
Abstract
Objectives
We explored medical students’ perspectives on and experiences of e-learning in Gaza and proposed relevant policy recommendations.
Methods
We administered an online questionnaire to medical students in Gaza exploring (1) demographics, computer skills, and time spent on e-learning; (2) students’ perception and challenges of e-learning; and (3) students’ preferences of continuing medical e-learning in the future. Analysis was done using SPSS version 23.
Results
Out of 1830 students invited, 470 responded, and 227 of them were basic-level students. More female students responded (58.3%, n = 256). Most participants (n = 413, 87.9%) reported moderate to high computer skills allowing them to access e-learning. Before coronavirus disease-19 (COVID-19), over two-thirds (n = 321, 68.3%) spent 0-3 hours on e-learning. After COVID-19, the majority shifted, and 306 students (65.1%) reported spending at least 7 hours on various e-learning sources. The challenges for clinical-level students were mainly related to lack of practical training in the hospital (n = 196, 80%), followed by lack of interactions with real patients (n = 167, 68.7%). As for basic-level students, a majority (n = 120, 52.8%) reported lack of practical skills (eg, lab skills) as a challenge followed by unreliable internet access (n = 119, 52.4%). Pre-recoded lectures, readily available educational videos were used more than live lectures. Less than a third of all students (n = 147, 31.3%) wanted e-learning in the next term.
Conclusions
Medical students in Gaza don’t have a favourable experience with online medical education. There need to be actions to help overcome the challenges faced by students. This requires orchestrated actions by the government, universities, and local and international organizations.
Introduction
In December 2019, a new variant of Coronavirus was detected in patients with pneumonia in Wuhan, China. 1 The diseases it causes, coronavirus disease-19 (COVID-19), was declared a pandemic by the World Health Organization (WHO) on March 11th, 2020. 2 In response, international and national strategic plans were urgently taken and implemented to mitigate its consequences and prevent further losses. Since then, almost all countries around the world have experienced uncontrolled outbreaks with thousands of losses in lives.
The occupied Palestinian territories (oPt) comprise the West Bank and the Gaza Strip, which are geographically separated from each other. In the Gaza Strip, the first cases were confirmed on March 22nd in two Palestinians who returned from Pakistan, and community spread occurred on August 25th, when a full lockdown was imposed. 3 The ensuing state of emergency mandated the closure of educational facilities, including medical schools, and the suspension of face-to-face educational activities. As a result, e-learning was adopted as the new method of teaching in light of the public health measures and restrictions.
Similarly, educational authorities in nearly all countries have stopped face-to-face teaching, and the education of at least one billion students around the world has been interrupted. 4 Medical education has a peculiarity in that it requires close interaction with patients and doctors. The educational activities are conducted in hospitals or in schools that are attached to hospitals, which poses a significant risk to further spread the infection in the community. Therefore, transitioning to e-learning became a necessity. Technology has provided a valuable alternative to face-to-face teaching activities by delivering high-standard educational material online. Many institutions around the world have taken interest in how to better present educational content online, engage teachers, and conduct assessments.
Although online learning has been used before to deliver education and teaching activities, this is the first-time educational organizations in oPt have to deliver all of their activities and programs completely online. As the pandemic is still ongoing and educational institutions incorporate e-learning into the ‘new normal’, 5 there is a need to understand the perspectives of the students regarding online learning, the barriers and challenges of it, and the potential of incorporating it into traditional education in the future. This study seeks to understand those aspects in a special context, that of protracted conflict and blockade in the Gaza Strip.
Methods
This was a cross-sectional, descriptive study conducted to explore medical students’ opinions on and experiences of e-learning amid COVID-19 in the Gaza Strip. An online, self-administered Google form was created, and pretested on 10 students, and then students were invited to respond to the questionnaire. The questionnaire was open for a period of ten days in the end of December 2020 and start of January 2021. All medical students in the Gaza Strip, from first to sixth year from both medical schools in Gaza – the Islamic and Al Azhar universities – were eligible to take part in the study and were invited to participate. Any medical students, including Palestinian ones, outside of the Gaza Strip were excluded and thus not invited to take part. A description of the study, including its aims and objectives, was included in the beginning of the questionnaire. We considered answering the questionnaire and submitting the answers as consent to be part of the study. Ethical approval for the study was obtained from the Helsinki Committee within the Palestinian Health Research Council (PHCR/HC/971/21).
