
Abstract
OBJECTIVES
Opioid overdose deaths remain a major health issue in the United States (US). As future physicians, medical students must receive comprehensive training to recognize and manage opioid overdoses. This study aimed to highlight training gaps at the medical student level and understand students’ attitudes toward patients with opioid use disorder (OUD).
METHODS
We assessed baseline knowledge of and attitudes toward the management of opioid overdoses and naloxone administration among medical students in the US. Two validated survey tools (Opioid Overdose Knowledge Scale and Opioid Overdose Attitude Scale) were administered to medical students training at accredited institutions along with supplemental questions measuring knowledge and attitudes towards opioid overdose management, naloxone administration, and prior training.
RESULTS
The final sample had N = 73 participants from US medical schools with a mean age of 25.3 (range of 22–37): 72.6% of respondents were female. Although most respondents reported personal/professional experience with OUD before medical school, they expressed interest in additional training. Knowledge surrounding opioid overdoses increased insignificantly over the 4 years of medical school. However, there was a significant increase in both perceived competence in overdose recognition/management and in concerns about intervening from the first to fourth year of medical school. Female respondents had significantly lower perceived competence and readiness to intervene sub-scores than male counterparts; however, there was no significant difference in overall attitude and knowledge scores when stratified by sex. Incorporating opioid overdose prevention training (OOPT) into early medical education was favorable among respondents, who expressed an overwhelming interest in learning and supporting patients with OUD.
CONCLUSIONS
Given the ongoing opioid crisis, medical students are ideally placed to identify and manage opioid overdoses. Medical students are ready to receive this training, thus strengthening the argument for OOPT integration into early medical student curricula.
Introduction
The Centers for Disease Control and Prevention reported more than 841,000 opioid-related deaths from 1999 to 2019. 1 In 2018, the United States (US) Surgeon General issued a public health advisory, encouraging all Americans to carry naloxone to be ready to respond to an opioid overdose. 2 Harm reduction measures, early recognition of opioid overdose, and readiness to intervene are critical to prevent morbidity and mortality.
Physicians play an important role in prescribing opioids, recognizing misuse, and preventing adverse events related to opioids. Despite their central role, healthcare professionals continue to report low knowledge and confidence surrounding the administration of the opioid antagonist naloxone, a critical tool for harm reduction in opioid use disorder (OUD).3–5 Current research suggests that barriers to opioid overdose recognition and naloxone use are not specific to attending physicians and affect graduate medical trainees as well.6,7 Discrepancies in the literature point to a disconnect between the perceived importance of opioid overdose prevention training (OOPT) and the actual integration of this topic into medical education.6–8
In recent years, multiple studies have highlighted promising results after implementing OOPT early in undergraduate medical training.6,9,10 To eliminate knowledge deficits among trainees and attendings and to encourage the prioritization of substance use education models in medical school curricula, many have advocated that OOPT programs should be implemented during early stages of medical student education. 5
Since 2013, the Opioid Overdose Knowledge Scale (OOKS) and Opioid Overdose Attitude Scale (OOAS) have been used to assess opioid-related knowledge and attitudes among healthcare providers and students. 11 These psychometric instruments were developed using data from two independent samples of family and friends of people who use heroin as well as healthcare professionals working in substance use treatment services in England. The original OOKS is a 45-item survey, and the OOAS is a 28-item survey grouped into three subscales: competence, concerns (about intervening), and readiness (willingness to intervene). These scales have since been validated by physicians, medical students, and pharmacists internationally. 11
In this study, we administered a modified OOKS and OOAS to first-, second-, third-, and fourth-year medical students training at accredited US institutions to measure knowledge and attitudes towards opioid overdose management and naloxone administration. The objectives of this study were to highlight training gaps at the medical student level and better understand student attitudes toward and perceptions of patients with OUD.
Materials and methods
Approval was obtained from the University of Massachusetts Chan Medical School Internal Review Board (IRB) and Students as Research Subjects (SAS) Ad Hoc Advisory Committee (Protocol: H00020732, approval date September 16, 2020). This was a cross-sectional study, and data were collected from September 30, 2020 to December 30, 2020. Data were collected from US-based subjects, and the study team was based in Worcester, Massachusetts. Study methods and results are reported according to guidelines set established in Consensus-Based Checklist for Reporting of Survey Studies (CROSS). 12
Survey adaptation and assessment
The study survey instrument was adapted from the standardized OOKS and OOAS, after obtaining approval from the creator of the tools and was adapted based on our research team's knowledge from previous studies and feedback obtained from content domain experts. 11 Twelve items from the original validated OOKS and 25 questions from the original validated OOAS were selected for use to avoid redundancy and two open-ended questions were added to better characterize medical student experiences with OUD and management. The survey was piloted on N = 10 individuals (five content matter experts and five medical students), and revised for clarity prior to deployment of the survey.
