
Abstract
As future physicians, first-year medical students are well positioned to work on the long-term creation of a more equitable healthcare system. But how prepared are first-year medical students to begin the work of dismantling structural racism in the US healthcare system? In this study, we analyzed a sample of 75 medical-student reflective responses to a book focused on the legacy of racism in medicine. Our findings indicate that students enter medical school in a range of states of critical consciousness that are visible in their “stances” toward addressing racial inequality in the healthcare system. The stances described in our findings extend the critical consciousness framework, providing a more nuanced understanding of students’ starting orientations to health justice. Because students arrive in different stances toward confronting the systemic inequalities inherent to the US healthcare system, understanding these stances may help medical educators tailor learning experiences to medical students’ needs more effectively.
Keywords
Unresolved historical injustices have compounded the effects of the COVID-19 pandemic on Black, Latino, and Indigenous communities in the United States (Whitacre et al., 2021). The spread of the virus in these communities created a synergistic epidemic of disease, economic hardship, homelessness, and food insecurity that could no longer be ignored by healthcare providers, administrators, and politicians (Bambra et al., 2020; Krieger, 2020). In 2020, as the burden of COVID-19, the murder of George Floyd, and existing disparities deteriorated the health of racialized communities, the situation became so dire that the American Heart Association issued an urgent call to action to immediately address structural racism as a fundamental driver of health disparities (Churchwell et al., 2020). A call to address the structural violence of American healthcare, published in the American Journal of Public Health, begins with a single word in capital letters: ENOUGH (Krieger, 2020).
The inequities in health outcomes highlighted by COVID-19 are neither natural nor necessary (Bailey et al., 2017; Zimmerman & Anderson, 2019), and scholars from all corners of medical education agree the time has come to prepare our health system for change. As future physicians, first-year medical students are well positioned to dismantle racist systems in healthcare and replace them with more equitable systems of care (Ward & Randall, 2020). At present, well-reasoned processes for engaging students in anti-racist advocacy activities and addressing bias within the health professions learning environment have been conceptualized and discussed (Fadoju et al., 2021; Mateo & Williams, 2020). However, the current medical education literature does not provide researchers and medical educators with frameworks to conceptualize and design educational experiences that foster students’ development as anti-racist practitioners. Without theoretical tools to guide the development of students’ attitudes, skills, and knowledge, medical educators run the risk of providing students with health justice experiences that are mismatched with the strengths and needs of medical students. The consequences of these mismatches in medical education may have long-term negative impacts on the health of patients of color.
This study is a first step in the process of identifying key features of medical students’ development into anti-racist medical practitioners so that medical educators are better able to meet students where they are in their degree of readiness to promote health justice. To support medical educators in this goal, we conducted a qualitive analysis of student writings generated during a medical school orientation week book club activity. These writings provided insights into the ways that medical students in one large, urban medical school on the West Coast of the United States conceive of their relationship to race-conscious and anti-racist medicine.
We used critical consciousness (Freire, 2013, 2018; Jemal, 2016, 2017, 2018) as a central framework to examine how beginning medical students engaged with issues of race, power, and oppression. Critical consciousness is a powerful means of exploring how medical students begin their medical training in various stages of a journey toward achieving a deeper awareness of systemic injustices embedded in the health system. Our analysis identifies five manifestations of this awareness that we describe as a series of “stances” taken by the students in their written responses to their readings and discussions about racism in medicine. These stances may play a valuable role in supporting students’ development into anti-racist healthcare practitioners and in advancing their development into advocates for the transformation of medical education itself into an anti-racist space. We hope that medical educators will be able to use the stances described in this paper to better differentiate learning experiences for students on their journey to develop personal responsibility for recognizing, disrupting, and transforming systemic racism in medicine and healthcare systems.
Background
Although our medical school had already begun to develop curriculum centered on Health Justice and Systems of Care (HJSC), the tragic murders of George Floyd, Ahmaud Arbery, and Breonna Taylor that sparked nationwide protests against police violence and demonstrations for racial justice required an urgent response to address the educational needs of our incoming students during the summer of 2020 (Cerdeña et al., 2020). The protests amid the pandemic demanded an intervention that would highlight the violence and health disparities that disproportionately impact Black and other communities of color in the United States and the structural racism that pervades America’s institutions. Medical schools across the country sought ways to respond to growing calls (often from their own students) to acknowledge the racism, discrimination, and other unjust practices that exist within medicine and contribute to health inequities, from accessing care to health outcomes.
Our school of medicine was poised to take up this challenge. We drew on faculty expertise from the Office for Social Justice, the Office of Diversity and Inclusion, our Narrative Medicine program, and social justice–oriented student groups to explore the ways that race interacts with social conditions to undermine the well-being of racial and ethnic minorities in the United States. As part of the pilot phase of the HJSC longitudinal course required for all medical students in the pre-clerkship and clerkship phases, starting with the class of 2025, the administration decided to require all incoming medical students to read Fatal Invention: How Science, Politics, and Big Business Re-create Race in the Twenty-First Century by Dorothy Roberts (2012) and participate in a discussion and reflective writing exercise during orientation week in August 2020. The book investigates how the association of race and biology is perpetuated through problematic and even potentially harmful practices such as racialized medicine, the development of medications with racial indications, and race-based genetic testing.
Anti-racist Medical Education: Why, and Why Now?
In Fatal Invention, Roberts (2012) reports that racial disparities in health outcomes are not the result of accidental bad behavior by isolated individuals. Rather, they are the expected result of a system of racialization that has materially and negatively affected outcomes for minorities through a range of political, economic, and scientific levers for more than two centuries. Roberts describes how medical research has found no systematic evidence that supports differences in biology, physiology, or genetics among racial categories. Yet, racial categories continue to be routinely used as predictive or diagnostic tools in medical research and practice. Roberts asserts that the racialization of medical care is not a historical contingency of medicine in the United States; it is a design woven into the fabric of the medical system through a range of policy and economic initiatives. In a systematic review of racism as a social determinant of health, Paradies et al. (2015) found the consequences of racism in society and health care are directly responsible for worsening outcomes for people of color. Ultimately, COVID-19 brought these disparities in outcomes into sharp focus, but health injustice has been an enduring feature of the US healthcare system throughout its history.
In addressing the root causes of racial disparities in health outcomes, health professions educators such as Cerdeña et al. (2020) advocate for a new, race-conscious approach to medical education that acknowledges the ways that race can impact the health of patients without further ensconcing the system of racism that perpetuates inequality in health care. This new approach, broadly described as anti-racist medicine, avoids key pitfalls of previous “cultural competence” approaches to medical education and practice (Brottman et al., 2020). In its contemporary form, cultural competence focuses on the values, behaviors, and attitudes of healthcare providers as they interact with people of different cultural and linguistic backgrounds (Centers for Disease Control and Prevention, 2021; Zanting et al., 2020). In a survey of 56 healthcare professionals’ perceptions of cultural competence, Shepherd et al. (2019) found that providers valued interpersonal cross-cultural attitudes but “systemic cross-cultural approaches . . . such as a recognition of racism, power imbalances, entrenched majority culture biases, and the need for self-reflexivity . . . were scarcely acknowledged” by the respondents (p. 19).