The online questionnaire (Supplement 1) was composed of three sections. The first section included information about demographics, computer skills, time spent on e-learning before and after COVID-19, and the most commonly used online platforms. After discussion, we decided to free the participants from any rigid criteria or classification for Information Technology (IT) skills and leave it up to each participant to decide their Information Technology (IT) skills that are sufficient to access the online resources they need. The second section utilized three Likert-scale 6 questions to explore students’ perception, method effectiveness, and main challenges of e-learning. The third section of the questionnaire explored advantages and disadvantages of e-learning. The last question explored students’ preference towards continuing medical education virtually for next semester. The analysis of data was done by using the Statistical Package for the Social Sciences (SPSS) version 23 statistical software. We primarily used descriptive statistics to report students’ responses, and we compared between basic-level students (those in their first, second, and third year) and clinical-level students (those in their fourth, fifth, and sixth year).
The study generally follows the SQUIRE-EDU publication guidelines for education improvement. 7 We opted for adding an additional section to offer policy recommendations based on the findings of the study. These actionable recommendations offer ways forwards to provide better and more effective delivery of online medical education in the Gaza Strip as well as similar contexts of prolonged conflict and occupation.
Results
The population eligible to answer the questionnaire and participate in the study were 1830 students. We calculated the sample size needed to run statistical analysis and have significant findings based on a confidence level of 98% and a 5% margin of error, which yields a sample size of 419. In our study, a total of 470 students responded, which is higher than the required sample size, yielding a response rate of 25.7%. Forty-eight percent (n = 227) of respondents were basic-level students and 243 were clinical-level students. The mean age of basic-level students was 18.8 (±1.05) and that of clinical students was 22.1 (±1). There were more female respondents (58.3%, n = 256) than males.
