
Abstract
Guidelines for professionals practising in healthcare settings recommend that autistic people seeking care should receive neurodiversity-affirming support. However, education on neurodiversity is not widely included in health professional training in Australia. With a focus on health equity for autistic, neurodivergent people, we conducted a healthcare improvement initiative addressing the need for neurodiversity education in an Australian tertiary hospital through a change process. This project was conducted from May to November 2022, led by neurodivergent, disabled doctors who developed neurodiversity education for two hospital departments, refined through Plan-Do-Study-Act cycles and feedback surveys. The feedback survey, which included an opportunity to provide comments, was completed by 29 of 44 attendees, a response rate of 66%. Respondents agreed the education was relevant to their work (97%, n = 28), and reported more confidence (83%, n = 24) and acceptance (90%, n = 26) of autistic patients and colleagues. Themes identified in the analysis of the open-ended questions included reducing negative attitudes (biases), recognizing unmet neurodiversity learning needs, and a shift in perspective. Neurodivergent doctors led this healthcare improvement project to educate hospital clinicians about neurodiversity. The theme of reducing bias emerged from the open-ended responses, highlighting the importance of this work, given bias contributes significantly to health inequity.
Lay abstract
Barriers to autistic people accessing healthcare include health professionals with negative attitudes (biases). This study created training for hospital doctors and nurses about reducing healthcare barriers so autistic people can be included. We taught about neurodiversity affirming support, which means accepting and valuing neurodivergent people because they belong in our diverse society. The team included two neurodivergent, disabled doctors, and two research experts. The training was based on guidelines about quality hospital care, supporting autistic people, and the experiences of neurodivergent doctors. Meetings were held with hospital education leaders to find out what kinds of training doctors and nurses preferred. A feedback survey was created to find out about experiences within the training. Three groups received the training. First was Junior Medical Officers in the Emergency Department, who are qualified doctors training to become specialists. The second was specialists and doctors in the final stage of training before becoming specialists in the Geriatric Medicine department. The third was nurses in the Emergency Department. The majority of the survey responses said the training was relevant and made them feel more confident in supporting and more accepting of autistic people. Themes from the open-response questions were “bias,” “neurodiversity knowledge” and “perspective shifts.” These describe becoming aware of biases and stigma and having these challenged; wanting to know more about supporting neurodivergent people; and changing their point of view to understand neurodivergent people. These findings can support other hospitals to train staff about neurodiversity-affirming support.
Introduction
Neurodivergence is an umbrella term inclusive of mind and brain differences such as autism, which diverge from societal expectations of normative functioning (Kapp, 2019). Although not all neurodivergent people experience disability, the interaction between neurodivergence and the attitudinal, cultural, political, and environmental expectations of society is often disabling (Berghs et al., 2019; Kapp, 2019; Kayess & French, 2008; Shaw et al., 2024). As a result, their opportunities, participation, and autonomy in society are compromised (Kayess & French, 2008), which causes significant disadvantages including disparities in health and well-being (Australian Institute of Health Welfare, 2024; Newell et al., 2023). Health disparities experienced by autistic people include higher rates of premature deaths, preventable diseases, avoidable hospitalizations, and suicides (Hwang et al., 2019; Newell et al., 2023; Vohra et al., 2016). This health inequity is one of the driving forces behind the collective activism efforts of the disability rights and neurodiversity movements (Kapp, 2019; Kayess & French, 2008). Health inequity also provides an ongoing focus for improvement efforts within healthcare systems (Arnold et al., 2024; Huang et al., 2024).
