
Abstract
Background
Racialized health inequities are poorly addressed in medical education, often presenting race without social context and perpetuating racialized biases. Reframing the understanding of race as a social construct and incorporating anti-racism education into medical curricula are essential to mitigate health inequities. Our study describes an anti-racism curriculum audit conducted for the University of Ottawa Undergraduate Medical Education pre-clerkship program. This audit informed the development of an anti-racism toolkit designed to serve as a systematic guide for medical schools undertaking curriculum reforms.
Methods
A comprehensive anti-racism curriculum audit was conducted on pre-clerkship curriculum content from May 2020 to August 2021. Content flagged for concern was categorized into 4 themes: insufficient representation of racialized populations, race-based generalizations, cultural insensitivities, and reinforcement of stereotypes.
Results
The curriculum audit evaluated 772 course modules, completed by 18 medical students. A total of 224 (31.6%) modules contained one or more racial biases. The most prevalent concern was insufficient representation of racialized populations, identified in 145 flagged comments (55.1%). Curriculum content also perpetuated race-based generalizations (n = 75 flagged comments, 28.5%), racial stereotypes (n = 23 flagged comments, 8.8%), and cultural insensitivities (n = 20 flagged comments, 7.6%).
Conclusions
This anti-racism curriculum audit revealed a lack of diverse representation, alongside the persistence of race-based generalizations, stereotypes, and cultural insensitivities in a large proportion of the pre-clerkship curriculum. An anti-racist lens and curriculum are necessary to reduce bias in medical education and empower medical students to provide equitable care to the diverse Canadian patient population.
Keywords
Introduction
Medical care has a longstanding history of racial inequities, with compelling evidence suggesting that health inequities disproportionately affect racialized communities in Canada and around the world. 1 These race-based inequities have resulted in higher rates of morbidity and mortality among racialized patients who seek care in the Canadian medical system. An expanding body of literature shows that medical education curricula contain implicit and explicit biases with respect to race, ethnicity, gender, and other social identities. 2 Medical research and education have contributed to perpetuating these biases and reinforcing false beliefs and stereotypes regarding biological differences between racial and ethnic groups, which further exacerbate health inequities and resource gaps within marginalized communities.2,3
Studies show that patients who identify as racialized are more likely to die from pregnancy-related complications, heart disease, cancer and coronavirus disease compared to non-racialized patients.4–6 Furthermore, a 2022 Statistics Canada report revealed that Black and South Asian populations had significantly higher coronavirus-related mortality rates compared to non-racialized groups. 7 This report concomitantly highlights that Black individuals often receive poor preventative healthcare in their early years, leading to the development of chronic conditions, which translates to an increased probability of mortality from coronavirus.5,8 To add to this burden, studies show that individuals who have experienced racism in medicine are considerably more likely to delay seeking medical attention, leading to more unresolved healthcare needs.7,9
Racism is a broad concept that can be discussed at many different levels. Systemic racism encapsulates all manifestations of racism, which may then be further subdivided into individualized and structural racism. 10 Individualized forms of systemic racism include internalized racism, which refers to negative self-perceptions and the acceptance of negative societal beliefs or stereotypes about one's own racial group.10,11 Interpersonal racism involves race-based discrimination between individuals, including both implicit bias and overt acts of prejudice. 10 Structural racism refers ways in which societies foster racial discrimination through mutually reinforcing systems of housing, education, employment, earnings, benefits, credit, media, health care, and criminal justice. 12 Institutional racism refers to differential access to goods based on race or policies and practices within specific institutions or organizations that contribute to the production of racialized inequities.10,11
To address the harmful health effects of racism in the Canadian health care system, medical schools must acknowledge their role in dismantling structural racism by teaching their trainees to recognize, understand, and actively confront racism in medicine.13,14 In Canada, undergraduate medical curricula do not consistently teach about racism and its role as a determinant of health. It is an unfortunate reality that racial inequities are embedded in medical curricula, as evidenced by numerous examples, such as the scarcity of darker skin tones in medical textbooks. This racial underrepresentation creates assumptions where “normal presentations” are based on white populations and inferring white as the default race when no race is mentioned.15–18 This assumption is often referred to as a white standard (or a white norm), where whiteness defines the normal or accepted range of conduct and characteristics, and all other racial categories are contrasted with whiteness as deviations from the norm. 19 This persistent disregard also fails to train learners to recognize skin changes on varying skin tones, significantly impacting diagnosis and subsequent medical management. Race-based stereotyping and generalizations are commonplace in medical teaching, and these biases form the basis of cognitive shortcuts that have a powerful influence on medical decision-making and practice. 3 Clinical practice has historically and incorrectly used race as a biological proxy for genetic variation when it is, in fact, a social construct. 17 Race has been used as an intrinsic component to adjust clinical diagnostic algorithms, such as assigning higher estimated glomerular filtration rate (eGFR) to Black patients with the assumption that Black individuals have greater muscle mass or through the race-based correction of spirometry values for Black and Asian patients based on an unfounded theory that these populations have a lower lung capacity compared to white individuals.20–23 These “race-based adjustments” imply a white standard to which other non-white values need adjustment, 22 leading to harmful diagnostic and treatment errors among racialized patients.