Table 1 shows the self-reported computer skills proficiency of the students as well as the time they spent on e-learning before and after COVID-19 and the most commonly used platforms they utilize. Computer skills included proficiency in using online educational platforms and computer programs such Microsoft Office Word and PowerPoint. Most participants (n = 413, 87.9%) reported having moderate or high IT skills allowing them to access e-learning easily. Computer skills were significantly higher (P = .047) among clinical students as 222 (91.4%) of them reported moderate or high computer skills compared with 191 (70%) among basic-level students.
Participants’ responses to their perceived IT skills, hours they spent on e-learning before and after COVID-19, and the most common platforms they use after COVID-19. More than 1 answer was allowed for the platforms question.
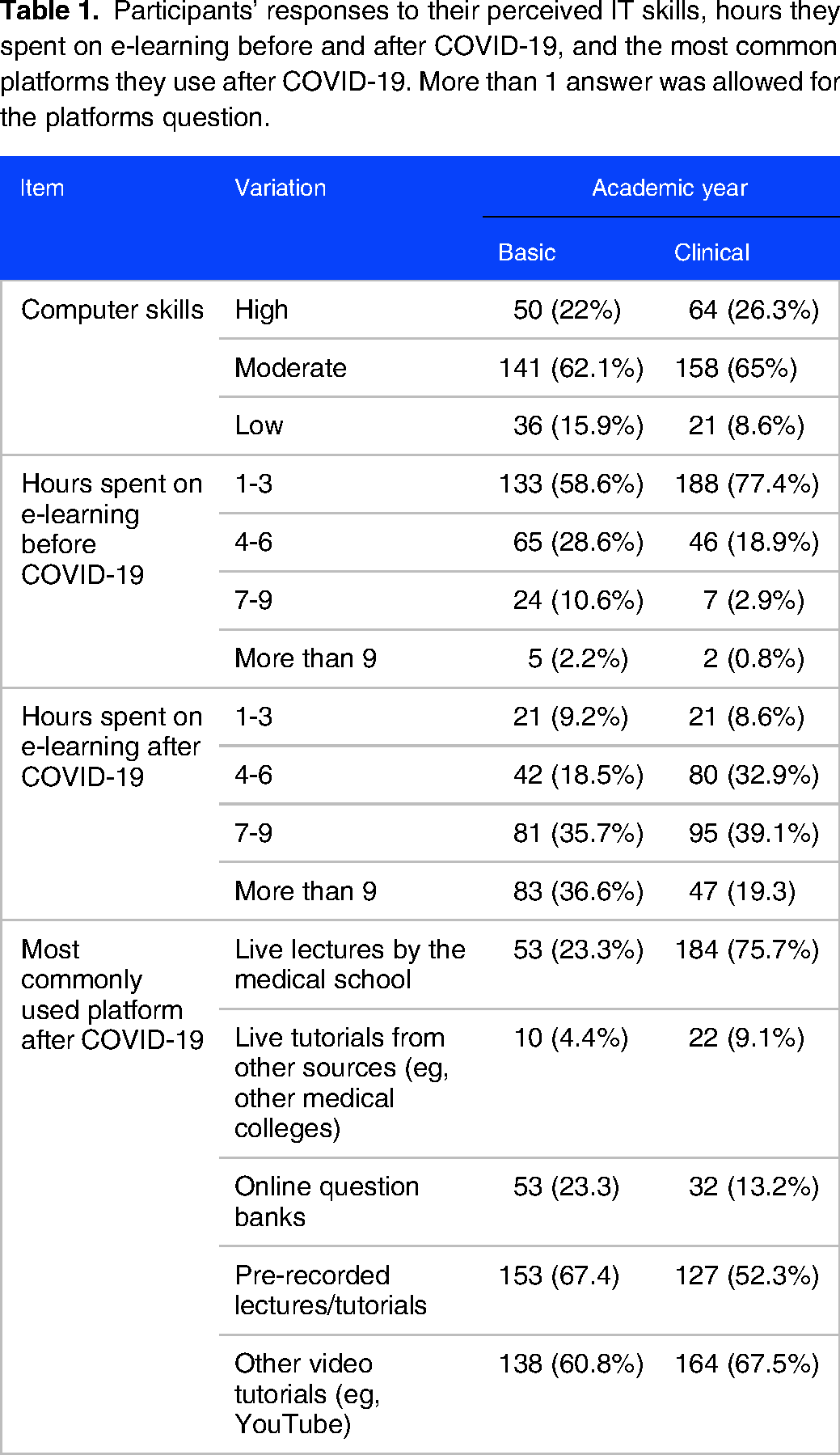
Prior to the pandemic, students used to complement their traditional studies with independent use of online educational platforms such as pre-recorded videos, UpToDate, YouTube, and other online resources. Before COVID-19, the majority of students (n = 321, 68.3%) spent three hours or less on e-learning. This changed after COVID-19 as students started spending many more hours on e-learning. As both Islamic and Al Azhar universities shifted to e-learning, 306 students (65.1%) reported spending at least 7 h on e-learning, whereas only 42 students (8.9%) reported spending 3 h or less. More students used pre-recoded lectures, readily available educational videos (eg, YouTube) than live lectures by their medical school. More clinical-level students (n = 175) used multiple online platforms than basic-level students (n = 123).
