
Abstract
OBJECTIVE
This study examines the perceptions of Lebanese medical students and graduates regarding the switch to electronic learning (e-learning) and measures their psychological distress amid the COVID-19 pandemic, compounded by an unprecedented financial collapse and the August 4 Beirut blast.
METHODS
This is a national cross-sectional descriptive study, consisting of a 48-item questionnaire, diffused online to Lebanese medical students between February 8 and 21, 2021. The survey divided into 5 sections assesses for (1) Sociodemographic information, (2) implemented changes in medical education delivery precipitated by the pandemic, (3) students’ perceptions regarding the effectiveness, advantages, and barriers of e-learning, and (4) role of e-learning in clinical training. Finally, students’ psychological distress was measured, using the Kessler 10-item distress scale (K10). Descriptive analyses were performed using Stata version 13 and Excel.
RESULTS
1060 responses were recorded (27% response rate) across all Lebanese medical schools. Although 71.6% of participants found e-learning to be stimulating, half of the participants thought it was not equally effective to face-to-face learning. Around 73.1% of students felt they were not able to learn hands-on clinical skills. Lebanese students identified cost savings (food, transportation etc) and poor internet connectivity are the most common advantage and barrier, respectively; 77.8% of participants showed high/very high levels of distress (K10 score ≥22).
CONCLUSIONS
Ensuring accessibility and availability of resources such as electricity and internet is of utmost priority. Lebanese medical schools need to incorporate clinical training experiences to their virtual platforms to maintain the quality of medical education to their students. A particular attention to students’ mental health is warranted, by increasing awareness and access to mental health services.
Introduction
Over the years, approaches to medical education have significantly changed, with a progressive shift from traditional classroom teaching to using innovative tools and technologies, to meet the students’ needs and expectations. From moving classrooms into public spaces such as museums or parks 1 to utilizing simulation training, 2 technology has been a technique to bridge the gap in medical education.
On March 11, 2020, the World Health Organization declared coronavirus disease 2019 (COVID-19) to be a pandemic disease, 3 which posed a serious challenge to the delivery of medical education and clinical training in the healthcare sector. Thus, there was a worldwide switch to electronic learning (e-learning) to deliver medical education, in order to reduce viral transmission. 4 This unprecedented pandemic has provided researchers and educators with the unique opportunity to evaluate the effectiveness of online teaching platforms and strategies in medical education. A systematic review done in 2019 highlighted that both offline and online learning have equivalent examination outcomes. 5 Drawbacks and challenges of medical online learning have also been documented. 4 Some of the challenges faced by students include loss of engagement with the loss of the face-to-face interaction, loss of assessments, and technology-related issues such as loss of confidentiality.6,7 The clinical exposure of medical students and graduates was found to be particularly limited in the setting of a highly contagious pandemic. In fact, many newly established policies, including the cancellation of elective surgeries and the transition to telemedicine have limited medical students’ hands-on clinical experience as part of their curricula. 8
Lebanon is a low-income middle eastern country, with a total surface area of 10 452 km2, hosting 6.9 million residents, 87.2% of whom live in urban areas, including 2 million refugees and 500 000 migrant workers. 9 Alongside the pandemic, the country has been going through one of its major socioeconomic crises due to hyperinflation and corruption. The Lebanese population was also subject to the biggest non-nuclear explosion in the world, in August 2020, leading to the destruction of the country's infrastructure and further economic decline and instability.10,11
Before the pandemic, e-learning has never been a part of formal education in Lebanon where most schools and universities were neither equipped nor experienced for this transition. Since the declaration of the first case of COVID-19 in Lebanon, the Lebanese Ministry of Education took quick and firm measures to close schools and universities early on, to prevent the disease spread. 12 During the lockdown, online teaching became the new norm in Lebanese academic settings, including medical schools.