The pursuit of health equity, a state in which healthcare systems are responsive to the diverse healthcare needs and potential of all people, regardless of their individual social position or circumstances (National Academies of Sciences & Medicine, 2017), is important to communities affected by health disparities and is part of the “quintuple aim” of healthcare quality improvement science (Nundy et al., 2022). This field recognizes that the domains of health equity, healthcare system efficiency, the experience of care for consumers and providers, and population health outcomes are inextricably linked (Backhouse & Ogunlayi, 2020). Furthermore, improvement in one domain has a reinforcing effect on improvement in the other domains (Nundy et al., 2022). Quality improvement interventions therefore employ a systematic process of harnessing knowledge to measurably improve specific aspects of healthcare delivery (Backhouse & Ogunlayi, 2020). Quality improvement science differs from research (Backhouse & Ogunlayi, 2020). Research uses a scientific approach to developing new knowledge, through rigorous methods that address clearly defined scientific questions (Backhouse & Ogunlayi, 2020). Contrasting this, healthcare quality improvement studies seek to improve healthcare using established knowledge and guiding theories of learning, change, or implementation (Ogrinc et al., 2019). A quality improvement change intervention involves planning and testing changes to healthcare delivery through iterative adjustments, learning through comparison of the results of the tests to predicted outcomes (Backhouse & Ogunlayi, 2020). Over time, this continuous adaptation and refinement builds evidence for the change (Backhouse & Ogunlayi, 2020).
A quality improvement approach to a health disparity problem involves engaging with communities affected and involving them in the planning, design, and delivery of interventions (Nundy et al., 2022; Purnell et al., 2016). Leveraging community insider knowledge through participatory approaches means interventions will be more likely to achieve their aims since they will be structurally and culturally appropriate for the communities they serve (Den Houting, 2021; Purnell et al., 2016). Two common problems that cause health disparities for societally marginalized communities are healthcare access barriers, and biases held by health professionals towards disadvantaged communities (Nundy et al., 2022; Purnell et al., 2016). Both causes are potentially modifiable, making them relevant targets for healthcare improvement interventions.
Implicit negative biases, which are judgments made without conscious effort, occur within moments of non-autistic people encountering autistic people (Sasson et al., 2017). In contrast, encounters between autistic people are not lacking on measures of rapport or accurate information exchange (Crompton, Ropar, et al., 2020; Crompton, Sharp, et al., 2020; Rifai et al., 2022). It is not yet known whether non-autistic people can learn to communicate in similarly accurate, unbiased ways with autistic people. However, interventions that reduce bias toward autistic people by teaching non-autistic people to be more inclusive hold promise (Gillespie-Lynch et al., 2022; Saade et al., 2023; Waisman et al., 2023). Bias can be reduced by increasing one's autism knowledge or through interactions with autistic people who disclose their autism diagnosis (Gillespie-Lynch et al., 2022; Sasson & Morrison, 2019; Waisman et al., 2023). Therefore, it might be that educating non-autistic people to reduce their biases is best achieved by educators who are themselves autistic.
When it comes to the problem of healthcare barriers, autistic healthcare consumers experience barriers to accessing care, and autistic health professionals experience barriers to employment (Doherty et al., 2022; Shaw et al., 2023). In Australia, one in five people have a disability yet employment of people with disabilities in the public sector, including government healthcare services, lags below the national target of 7% (Commonwealth of Australia, 2020). Healthcare services increasingly recognize that reducing disparities for underemployed groups of health professionals is important since it can improve healthcare safety and quality (Silver et al., 2019; Tsugawa et al., 2017). This is because healthcare professionals who belong to marginalized societal groups improve health outcomes when they deliver care to consumers belonging to those same groups (Silver et al., 2019). Evidence for improvements in population health outcomes arising from concordance between healthcare provider and consumer attributes includes the reduction of preterm births among First Nations babies in Australia (Ireland et al., 2022), the increased life expectancy and reduced mortality for Black people accessing primary care in the United States (Snyder et al., 2023), and a greater likelihood of survival among women experiencing an acute myocardial infarction (Greenwood et al., 2018). As more disabled health professionals enact their right to employment, the outcomes of disabled patients could be compared for differences arising as a result of receiving care within services that do or do not, reduce employment disparities for disabled health professionals (Bernard et al., 2023; Iezzoni, 2016). When healthcare professionals and patients share identity attributes it can reduce healthcare disparities and furthermore, disabled health professionals can advise services on reducing barriers from their own lived experiences (Doherty et al., 2024; Iezzoni, 2016; Silver et al., 2019).