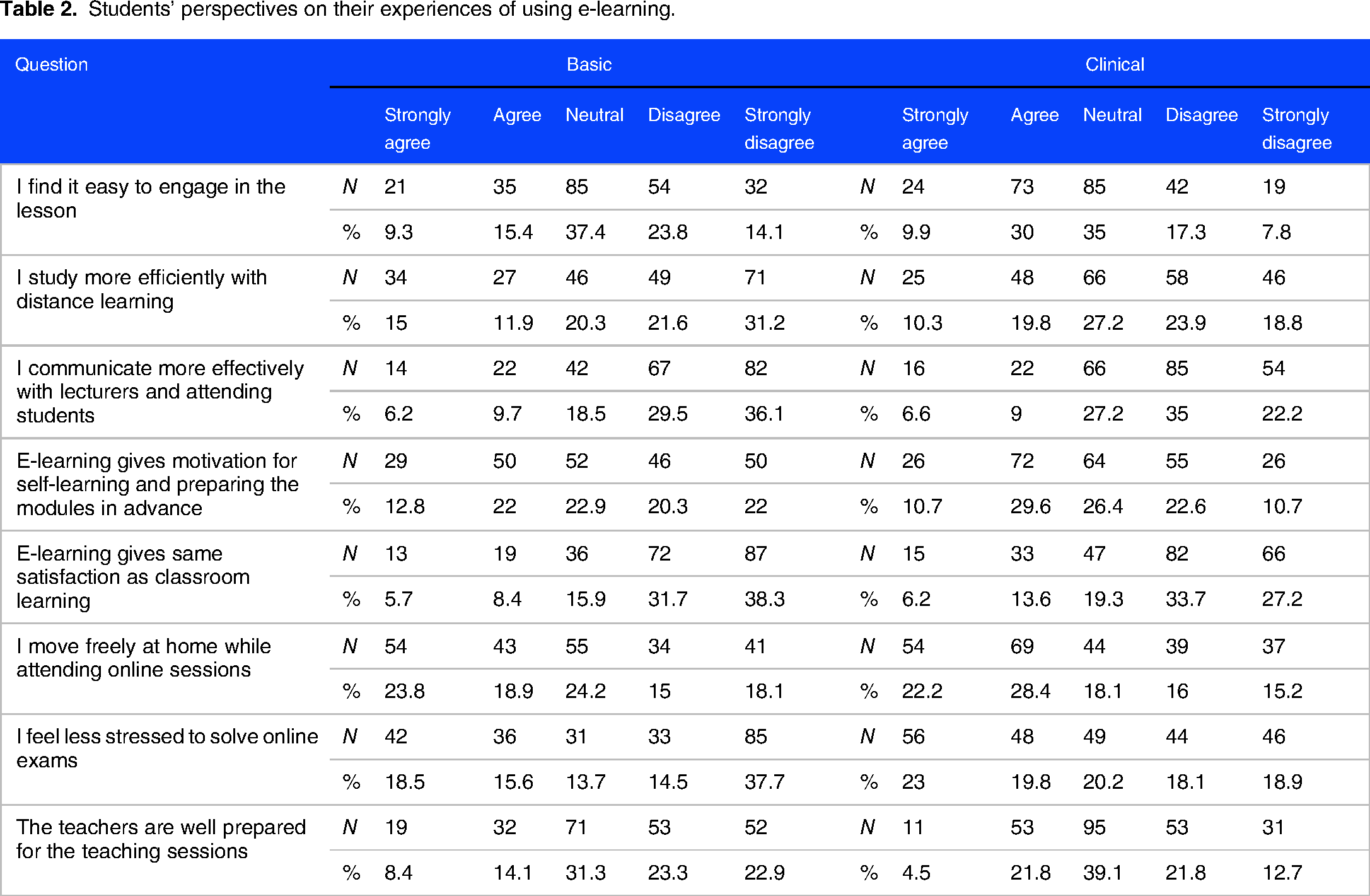
Students’ perspectives and experiences of using e-learning modalities and platforms as a main part of their medical education is reported in Table 2. Clinical students reported feeling less stressed doing online exams than their peers in basic years (43% vs 34%) and reported feeling more capable of engaging in any online lesson (40% vs 25%). Over half of students (n = 288, 61%) reported that interactive communication with lecturers online is difficult and they found themselves less motivated to prepare lessons in advance which might lessen the desired maximum benefits from lessons. Two-thirds of basic-level students (n = 159, 70%) and (n = 148, 60.9%) of clinical students reported being more satisfied with classroom learning than e-learning, although they have the possibility of moving freely at home during online classes. Overall, clinical-level students were more flexible to positively accept online learning to be part of their medical education than their counterparts in basic levels.
Students’ perspectives on their experiences of using e-learning.