Although racism and other forms of conscious or unconscious bias will perpetuate disparities in medicine, little guidance has been published on strategies to identify and eliminate structural racism from medical curricula. 24 The Medical Council of Canada (MCC) has recently included “Black Health” and “Providing Anti-Oppressive Health Care” to the MCC examination objectives under the “medical expert” role, as outlined in the Canadian Medical Education Directives for Specialists (CanMEDS) framework.25,26 Regardless of these objectives being designed to describe the attributes expected of medical graduates entering residency in Canada, they remain poorly addressed and implemented in medical school curricula. In the context of this work, we approach racism primarily from an institutional perspective, with a focus on medical education. We identified 4 key components within a medical curriculum that reflect institutional and/or structural racism: (1) lack of diverse representation, which refers to the absence or underrepresentation of racialized individuals or perspectives; (2) race-based generalizations, which refers to assumptions or statements applied broadly to groups based on race; (3) cultural insensitivities, which refer to inappropriate or dismissive responses to the beliefs, customs, or experiences shared within a culture; and (4) reinforcement of stereotypes, defined as the perpetuation of fixed and overgeneralized beliefs about racialized groups.
This study aimed to describe an anti-racism curriculum audit conducted within the University of Ottawa Faculty of Medicine Undergraduate Medical Education (UGME) Medical Degree (MD) program. The primary objectives were to: (1) identify areas within the pre-clerkship MD program curriculum that were deemed as being culturally insensitive, holding race-based generalizations, reinforcing stereotypes or lacking diversity; (2) create an anti-racism toolkit to facilitate the identification of racial biases within medical curricula; and (3) provide anti-racism recommendations for curricular reform to the Faculty of Medicine MD Program Curriculum Committee. The results from this work can serve as a tool to guide anti-racism curriculum work for other medical education programs.
Methods
University of Ottawa Pre-Clerkship Curriculum Overview
Pre-clerkship is a 2-year introduction to pre-clinical medicine, which consists of the components listed in Figure 1. All teaching content is delivered in French or English, according to the language stream of instruction. The detailed breakdown of the pre-clerkship curriculum content is available in Supplemental Material 1. Clinical opportunities are also incorporated within the pre-clerkship program, specifically for family medicine, rural exposure, and elective shadowing opportunities. The pre-clerkship years serve as a foundation for the subsequent clerkship years, which are predominantly composed of clinical rotations.

University of Ottawa Pre-Clerkship MD Curriculum Teaching Components.
