogy and with antiracism praxis, we designed group discussions to be structured to encourage participants to share their lived experiences and work experiences related to racism and to discuss how those experiences affect perceptions of the course material. We also used exercises on articulating shared values through self-reflection and storytelling throughout the course. 32 In large and small group discussions, faculty and peers offered coaching on how these conversations could be initiated with trainees and colleagues at home institutions and addressed the barriers to having these conversations. The use of community building, articulating shared values, self-reflection, and storytelling can all lead to greater comfort in engaging in antiracism conversations and thus making them more likely to occur.
Domain 3: Collaborative project-based learning
Collaborative project-based learning was used to catalyze antiracist action. This domain was critical to improving self-efficacy, a belief that course participants could achieve their goal through real-time, hands-on work. Building on the work done through Domain 1, participants developed a project that was informed by theory and would address a racial inequity or racist structure at their home institution. By focusing on a formal real-world action project, participants could directly apply the theory, knowledge, and skills learned in didactics and structured conversations. 20 Participants deepened their learning by seeing how the material could be used to solve a specific problem and where adaptations may need to be made to fit real-world challenges in their professional work environments. A motivating premise of the course is that by engaging with and making progress on a real-world problem of their choosing, with the guidance and support of course coaches, their confidence in their ability to make change more broadly will grow. 20 Selected projects are presented in Table 2 and spanned several domains including addressing racism through workplace environment and culture change, curriculum development for trainees and faculty, research, and clinical care delivery to patients.
Selected antiracism projects conducted by course participants.

We developed a worksheet informed by the theories presented in the course and provided a set of prompts to help participants effectively present their project to a small group (5 learners per group) to which they were assigned in the course. During parts of the last 3 course sessions, participants presented their project and received timed feedback from other participants and a skilled faculty coach. These project-based workshops occurred 3 times and each participant presented their project twice. Participants used the time between sessions to self-pace the development of their projects. We also provided optional individualized faculty coaching between sessions to further develop projects, although these were not extensively used by participants.
Data collection
All surveys were administered via Google Forms. Surveys were administered during the course sessions to increase the response rate. Participants who did not complete their survey during the session were given weekly reminders for up to 4 weeks. Participation was entirely voluntary. We included participants in the study sample if they provided informed consent to participate in the evaluation and completed both of the pre- and post-course surveys. The Cambridge Health Alliance Institutional Review Board reviewed this study and determined that it has exempt status.
The pre-course survey collected demographic data and obtained consent to participate in the study. Pre- and post-course surveys included a set of 15 identical questions regarding participant self-rated knowledge of, comfort with, and self-efficacy in addressing racism that were designed to correspond to the aims and learning domains of the course. In addition, the post-course survey included additional questions assessing participants’ perceptions of the course and its impact on self-reported skills attainment, confidence, and commitment to antiracist action. For the first cohort, the post-course survey had 16 additional items assessing the course and its impact. On review of the post-survey, prior to giving it to the second cohort, we removed 4 of these items due to 2 not being directly related to the goals of the course and 2 providing duplicate information to other questions on the survey. This resulted in 12 items assessing participants’ reactions to the course and its impact for both the first and second cohorts. Questions for these surveys were developed, reviewed, and revised several times by the study team, as no previously validated evaluation measures for these domains in medical education and practice were available. We used 7-point Likert scale response categories for all questions and assigned numeric values to correspond to each Likert-scale response (1 = strongly disagree; 2 = disagree; 3 = somewhat disagree; 4 = neither agree nor disagree; 5 = agree somewhat; 6 = agree and 7 = strongly agree) in order to calculate mean scores for pre- and post-course responses to each item. All surveys that were completed were completed fully, and there were no missing data.