To our knowledge, our study is the first to assess the perceptions of Lebanese students from all medical schools (public and private) regarding e-learning and measure their psychological distress. We believe that exploring the perceptions of medical students themselves regarding the benefits and challenges of e-learning will allow medical institutions to improve the quality of delivery of medical education in our country and other similar settings.
Materials and Methods
Questionnaire Design
This is a cross-sectional study conducted on a national level via an online survey. A 48-item questionnaire in English was devised following a literature search on currently used online teaching methods and the changes implemented to medical education following the pandemic, worldwide. This author-developed survey was adapted to the Lebanese context after piloting the questions among a group of 20 medical students belonging to public and private Lebanese universities (the survey sections and items are shown in Online Supplementary Appendix 1). Piloting improved the quality of the questions in terms of enhancing the language, adjusting the wording so that the context is better conveyed, and addressing redundancies. As shown in Appendix 1, the first 2 sections of the survey were I. the consent form with a box to be ticked by the consenting participant to be able to move forward with the survey and II. Sociodemographic information including gender, age, medical school, academic year, living condition, and location. Parts III to V tackled changes in medical education precipitated by the pandemic, students’ perceptions regarding the benefits and barriers of e-learning, and the role of e-learning in clinical training, respectively. The last section (VI) assessed the students’ psychological distress, using the 10-item Kessler distress scale (K10). Each of the 10 items is scored on a Likert scale going from 1 to 5 with 1 being none of the times and 5 being all of the times. 13 The scale total score ranges from 10 to 50. Scores of 10 to 15 correspond to low distress, scores of 16 to 21 correspond to moderate distress, whereas scores of 22 to 29 correspond to high psychological distress and finally scores of 30 to 50 correspond to very high distress. The categories of low and moderate distress were grouped and coded together as 0, while categories of high and very high distress were grouped and coded together as 1, in the statistical analysis.
Participants
All 3878 graduate medical students or past year graduated medical doctors from 7 registered Lebanese medical schools were eligible to participate. There were no exclusion criteria.
Questionnaire Distribution
The survey was created using Google Forms, an online survey software, and disseminated to Lebanese medical students via emails through their official institutions as well as social media platforms. There was an outreach to all the 7 registered medical schools in Lebanon, by involving the deans of medical schools, as well as students’ representatives of each class in each medical school to increase rate of participation. The survey was accessible via an anonymous link and open for a 2-week period (February 8-21, 2021).
Consent and Ethical Considerations
Participation was voluntary, and participants were informed prior to starting the survey that all data collected was nonidentifiable and only used for research purposes. A mandatory selection box consenting to participation and confirming that this was the first time completing this survey was included at the beginning of the survey to avoid duplicate answers, while preserving anonymity.
The study was conducted according to the ethical principles stated in the Declaration of Helsinki (2013). It was approved by the Institutional Review Board (IRB) at the University of Balamand and St. Georges Hospital University Medical Center, Beirut, Lebanon (IRB-REC/O/001-21/4420).
Statistical Analysis
Data was exported from Google form to Stata version 13 and Microsoft Excel (Excel V.16.29, 2019). Descriptive analyses involve description of data in terms of frequencies, percentages, means, and standard deviation. Measurement of these statistics depend on the variables either to be categorical or continuous in nature. Accordingly, frequencies and percentages were generated for categorical variables and means and standard deviations for continuous variables (only one variable).
Results
Population Sample
Out of a total of 1060 responses recorded (27% response rate) across all Lebanese medical schools, 60.8% (n = 645) are female respondents and the mean age is 22.25 ± 2.82 years. The majority, 82% (n = 870), are current students, and 18% are past year graduates. Around two-thirds of participants live in the capital, Beirut, and its suburbs, and 87% (n = 925) live with their families. The full set of sociodemographic data is shown in Table 1.
Sociodemographic Characteristics of Participants (n = 1060).

Mean ± standard deviation is mentioned for continuous variables.