Healthcare professionals’ knowledge about reducing access barriers and reducing bias is therefore important to the pursuit of autistic people's health equity (Doherty et al., 2022, 2023, 2024). These considerations are also reflected in clinical practice guidelines for supporting the well-being of autistic people in Australia (Trembath et al., 2022). The guidelines are designed for use in healthcare settings and were produced utilizing participatory approaches involving autistic people at all levels of design, leadership, and community consultation (Trembath et al., 2022). A similar process was used in the development of counterpart guidelines for autistic people in New Zealand (Whaikaka, 2022). Both sets of guidelines recommend autistic people in healthcare settings should receive neurodiversity-affirming supports, which are further described as individualized accommodations that are strengths-based and facilitate attainment of autistic people's participation, well-being, autonomy, and human rights (Trembath et al., 2022; Whaikaka, 2022). However, despite these recommendations, to our knowledge education about neurodiversity and neurodiversity-affirming supports has not been commonly included in the education activities of health professionals in Australian hospitals.
The study addressed the gap between guideline recommendations and hospital clinician education by leveraging the lived experiences of neurodivergent, disabled doctors to design and implement neurodiversity education in an Australian hospital, for the first time. The aim was to improve adherence to the clinical practice guidelines for supporting autistic people (Trembath et al., 2022; Whaikaka, 2022) by addressing clinician educational needs regarding neurodiversity, neurodiversity-affirming supports, and the barriers that may prevent delivery of these supports including healthcare professional biases and lack of accessibility (Sasson & Morrison, 2019; Trembath et al., 2022; Whaikaka, 2022). A quality improvement approach was utilized, adding to existing research by describing how stakeholder engagement facilitated the change process and shaped iterative adaptations of the neurodiversity education intervention (Ogrinc et al., 2019). By reporting this health professional education change process and the experiences of participants, the study can serve as a model for other healthcare services undertaking similar improvements.
Method
Context
The study was conducted across two departments, Geriatric Medicine and the Emergency Department (ED), at Sir Charles Gairdner Hospital, a metropolitan tertiary public hospital in Australia. Usual hospital education processes involved department education leaders planning and organizing education programs to meet the professional development needs of staff in their departments. Education for Geriatricians and Geriatric Medicine Advanced Trainee Registrars was delivered via an online meeting platform. In the ED, education was held in-person with separate teaching sessions for nurses and for Junior Medical Officers (JMOs).
The quality improvement team included two study leads, an autistic, ADHD, disabled Geriatrician, and a neurodivergent JMO working in the ED. They identified a lack of neurodiversity and autism education for staff in their respective departments and sought to change this. The departments were selected as a convenience sample, based on the study leads’ knowledge of local workflow processes and connections to stakeholders and participants, predicting these factors would support a quality improvement change process. Two academic researchers completed the team, contributing expertise in healthcare professional education and inclusive workplaces for autistic people.
Stakeholders
Stakeholders were initially engaged through the study leads meeting with Geriatric Medicine and ED education leaders (n = 4) in May 2022, to review existing processes, seek perspectives and feedback about neurodiversity as an education topic, and tailor the education activity to the needs of each participant group. Stakeholder discussions focussed on confirming the absence of neurodiversity education for clinicians in the departments and reviewing the clinical practice guideline recommendations about neurodiversity affirming supports for autistic people that had recently been published in Australia and New Zealand (Trembath et al., 2022; Whaikaka, 2022). Stakeholder consensus on the proposed study was achieved, with the agreed aim of educating clinicians about neurodiversity to improve their knowledge and capability to adhere to guideline recommendations. Stakeholders determined the need for a feedback survey to assess participant perceptions of the relevance of neurodiversity education, their neurodiversity education needs, opportunities to improve the education experience, and to share the findings of the study with stakeholders and through publication. Three teaching sessions of 1-hr duration each were allocated for this project, allowing the neurodiversity education to be delivered to different groups of hospital clinicians: ED JMOs, Geriatricians and Geriatric Medicine Advanced Trainee Registrars, and ED nurses.