Rationale for Initiating an Anti-racism Curriculum Audit
We initiated a curriculum review following discussions of harmful race-based generalizations and gaps that were identified within the pre-clerkship MD curriculum at the University of Ottawa. These discussions were amplified during the COVID-19 pandemic and in the wake of the murder of George Floyd, which brought renewed attention to the persistent social and health-related impacts of anti-Black racism and created a heightened sense of urgency for meaningful action. Two key initiatives emerged from these discussions between leaders, students, and educators within the faculty of medicine: the establishment of the Anti-Racism Curriculum Working Group (ARCWG) and the launch of an anti-racism curriculum audit. The ARCWG, chaired by co-author GE, was mandated to develop recommendations for integrating anti-racist and race-conscious medical concepts into the University of Ottawa's MD program.
This project served as an environmental scan to spearhead a program-wide development and implementation of an anti-racism curriculum. This pre-clerkship curriculum audit was the first step toward the development of an anti-racism toolkit. This approach has been applied to the clerkship (years 3 and 4 of the MD program) curriculum audit, where findings will be presented in a subsequent publication.
Development Process of an Anti-racism Toolkit
We completed the pre-clerkship curriculum audit with the support of the Faculty of Medicine Anti-Racism Curriculum Working Group (ARCWG). Two medical students (PB and SH) led the review with substantial support from the University of Ottawa Faculty of Medicine. The student leads collected all course content outlined in Figure 1 from the Ottawa Elentra Consortium, an online platform to manage and deliver curriculum content to learners. 27 Student leads completed an initial review of the year-one curricula prior to the commencement of the full audit, guided by The Upstate Bias Checklist: A checklist for Assessing Bias in Health Professions Education Content. 28 This checklist is designed for faculty members when developing or reviewing content delivered for medical learners, with an overarching goal of avoiding the burden on learners to call attention to biased material. The checklist is sectioned into thirteen domains known to be prone to bias: (1) race and ethnicity, (2) sex and gender, (3) sexuality, sexual behavior and sexual orientation, (4) disability and ableism, (5) mental health and substance use, (6) weight and weight bias, (7) immigration status, nationality and language, (8) poverty and socioeconomic status, (9) age and ageism, (10) religion, spirituality and culture, (11) incarceration and carceral status, (12) rural health and rurality, and (13) interprofessional communication. To our knowledge, this checklist has not been formally evaluated or implemented outside its original context at SUNY Upstate Medical University. Nonetheless, the checklist has been explicitly designed for content development and review in health professions education and provides a comprehensive framework for identifying and categorizing bias, with domains directly relevant to the objectives of this audit. We therefore utilized the race and ethnicity domains as a guide when conducting the initial review for our preliminary audit. Race was defined as a social construct that groups humans based on shared physical or social qualities, and ethnicity was defined as groups that share a common identity-based ancestry, language, or culture. 28 The items we utilized from the checklist during the initial review included (1) “Are explicit biological differences between racial or ethnic groups stated?” and (2) “Are biological differences between racial or ethnic groups implied.” When we identified such implications, we further assessed whether the content was essential, scientifically accurate, defined racial groups as biological constructs, and whether the information was used in standardized examinations. We also addressed the promotion of stereotypes, bias, shame, and stigma.
Student leads independently reviewed all first-year semester one (Foundations Unit, described in Supplemental Material 1), guided by The Upstate Bias Checklist, and compared findings to ensure consistency and accuracy. We curated a modified checklist, or toolkit, with 3 main considerations to flag: opportunities for increased representation, race-based generalizations, and cultural insensitivities. This preliminary toolkit served as the foundation for the instructions we provided to the student volunteers (see Supplemental Material 2).
Volunteer Recruitment
Once faculty members approved the preliminary toolkit, we initiated volunteer recruitment. We invited medical students across all 4 years of the UGME program at the University of Ottawa to volunteer. Interested students completed a Google Form to indicate their cohort, language preference for reviewing content (French or English), and available time commitment. Volunteers also had the opportunity to rank curriculum content to review based on preference. Once we recruited volunteers, we assigned course material to each student. We allocated course materials based on preference and current year of study, ensuring we restricted students to reviewing course content they had previously completed. We shared an email outlining the instructions, timeline, responsibilities, as well as the year-one audit results with the volunteers (see Supplemental Material 2). We allotted a timeline of one month for completion for each student. We instructed volunteers to flag areas that contained race-based generalizations, lacked representation, or were deemed culturally insensitive. Furthermore, we encouraged volunteers to identify and propose specific areas within the curriculum where increased representation should be considered. To recognize efforts, we provided hours towards the medical student performance record, an academic document describing student performance in medical school, as well as a letter of recognition from the assistant dean of equity, diversity, and Inclusion upon request (ES).