In medical education, racist biases are often imparted to students during medical education by more senior practitioners through the hidden curriculum and other systemic avenues. Racist biases may also be reinforced by the ways that biomedical tests, medical literature, and research projects use race as a core variable (Owens & Walker, 2020; Roberts, 2012). Anti-racist approaches to medicine seek to mitigate these artifacts of systemic racism by training healthcare providers to examine the systemic dimensions of racism as it is manifested in medicine. This includes teaching students to be critical of how race is used in medical research, to understand the consequences of racism on health, and to support patients who face race-based structural barriers to obtaining quality health care. Further, these approaches are essential to achieving a meaningful and lasting state of health justice for all patients (Tobin-Tyler & Teitelbaum, 2018). For these reasons, anti-racist medical education must begin with the education of medical students.
Contemporary Approaches to Anti-racist Medical Education
Although some medical educators such as Goldfarb (2019) have expressed concern that the integration of health justice into medical school curricula could distract students from their basic science education, several groups of medical educators have spoken out in favor of producing skilled practitioners who are also capable of addressing the root causes of health injustice in the United States, beyond superficial acknowledgment of the social determinants of health and rudimentary attempts at cultural competence (Cerdeña et al., 2020; Crear-Perry et al., 2020; Heard-Garris et al., 2020; Karani et al., 2017; Paton et al., 2020; Wear et al., 2017). Sharma et al. (2018) note that when medical education fails to connect cultural competencies, social determinants of health, and adverse childhood experiences to the societal systems that produce these outcomes, it fails to prepare students to make meaningful changes to the underlying conditions that cause health inequities. According to Sharma et al., “Educators talk about poverty, but not oppression, race but not racism, sex but not sexism, and homosexuality but not homophobia” (p. 25). To this end, Sharma et al. propose adopting not just new content or better curricula but educational experiences that focus on cultivating the habits of mind and action that can lead to reductions in equity gaps.
As medical educators come to consensus on the need for health justice and anti-racist instruction in medical education, curriculum designers, faculty, and physicians are working together to confront the challenges of changing medical education from multiple angles (Brottman et al., 2020). Some authors such as Gonzalez et al. (2018) favor a focus on improving instructors’ capacity for delivering antibias training, whereas others focus on helping clinicians recognize privilege and bias (see Holm et al., 2017), and others still focus on the materials and teaching practices used in medical school (Amutah et al., 2021; Krishnan et al., 2019; Godley et al., 2020). These early efforts have demonstrated some successes, with one meta-analysis finding that individual educational interventions can promote clinical empathy in physicians, a key factor in reducing bias against patients of color (Fragkos & Crampton, 2020).
Toward Critical Consciousness in Medical Education
Addressing issues of racism in medical education will require more than a change in practice or tweaks to curricula. As Kumagai and Lypson (2009) wrote in their critique of cultural competency approaches to achieving health justice in medical education, dismantling racist dimensions of the healthcare system will require medical students to develop the ability to identify and neutralize the mechanisms of racism and, more, to want to act against racist systems (Bleakley, 2017). Fortunately, education researchers have developed a framework, critical consciousness, for describing how such an expansion of perception and action might occur.
Brazilian educator Paolo Freire conceived of critical consciousness as an individual’s ability to recognize systems of oppression and to take action against oppressive elements in order to transform one’s social, intellectual, and material reality. Freire (1968/2018) proposes this democratic pedagogical approach as a counter to the “banking model” of education, a hegemonic approach that treats learners as passive recipients of knowledge that reproduces the ideologies of the ruling class and reaffirms existing power relationships. Since its introduction in Freire’s Pedagogy of the Oppressed, critical consciousness has been studied, critiqued, and further developed by scholars, resulting in a rich body of literature that explores its philosophical, theoretical, and practical dimensions.
Carlson et al. (2006) used the concept to develop a theory of critical consciousness that further describes how critical consciousness can be observed in learning experiences. In this model derived from qualitative studies of “photovoice” presentations (combinations of still images and voice-overs) by members of poor and oppressed communities, Carlson et al. describe how individuals in an oppressed community grow and change as they develop agency in their own struggle for liberation. Through debate, discussion, and reflection, oppressed peoples can be seen to move from passivity to action. This process is fundamentally radical in nature in that it enables oppressed peoples to strike at the roots of oppression in their shared realities and to slowly build an existence free of political, economic, and social domination by hegemonic forces. Expanding on this work, Jemal (2016, 2017, 2018) conducted a review of several strands of scholarship on critical consciousness. She found that the concept serves as an “antidote to inequity and the prescription to break the cycle” of oppression that manifests in education and healthcare systems (Jemal, 2017, p. 602). These conceptions of critical consciousness are part of a growing empirical body of literature that seeks to measure and define the phenomenon (Andrews & Leonard, 2018; Diemer et al., 2017) in ways that are productive for scholars in multiple fields.
The process of developing critical consciousness is not easy, and it may cause discomfort for students, instructors, and clinicians as they identify and confront unpleasant realities about inequities in systems of care as well as latent biases or microaggressions that may manifest during clinical encounters (Dao et al., 2017; Frambach & Martimianakis, 2017; Setchell & Daiziel, 2019; Zaidi et al., 2017). As Halman et al. (2017) note in their literature review of critical consciousness in health professions education, critical consciousness requires that teachers, learners, and clinicians exhibit a willingness to challenge their own positions of power and privilege. Halman et al. note that medical students are in a particularly complex position. Regardless of their background, medical students arrive in their training as a privileged group by virtue of their association with health professions education and elite educational institutions but also enter at the bottom of a hierarchical system that places enormous cognitive, emotional, and identity-based demands on them from the very start of their education. This position makes the existentially demanding work of developing critical consciousness still more difficult.
Our review of the literature indicates that (1) health justice and anti-racist medical education are necessary to an equitable medical system; (2) medical educators may need additional theoretical tools to support their creation of anti-racist medical education programs; and (3) deeply worked theories of critical consciousness offer explanatory, theoretical, and design tools for facilitating the development of these programs. Although we have found few qualitative studies that use student voices to provide key insights into their perceptions of health justice work, such as Ona et al. (2020), our analysis in this study draws primarily from students’ own voices and writings to provide a new window into how medical students see their role in creating an anti-racist system of medicine.
Methods
The methods and analysis that follow provide conceptual and contextual frames for supporting medical educators in selecting effective health justice activities at the appropriate times in the student’s development and in ways that engage students in the pursuit of equity, justice, and health for all people. Our methodological framework was influenced by Denzin’s (2017) critical qualitative inquiry approach to research, which aims to rectify injustices and change society rather than to simply generate knowledge.
Research Question
While our initial review of student responses stemmed from our interest in the effectiveness of the reading group interventions, our reading impressed on us the variety of interpretations that students generated from the same text. Explaining this broad variation required the application of a robust framework, which was provided by the body of literature on critical consciousness. As we began to read student responses more deeply, we formulated a broad research question to guide our investigation: In what ways do matriculating medical students exhibit aspects of critical consciousness in their reflections on texts about racial injustice in medicine, and what can this tell us about developing anti-racist medical education?
Intervention Design
As an extension of the anti-racism summer book club, the incoming medical-student cohort of 2020 was required to participate in an hour-long discussion of Fatal Invention during orientation. The medical students were joining an important conversation happening within the medical school’s community, and even more importantly, they were being asked to consider and reflect on their own beliefs and assumptions about race and its uses in medicine and science, which could have a significant impact on their practice as future physicians and public health professionals. To learn about student responses to issues of health justice, we developed an educational experience that was informed by the reflective practices of narrative medicine and aligns with several principles of anti-racist medical education described by Halman et al. (2017). These included creating an assignment that (1) promotes authentic dialogue, (2) invites students to question the status quo, and (3) creates cognitive disequilibrium.