Intervention
The study leads planned a neurodiversity education presentation with a focus on autistic people who work in and use hospital services. A literature search of existing models identified no neurodiversity education programs created by and for Australian, neurodivergent hospital clinicians. Education content was developed by the study leads following review of autism education research (Gillespie-Lynch et al., 2022), guidelines relating to quality healthcare standards for hospitals (Australian Commission on Safety and Quality in Health Care, 2017), and the autistic community co-produced guidelines about neurodiversity affirming support of autistic people in healthcare settings (Trembath et al., 2022; Whaikaka, 2022). Discussions regarding the study leads’ own lived experiences of neurodivergence and disability and how these interacted with their experiences of healthcare as both consumers and providers also influenced the neurodiversity education design. The priority topics chosen for the neurodiversity education were autistic people's health equity, healthcare provider biases, and barriers to healthcare experienced by neurodivergent people. Study lead discussion outcomes and reflections were recorded using the workplace text-based online messaging platform. After considering the risks and benefits of workplace disclosure, (Edwards et al., 2024) The study leads decided to openly disclose their neurodivergence and disability to participants during the delivery of neurodiversity education, with the goal of reducing participant negative biases. (Crompton, Sharp, et al., 2020; Heasman & Gillespie, 2019; Rifai et al., 2022).
Evaluation measures
Department education records captured the neurodiversity education sessions as they occurred over time and the total number of participants was determined by the study leads counting and recording this during the sessions. This was used to determine the survey response rate.
A feedback survey aiming to investigate the experiences of staff attending neurodiversity education, comprising seven questions (Appendix 1) taking approximately 3 min to complete, was developed. The survey was designed according to the stakeholder priorities of investigating the perceived relevance of neurodiversity education and the neurodiversity education needs among participants, as well as identifying opportunities to improve the education experience. The initial draft of the survey was written by the study leads, then distributed to stakeholders (n = 4) who assessed the survey items for content validity. Stakeholder feedback regarding clarity and wording of the survey items was incorporated into the survey (Appendix 1) which asked participants to respond to questions on a 5-point Likert scale; multiple-choice questions; and two open-ended questions, “Was there anything about the presentation you found particularly useful?” and “Do you have any other feedback?” The feedback survey underwent validation of the distribution process among participants attending the first neurodiversity education for ED JMOs (Figure 1). No additional feedback was received, and no further changes were made to the survey instrument.

Iterative adaptations of the neurodiversity education.
At the subsequent teaching activities for Geriatric Medicine doctors and ED nurses, participants were offered the finalized feedback survey at the conclusion of the neurodiversity education. Stakeholder meetings informed the survey distribution with an online survey link emailed to Geriatricians and Geriatric Medicine Advanced Trainee Registrars by the department education leads after the teaching activity, using the SurveyMonkey™ program. For ED nurses, the survey was offered on paper at the end of the activity.
Plan-Do-Study-Act (PDSA) cycles were used to iteratively improve neurodiversity education (Taylor et al., 2014). The study leads met with stakeholders and one another prior to each session to review feedback survey responses, reflect on experiences, and decide on process changes to test through iterative adaptations. All stakeholder meeting decisions and outcomes were recorded and circulated by summary emails after each meeting.
Analysis
Descriptive statistical analysis of quantitative results was completed in Microsoft Excel, including the survey response rate and median responses for categorical survey items. For the free text responses, the lead author undertook analysis drawing from the principles of deductive thematic analysis to qualitatively analyze participant data, which involved a “top-down” approach utilizing an existing conceptual framework to structure and interpret data (Braun & Clarke, 2006). This decision reflected the quality improvement design of this study, which did not seek to create new scientific theory through qualitative data analysis and instead aimed to understand participant experiences in relation to identified stakeholder priorities and the healthcare quality improvement aims of the study. Therefore, the framework for analysis of qualitative data in this study comprised the guiding survey question, “Was there anything about this presentation you found particularly useful?” and the study aims of educating hospital clinicians about neurodiversity affirming practices and reducing access barriers and bias experienced by autistic people in healthcare settings. The lead author entered the raw data from the surveys word for word into Microsoft Excel, then read and re-read the responses in full to become familiar with the data. Following this, the lead author assigned initial codes to the data, derived from the framework. These initial codes were grouped into categories to derive themes and subthemes from the data. Ongoing comparison of the data to the framework was continued until no new insights were gained from the data. Once this independent review was completed, the raw data, codes, and themes were reviewed by the second study lead who provided feedback via discussion. No changes were made after robust discussion between the study leads, which focused on alignment to the framework to achieve consensus.