Statistical analysis
Results from the 2 cohorts of participants in the course were very similar and thus we combined them for all analyses. We examined participants’ demographic characteristics including race, pronouns, region of current practice, medical specialty, and year that participants completed clinical training using descriptive statistics. We compared the demographic characteristics of course participants included and excluded (due to nonresponse, n = 7) in the study and found them to be largely similar (data not shown). We assessed pre- to post-course changes in survey responses for each paired item by calculating a mean item response from the numeric scale scores (range of 1-7) for the pre-course survey responses and the post-course survey responses and then compared pre- to post-course differences using the Wilcoxon signed rank test for continuous measures. We used descriptive statistics to analyze post-survey questions assessing perceptions of the course and its impact. We considered P-values of <.05 to be statistically significant. All analyses were conducted using SAS version 9.4 (Cary, N.C).“The reporting of this study conforms to the DoCTRINES statement 33 [Doctrines-guideline-checklist].
Results
There were 50 participants in this course (25 participants in each of the 2 cohorts), and no one dropped out of the course. Seven participants declined to complete the survey. Thus, we analyzed survey results for 43 of 50 participants (86%) who met the inclusion criteria. Table 3 shows the demographic characteristics of participants: 79% used she/her pronouns, 7% were Asian, 13% were Black, 4% were multiracial, and 44% were White. Study participants represented 9 different specialties and graduated from their clinical training between 1980 and 2019.
Survey participant characteristics.

Participant changes in knowledge, comfort, and self-efficacy
We found statistically significant pre- to post-course improvements in all 15 survey questions across all domains (knowledge, comfort, and self-efficacy) (Table 4). For example, we found improvements in participants’ understanding of the historical context of institutional racism in medical institutions (mean score change: 5.12 [SD 1.00] to 6.42 [SD 0.76], P < .001) and their understanding of how individuals develop their racial identities over time (mean score change: 4.49 [SD 1.35)] to 6.33 [SD 0.71], P < .001) increased. Additionally, participants indicated increased comfort talking to colleagues (mean score change: 5.21 [SD 1.08] to 6.19 [SD 0.70], P < .001) and trainees (mean score change: 5.42 [SD 1.35] to 6.49 [SD 0.63)], P < .001) about racism. Participants’ reported self-efficacy also increased after the course. For example, participants indicated they felt more able to make the changes necessary to address racism in patient care at their home institution (mean score change: 4.51 [SD 1.35] to 5.56 [SD 0.91], P < .001), more confident they could teach learners how to decrease racial bias in patient care (mean score change: 4.84 [SD 1.27] to 5.56 [SD 0.91], P < .001) and more confident initiating conversations about racism with colleagues (mean score change: 4.93 [1.14] to 6.07 [0.77], P < .001).
Pre–post-course changes in self-reported knowledge, comfort, and self-efficacy.

P-value calculated using the Wilcoxon signed rank test for paired data comparing responses on pre- and post-course surveys. Scale used is 1 = strongly disagree; 2 = disagree; 3 = somewhat disagree; 4 = neither agree nor disagree; 5 = agree somewhat; 6 = agree and 7 = strongly agree.
P < 0.05, bolded.
Participants’ indicated high levels of agreement with many positive perceptions of the course and its impact (Table 5). We analyzed the 12 items assessing these domains that were answered by both the first and second cohorts. All respondents agreed that they would recommend the course to their colleagues and that the course helped them develop strategies to address racism in their home institutions. The majority of respondents agreed (somewhat agree, agree, and strongly agree combined) that the course made them more likely to work on addressing racism at their home institution (93%), that they were more committed to reducing racism through their professional work (95%) and more likely to implement their proposed project (88%).
Participant perceptions of the course and its impact.

Discussion
This evaluation suggests that our longitudinal, project-based course was well-received by participants and resulted in improvements in self-reported participant knowledge, comfort, and self-efficacy in addressing racism within their professional roles. We found statistically significant improvement in every one of our 15 paired pre- and post-course survey questions. Specifically, we observed improvements across all 3 of our educational aims: (1) to increase knowledge of racism's impacts on the practice of medicine; (2) to increase comfort with and capacity to engage in antiracism conversations at one's home institution; and (3) to increase a sense of self-efficacy to engage in strategic, project-based antiracism work at one's home institution. Our experience in implementing the course along with the positive evaluation described suggests that this course helped support postgraduate physicians in addressing racism at their home institutions.