Discussion groups consisted of 18–20 students and one faculty member who facilitated conversation and provided thematic questions for consideration. After participating in the book discussion activity, students were asked to share their reflections on their experiences of reading and discussing the book by answering several open-ended questions and responding to a writing prompt:
What, if anything, do you see differently as a result of reading the book?
What, if anything, do you see differently as a result of discussing the book with your peers?
At the end of her book, Dorothy Roberts says that we, as a nation, are at a crossroads. She asks: “Will Americans continue to believe the myth that human beings are naturally divided into races and look to genomic science and technology to deal with persistent social inequities? Or will they affirm our shared humanity by working to end the social injustices preserved by the political system of race?” (312). Pointing to the detrimental effects of the first option, Roberts urges us to “choose the other path of common humanity and social change if we are to have any hope for a more free and just nation” (312). As a medical student, what does choosing the path of common humanity and social change look like for you? How might you reimagine or reinvent your role as a medical student to set you on this path? You may address your education, actions, and advocacy or any part of the medical-student experience.
We hypothesized that the sufficiently complex source material for discussion and asking open-ended questions would provoke students to respond in ways that provide insight into their perceptions of race and health justice and would elicit diverse perspectives from the students. The book also presents a range of empirical evidence and perspectives on racism in medicine that are at a suitable level for beginning medical students. This study was approved by the university’s Institutional Review Board.
Analysis
Responses and Demographics
Our sample included 163 student responses collected via Qualtrics from a total class of 183 enrolled students (91% response rate), and all respondents replied to all three questions in the assignment. Although our analysis does not directly tie student responses to racial or ethnic backgrounds, Table 1 provides a comparison of the demographics of KSOM’s entering class of 2020 versus national trends in medical school enrollment for the same year in hopes that this will help other schools in using the study’s findings in their context.
KSOM Class of 2020 Demographics vs. US Medical School Enrollment (American Association of Medical Colleges, 2021), with Percentages Rounded to the Nearest Whole Number
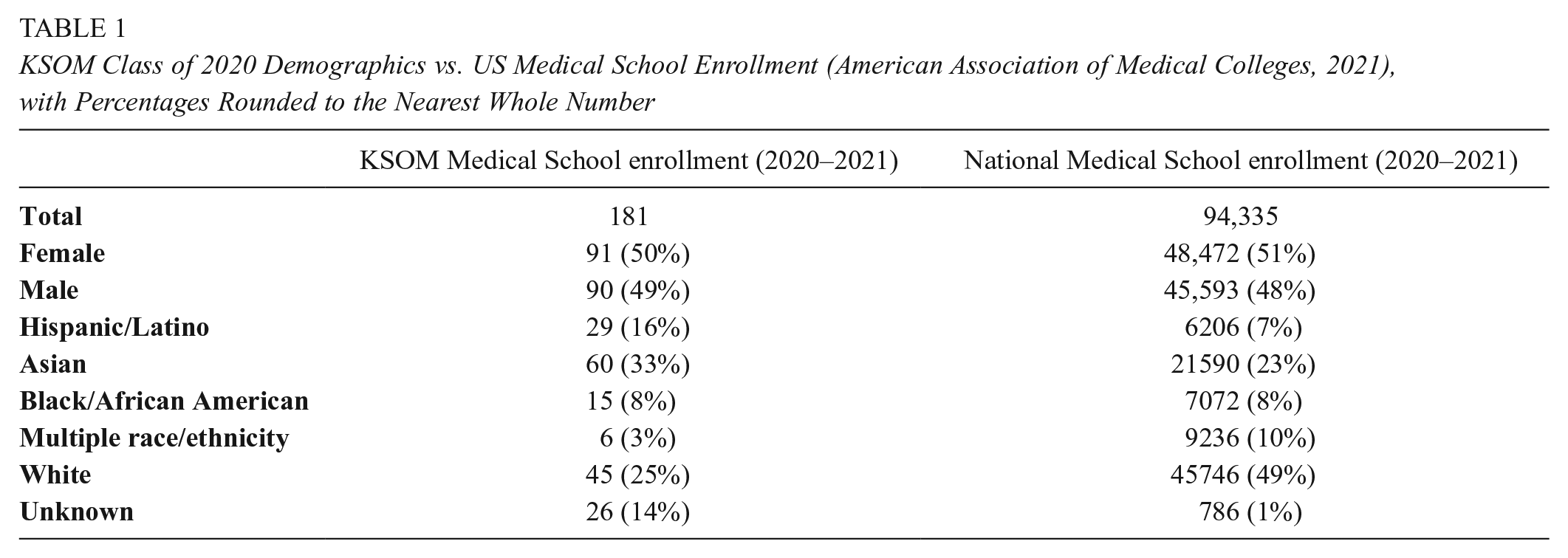
In terms of racial identification, the overall class composition includes higher percentages of Asian and Latino students than the national average, lower percentages of White-identifying students, and comparable numbers of Black/African American students.
Sampling and Coding
We conducted our data analysis using the Dedoose qualitative data analysis software. Students’ responses were uploaded as discrete documents, and each reviewed response was divided into three excerpts corresponding to the three questions in the assignment. Student responses were anonymized before being uploaded to Dedoose. Unless students disclosed information about themselves as part of their response, the authors did not make attempts to apply gendered, racial, or age labels to the respondents.
At the outset of the coding, the team adopted a systematic sampling method that used an initial sample of responses to norm the coding framework, then expanded to a larger sample of responses (Green & Thorogood, 2018). The first author drew a sample of 25 of the total 163 assignment responses (each containing one student’s responses to all three questions) to use in norming codes based on the critical consciousness framework and as a first pass of open coding for other themes that arose in students’ reflections. The initial round of coding from the theoretical framework used Miles et al.’s (2019) method of provisional coding, beginning with Jemal’s (2017) interpretation of the critical consciousness construct as it was described in Carlson et al. (2006). In this summary of the literature on critical consciousness, Jemal summarizes Carlson’s four stages of critical reflection development as (1) passive adaptation where helplessness contributes to one’s own oppression, (2) emotional engagement where emotions begin to orient individuals toward systemic causes, (3) cognitive awakening where individuals become aware of their complicity in maintaining oppression and realizing their ability to effect change, and (4) intentions to act. Each of these levels of critical reflection were treated as a code to be applied to the text. Additionally, subcodes were developed from related literature and through identification of recurring themes that emerged in the student responses. Student responses were analyzed from a sociolinguistic perspective, where semantics were treated as indicative of cognitive activities, beliefs, and emotions (Jaffe, 2009).
After coding the initial sample of 25 student responses (75 excerpts), the first author pulled key quotes and responses from Dedoose and presented them to the research team for discussion. The critical consciousness codes and new subcodes were assessed for fit by the research team in committee reviews (Merriam & Tisdell, 2015; O’Connor & Joffe, 2020). Following the initial pass and discussions, the team drew an additional 50 random student responses for the second phase of coding. These 50 responses were used to assess the fit of the emerging theoretical framework and to determine whether additional codes were necessary. In total, 228 excerpts from the 75 samples were fully coded. Appendix A includes a sample codebook of our thematic codes that may be used as a starting place by other researchers.
Researcher Reflexivity
The research team involved a total of six faculty members in the Department of Medical Education. We engaged in iterative rounds of discussion to ensure engagement in appropriate reflexive discourse around our findings (Ng et al., 2019). For example, we frequently discussed how our faculty roles may have influenced how we analyzed the students’ reflections. We also considered how our multiple positionalities—influenced by our racial, ethnic, class, sexual orientation, and gender identities and our varying degrees of privilege or lack thereof—shaped our perceptions of the overall topic of anti-racist medical education and ways in which we interpreted the data.