Ethical considerations
The study was exempted from the institutional research ethics review pathway under the National Statement on Ethical Conduct in Human Research (5.1.22) following registration and approval of the study protocol with the institutional Quality Improvement Office (QA47173), and was deemed to be of negligible risk. (National Health and Medical Research Council, 2007) Reporting adheres to the Standards for QUality Improvement Reporting Excellence in Education reporting guideline checklist (Ogrinc et al., 2019).
Neurodiversity education participants were informed verbally that the project was registered as a quality improvement project and that completing the feedback survey was voluntary and anonymous. Participants were informed that the project aimed to improve education for hospital health professionals about neurodiversity, and that findings would be shared at conferences and in publications. Given the project was conducted at a single hospital site, with participants and stakeholders known to the researchers as workplace peers, anonymity of survey responses and stakeholders was a key consideration. Anonymity was protected by limiting the collection and reporting of participant and stakeholder information to their area of clinical practice only. Consent to participate in the survey was considered granted if participants chose to complete it.
Results
Plan-Do-Study-Act cycles
Neurodiversity education was delivered to 65 hospital staff across three sessions and PDSA cycles were used to iteratively advance the intervention in response to feedback and experiences. Participants’ area of practice is described in Table 1. Figure 1 shows the education content and activities as they were iteratively adapted over successive sessions.
Participant area of practice.
Plan-Do-Study-Act cycle 1
The objective of PDSA cycle 1 was to learn about barriers to delivering the neurodiversity education, and how participants would respond to the feedback survey. Concerns about the sensitivity of lived experience discussions were predicted by stakeholders and study leads to be a potential barrier to participant engagement. Psychological safety was therefore proactively managed by explaining the expectation for confidentiality of discussions to participants at the start of the neurodiversity education session, signposting potentially sensitive topics during the session, providing contact information for mental health support services, and giving explicit permission for participants to take breaks or use sensory, attention and emotional support strategies throughout the session (Figure 1). A slide presentation and an icebreaker activity were created and rehearsed by the study leads (Figure 1). The neurodiversity education was delivered to 21 ED JMOs and the feedback survey distribution process was validated, with a link to the survey emailed to JMOs following the teaching activity by ED education leadership staff.
Plan-Do-Study-Act cycle 2
The study leads reviewed their experiences and the outcome of the feedback survey distribution validation. There were only two survey responses, from 21 participants, a response rate of 9.52% (Figure 1). A delay of two days occurred between the neurodiversity education session and sending the survey link email, therefore emailing immediately after the activity was implemented, predicting this may improve the response rate. Stakeholder discussions predicted that adding content about autism in older people would improve engagement for participants from the Department of Geriatric Medicine (Figure 1). The second neurodiversity education session was delivered to 32 Geriatricians and Advanced Trainee Registrars.
Plan-Do-Study-Act cycle 3
The response rate for the second neurodiversity education session improved to 56.25% (n = 18/32). Stakeholder discussions about the learning style preferences of ED Nurses predicted interactive team-based activities would be preferred by this group (Figure 1). Task improvisation anxiety was predicted to be a potential barrier to participant engagement and this risk was managed by allowing participant choice to be involved in the activity or observe. Some aspects of the activity were disabling for the lead author including sensory overload from noise and reduced predictability due to task improvisation (Figure 1), so the second author led the interactive activity. The third neurodiversity education session was delivered to 12 ED nurses and 11 completed a feedback survey giving a response rate for the session of 91.67%.