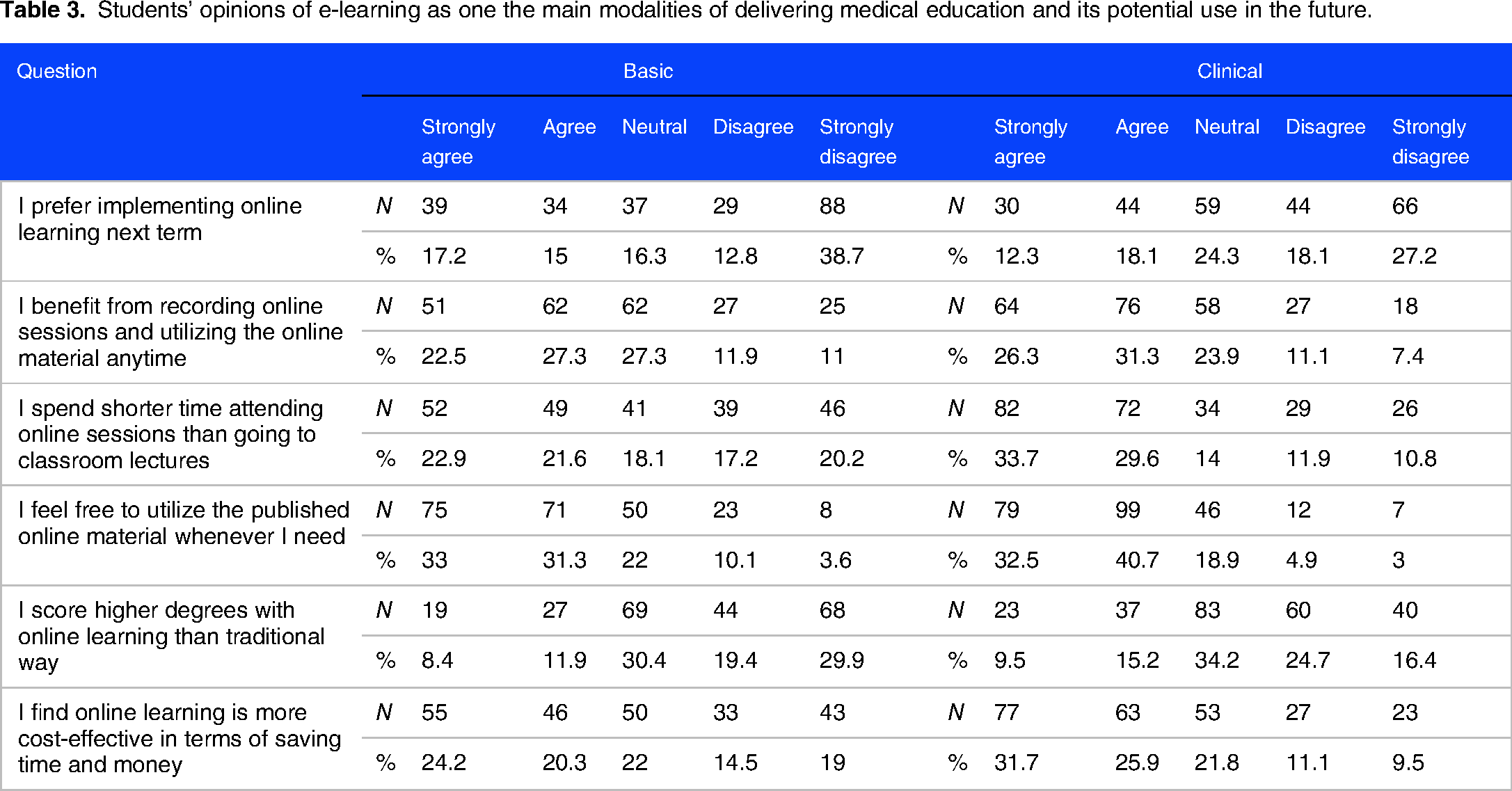
As shown in Table 3, less than a third of all students (n = 147, 31.3%) reported preference to have e-learning in the next term. This could potentially be explained by more students disagreeing or strongly disagreeing (n = 212, 45.1%) that they score higher grades with online learning compared with conventional education than ones agreeing or strongly agreeing (n = 106, 22.6%) with the statement. Moreover, as students used e-learning resources prior to the pandemic, more seemed to prefer and use material that is either recorded or readily published as they can access it based on their own pace and time. Furthermore, e-learning was notably more cost-effective to over half of all students (n = 241, 51.3%). Given the bad socioeconomic situation in Gaza, this point is an important one to be considered when formulating health education policies.