Delivery of Medical Education During the COVID-19 Pandemic
Pre-COVID-19 pandemic
Participants mostly engaged in 1 to 3 e-learning platform resources: around two-thirds of responders used video tutorials explaining concepts available on YouTube or provided by trusted resources such as Kaplan etc. Around 50% used Question banks (Kaplan and Uworld) in preparation for their exams. Only 20% (215 responders) reported using video tutorials provided by their medical schools. Out of all participants, 61% spent less than 9 h/week using e-learning methods. Only 9% spent more than 25 h studying online (Figure 1). Most participants, 96% (n = 1026), believed that question banks were the most effective e-learning method.
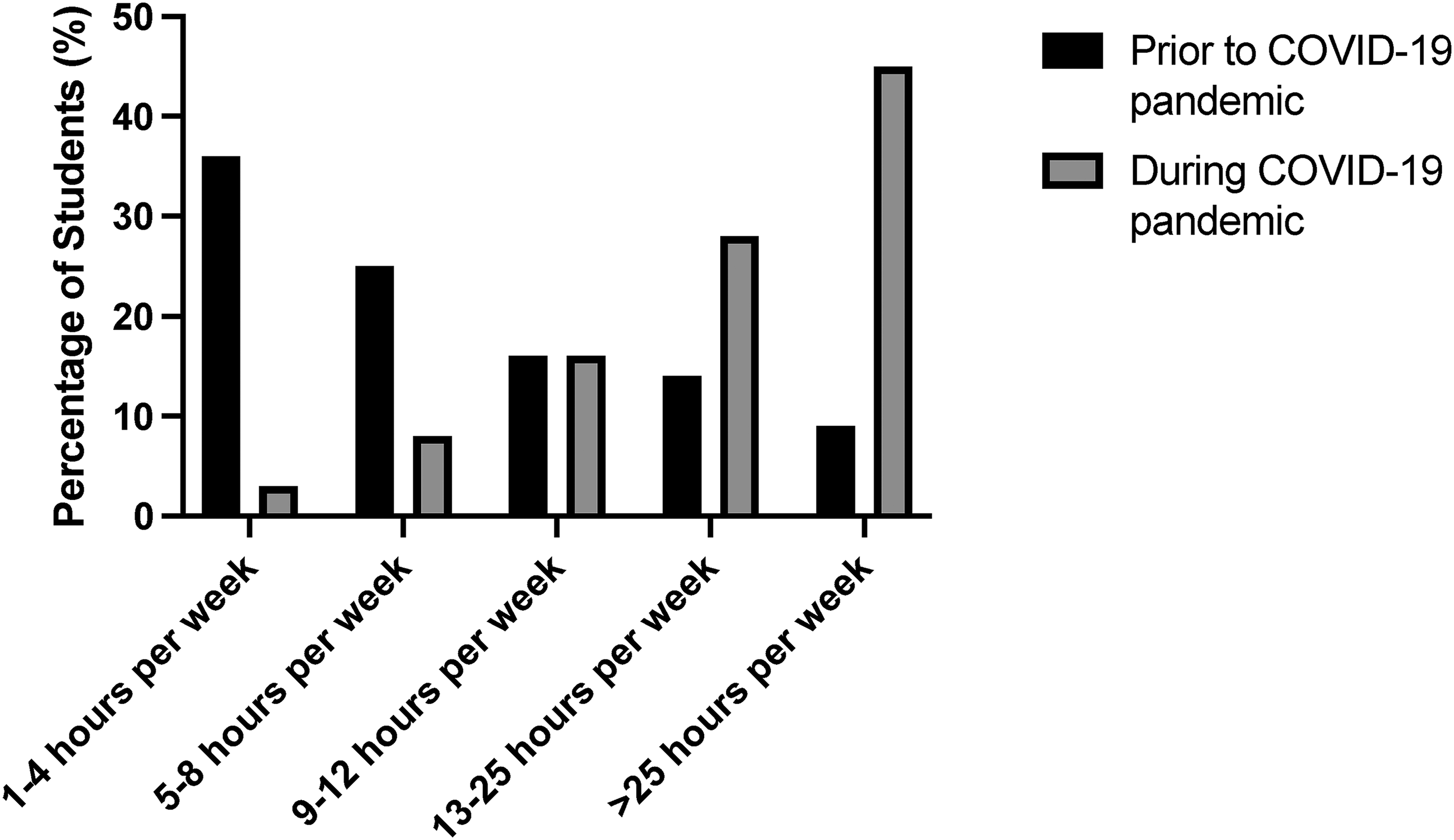
Average time spent using e-learning methods for studying before and after the COVID-19 pandemic.