Survey results
An overall survey response rate of 66% was achieved (n = 29/44). All Likert scale and multiple-choice items were complete except one Likert response item from one respondent. There were 26 responses to the open-ended survey items.
Figure 2 provides results for the responses to the Likert scale survey items. The median response to the item, “This topic was relevant to my work” was “strongly agree” with all except one respondent who did not complete that survey item selecting “strongly agree” or “agree” (n = 28, 97%). For the item, “After this teaching I feel more accepting of autistic colleagues” the median response was “strongly agree” with 26 (90%) respondents selecting “strongly agree” or “agree” and three (10%) respondents selecting the neutral response. For the item, “After this presentation I feel more confident caring for autistic patients” the median response was “agree” with 24 (83%) respondents selecting “strongly agree” or “agree” and five (17%) selecting the neutral response.

Survey responses of clinicians attending neurodiversity education.
For the multiple-choice survey items regarding neurodiversity topics respondents would like to learn about in future, the topics that received the greatest number of positive responses were “distinguishing between autism, ADHD, dementia and mental health issues” (n = 21, 72%), “reasonable adjustments for neurodivergent hospital staff” (n = 18, 62%), and “ADHD in medicine/ED” (n = 14, 48%).
The analysis of the open-ended survey items assisted with understanding participant experiences of neurodiversity education and what they considered particularly useful, in their own words. The themes and subthemes identified in the analysis are shown in Table 2, along with illustrative participant quotes.
Themes generated from open-ended survey response items with illustrative participant quotes.
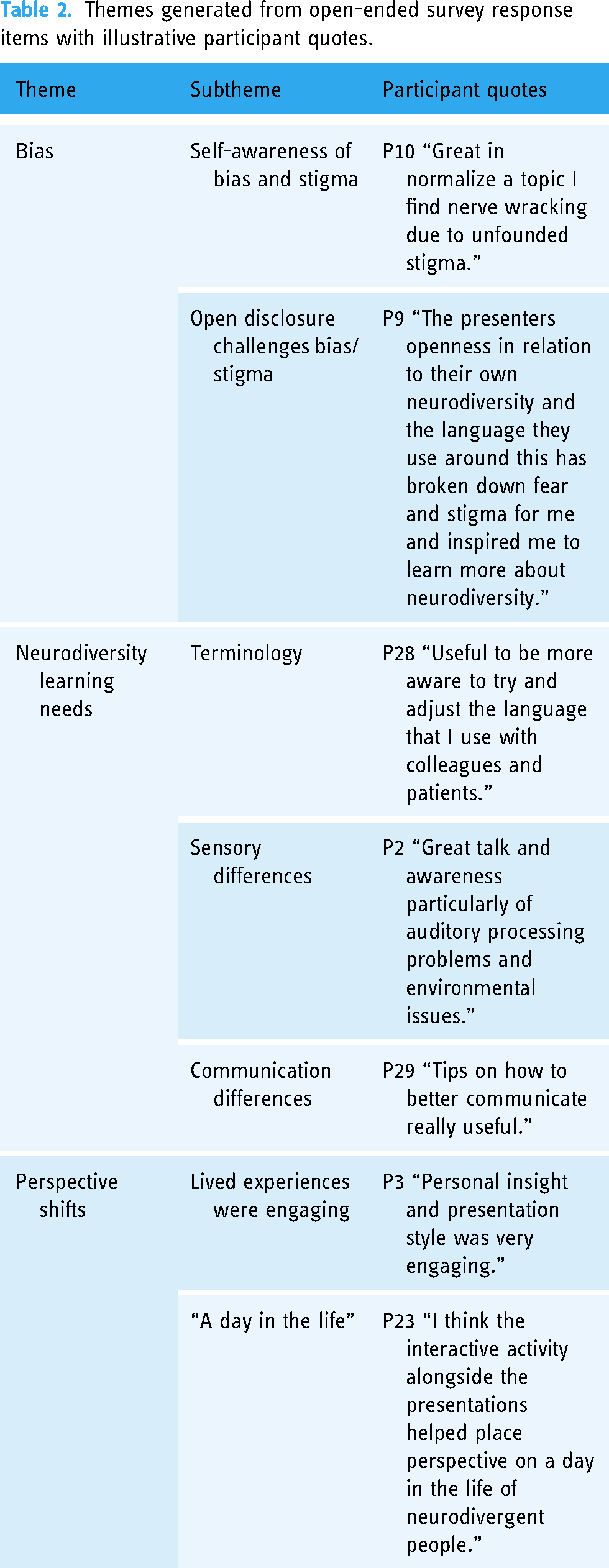
Changes in perspective and awareness of bias in relation to the topic of neurodiversity were evident, with participant 10 reporting the education initiative could “normalise” the topic of neurodiversity, and participant 9 reporting being challenged by the educators’ open disclosure of their neurodivergence, describing their “stigma” as “broken down” by the education experience. Two participants referred to the educator lived experiences, described as “personal insight,” that were shared by the educators, as particularly useful and engaging. Three participants reported the interactive activity in the final iteration of the neurodiversity education was particularly useful, with participant 23 reporting it complimented the didactic component of the education, and generated understanding of “a day in the life of neurodivergent people.”