Once volunteers completed their review, the 2 medical student leads (PB and SH) completed a final review of all content, ensuring consistency, thoroughness, and accuracy. In reviewing the aggregated feedback, student leads noted that several flagged concerns involved stereotyping, defined based on The Upstate Checklist as a fixed, overgeneralized, and oversimplified image or idea of a particular type of person or thing; often widely held and applied to whole groups of people. 28 As a result, “reinforcement of stereotypes was added as a district category during the content review process. This led to the establishment of 4 main categories: (1) lack of diverse representation, (2) race-based generalizations, (3) cultural insensitivities, and (4) reinforcement of stereotypes. Notably, each module could contain multiple flags across more than one category. We compiled the information in an Excel spreadsheet, organized by year, unit, teaching format, reviewed, and suggested changes. We completed this final review within a month, and the report was submitted to the University of Ottawa ARCWG. Subsequent steps included the ARCWG summarizing the results into a report and compiling recommendations related to curriculum development, faculty training, and policies to support anti-racism education in the MD program. 29 Following audit completion, we created a formalized toolkit as a blueprint to be used by other medical schools interested in initiating a curriculum audit (see Figure 2 for toolkit overview, and Supplemental Material 3 for the detailed anti-racism toolkit).

Anti-Racism Tool-Kit Overview.
Statistical Analyses
Descriptive statistics were used to summarize the data. Categorical variables were reported as frequencies and percentages. All summaries were conducted using Microsoft Excel.
Results
Proportion of Curriculum Content Reflecting Racial Biases
A total of 772 curriculum materials were reviewed by 18 medical students. The reviewed curriculum components included 645 didactic lectures, 55 case-based learning (CBL) sessions, 6 team-based learning (TBL) sessions, and 66 Society, Individual, and Medicine (SIM) lectures. Due to inaccessibility, we excluded 7 didactic lectures and 9 SIM lectures from the total count and omitted them from the audit. Figure 1 provides a detailed breakdown of each teaching format. We classified the flagged content into 4 main categories: (1) insufficient representation of racialized populations, (2) race-based generalizations, (3) cultural insensitivities, and (4) reinforcement of stereotypes. Overall, we identified racial biases in 31.6% of pre-clerkship content, with material flagged under one or more of these categories. We flagged slightly more material in year one compared to year 2 (29.8% and 33.5%, respectively). Among the teaching formats, we found CBL sessions had the highest proportion of flagged content, with recommendations made to 68.0% (n = 25) of year one and 40.0% (n = 30) of year 2 CBL sessions. Figure 3 summarizes these results.

Proportion of Course Material Flagged for Racial Biases.
Categorical Distribution of Flagged Curriculum Content
The most frequently flagged category was insufficient representation of racialized populations, constituting 55.1% (n = 145) of flagged concerns, with many lectures and sessions lacking adequate visual aids of disease manifestations on the skin of color. Race-based generalizations accounted for 28.5% (n = 75) of flagged concerns. These flags included those that framed race as a risk factor for disease states or painted racial/ethnic minoritized populations as being uniform. The portrayal of white patients was predominant in clinical vignettes and images, and thus positioned white patients as the standard point of reference or the assumed default for patient care. Cultural insensitivities and reinforcement of stereotypes comprised 8.75% (n = 23) and 7.6% (n = 20) of flagged material, respectively. Figure 4 summarizes these results.