Students’ opinions of e-learning as one the main modalities of delivering medical education and its potential use in the future.
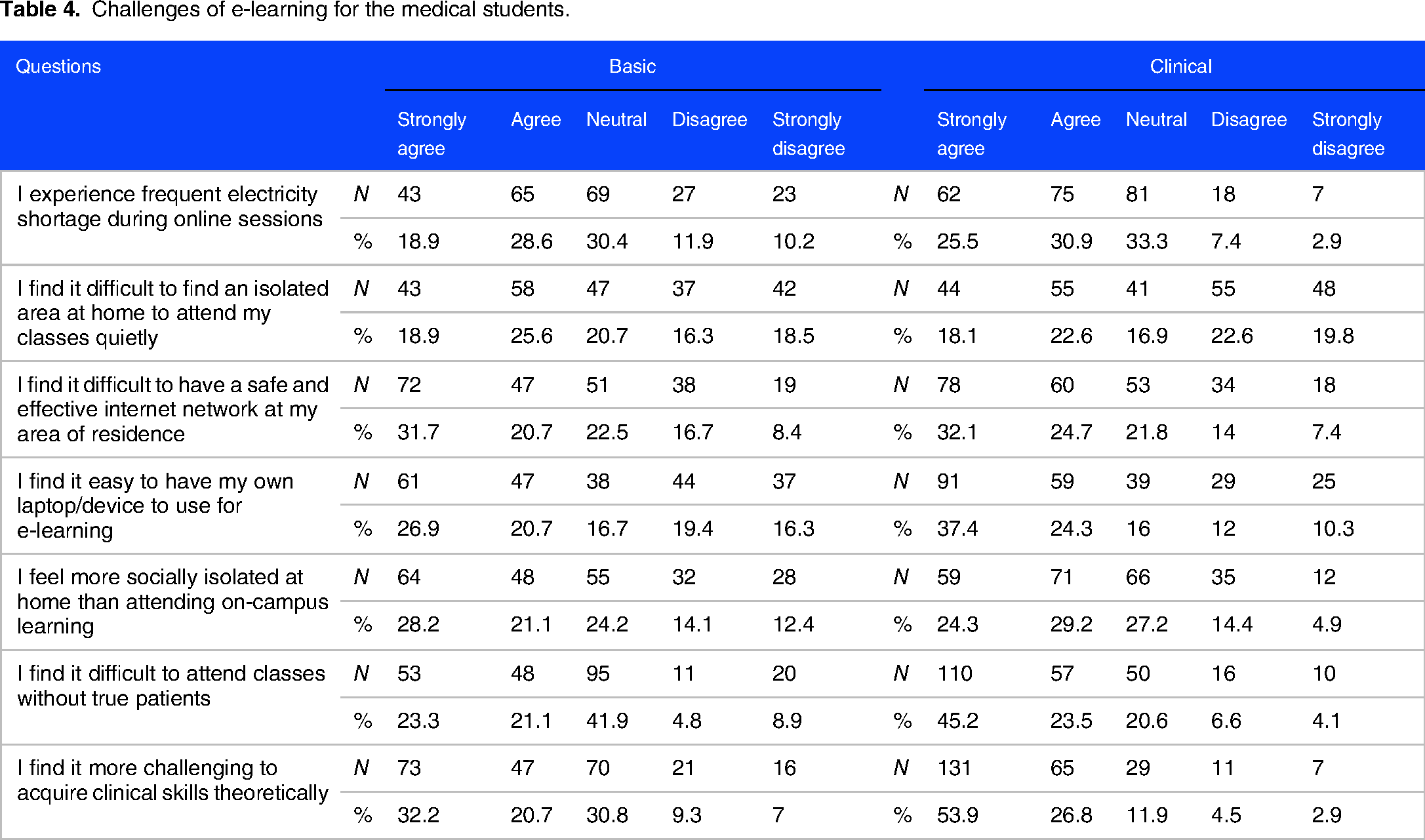
Challenges of online learning reported by the students are shown in Table 4. Challenges were related mainly to current poor socioeconomic conditions in Gaza, which manifest as chronic electricity shortages and cuts, inability to afford personal computer/device for each student, poor internet infrastructure and connectivity, and crowdedness in the household preventing students from having a personal space at home. Understandably, more clinical-level students (n = 196, 80%) agreed or strongly agreed that lacking practical skills is a challenge they face, followed by lack of interactions with real patients (n = 167, 68.7%). Lack of such interaction impedes their ability to completely benefit from online classes. As for basic-level students, more students (n = 120, 52.8%) reported lack of practical skills (eg, lab skills) as a challenge, followed by unreliable internet access (n = 119, 52.4%). Electricity shortage and prolonged cuts were still a main challenge reported by both levels as a considerable number agreed or strongly agreed that this is a challenge they face (n = 245, 52.1%).