Validity
The validity of our theme identification and interpretation of excerpts was established through a three-step process: constant comparison, committee review, and connecting our findings to the existing literature in medical education and critical consciousness. First, following the primary coding phase, we reviewed the remaining 88 responses for divergent material that did not fit into our evolving theoretical framework. This constant comparison of our pool of sampled responses versus the total corpus ensured that other voices and responses were included in our analysis. We found that the initial 75 responses provided sufficient evidence for our theme-identification process.
Second, following the early stage of theme development, we applied a committee approach to reviewing emerging themes and their fit with the theory of critical consciousness in the context of medical education. The first author (DAN) selected and presented a series of theoretically relevant student responses to two other authors (RH and JS), trained in qualitative methods, to assess the fit of the initial theory. Following the discussion and debate from this meeting, the themes and theoretical insights were revised and presented again to the remaining three authors for assessment and discussion. After the completion of the first draft, all authors and two outside reviewers with extensive expertise in qualitative methods assessed the draft for appropriateness of claims and findings.
Finally, as part of the interpretation process, we identified and incorporated additional aspects of the medical education literature that supported our interpretations of the student responses in our initial effort to build a new theory of critical consciousness in medical education.
Findings
In our interpretations of students’ reflective writings on the issue of systemic racism in medicine, we perceived that medical students arrive in a range of developmental states of critical consciousness that do not perfectly correspond to the published literature.
In working to understand how first-year medical students approach engagement with health justice in their responses and exhibit features of critical consciousness, we began to refer to students’ thoughts as evidence of a series of “stances” that fall along a developmental trajectory ranging from less critical to more critical. Stances are sociolinguistic phenomena that result from the cognitive, affective, and positional nature of a speaker in the social world and are evident from the words that people choose to describe their thoughts and emotions in a given context (Jaffe, 2009). The concept of a critical stance is described by Curzon-Hobson (2003) as a feature of critical pedagogy that emerges under delicate conditions of trust, authenticity, and respect for the interrelationships of teachers, learners, and others. As Curzon-Hobson notes, The critical stance is characterized by a willingness to challenge, recreate, and reimagine in a manner that is searching, persistent, and resolute. . . . This stance towards our experiences is underpinned by a recognition of one’s freedom to choose, the responsibility that comes with this projection, a rejection of unreflective acceptance of value and meaning, and a celebration of self-will and the will of others. (p. 202)
The critical stance resembles the kind of open, justice-oriented models that we found in the most complex thinking exhibited by the responses from medical students. It also provides a model of engagement with health justice that is open to change and evolution, and a method of explaining how individuals respond differently to the same kinds of health justice education interventions and information. Further, conceptualizing students’ attitudes as a range of more or less critical stances allowed us to describe how the interrelated webs of thoughts, attitudes, beliefs, values, and valence may be interwoven into action and discussions of justice and equity.
One of the benefits of adopting a “stance” approach to understanding students’ responses is that it does not blame or ascribe negative valence to students who are not ready to engage in the work of health justice. Students are not represented as static entities trapped in a single state but as people who can render their minds more open to the challenges faced by others, to new possibilities for action, and to greater wisdom. In the stances presented here, more activated stances are more closely aligned to the development of critical consciousness. Furthermore, we argue that these are desirable stances for students to take before engaging in the work of health justice. Although more research is needed to understand how and when these shifts occur, we posit that, as students grow and change through their medical education, they may adopt stances that are more or less critical or may take multiple stances toward different issues or intersections of identity and justice. As anti-racist medical educators, a key desired learning outcome of our health justice curriculum is to empower students to move to the most activated critical stances that can foster social transformation.
Our analysis and review of the literature identified five thematically important stances on the developmental continuum of critical consciousness. Some of these stances accord with existing theory on critical consciousness, though others present themselves differently from the current literature because of unique experiences and contexts of first-year medical students. These include:
Stance 1—Passive adaptation: In the literature on critical consciousness, passive adaptation occurs when people adapt their understanding of the world to remain passive in the face of injustice. Student responses from this stance may exhibit (1) resistance to discomfort, (2) appeals to natural order, and (3) resistance to shouldering the burden of equity work.
Stance 2—Cognitive engagement and emotional awakening: Responses from students in this stance exhibit elements of cognitive engagement with the problem of racism as a factual and material problem. Students further along the continuum also begin to connect their cognitive activities with emotions such as sadness, anger, or shock when recounting their exposure to instances of health injustice.
Stance 3—Intentions to act: When students described a desire to take future actions to engage in the struggle for health justice, we identified these responses as coming from an “intentions to act” stance. Students in this phase have integrated the cognitive and emotional responses to injustice and are looking for a way to impact these conditions in the world.
Stance 4—Diffuse responsibility: As students develop intentions to act, they may begin to describe the ways they imagine the medical profession must change to disrupt health inequities using broad statements about medical professionals and society as a whole. These typically include depersonalized language such as “we” statements and come from a stance of “diffuse responsibility.”
Stance 5—Personal responsibility: At the highest stance in our observations of critical consciousness, students make specific statements of personal responsibility for disrupting health inequities, provide critiques of medical practice that are followed by specific plans for action, and outline specific plans for engaging in social justice activities in the near future. Although systemic change is necessary to create the conditions for reducing health disparities, a personal responsibility stance prepares individuals to see themselves as active, vital agents in the work of health justice.
The following analysis provides specific examples and interpretations of each of these stances as we observed them in student responses, along with expanded discussions of these phenomena and triangulation with the existing literature on medical education. We encourage readers to refer to the Appendix for an additional codebook with examples and definitions.
Stance 1: Passive Adaptation
In Freire (2013, 1968/2018), Carlson et al. (2006), and Jemal (2017), the passive adaptation stage of critical consciousness is signified by an attitude of helplessness among oppressed people. In this mode of thought, people actively engage in continuing their own suffering by remaining passive participants in the larger systems that maintain their oppression. In Freire’s and Carlson’s framework, the passive adaptation to oppression is a logical response to an illogical condition that gives rise to a “magical” or “naive” belief that the inhabited system must function in ways that cause them to suffer, and that these systems are immutable and natural in their order (Holmes, 2013). Passivity denotes either an unwillingness or inability to participate in the process of imagining life to be different from its current state, and adaptation describes an active set of contortions in thought and action that preserve helplessness in the face of oppression. These beliefs about the world and the static nature of oppression are antithetical to the kinds of intellectual liberation that are central to critical consciousness.
In the responses to Fatal Invention, a small number of students exhibited a stance akin to passive adaptation regarding the role of race in medicine even after reading the text and engaging in group discussions. In the critical consciousness literature, we found evidence of three forms of passive adaptation stances that appeared in students’ responses: (1) resistance to discomfort, (2) appeals to a natural order, and (3) resistance to shouldering the burden of equity work. These three themes recurred in several student responses as part of a constellation of beliefs that hinder students from fully engaging in the promotion of health justice.
First, a passive adaptation stance involves resistance to discomfort, either through deflection or minimization of the current state of injustice. In Fatal Invention, Roberts (2012) discusses the multiple ways that racial structures woven into US society since the founding of the country have been used to structure most aspects of social and economic life. In this first excerpt of a student’s reflection, when asked: “What, if anything, do you see differently as a result of reading the book?” Student 1 pivots away from the issue of race to the concept of ethnicity: To me, the book was not about race, but rather ethnicity: the political atmosphere surrounding how we look and our genetic makeup. The cases she presented, the laws she discussed, and history she described revolves around the way society views different ethnicities. I still believe that the 0.1% difference in our genetics accounts for the differences in our appearances and is a determinant for our health.