Specific domains of neurodiversity education that were reported as particularly useful were from the didactic component of the education initiative. Five participants reported that information about neurodivergent peoples’ communication differences and communication supports was particularly useful, and four participants reported that general neurodiversity terminology was a particularly useful domain of education. No negative or adverse experiences were reported by participants in response to the question “Do you have any other feedback?” with six participants providing general positive statements such as “very helpful talk” (participant 22).
Discussion
This healthcare quality improvement study addressed the need for neurodiversity education among ED and Geriatric Medicine clinicians in a tertiary public hospital. Education priorities identified in the design process were negative attitudes, biases, and healthcare access barriers that contribute to autistic people's health inequity. The results of the change process described participant experiences of neurodiversity education in relation to their attitudes and beliefs about autistic people. To our knowledge, this study is the first in an Australian hospital to demonstrate neurodiversity education leading clinicians to report more confidence and acceptance towards autistic people.
The clinician attitude benefits seen in this study are in keeping with a growing body of research which shows autism education can improve knowledge and attitudes about autistic people, particularly when education programs are designed by autistic people (Ashworth et al., 2024; Gillespie-Lynch et al., 2022). In this study, the co-design process was neurodivergent-led, and the neurodiversity education was delivered by doctors who openly disclosed their neurodivergence to participants. This peer-led approach was similar to peer education used in other health professional education settings, in which consumers are involved in the design and delivery of education (Walsh et al., 2017). Peer education is effective at providing direct insight into healthcare experiences and can improve clinician attitudes, reducing stigma and enhancing empathy (Kang & Joung, 2020; Sreeram et al., 2024). Autism education research in non-healthcare settings has similarly shown that education delivered by people who openly disclose that they are autistic improves rapport, explicit biases, and social interest toward autistic people (Jones, DeBrabander, et al., 2021; Jones, Morrison, et al., 2021). Therefore it is not surprising that open disclosure of neurodivergence by peer-educators in this study was reported by participants to challenge their stigma and shift their perspectives toward a better understanding of neurodivergent experiences.
An alternative explanation for the clinician attitude benefits reported by survey respondents in this study is social desirability bias. Social desirability bias refers to the tendency to respond in a way that participants believe will be viewed favorably by others (Paulhus et al., 1991). It could be that the study leads’ relationship to participants as workplace peers introduced demand characteristics to the survey (Williamson, 2007). This refers to the possibility that participants self-edited their responses to portray themselves positively to the study leads, thus their responses were potentially incongruent with their true experiences. This possibility could be investigated in future tests of change, by introducing neurodivergent educators who are not known to participants and examining subsequent survey responses for differences arising as a result. If demand characteristics are determined likely to be present under conditions in which educators are known to participants, this could be investigated as a strategy to support the sustainability of change in future neurodiversity education quality improvement work. The influence of demand characteristics on the psychological environment of hospital workplaces might contribute to a workplace culture that is more insistent on inclusive clinician attitudes and behavior.