Participants
The study enrolled a convenience sample of first through fourth year medical students attending a four-year accredited allopathic or osteopathic program in the US. Exclusion criteria were as follows: individuals who were not able to read/write in English, and those unable or unwilling to provide consent. Participants were required to confirm attendance at a Liaison Committee on Medical Education (LCME) or Commission on Osteopathic College Accreditation (COCA) accredited four-year medical school by providing a school-issued email address.
The study was open to enrollment for a period of 90 days and advertisements were posted on social media platforms (ie, Facebook, Twitter, Instagram), student doctor forums (ie, Student Doctor Network), and local online student bulletin boards. Social media recruitment was leveraged to broaden the sample geographically while also maintaining a degree of anonymity (given the somewhat sensitive nature of the topic). The advertisement stated the participants would be answering a survey regarding OOPT in medical education. To incentivize participation, those who completed at least 50% of the survey were entered into a raffle for a $50 Amazon gift card.
Implementation of survey tool
Participants accessed the survey via a public link and subsequently read through an IRB-approved fact sheet to either accept (consent to) or decline study participation. Completion of the survey was considered as informed consent, which was approved by the IRB. Study data were collected and managed using Research Electronic Data Capture (REDCap), which is a secure, web-based software platform designed to support data capture for research studies.13,14 Participants were required to provide a unique, medical school issued email address (one not previously used in this study) to confirm student status and to prevent duplicate entries. Upon completion of the study (and after verification of eligibility by study staff) the data set was de-identified.
The study survey consisted of 4 sections: (1) demographics; (2) modified OOKS; (3) modified OOAS; and (4) open-ended questions (see Supplemental Material). The entire survey took approximately 20 min to complete.
Scoring of survey tool
The OOKS section was scored from 0 to 39, with higher scores reflecting greater knowledge on how to identify and appropriately intervene during an opioid overdose, including proper administration of naloxone. 11 OOKS questions were presented in one of three question structures: For “true or false” questions, response options included “true/false,” (+1 point if correct, + 0 points if incorrect) “I don’t know,” or “prefer not to answer” (both +0 points). Questions with one correct answer were converted to dichotomous responses of “correct” (+1 point) or “incorrect” (+0 points). For “select all that apply” questions, each correctly identified answer received 1 point, whereas incorrect answers received 0 points.
The OOAS section was scored from 0 to 125, with higher scores reflecting a more positive attitude towards intervening during an opioid overdose. 11 OOAS questions were presented on a Likert scale: reverse scoring was used for negatively worded items. Outcome measures for each participant who completed the OOAS section included four calculated scores: one total score and three sub-scores based on questions addressing areas of competence, readiness, and concern with respect to opioid overdose and management.
Two qualitative, open-ended questions regarding prior participant experience with opioid overdose recognition and/or management, naloxone training, or firsthand experience with OUD. Participants were encouraged to share their thoughts with the research team to better characterize medical student experiences with opioid overdose and OUD.
Statistical analysis
Descriptive statistics were calculated for demographic characteristics, specialty interest responses, and binary (yes/no) response questions related to opioid overdose education and/or training. Outcome measures of interest included both OOKS and OOAS total scores as well as OOAS sub-scores (competence, concern, readiness). Measures were then tabulated in the overall sample and stratified by sex and medical school year (MS1-4) to assess for subgroup differences. Stratification by other demographic variables (specifically age and geographic region) were not performed due to limited variability in the dataset. Hypothesis testing was performed to compare mean scores across respective categories: for normally distributed variables, Student’s t-test (binary variables) and ANOVA (greater than two groups) were used, and for non-normally distributed variables, Wilcoxon rank sum (binary variables) and Kruskal–Wallis H (greater than two groups) were used. Listwise deletion was applied in cases of missing data. All statistical analyses were performed using RStudio programming language software. 15
Thematic analysis was used to categorize and summarize open-ended survey data. Three independent reviewers read through all qualitative responses and generated a list of major themes. Researchers then met to review their findings, and three overarching themes were chosen to represent the data collected.
Results
Based on a final sample of 73 participants, the data is significant for differences in OOAS competence sub-scores when stratified for sex and overall OOAS score when stratified for academic year. Qualitative data showed marked interest by students to have OUD training as part of their undergraduate medical education despite majority of participants having prior exposure to individuals with OUD.