In the rest of Student 1’s responses, we found several conflicting thoughts emerge, including the assertion that “Medicine should not try to leap-frog over genetics in search of an inconsistent relationship between race and health.” Although the responses acknowledge the need to find ways to avoid unconscious racial bias in their medical practice, the initial impulse to redefine Roberts’s arguments denies or misses the central premise of the text. Ethnicity does have an anthropological and sociological meaning and function that is introduced but not elaborated on in the response, but this claim is distinct from Roberts’s arguments about the invention of race as a system that justifies and perpetuates oppression.
In shifting the dialogue from “race” to “ethnicity,” the response exhibits the kind of resistance that Wear & Aultman (2005) observed in their analysis of discussions of inequality with medical students. That is, when faced with the dissonance created by evidence of inequality (such as the role of medicine in perpetuating systems of injustice), students may respond by resisting the premise of the discussion, denying the validity of experiences of oppression, or attacking those who have been victimized by the same systems that benefit the privileged. Ultimately, students may shift arguments to avoid the uncomfortable realities of the factual and experiential histories of racism in medicine.
Student 2 provides another example that we interpreted as coming from a passive adaptation stance through a phenomenon that we observed as an “appeal to natural order”—that is, a belief that if racism did not exist, humans would devise another process for sorting and dividing people: The book’s thorough analysis of the social and political origins of race and the parallels that are drawn between early cranial measurement, eugenics, and, now, modern genetic analysis expose the repetitiveness of our tendency to internally rank our species. . . . If we didn’t have something as superficially apparent as skin color, I think humans would still invent some new way of delineating ourselves from one other just to rationalize a social ranking system.
This response contains a belief that the creation of systems of social control that lead to oppression (such as ranking systems and race) is a part of a natural tendency of human nature, speculating that humans “would invent” some other method of categorizing people into social ranks and that race is one surface-level option. This claim is antithetical to the uncomfortable thesis that Roberts (2012) provides in her book. As Roberts discusses at length, humans have indeed divided one another based on a number of characteristics, but that racism is not a natural system of ranking. As she notes in Fatal Invention, “Believing in the uniqueness and superiority of one’s own group may be universal, but it is not equivalent to race. . . . Unlike race, these observed differences did not create a set of discrete categories that every single person in the world must fit into from the day he or she is born” (Roberts, 2012, pp. 6–7). As a pervasive system of colonial control, racism is not an extension of a natural order; Roberts reminds us that it is a distinctly unnatural concept developed precisely to create unnatural divisions in the human family.
As observed in works on critical consciousness by Freire and Jemal, a passive adaptation stance can include a belief that systems exist as part of a natural order, in this case as an internal human drive to divide humans into classes or other categories. This subtle belief can complicate discussions of race because racializing systems were invented and continue to be propagated precisely because they are seen as a natural consequence of human behaviors or human nature.
Third, a passive adaptation stance can take the form of resistance to shouldering the burden of equity work. We saw many different examples of students expressing a belief that some physicians are called to work on the dismantling of racist systems in society, but that others justify reasons for opting out of that work. As Student 3 wrote: As a scientist, I do not believe that I am best suited to make nationwide policy decisions about race. While some students will pursue policy as a career I believe my future is in the operating room. . . . I am confident that in basing my medical practice on the principles of equality and equity for each of my patients I will be able to have a significant impact on the lives of my patients and have a small impact on the national inequalities that exist.
Although the student’s intention to treat patients equally at the microlevel is admirable, it ignores the strong evidence that microlevel solutions cannot address the kinds of systems-level issues associated with race that Roberts discusses in her book.
Stance 2: Cognitive Engagement and Emotional Awakening
In the critical consciousness framework described by Carlson et al. (2006), researchers identified emotional engagement and cognitive awakening as two separate phases in the development of critical consciousness. The sequential nature of this development is visible in the historical practices of teaching and learning with deeply oppressed peoples, as in the Russian Revolution. In these situations, proletarians became emotionally engaged in their own plight and used that emotional engagement to employ their collective cognitive resources to plan their liberation (Faulkner, 2017). Medical students are in a different position than the marginalized peoples that were the original subjects of the critical consciousness frameworks. US medical students face the obverse problem; they have been selected for their strong cognitive resources and have attended elite educational institutions, but some may need an emotional awakening to the suffering of others to continue the development of their critical consciousness faculties and their journey as anti-racist practitioners.
As McNaughton (2013) notes in her review of discourses of emotion in medical education, discussions of emotion and its role in medicine have historically been absent from medical education, despite the role of emotion as an embodied dimension of cognition, a sociocultural mediator of many medical practices, and a core type of labor taken up by physicians. Yet, McNaughton notes, emotions are also a central part of the ethics of practice in medicine, and students need techniques that allow them to make sense of the objective, the subjective, and the dissonant dimensions of their early experiences. For these reasons, the developmental trajectory of physicians as anti-racist practitioners must attend to both their cognitive engagement in complex problems of enacted practice as well as their emotional awakening to the needs of their patients.
Our analysis of matriculating medical students’ responses supports the important, interconnected role of cognition and emotion in understanding the physician’s role as an anti-racist practitioner such that it is more accurate to describe this stance as cognitive engagement and emotional awakening for this population. In many of the student responses reviewed, the distance between the students’ own experience of privilege and the experiences of their patients causes them to exhibit the signs of a cognitive awakening before finding their way to emotional engagement.
Cognitive engagement was marked by the use of words related to learning and thought, with students describing their thought processes in detail as they reflected on Fatal Invention. When students describe finding things “interesting,” summarize what they have learned, use quotations, or ask questions, they are approaching a subject using their cognitive toolset. For example, this response from Student 4 approaches the message of Fatal Invention as it influenced their own thought process: To me, her call to action seemed to accentuate the need for us to deracialize the biology of medicine, realizing race is a terrible proxy for genetic difference or variation, and that we need to redirect our attention to how race affects biology. I truly appreciated her logical breakdown of how economic resources could be best utilized and directed to create a better community and population health.
In this passage, the use of phrases such as “realizing” and “logical breakdown” helps to underscore the degree of cognitive engagement put forth by the student. They assess the strength of Roberts argument with critical faculties, discussed it with fellow students during the classroom session, and found that it provides an important lesson about their future as a physician. This degree of engagement with these concepts also contrasts with the comments of students in the passive adaptation stance in that the students have chosen to engage in a more nuanced or specific way with the book’s central thesis and its implications for their work in the future.
In examples of emotional awakening, students used words related to their feeling of safety, comfort, and confidence discussing these topics, and how these emotions now inform their recall of those instances. However, in looking across the responses from the students, we were struck by the strength of conviction shown by students who exhibited signs of both cognitive engagement and emotional awakening. In this example, Student 5 discusses how the arguments made by the book implore them to reevaluate their role in scientific research as it relates to race: I definitely learned that there is a great amount of work we as a society need to do in order to achieve true social change for this nation. This book allowed me to see in detail from the past to the present how society has changed and how much more we need to change to overcome the disparities and inequities that exist in our everyday lives. . . . I was shocked at how I, myself, also overlooked these details and how it could’ve affected the research I’ve conducted. It also made me question how and what I can do to help our society overcome these systemic inequities. Before I read the book, I assumed that there were biological and genetic differences between race. Growing up, I was taught about these differences and I had just accepted it. Additionally, when working in the medical field, I saw the importance of race when it came to diagnoses. The doctors that I had shadowed told me about how certain ethnic groups were at higher risk for certain diseases and ailments. As a student, I believed that they were predisposed to these diseases due to biological factors and genetics. However, what really caused these groups to be high risk was the racism they had faced. Their inequity in their environment caused them to be at higher risk for these diseases. After reading this book, I realized that humans are more similar than we are different. I learned that race was not biological, rather it was political. I was angry to find out that race was a product of racism. Race had started in order to hold power over certain groups. I was frustrated to read about the abuse that other races faced.