Post-COVID-19 pandemic
Within the pandemic context and the switch to exclusive e-learning, around 45% of participants spend more than 25 h per week studying online, and 27.7% spend between 13 and 25 h/week. Students use 1 to 2 devices (94% use laptops, 63.5% use their phones, and only 30% use their tablets). Furthermore, 73% of responders report that their medical school followed a preset curriculum. Considerably 92.3% (n = 978) report their school delivered live talks/lectures using platforms such as WebEx and Zoom, and 66.7% (n = 706) report they were taught using prerecorded material.
Most or all sessions were found to be interactive by 56.1% (n = 593) of participants.
Instructors were reported to be responsive and available for students after the online sessions by 84% (n = 884) of participants.
A total of 73.7% of participants (n = 781) report their exams were held in person. Around 20% (n = 209) report that the number of evaluations was reduced compared to previous years.
Perceptions Regarding the Effectiveness, Advantages, and Barriers of E-Learning
Out of all participants, 71.6% (n = 715) find the online teaching to be stimulating, and 58.5% (n = 586) find it was easy to engage in the lessons. Around two-thirds of the medical students feel able to ask questions and enjoy the online teaching. However, half of them did not find the online teaching to be equally effective to the face-face teaching and favored the latter over the former. Around 72% (n = 727) think that the instructors were well prepared for the teaching sessions, and 66.1% (n = 677) believe that the instructors knew how to handle the technological devices and platforms. Nevertheless, around 93% (n = 980) think that instructors may benefit from a special training to improve the e-learning experience.
Last, concerning hands-on clinical training, 80% of students feel that e-learning has not successfully replaced the clinical teaching they received from direct patient contact and 73.1% (n = 765) feel they were not able to learn practical clinical skills through e-learning. Around 60.2% (n = 603) believe they may have lost an academic year of their medical journey. Only 2.7% (n = 28) of participants wish to continue exclusive online learning after the pandemic is under control. Around 45.2% (n = 477) of participants wish to return to exclusive face to face classes.
Figure 2 describes the advantages and disadvantages of e-learning compared to face-to-face learning as perceived by the Lebanese students.

Advantages and disadvantages of e-learning versus face-to-face learning.
Stressors and Psychological Distress
When assessing the different possible stressors that had an impact on the medical students’ learning experience and performance, students reported that the pandemic, deteriorating socioeconomic and political situations, in addition to the Beirut August 4, 2020, blast to be major stressors (Figure 3). More than two-thirds of participants (77.85%; n = 791) show a high/very high levels of distress (score ≥22), as demonstrated by the K10 distress scale.

The perceived impact of different stressors on the engagement and performance of Lebanese students in their medical education.