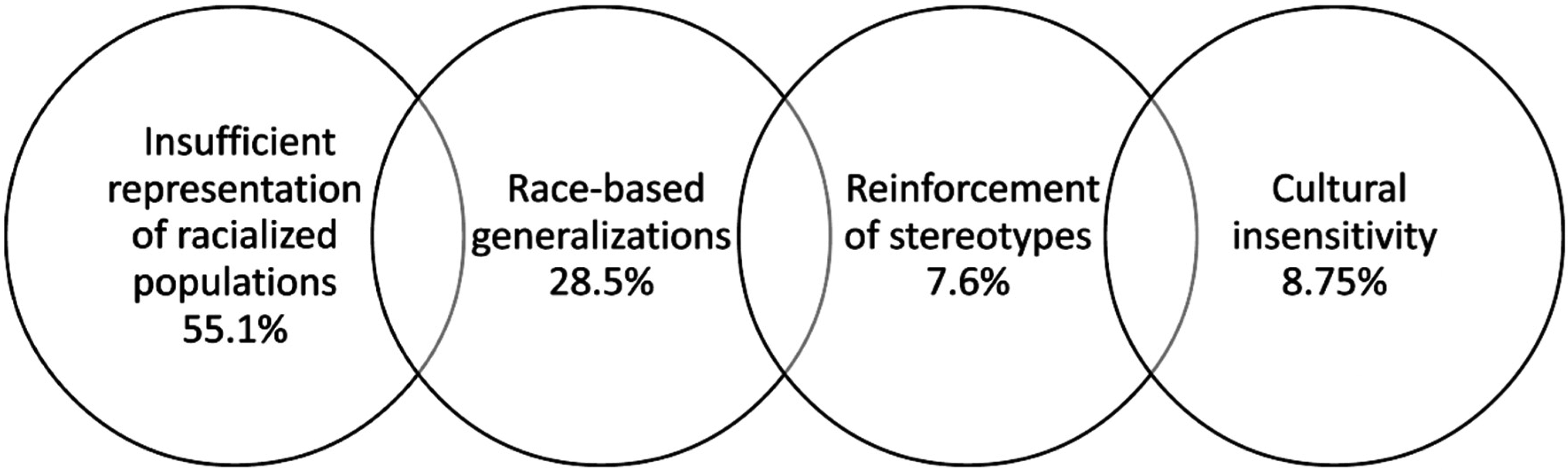
Proportion of Flagged Course Material According to Categories Established Through Audit.
Discussion
This project provides a comprehensive roadmap for medical schools to employ a systematic anti-racism curriculum audit, offering a replicable methodology to identify and address racial biases in medical education. The anti-racism curriculum audit, encompassing 772 modules across the first and second years of the MD program at the University of Ottawa, revealed a strikingly high proportion of underrepresentation of racialized populations, race-based generalizations, cultural insensitivities, and reinforcement of stereotypes. These findings uncover the racial inequities woven within medical teachings and encourage medical schools across the nation to critically evaluate and reform the curricula, with the collective goal of providing equitable care to our diverse patient population.
In many medical schools, the “hidden curriculum,” defined as the set of implicit influences to survive an institution, such as unspoken rules, customs, and rituals, insidiously perpetuates that poorer health outcomes among racialized communities are the result of biological and cultural inferiorities. 30 These misconceptions instill false beliefs and unconscious biases that propel systemic racism and influence medical judgement that continues to shape the perception and treatment of racialized minoritized populations in the healthcare system.31,32 Notions such as Black individuals age slower, possess thicker skin and have a higher pain tolerance compared to white individuals are few of many falsifications that not only lack scientific merit, but perpetuate harmful stereotypes that lead to suboptimal care. 31
Our findings reveal that nearly one-third of the pre-clerkship curriculum contained racial biases, with more than half of the flagged content attributed to insufficient representation of racialized populations. The predominance of white populations in clinical vignettes and medical imagery within the medical curricula echoes previous curriculum reviews and textbooks. 33 When race is included, it is often presented as a “white versus non-white” dichotomy, a perspective that minimizes the rich heterogeneity of non-white populations and implicitly establishes whiteness as the normative standard. 19 Moreover, the portrayal of race in medicine is often oversimplified. Broadly categorizing patients as “Black” or “Indigenous” disregards the complexities of racial identity, diluting the diversities within groups. These implications have transient impacts far beyond the classroom, as they can have potentially life-threatening consequences in clinical practice. The eGFR calculation, for example, is a widely utilized clinical algorithm that incorporates race as a covariate and simplifies the race coefficient as “Black” or “non-Black.” This dichotomy incorrectly assumes all Black patients have similar genetic ancestry, a shortcoming that has severe ramifications, including delayed listing for donor kidney transplantation when urgently required. 20
The outcome of our work has now been translated into a call-to-action. A set of recommendations, established by the University of Ottawa ARCWG, has been provided to the Faculty of Medicine to integrate anti-racist and race-conscious medical concepts within the MD program. 29 Findings of this audit have been further leveraged to support the development of a longitudinal anti-racism curriculum with clear descriptions of the concepts, issues, topics, and skills to be taught, alongside guidance on how the curriculum could be effectively integrated into the current program.