This student’s response employs a range of highly charged words that express emotions such as shock, anger, and frustration. These powerful emotions arise from a sense of betrayal; powerful authorities and mentors in the life of the student had used race as a central tool for describing cause and effect in ways that ultimately did not accord with dispassionate scientific practices.
This next excerpt illustrates how both cognitive engagement and emotional awakening can help students of color contextualize their experiences in medical sciences and education. Here, Student 6 acknowledges her own intersectional position as a woman of color, and how this has informed her experience in interacting with the artifacts and processes of clinical research: As a Black woman and someone who actively seeks to learn more about Black history and the REAL history of the United States (and not the watered-down version taught in public schools), I knew that race did not have a biological basis but didn’t really understand how race came to be. I also appreciated that she said that although race has no biological basis, it DOES have biological effects, decreasing the health of populations. This further affirmed the work that I hope to do to work to dismantle racism in medicine and give adequate care to Black and other minority groups that are often at a disadvantage in this country’s medical system. I also worked on a research project examining the use of race in medical guidelines, so this book was really relevant to me and my experiences. Through my project, I determined that people were using race as a biological factor within the very guidelines that are used to determine a plan of treatment. For example, there was a guideline that said Black patients shouldn’t be tested for urinary tract infections. There were also countless other examples that I found. I also like that the book mentioned how there was rarely ever any evidence or studies backing up the use of race within treatment or research studies because that’s exactly what I found in my research as well. This book reaffirmed that my project was important and a necessary topic to explore within medicine, and it made me really proud and happy that I was chosen to collaborate on that project.
As Student 6 notes, reading Roberts’ book thus served a dual function in connecting her cognition and her emotions. First, it provided her with factual information that answered her own questions about the origin of race, a topic that is suppressed in broader discourses within American education. Second, reading the book surfaced new connections between her past research activities and the valence that she attached to them. In addition to affirming her research findings, the process of engaging in health justice work through retrospective reflection made her feel “really proud and happy” about her past work. It is possible that engaging students’ cognition related to social justice may also bring emotional valence to their past experiences and promote engagement in health justice advocacy.
As students learn from their cognitive activities in medical school, medical educators should carefully consider how students’ emotional awakening may simultaneously drive learning. As identified in several studies from outside of the US context, students’ abilities to understand their own emotions can have important outcomes in the development of professional identities (Helmich et al., 2018; Rieffestahl et al., 2021). Further, in reviewing the existing literature on emotional intelligence in medicine, Cherry et al. (2014) note that “medicine is an emotionally demanding practice and medical education is an emotional process,” but emotional experiences are often regarded “as collateral to the central task of acquiring and applying practical competence” (p. 48). Consequently, medical students are expected to exhibit a stance akin to what Underman and Hirshfield (2016) describe as detached concern with a belief that their own emotional engagement may skew their judgment. Reflecting the perception that professional identity formation occurs apart from emotional development, contemporary models of professional identity formation do not contain space for helping medical students learn to manage the complex emotions that arise around their work, much less the emotional burdens associated with addressing health justice (Creuss et al., 2015). In guiding students to act productively on the emotional awakening that follows closely on the heels of their cognitive engagement, medical educators may find ways to bridge gaps between the detached concern of inaction and the motivation to act.
Stances 3, 4, and 5: Intentions to Act, Diffuse Responsibility, and Personal Responsibility
In the framework that emerged from our coding of student responses, we observed that a stance that includes intentions to act serves as a boundary between students who have progressed from cognitive engagement and emotional awakening to more advanced critical stances. When students declare an intention to act on issues of health justice, they move from a passivity that accepts the reality of the injustice faced by patients into an activist stance. That activism is the central goal of critical consciousness, where medical students become active participants in the creation of new possibilities, actions, and responsibilities that can lead to the remediation of injustice. These three stances are presented together to highlight their relationships and to demonstrate the increased levels of activation associated with each stance.
We identified three stances associated with the activation that is emblematic of the development of critical consciousness: intentions to act, diffuse responsibility, and personal responsibility. Each of these three distinct stances represents greater and more specific commitments to creating change to the systems that produce inequitable outcomes in health care. In this section, we present evidence for stances 3, 4, and 5 in sequence to illustrate how these stances transform from vaguely defined instincts about the need for critical change into assertions about the physician’s role in that critical change and finally to the individual’s specific personal commitments to engaging in anti-racist medicine. These stances are presented together to illustrate the subtle differences in activation exhibited in each stance.
Intentions to Act
Students who exhibited an intentions-to-act stance often described the important role that healthcare providers play in eliminating health inequities, as well as actions that they may take at some later date. In this example from Student 7, the writer describes their intentions to vote to change the system: For myself, at this time, I think it’s important to continue educating myself from diverse sources about inequity and racism in our healthcare system, in government, and in our communities. As a medical student, I hope to advocate for change to eliminate these inequities, whether it be as part of a student advocacy group or whether it be through conversations with my friends, family, and colleagues. I also personally am committed to being active politically and encouraging others to vote in order to effect change on a legislative level—both locally and federally—as well.
When students respond from an intentions-to-act stance, they exhibit the dawning of a critical awareness of their role in changing medical practice and society. However, these responses are marked by a lack of specifics about how they will engage in changing society. In Student 7’s responses, they affirm their commitment to acting in ways that promote equity but describe only general plans to join a student advocacy group and vote for legislative change. Although these are laudable goals and indicate an understanding that action is necessary to change the system, they are still less robust and specific than the diffuse and personal responsibility stances.
Diffuse Responsibility
From a stance of diffuse responsibility, many students discussed how all physicians, healthcare workers, and the healthcare system must work to dismantle systemic racism. This is evidenced in discussions about how “we” and “physicians” must act, but devoid of singular personal pronouns or connections to the individual’s experience. Student 8’s response calls for strong actions to remedy the injustices faced by patients, but focuses on how a diffuse “we” must engage in these actions: I think this book really opened my eyes to the underlying issues which inform the practice of medicine to the present day. To be actively anti-racist, we, as future physicians, need to critically examine every aspect of medical practice ranging from the tests we use to diagnose our patients to how we think about prescribing medications. Furthermore, it is not adequate to simply understand these truths for ourselves, we need to be vocal with senior physicians we may work with during medical school and with undergrad or high school students we may mentor.
Although the student describes their motivation to challenge the status quo in medicine and medical education, their shift from “I” to “we” indicates that the student is still growing toward a vision of themselves as an individual actor against health injustice within the medical group, feeling more comfortable in taking on the responsibility as part of a group but unclear on their specific responsibilities.
Personal Responsibility
In the personal responsibility stance, responses can contain similar sentiments as those categorized as diffuse responsibility but include very clear statements of personal intent to act. In one such response, Student 9 describes the similar goal of vocally pushing back when faced with outdated assumptions about race and medicine: When I first considered what my own action could look like, I felt discouraged by my position on the bottom of the medical hierarchy. Though that will be true for now, I still have agency and influence among my medical teachers. Believing that I can’t enact change due to my own position on a hierarchy is self-defeatist thinking and will only perpetuate bias. As a medical student, I occupy a position of privilege in my community. I intend to use this position to advocate for social changes that would have positive health outcomes for patients.