Discussion
Our study demonstrated that many students had relied on e-learning strategies prior to the pandemic, however, there was a noticeable yet anticipated increase in the time spent using e-learning methods during the COVID-19 pandemic by most students, as shown in Figure 1. Most Lebanese medical students found online learning to be flexible, cost-effective, time-saving, stimulating, and enjoyable. At least half of the students found e-learning methods to be as effective and impactful on their future career as in-person teaching. Perceptions of medical students regarding e-learning have been explored in a neighboring Arab country, Saudi Arabia, prior and during the pandemic (in 2017 and 2019). 14 These results are in agreement with findings from Al-Balas et al who demonstrated that around 80% of Jordanian medical students reported improvement in accessibility and time management/saving after the establishment of distant learning during the pandemic. 15 This teaching modality grants a personalized learning experience, allowing the medical student to have greater control over the educational content as well as the sequence and the timing of the learning sessions.16–18
In terms of barriers, almost 80% of the Lebanese students complain of poor internet connectivity. Electricity outage is the second most reported concern. Our findings are comparable to data from other low to middle income countries in the Arab region and the world.
In a systematic review and meta-analysis done in Brazil, 4 main categories of barriers to the implementation of online learning were identified. These included lack of planning and implementation of online learning, lack of resources, technology usability problems, and limited interaction between teachers and students. 19 The first 3 barriers were clearly identified in the Lebanese setting. Similar challenges related to poor resources were found in under developed countries such as Afghanistan, 20 Pakistan, 21 and Sri Lanka. 21
Lebanon's infrastructure has been without any maintenance since the civil war in 1975. The country's subsequent governments have also failed to address the power outages or find a sustainable short or long-term solution. Poor internet connection can also be related to the country's deprived infrastructure. These concerns are thus the main barriers to be quickly addressed to improve the e-learning experience in Lebanon.
Limitation of interaction with peers and teachers virtually is inconsistently reported in the literature: while this was a concern reported by medical students in Brazil, 22 Saudi Arabia, 23 and Greece, 24 preserved or improved interactions with peers and instructors were reported to a certain extent in our study as well as other countries like Jordan. 15
While the preclinical phase of medical curricula was somewhat “successfully” replaced by the novel culture of “online home learning,” the lack of hands-on training may have serious implications on the quality of training of the current cohort of students, which was a clear concern raised by Lebanese students and past year graduates. 25 Implementation of virtual simulation platforms and increasing students’ exposure/attendance of telehealth visits/rounds are 2 plausible solutions for students who are in the final stages of their medical education. These methods were successfully adopted in several medical schools around the world. For example, an innovative design of a virtual video-based medical student elective in the department of head and neck surgery at the university of Pennsylvania has been very successful in accomplishing the main goals of students’ exposure to the specialty and engagement with the faculty. 26 Didactic meetings including morning reports, seminars, and departmental grand rounds have also been converted into online video conferences in multiple medical faculties throughout the world.27–31 In addition, to better simulate clinical teaching, some medical schools established online virtual patient encounters and case-based learning tutorials.30,32 For example, Chandra and colleagues at Thomas Jefferson University Hospitals have organized a virtual emergency medicine rotation where medical students conducted virtual follow-up visits with patients that have been in the emergency department in the past 48 h. 33 The encounters are directly supervised by the attendings allowing the students to get rapid direct faculty feedback. 33 These innovative techniques are encouraged to be used regularly in all medical schools across the country.
On a psychological level, more than two-thirds of participants have been experiencing high to very high levels of distress. These results were concordant with a similar study conducted at the American University of Beirut, Lebanon that showed 69% of medical students (n = 374) are experiencing moderate to severe psychological distress during the pandemic, using the 10-item Perceived Stress Scale and the 4-item Patient Health Questionnaire for Depression and Anxiety. 34 Al Tammemi et al reported similar findings in Jordanian medical students (n = 381), with around 69.5% (n = 265) having experienced severe distress during the pandemic, using the same K10 scale. 35
High levels of distress in medical students are usually multifactorial and may have been already present, to a certain extent, before the start of the pandemic. In fact, fear of examinations, high educational fees, parental expectations, peer pressure, burnout, lack of leisure time and the continuous need for higher education are all psychological stressors that can negatively impact the social and psychological well-being of medical students.36,37 In 2016, a study by Talih and colleagues has shown that up to 43% of Lebanese medical students were experiencing burnout, with around 24% reporting depressive symptomatology and 14.5% having suicidal ideations. 38 The COVID-19 pandemic has exacerbated mental health problems, by exposing a wide array of new constraints that negatively impact the psychological status of medical students. To start with, medical students had significant concerns about their graduation and the real effectiveness of the delivery of medical education. In addition, while most people were able to self-isolate together with their family members who were all working from home, medical students were pressured to self-isolate alone given their high risk of exposure.