Beyond our institutional outcomes, our work aligns with broader scholarly efforts. A recent scoping review by Binda et al 34 underscores the growing attention for anti-racism education in undergraduate medical training and the need to equip future physicians with the skills required to address systemic racism in healthcare. The review outlines key considerations for anti-racism undergraduate medical curricula design and implementation, including addressing racial inequities, integrating and expanding upon anti-racism strategies throughout medical training, and aligning assessments with learning objectives. Our audit contributes to select proposed directions by providing a structured, racial bias-informed toolkit to identify racial inequities in existing content within medical curricula and by informing ongoing faculty-wide efforts to embed these findings into a longitudinal framework.
Beyond our local institutional context, medical schools can use the proposed toolkit as a guide, adapting its components as needed to identify gaps within curricula. As our audit was embedded within larger faculty collaborations and anti-racism initiatives, similar structural support would be essential for other institutions to achieve sustained, longitudinal impact. By providing a replicable methodology and defined thematic categories of bias, this study offers a practical tool for advancing anti-racism in medical education.
Limitations
The hidden curriculum is a powerful influencer of attitudes and behaviors in medicine, which can undermine the formal curriculum. 35 Our curriculum audit did not aim to capture the nuances of the hidden curriculum, posing an inherent limitation to comprehensively addressing racism in medicine. While we aimed to capture the various facets of racial biases within the University of Ottawa MD program pre-clerkship curriculum, the 4 themes of racial bias presented remain non-exhaustive, as structural racism is complex, multifaceted, and dynamic. The term structural racism is often used interchangeably with systemic or institutionalized racism, although previous works have proposed distinct definitions for each, further emphasizing these complexities.10,11 Furthermore, there are noteworthy intersectional dimensions such as ageism, ableism, and sexism that are important considerations but fell outside the scope of this audit. We also acknowledge that racialized groups are not monolithic and vary in subjective lived experiences that may be overlooked within medical education. Nonetheless, the toolkit serves as a practical resource and should be utilized alongside faculty-wide efforts to enact long-standing efforts to integrate anti-racist and race-conscious medical concepts with medical curricula.
We conducted the curriculum audit during early stages of faculty-wide reform efforts at the Faculty of Medicine in 2020, limiting our audit to the 2020 to 2021 curriculum content. Given significant shifts in the political and social landscape since 2021, particularly around issues of equity and inclusion in education, it is important to acknowledge that some aspects of the current context may differ, and future audits should consider these evolving dynamics. Nonetheless, lectures and sessions are delivered by sessional instructors, and course content has historically been passed down from year to year between presenters, with minimal to no changes made to course material. While informal student feedback suggests that the current course content remains largely unchanged from previous years, a formal assessment is required to confirm.
Anecdotally, the nature of the internal review conducted by medical students indicates that the auditors were trained by the same curriculum they were auditing. Future audits may benefit from external auditors to mitigate biases. Additionally, inter-auditor differences were noted and mitigated by a secondary review by lead authors; however, a more robust training session could serve to further enhance inter-rater reliability.