Study population
One hundred and forty five initial responses were received. Seventy-two entries were excluded due to failure to use a valid, unique school-sponsored email address and/or failure to complete >50% of the survey. The final sample consists of N = 73 participants from five US allopathic medical schools. Mean age of the sample was 25.3 years (SD = 2.0), and the sample 73% was female, making the study sample slightly older and more female than the general population of US medical students (mean age 24, 52% female).16,17 Demographic data are presented in Table 1.
Participant demographics

Abbreviations: MS1, first-year medical student; MS2, second-year medical student; MS3, third-year medical student; MS4, fourth-year medical student.
Each respondent could select
In terms of training/education history, 56.2% of respondents described previous formal training in opioid overdose education and/or naloxone administration. Training sites included community outreach and/or advocacy groups, school-sponsored initiatives, and emergency medical services. Additionally, 90.4% of respondents agreed that their home institution should have mandatory OOPT during the MS1 year. Most respondents (87.7%) felt that formal training on opioid overdose management/naloxone administration should be required for medical students, and 94.6% said they would be interested in attending a naloxone training session at their home institution. Twenty-four percent of students reported that their medical school required formal opioid overdose training as part of their current curriculum; 21% were unsure.
OOKS & OOAS scores
The mean total OOKS score for participants was 29.7 (on a scale of 0-39). Respondent scores were then stratified to compare knowledge levels across sex and medical school class year (Table 2), which yielded no significant differences (P = .583 and .179, respectively).
OOKS scores, by sex and by medical school class year.

Abbreviations: OOKS, Opioid Overdose Knowledge Scale; SD, standard deviation.
The mean overall OOAS score for participants was 94.9 (on a scale of 0-125). Mean competence, concerns, and readiness sub-scores were 21.6 (standard deviation [SD] = 5.5), 30.2 (SD = 3.8), and 43.2 (SD = 3.5), respectively (Table 3). When stratified by sex, significant differences in overall OOAS score (P = .010), and competence (P = .006) and readiness (P = .047) sub-scores were identified, which favored male respondents. No significant difference in concern sub-score (P = .214) was identified. When data were stratified by class year, statistically significant differences were identified among OOAS overall score (P = .005), as well as competence (P = .020) and concern (P = .019) sub-scores, with scores generally increasing from years 2 through 4. No significant difference in the readiness sub-score (P = .087) was identified when stratified by class year.
OOAS scores and sub-scores, by sex and by medical school class year.

Abbreviation: OOAS, Opioid Overdose Attitude Scale.
Statistical significance.
When stratified by history of prior training, participants who had attended a naloxone training session in the past scored significantly higher on the OOAS overall, OOAS competence and OOAS readiness, but not on the OOAS concerns subscore.
Open-ended questions: experiences and perceptions of opioid overdose & naloxone administration
Participants were asked to elaborate on any experiences they have had with opioid overdose prevention and/or OUD in the open-ended portion of the survey. In total, there were 31 respondents for this portion of the survey and 3 major themes were identified. Exemplar quotes for each theme are displayed in Table 4.
Illustrative quotes from open-ended question responses.