As a result of imagining themselves personally in the situation, Student 9’s response also attends to their position in the broader world of medicine and society. As the student notes, medicine is a hierarchical discipline, and there is some danger in taking a stand on issues of medical bias when it puts one in conflict with a medical educator. But in acknowledging their feelings of discouragement, the student notes that believing that they cannot enact change is “self-defeatist thinking and will only perpetuate bias.” The courage to acknowledge one’s limited position as a medical student and attempt to reconcile it with one’s perceptions of justice is also exhibited by Student 10 in describing their own struggle: When thinking about such a topic, it often becomes a little overwhelming. I sometimes feel as though there is no way that I can affect social change—I am just one person! I don’t even have a medical degree. What can I do to be a part of the change? However, if this pandemic has taught me anything it’s that it takes every individual in a society to effect change. . . . Similarly, if I make an effort to have these difficult conversations about social injustices and health disparities, then I am doing my part to help steer the course towards social change. . . . I will be learning about and seeing these health disparities firsthand. Thus, it is my responsibility to pass on what I learn to others.
Rather than seeing the limitations of their reach as a reason not to act, Students 9 and 10 both commit to supporting health justice in ways large and small from their position as learners. But in describing a responsibility to “pass on what I learn to others,” Student 10 also describes a core role of the physician as a teacher. Given the importance of the role of physicians in public discourse about health justice, this commitment to sharing their knowledge and experience with the public could have a profound impact in the long term. Teaching and public outreach are also core tenets of critical consciousness, as they play central roles in helping to raise the consciousness of other people.
In addition to the personal commitment to act in ways that promote equity, some students also indicated an awareness of their role in serving as leaders in the struggle for health justice. Student 11 wrote: As a medical student not only do I have a role of learning how to provide treatment to patients directly, but also the duty to evolve into a community leader who works as an advocate for people that have been systematically left behind for centuries. Additionally, I have to evolve into a physician who works to promote social change for my patients and to work with my colleagues to educate our country that race is not rooted in biology. My goal is to help everyone in our country to come to an understanding that systemic injustices are the root of the health disparities, not artificial biological differences that have been falsely promoted to create systems of oppression.
Student 11 joins Student 10 in identifying their role as someone who must “educate our country” about the role of injustice in causing health disparities. The student also acknowledges that this is a process where they must consider not just leadership within their own hospital setting. They must also demonstrate an awareness of the situation of medicine within a broader social context. These kinds of comments highlight two educational duties that exist for physicians: a duty to educate the public about health, and a duty to lead society in directions that preserve health (Cruess & Cruess, 2010).
In this final student response in our analysis, Student 12 demonstrates a high level of critical awareness as they note specific features of how they envision their role in the struggle to achieve health justice. Speaking directly from their perspective as a member of the Latinx community, this student’s response highlights a number of sources of medical knowledge that they think might perpetuate inequity in health care: As a medical student, I believe choosing the path of common humanity and social change looks like leveraging my role as a scholar within medical education to speak my truth of my Latinx community and challenge the system directly. I think it is important to have a critical lens and question/challenge in each of the following areas:
Medical textbooks that further perpetuate the biological determinants of race
Individuals (including but not limited to faculty members, professors, lectures, mentors, and/or peers) that continue to create a stigmatized view of race whether this is within the hospital or even in clinical rounds
Patient interactions (one-on-one) including racially biased clinical notes on charts or explanations of disease in rounds
Larger systemic institutions like hospitals still using race when assessing eGFR or other outdated algorithms that are using race as a risk factor to diseases.
In pointing to a need for a critical perspective on these four sources of knowledge, the student’s response highlights the importance of questioning received knowledge that has been built on the shaky ground of race-based approaches to medicine. Building from their identification of sources of injustice that they are preparing themselves to challenge as they move through their medical education, the student also describes how they intend to take personal responsibility to change themselves as they “reimagine” their role to include advocacy: Beyond this, I would also reimagine my role as a medical student to serve as an advocate by doing the following (besides the above):
Add a layer of additional factors that impact health (e.g., racism, structural violence, disenfranchisement, dehumanization, and public policies) as I learn each medical condition. I will focus on the direct science of pathology and do my best to acknowledge and change any of my implicit biases.
Be self-aware of treating patients from minority communities with close care to do my best to narrow the chasm in communities of color not only having lack of healthcare access but also inferior healthcare (as noted by Dr. Roberts) on an individual level.
Push for research that is driven by science (not by race) while also ensuring communities of color are becoming represented in research.
Push for policy changes to expand social welfare of communities of color (especially the undocumented immigrant population, incarcerated population, and Black population).
As the final exemplar in our analysis, this student’s response comes from a place of ambition, imagination, and deeply felt commitment to health justice. Their stance allows for emotion, reason, and action to exist and align as a statement of specific, personal commitment to health justice. This stance is the essence of the critical consciousness that we wish to cultivate in our students and may serve as the central goal of future designs for programs in health justice education.
Discussion
The evidence from student responses in this study supports two findings that are relevant to investigators in medical education. First, in addressing our research question, we found that students enter medical school at various points on a spectrum of critical consciousness development that spans from passive adaptation to the status quo to feelings of personal responsibility for promoting health justice. Second, this spectrum is characterized by a range of stances that proceed from less to more critical and activated. Although students are likely to move through these stances as they grow and develop wisdom from their clinical work, more research is necessary to determine whether it is possible for students to experience a quantum leap from a lower level of critical consciousness to a higher level without considerable time, thought, discussion, and reflection. As students change their stances, we might expect their perceptions of their role in the fight for justice to change; equally, as their role within medicine changes, their stance may change as well. However, more research is necessary to identify how and why such changes occur and whether students may also experience devolutions in their states of consciousness as well.
Implications for Medical Educators
Although more research is necessary, we present three broad principles that may help to create the conditions necessary to shift students from lower to higher critical consciousness stances. These principles focus on the ways that the stance framework provided here might influence how we think about the development of dimensions of critical consciousness development from curricular, individual, and community perspectives.
Curricular Approach—Provide Multiple On-ramps
As we found in our reading of student reflections, not all students arrived in their first year in the same stance. Each student in our study had their own story, their own identities, and their own set of orientations to the work of achieving health justice. As part of their process of professional identity formation, students’ development of critical consciousness may span many patient encounters and many years as they become progressively more involved in clinical practice (Manca et al., 2020; Zaidi et al., 2021). Because we anticipate that students’ level of critical consciousness will affect how they receive and understand learning opportunities in health justice, their opportunities to learn and grow must be targeted at a level that is appropriate for them.
We suggest that curriculum developers and medical educators create multiple ways for students to become involved in the work of health justice so that students are guided to the right opportunities to become engaged at the right time in their professional formation. These “on-ramps” to health justice work could include optional experiences such as community service opportunities, featured patient or patient advocate speakers, or other kinds of activities that may already be in progress at an institution. An example from our new health justice curriculum was an instance where a small group of advanced first-year students approached the course directors seeking deeper opportunities for action to be included in the curriculum. This feedback is being used to design future sessions, and it served as an opportunity for the course directors to guide the students to an on-ramp for an option to apply to participate in a longitudinal experience working with our Street Medicine program that serves local unsheltered individuals. Another potential approach may focus on using the stances in the medical-student coaching process. Coaches may find the stances particularly useful in assessing how students are developing because of their experiences and to provide students with experiences that will further promote their development as anti-racist practitioners.