Lastly, an inherent limitation of this audit was that although learning objectives are identical, the lecture material delivered is different between French and English cohorts, therefore, potentially generating different recommendations. This limitation pertains uniquely to the University of Ottawa, as it is the sole bilingual medical school in Canada. Although beyond the scope of this audit, efforts to standardize content across language cohorts would promote uniformity and reduce potential discrepancies in learning experiences.
Conclusions
Medicine relies in part on the art of pattern recognition—a skill that cannot be acquired effectively in diverse groups when not adequately showcased. This anti-racism curriculum audit revealed that much work is required regarding anti-racist teachings in medicine. Findings revealed a lack of diverse representation, alongside the persistence of race-based generalizations, stereotypes, and cultural insensitivities in a large proportion of the pre-clerkship medical curriculum. Medical students are more comfortable identifying conditions with increased exposure, which ultimately enhances our ability as physicians to provide culturally sensitive care. Adopting an anti-racist approach in medicine is necessary to reduce bias and empower medical students to provide equitable care to the diverse Canadian patient population.
Reporting Guidelines
We utilize the Standards for Quality Improvement Reporting Excellence (SQUIRE) 36 checklist to ensure all necessary items are included in reports of improving healthcare (Supplemental Material 4).
Supplemental Material
sj-pdf-1-mde-10.1177_23821205251390303 - Supplemental material for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit
Supplemental material, sj-pdf-1-mde-10.1177_23821205251390303 for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit by Patricia Burhunduli, Saada Hussen, Yuanyi Song, Laura Muldoon, Lisa Abel, Kassia Johnson, Craig M. Campbell, Jasmin Pagé, Gaelle Bekolo Evina and Ewurabena Simpson in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205251390303 - Supplemental material for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit
Supplemental material, sj-docx-2-mde-10.1177_23821205251390303 for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit by Patricia Burhunduli, Saada Hussen, Yuanyi Song, Laura Muldoon, Lisa Abel, Kassia Johnson, Craig M. Campbell, Jasmin Pagé, Gaelle Bekolo Evina and Ewurabena Simpson in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-3-mde-10.1177_23821205251390303 - Supplemental material for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit
Supplemental material, sj-docx-3-mde-10.1177_23821205251390303 for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit by Patricia Burhunduli, Saada Hussen, Yuanyi Song, Laura Muldoon, Lisa Abel, Kassia Johnson, Craig M. Campbell, Jasmin Pagé, Gaelle Bekolo Evina and Ewurabena Simpson in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-4-mde-10.1177_23821205251390303 - Supplemental material for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit
Supplemental material, sj-docx-4-mde-10.1177_23821205251390303 for Developing an Anti-Racism Tool Kit for Medical Education: A Pre-Clerkship Curriculum Audit by Patricia Burhunduli, Saada Hussen, Yuanyi Song, Laura Muldoon, Lisa Abel, Kassia Johnson, Craig M. Campbell, Jasmin Pagé, Gaelle Bekolo Evina and Ewurabena Simpson in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors wish to thank the members of the Anti-Racism Working Group, including Drs Denice Lewis, Cathy Tsilfidis, and Monnica Williams, for their commitment during project implementation. We would like to acknowledge Drs. Avery Palmer, Haley Gommerman, and Rahul Kapur for their contributions to review content and for their work on the parallel Indigenous curriculum audit, where findings will be published once complete. We would like to thank all curriculum audit volunteer auditors: Drs Abdullah Haroon, Anand Dhatt, Chanhee Seo, Dana Ghanem, Deion D'Souza, Eimaan Khan, Grace Zhu, Ibrahim Mohammad, Libny Pierre-Louis, Linda Mardinos, Nacera Hanzal, and Naomi Abayomi.
Ethical Considerations
There are no human participants in this article, and informed consent is not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Authors’ Contributions
ES and GEB suggested the study conception and design, and all authors provided insight and feedback. PB and SH performed material preparation, data collection, and data analysis. YS supported data analysis. PB and SH wrote the manuscript, and all authors contributed to editing and reviewing. PB completed the interpretation of data and final manuscript revisions. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Ottawa Faculty of Medicine.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the present study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.