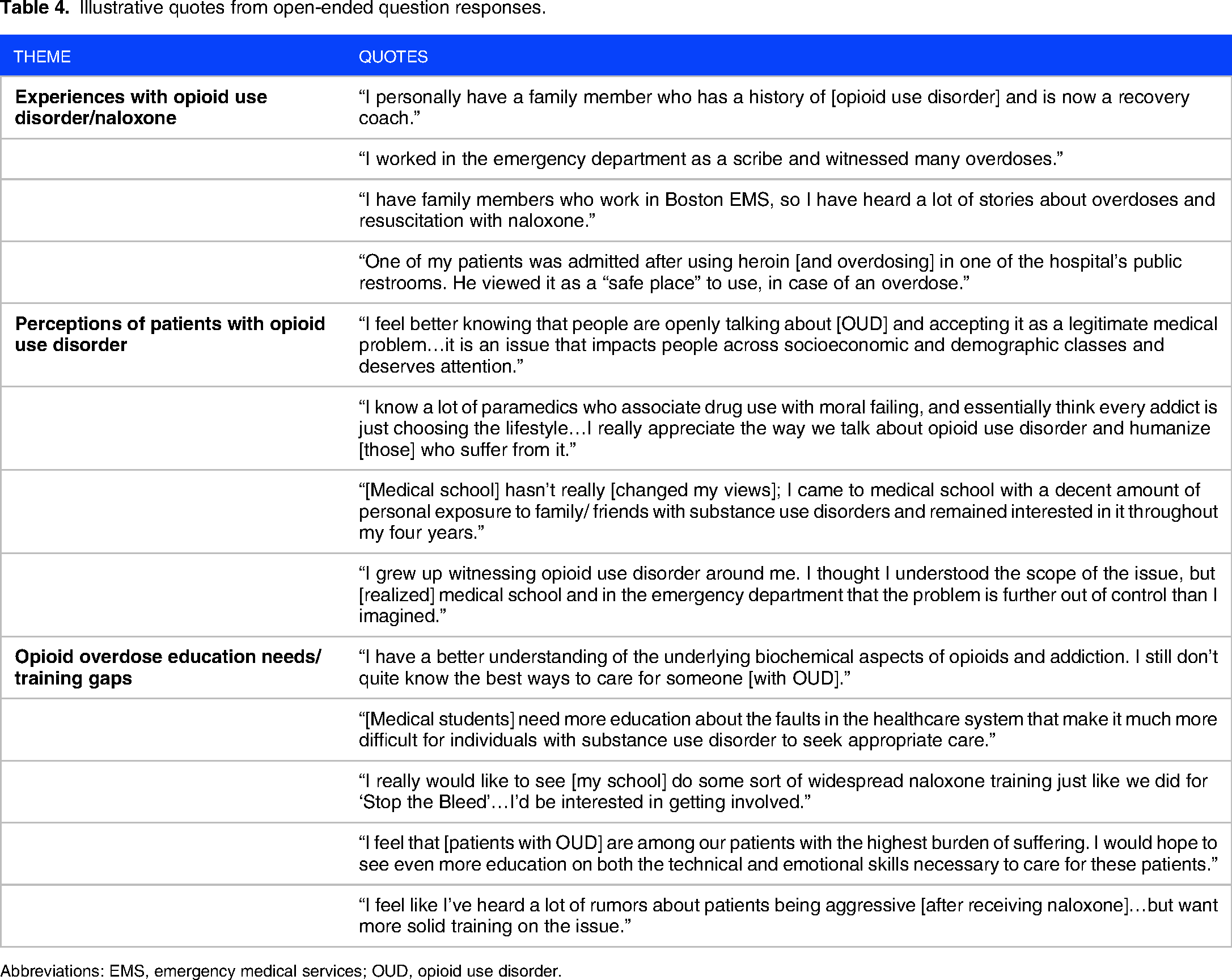
Abbreviations: EMS, emergency medical services; OUD, opioid use disorder.
Student experiences with opioid use disorder and/or naloxone use were far-reaching: Respondents highlighted pre-clinical training, clinical clerkships, and emergency medical services experience (ie, prior work as paramedic or emergency medical technician) as the primary healthcare-related settings where experiences with opioid overdose prevention and/or naloxone use took place. Many respondents also mentioned experiences with friends and/or family members who struggled with OUD.
Student perceptions of individuals with opioid use disorder varied over time: Participants were asked to describe their perceptions of individuals with OUD, and if/how these perceptions have changed during medical school. Responses varied and reflected positive, neutral, and negative perceptions; however, most were positive or neutral. Positive perceptions includes increasing empathy for patients with OUD after learning about the complications and barriers to care they face, and after gaining a better understanding of the physiology of substance use disorders as they progressed through medical school. Only one student reported increasingly negative perceptions of individuals with OUD but did not elaborate on contributing factors. Other students described no change in (neutral) perception over time and cited extensive personal experience with OUD and/or naloxone use through encounters with family and/or friends prior to medical school.
Students overwhelmingly expressed a desire to help patients with opioid use disorder and receive more education surrounding opioid overdose management and naloxone use: Another major theme highlighted among respondents was an interest in improving opioid overdose response/naloxone administration education at the medical student level. Nearly half of respondents expressed a desire to improve, expand, and/or participate in formal naloxone training programs at their respective institutions. This desire appears to be motivated by a number of factors, including but not limited to: uncertainty and frustration regarding the marginalization of patients with OUD, realization that the scope of the opioid epidemic is much larger than initially thought, and reflecting on individual interactions with patients. Most respondents agreed that medical education should focus more on humanistic aspects of treating OUD.