Our findings are consistent with the results of other studies suggesting that antiracism training is generally well received by postgraduate physicians.17,19,34 Our study adds to this field of work by describing the implementation and evaluation of a multisession project-based course on a virtual platform to a diverse national cohort of postgraduate physicians both within and outside academic programs.
We learned several lessons from this work. First, by creating opportunities to focus on both individual practice and community-building, our course may have provided a learning environment that was conducive to both personal growth and collective learning. Second, our emphasis on discussing theory to understand how racism operates in professional environments may have increased participants’ knowledge of how to identify and address racism in professional practice. Finally, we presented theory and action as necessary parts of a whole by applying the theory discussed to the implementation of a formal action project. While we did not formally evaluate participants’ experience of having a formal project as a part of the curriculum, through numerous informal interactions with participants, we believe our use of the formal projects may have enhanced learning of taught material through their implementation in real-world settings in which learners were required to self-identify, adapt, and plan formal action projects that had high relevance at their home institutions.
There were several limitations to our study that must be noted. Course perceptions may have been influenced by prior experiences and lived experiences, although we did not specifically evaluate this question. The intervention was only 5 sessions, with no long-term curricular programming and this may limit the impact of the course. In addition, we did not collect long-term follow-up data on the outcome of the antiracism projects initiated as part of the course. Thus, we do not know the extent to which these projects were ultimately implemented or effective, although we plan to evaluate this critical question in future studies. Also, our evaluation relies on self-reported measures of change in knowledge, skills, and self-efficacy in taking antiracist action, rather than directly measured behaviors or actions. However, positive changes in measures of task-specific self-efficacy suggest a higher likelihood of actions, in this case antiracist actions, as well as persistence in these efforts when presented with barriers or challenges. 35 Additionally, we developed this course in 2020 with a desire to create and implement a curriculum on antiracism to address a critical gap in antiracism teaching available to postgraduate physicians. In this setting, we created survey measures that were not validated to allow us to evaluate the curriculum. We recognize that this evaluation is limited and that future studies are needed to assess the long-term impacts of the course that include changes in behavior and actions, project implementation, and qualitative information on how course graduates felt the course impacted their ongoing antiracism work. Finally, we piloted this course with physicians only. However, recruiting an interprofessional group of learners in the future may create a more diverse learning environment and have broader impacts at participants’ home institutions.
Conclusion
We demonstrated improvement in self-reported knowledge, comfort, and self-efficacy in addressing racism in medicine among participants of our longitudinal antiracism course. Our approach may be of value to other groups motivated to work on addressing racism in medicine, particularly in supporting highly motivated individuals interested in supporting antiracist organizational change at their medical institutions. We believe learnings from our evaluation may be applicable to interprofessional learning settings and institutional learning settings.
Supplemental Material
sj-docx-1-mde-10.1177_23821205241303643 - Supplemental material for From Theory to Action: Evaluation of a Longitudinal Project-Based Antiracism Course for Post-Graduate Physicians
Supplemental material, sj-docx-1-mde-10.1177_23821205241303643 for From Theory to Action: Evaluation of a Longitudinal Project-Based Antiracism Course for Post-Graduate Physicians by Camila M. Mateo, Danny McCormick, Chrissie Connors and Gaurab Basu in Journal of Medical Education and Curricular Development
Footnotes
Ethics and Consent
The Cambridge Health Alliance Institutional Review Board reviewed this study and determined that it has exempt status. Informed consent was collected from all study participants.
Acknowledgments
The authors would like to acknowledge the work of all faculty involved in this course both past and present, without whose contributions the course would not have been possible.
Author Contribution
Made a significant contribution to the concept, design, acquisition, analysis, or interpretation of data—CM, DM, CC, GB. Drafted the article or revised it critically for important intellectual content—CM, DM, CC, GB. Approved the final version of the article for publication—CM, DM, CC, GB. Agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity—CM, DM, CC, GB.
DECLARATION OF CONFLICTING INTERESTS
None of the author(s) have conflicts of interest to disclose. No authors have published, posted, or submitted any related papers from this study.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.