Engaging hospital education leaders as stakeholders in this study ensured neurodiversity education aligned with local workflow processes and addressed stakeholder priorities of improving the adherence of their departments with guideline recommendations and ensuring the education experience was relevant to the work and learning needs of their staff. The quality improvement team drew upon education leaders’ knowledge of participant learning preferences. This supported iterative adaptations to the neurodiversity education, to suit the preferences of different groups. Adaptations utilized approaches that have been successful in medical education contexts, including didactic presentations and team-based activities (T. Huang et al., 2024). Survey responses identified topics desired by participants for future neurodiversity education sessions in our hospital departments, offering direction for future research and quality improvement initiatives.
Conclusions
The healthcare improvement team, led by neurodivergent, disabled doctors, introduced neurodiversity education for clinicians in an Australian tertiary hospital as a change process aiming to improve adherence to guideline recommendations for supporting autistic people in healthcare settings (Trembath et al., 2022; Whaikaka, 2022). Participants reported more confidence and acceptance toward autistic people following neurodiversity education. Open disclosure of neurodivergence by peer educators was reported by participants to challenge their stigma and shift their perspectives toward a better understanding of neurodivergent experiences. Therefore, a lesson learned is that when doctors can disclose their neurodivergence and disability openly in the workplace, disclosure itself supports transformation toward inclusive, neurodiversity-affirming healthcare services. This highlights a need for healthcare service leadership teams to understand and remove barriers to workplace disclosure of neurodivergence and disability. Limitations of this study include the recruitment of participants from a single hospital site which may reduce generalizability of the findings and administering surveys at a single timepoint post-education which cannot assess changes in participant responses over time. Next steps will involve investigating the effectiveness, scalability, and transferability of this model in different healthcare settings and involving neurodivergent healthcare consumers, as well as providers, in future iterations to ensure their views and priorities are represented.
Supplemental Material
sj-docx-1-ndy-10.1177_27546330251317807 - Supplemental material for “After this presentation, I feel more confident caring for autistic patients”: The impact of neurodivergent doctors educating hospital staff about neurodiversity
Supplemental material, sj-docx-1-ndy-10.1177_27546330251317807 for “After this presentation, I feel more confident caring for autistic patients”: The impact of neurodivergent doctors educating hospital staff about neurodiversity by Sarah Bernard, Natalie Teasdale, Courtenay Harris and Sonya Girdler in Neurodiversity
Footnotes
Acknowledgments
The authors wish to thank the Sir Charles Gairdner Hospital Geriatric Acute and Rehabilitation Medicine Department staff and Emergency Department staff for their support of this study.
Authors’ contribution
SB: conceptualization, methodology, data collection, analysis and interpretation of results, and writing—original draft. NT: conceptualization, methodology, data collection, analysis and interpretation of results, writing—review and editing. CH and SG: methodology, analysis, and interpretation of results, writing—review and editing. All authors contributed equally to reviewing, editing, and approving the final manuscript.
Author Note
Sonya Girdler is also affiliated with Curtin Autism Research Group, School of Allied Health, Curtin University, Perth, WA, Australia and Center of Neurodevelopmental Disorders (KIND), Karolinska Institutet, Stockholm, Sweden.
Declaration of conflicting interests
The authors declare the following potential conflicts of interest with respect to the research, authorship, and publication of this article: SB and NT declare affiliation with Autistic Doctors International. SB declares employment and advisory roles with organizations that provide services and support to autistic people, and with disability advocacy organizations.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability
The dataset for this study is not publicly available as per the institutional Quality Improvement and Ethical Review process, which did not include permission for public data sharing. Requests to access the dataset can be directed to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
Appendix 1. Teaching Activity Feedback Survey
Strongly agree
Agree
Neither agree nor disagree
Disagree
Strongly disagree
Strongly agree
Agree
Neither agree nor disagree
Disagree
Strongly disagree
Strongly agree
Agree
Neither agree nor disagree
Disagree
Strongly disagree
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.