Discussion
Although most study respondents reported personal and/or professional experience with OUD prior to medical school, they expressed interest in (and desire for) additional training. In our sample, knowledge surrounding opioid overdose increased over the four years of medical school but not significantly. Attitudes surrounding opioid overdose did, however, change: there was a significant increase in both perceived competence and concerns about intervening from MS1 to MS4. The concept of incorporating OOPT into early medical school education was favorable among respondents, who expressed an overwhelming interest in both learning and supporting patients with OUD.
In terms of OOAS, total scores and competence and concern sub-scores increased by class year, suggesting that cumulative clinical experiences throughout medical school could lead to a higher degree of self-perceived competence and concern when responding to opioid overdoses. It is also important to consider respondents’ healthcare experiences prior to medical school (ie, via work, volunteering, shadowing). These experiences were often cited as drivers of attitudes and perceptions. While most students enter medical school with some exposure to the healthcare system, the type of experience will matter; for example, students who previously worked in emergency medical services are more likely to have particularly relevant experiences. While this study is not powered to detect these differences, it identifies an important population of potential allies when aiming to implement future OOPT in medical school training.
Female respondents having significantly lower overall OOAS scores and perceived competence sub-scores compared to male respondents is consistent with previous literature: the effects of sex and gender on medical student self-confidence have been documented for years.18–20 Given these findings, future work is needed to better understand specific factors that contribute to self-perceived competence when responding to and managing an opioid overdose.
Approximately half of the respondents endorsed prior formal opioid overdose education and/or naloxone training; yet an overwhelming majority expressed interest in attending a future training session. Although most participants expressed positive attitudes towards opioid overdose training, and caring for patients with OUD in general, a small subset (<10%), expressed negative/neutral perceptions commonly associated with stigma. The varied distribution of attitudes towards OUD suggests that limiting training to opioid overdose recognition and response education is not sufficient. Rather, incorporating implicit bias training into OOPT may be beneficial and necessary to improve medical trainee attitudes.
Limitations
As with all survey research, our study has some important limitations to be considered. This was a convenience sample, and thus may not have been powered to detect some differences between groups. Recruitment methods may also have led to selection bias as medical students that did not have accounts on social media/medical platforms may not have had the opportunity to participate. Additionally, the presence of response bias is worth considering. Since participants were asked to provide an official institutional email address to verify eligibility, it is possible that some may have been reluctant to provide survey answers or report attitudes perceived as socially undesirable. Alternatively, participants with a personal history related to opioid use may have been more likely to engage, and conversely people with less experience may have been less likely to respond, leading to non-response bias. Future research should aim to target a more comprehensive medical student demographic with institutional diversity (including osteopathic representation), as well as racial and ethnic diversity. 21
Conclusion
The overarching goal of OOPT programs is to provide effective, evidence-based training for healthcare professionals and students alike to prevent opioid overdoses. To achieve this goal, particular attention must be paid to participants’ knowledge and attitudes regarding opioid overdose management and naloxone administration. In this study, we used two existing, validated questionnaires intended to measure knowledge and assess attitudes about opioid overdose management and naloxone administration to understand these phenomena among medical students in the US. Given the ongoing opioid crisis, medical students are in an ideal position to identify and manage opioid overdoses as well as educate patients about harm reduction and treatment options. Our study provides evidence that medical schools can better prepare students to act, thus strengthening the argument for OOPT integration into first-year medical student curricula.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231225923 - Supplemental material for Opioid Overdose Recognition: A Survey of Perceived Preparedness and Desire for Curricular Integration Among Current US Medical Students
Supplemental material, sj-pdf-1-mde-10.1177_23821205231225923 for Opioid Overdose Recognition: A Survey of Perceived Preparedness and Desire for Curricular Integration Among Current US Medical Students by Lindsay Walsh, Brittany Chapman, Jennifer Carey, Kayla Loycano and Stephanie Carreiro in Journal of Medical Education and Curricular Development
Supplemental Material
sj-docx-2-mde-10.1177_23821205231225923 - Supplemental material for Opioid Overdose Recognition: A Survey of Perceived Preparedness and Desire for Curricular Integration Among Current US Medical Students
Supplemental material, sj-docx-2-mde-10.1177_23821205231225923 for Opioid Overdose Recognition: A Survey of Perceived Preparedness and Desire for Curricular Integration Among Current US Medical Students by Lindsay Walsh, Brittany Chapman, Jennifer Carey, Kayla Loycano and Stephanie Carreiro in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
We would like to thank Drs. Jeffrey Lai and Albert Conicella (University of Massachusetts Chan Medical School) for their valuable feedback during the survey development and piloting phases of the study. We would also like to thank the participating medical students for their time and valuable insights.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health, (grant number K23DA045242, PI: Carreiro).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.