Differentiating instruction based on students’ stances may have considerable benefits for students. While more evidence is needed in future studies, it is possible that a mismatch between the design of health justice learning experiences and students’ level of critical consciousness may lead to some of the negative dynamics reported in the literature. Students who are in a passive adaptation stance may feel bored, disconnected, threatened, or compelled to play a devil’s advocate role in discussions that require greater degrees of critical consciousness to undertake. Equally, students who have developed intentions to act may feel bored, disconnected, or burdened by a need to review the factual and emotional dimensions of health justice that they have already encountered in their own journeys.
In anti-racist medical curricula, events may need to be sequenced in ways that promote the development of critical consciousness and changes in stances. Certain activities may also benefit from a mixture of students of various stances, as peers can have a greater effect on one another over time. Although more research is needed to make specific claims about the effectiveness of different interventions, this approach may prove especially useful to schools that have adopted longitudinal health justice curricula.
Individual Approach—Feed the Champions but Avoid Minority Taxation
Feeding the champions is a concept from professional development that involves providing resources, leadership opportunities, and recognition to those who are most willing to adopt and model new practices. The champions can speak to the tangible benefits of an intervention to more hesitant members of the community. Similarly, in health justice education, identifying and resourcing the most activated students who exhibit more critically conscious stances could help to accelerate other students’ involvement in health equity work.
However, a word of caution in this strategy: Several authors warn against placing this burden entirely on students of color, and Ona et al. (2020) found that the implementation of an anti-racist program for medical students failed to attend to the needs of students of color themselves. During the anti-racist program, students of color were under the added burden of explaining racism to White students who have not experienced it. Further, Ona et al. found that when participating in anti-racist trainings that are aimed at a predominantly White audience, students of color do not receive opportunities to discuss and unpack their own emotional and cognitive experiences of racism. This burden, called the minority tax, is an expectation that students of color will spend their time educating their peers about the importance of health equity. While we saw several examples of self-identified students of color wishing to take up a greater leadership role in educating their peers and physicians about health justice, this sentiment was not universal. Rather, it may be worthwhile to enforce the majority tax, which places the burden of learning about the importance of health justice on those who need education on the matter (Mensah, 2020). This approach also seeks to establish more robust allyship practices that are supportive of students and patients of color.
Community Approach—Holistic Development of a Community of Practice
Our analysis indicates that students in more critically conscious stances are highly motivated to engage in learning about health justice and may have much to teach faculty about the value, meaning, and outcomes of equity work. Therefore, a community of practice approach may yield opportunities to improve teaching about health justice groups by treating faculty and students as interconnected communities (Lave & Wenger, 1991; Steinert, 2010; de Carvalho-Filho et al., 2020; Wenger, 1998). In a community-of-practice approach, faculty and students can play important roles in mutually reinforcing the importance of health justice, creating spaces for egalitarian discussion, and providing students with opportunities to inform faculty beliefs about health justice. Further, it provides opportunities to place more activated, critically conscious students at the center of community discussions and work rather than at the peripheral locations reserved for students. By breaking down the traditional structures that place students in the distal role of newcomer, they may be better able to galvanize other students into action.
Taken together, using an understanding of the stances to plan multiple on-ramps to health justice work, identifying and feeding the champions, and fostering a community of practice will help create the right conditions in the learning environment for other instructional interventions to have the maximum benefit.
Limitations
This study has several limitations that should be considered by future scholars as they apply our theory and findings to their contexts. Broadly, these include:
Our sample was confined to medical students at a single institution. Though our sampled population is demographically similar to those at other large, urban medical schools, researchers may encounter other dynamics at institutions such as historically Black colleges of medicine or medical schools that are embedded within rural health centers. Further, admission priorities across institutions may complicate the sample of stances available.
Our theory is built from students’ responses to a single intervention and provides only a snapshot of students’ thinking. More research using different epistemic modes will be necessary to trace student thinking as it changes and develops over time.
Our qualitative approach did not allow us to provide quantitative data on distributions, counts, or other measures of frequency related to students’ stances. Future research may use quantitative measures such as those provided by Diemer et al. (2017) to provide snapshots of distributions and changes.
Our sample of student responses was chosen without attention to demographics. Except in cases where students specifically referred to their own backgrounds as part of their responses, no demographic information was used to guide the selection of the sampled responses. Although all responses were ultimately reviewed as part of the constant comparison process, researchers’ use of demographics to weight the sample may produce a different kind of result or a different study.
Directions for Future Research
By integrating the theory of critical consciousness stances presented in this paper, along with the three implications for practice described in the discussion, we believe that medical educators will be better positioned to overcome the challenges identified in the current literature on health justice and anti-racism education. However, this research has raised a host of new issues for future study. In our future studies exploring the development of critical consciousness, we will explore questions such as:
Do health justice activities influence students differently if they are in different stances?
Can quantitative measures of critical consciousness be used to externally validate the stance framework?
Do stances change naturally over time, and how might the stances look different in resident populations?
We invite other scholars and researchers to use this model to investigate these questions as well in their own contexts and populations.
Conclusion
Health justice education is a challenging area of medical education research, and little is known about how medical students evolve into practitioners who are prepared to take on the work of advocating for equity in the health system. Researchers, curriculum developers, and medical educators have much more to discover about how their incoming students approach their roles as health justice and anti-racist medical advocates. By seizing this moment to develop more targeted health justice education experiences, medical educators may help to foster the growth of the anti-racist practitioners who will lead the charge to promote equitable healthcare outcomes in our society.
Footnotes
Appendix
Acknowledgements
We would like to thank Drs. Pamela Schaff, Sonali Salluja, Edgar Rivera Colón, Charles Kaplan, Seth Holmes, and Ricky Bluthenthal for their key contributions, critical feedback, and vigorous debates during the development and completion of this project.
Authors’ Note
This study was approved by the University of Southern California’s Institutional Review Board.
Authors
DANIEL NOVAK is director of scholarly activities in the Office of Medical Education Research and assistant professor of social medicine, population, and public health in the University of California, Riverside School of Medicine. His research interests include theoretical approaches to instructional design in professional education, equity in the development of digital health and educational technologies, curriculum renewal in medical education, and curricular approaches to promoting medical-student research and scholarship.
RONAN HALLOWELL is assistant professor of clinical medical education in the Department of Medical Education of the Keck School of Medicine of the University of Southern California. His research interests include health justice education, the learning sciences, Native American medicine traditions, narrative medicine, and transformative learning.
KAIROS LLOBRERA is assistant professor of clinical medical education and director of diversity and inclusion programs at the Keck School of Medicine of USC. His academic interests include narrative medicine; undergraduate, graduate, and pre-health education; US immigration; critical race theory; and US ethnic/minority literatures.
JACOB SCHREIBER is instructor of clinical medical education in the Department of Medical Education at the Keck School of Medicine of the University of Southern California. His research interests include medical student and practitioner wellness, discourses of medical practice and physician acculturation, and curriculum evaluation.
ERIKA WRIGHT is an assistant professor of clinical medical education, associate director of the Keck School of Medicine's narrative medicine and HEAL (humanities, ethics, art and the law) programs, and a lecturer in English Department at the University of Southern California. Her current research focuses on the role of medical/health humanities in medical education and the representation of confidentiality in Victorian literature and culture.
DONNA ELLIOTT is a professor of clinical pediatrics (educational scholar), vice dean for medical education and chair, Department of Medical Education at the Keck School of Medicine of USC. Her research interests include healthcare disparities, structural competence, and professional identity formation.