On the other hand, Lebanese medical students experienced unique additional stressors that further impacted their psychological well-being. Unfortunately, the country has been experiencing a severe political and financial crisis that significantly impacted their ability to afford their medical education, as well as their leisure activities that used to relieve their distress. In addition, the Beirut blast was a major traumatic event during which Lebanese medical students witnessed the destruction of their city, homes, and university hospitals as well as the injury or death of colleagues, neighbors, and family members. High levels of depressive, anxiety, and post-traumatic stress disorder symptoms were shown to be reflected by the K10 scale. 39
Finally, our study is not without any limitations. Despite a good response rate of 27% yielding a large sample size of 1060 responses, this study included a convenience sample, with no prior determination of a sample size. It is also possible that those who chose to respond to the survey were different from those who did not respond causing selection bias. Moreover, like face-to-face interviews, the participants may understand and interpret the questions differently, which makes it difficult to correctly assess the accuracy of the responses. In addition, except for the K10 psychological distress scale, the survey's different questions were devised then piloted by the authors, in the absence of prior validation study. Furthermore, the K10 questionnaire is a simple screening tool. Although it gives cutoff scores that can be correlated to clinical severity, the actual diagnosis of depressive and anxiety disorders must be done using a clinical diagnostic tool administered by a clinician. The ten-item (K10) and 6-item (K6) versions of the Kessler Psychological Distress Scale were translated to Arabic and tested for their reliability and validity in the Palestinian population. 40 These versions were not however studied in the Lebanese population. The English version was used in our survey given that it is an official language used in teaching medical schools. Finally, our study included only Lebanese medical students. Thus, our results are not necessarily representative of the perspectives of other Lebanese college students in other academic fields, or medical students from surrounding countries.
Conclusion
The rapid transition to e-learning forced during the pandemic created many challenges for medical students and instructors in low to middle income countries. Lessons learned from Lebanese students include the need for further preparation and training among instructors, in addition to increased accessibility and availability of resources such as electricity and internet for an improved e-learning experience. Further incorporation of clinical training experiences within the e-learning strategy is needed. It is recommended to combine live and virtual learning for more effective outcomes, as perceived by students. Most importantly, medical schools, notably in Lebanon, are recommended to give a particular attention to their students’ mental health, in these unprecedented times. Awareness campaigns to students regarding psychological distress, depression, anxiety, and suicide are highly needed. In addition, virtual psychological services should be made easily accessible to all students.
While this work mainly focuses on the early period of the pandemic, future work should investigate how students adapted to e-learning strategies away from the immediate threat of the pandemic, in addition to studying the perceptions and psychological distress of the instructors and clinicians providing medical education and training themselves. A multidisciplinary work involving students, instructors, policy makers, and governmental entities is encouraged to develop strategies aiming at enhancing the medical e-learning experience and mitigating mental health disorders in the face of global crises.
Supplemental Material
sj-docx-1-mde-10.1177_23821205231209106 - Supplemental material for Insights of Medical Students and Graduates Toward Electronic Learning During the COVID-19 Pandemic in Lebanon: A National Cross-Sectional Study
Supplemental material, sj-docx-1-mde-10.1177_23821205231209106 for Insights of Medical Students and Graduates Toward Electronic Learning During the COVID-19 Pandemic in Lebanon: A National Cross-Sectional Study by Maroun Bou Zerdan, Youssef Bouferraa, Morgan Bou Zerdan, Josleen Al Barathie and Rita Khoury in Journal of Medical Education and Curricular Development
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.