Challenges of e-learning for the medical students.
Discussion
This study aimed to understand medical students’ experiences and perspectives in the Gaza Strip on receiving medical education online during the COVID-19 pandemic. E-learning was adopted as the learning platform during the pandemic in the Palestinian medical schools, and this was the first time it was used. We found that medical students significantly increased their time spent on online educational software and resources despite a variety of socio-economic and logistic challenges facing them. Students’ perspectives differed in terms of their ability to effectively interact with online education and their capability of using the online educational platforms. As well, there was no consensus among students on the effectiveness of e-learning as a future learning platform, the challenges and obstacles they faced in the virtual learning and their overall satisfaction on e-learning during COVID-19 pandemic.
In the last two decades, medical education has benefited from digital technology and had adopted new learning strategies such as virtual meetings and interactive simulations labs. Harnessing technology in the field of education is believed to enrich the educational process and make it more effective. 8 Indeed, technology-based learning in some medical disciplines such as anatomy was found to be more useful and effective than traditional one. 9 This goes in line with the perspective of some of our population, which reported finding online learning more flexible and less stressful, both elements potentially contributing to an effective educational process. An initiative from Oxford University targeting medical students in Gaza utilizing online education found this method to be effective and received positive feedback from the students. 10
Distance learning added flexibility to the educational process as students can learn vast amounts of knowledge without the need to travel. Moreover, it allowed the educational process to be personalized; students have more control over the learning pace time, contents and sequence.11,12 Our study demonstrated that the most reported advantage of e-learning is the ease of access, especially to asynchronous forms of e-learning, such as prerecorded lectures, as students can repeatedly watch lectures and other educational material as many times as they need. Other advantages for shifting to e-learning for both basics and clinical years include saving transportation fees, flexibility, and ability to learn comfortably while at home.
Synchronous, interactive and two-way learning is more effective to enhance self-motivation and communications with teachers and peers. 13 When students are actively involved in the educational process, they tend to be more motivated to engage with the teachers and engage actively. 14 The interaction between teacher and student along with face to face and emotional support are essential elements for effective learning. 15 The findings from our study reflected these sentiments as students from both basic- and clinical-level highly reported as a negative aspect of e-learning the lack of effective communication and engagement with lecturers.
The lack of technology, infrastructure, electricity cuts and poor quality of internet services are barriers that impact both students and teachers. 16 In Gaza Strip, students reported the impact of economic depression and logistics shortage on their ability to access e-learning. Frequent electricity shortage during online sessions and the difficulty to have a reliable internet connection at home were among the most reported challenges to e-learning. Furthermore, the inability of families to secure a device for each student in the household was yet another hurdle to accessing e-learning that is secondary to the economic and logistics conditions.
In this study, more than 50% of all students reported their unwillingness to continue online learning as they are reluctant to accept e-learning as an essential part of medical teaching system. This reluctance can be attributed to a large extent to the poor socio-economic status and unreliable connectivity and infrastructure in the Gaza Strip which hinders e-learning. Also, the reason behind this could be explained by the findings that both basic- and clinical-level students admitted it is difficult to acquire clinical skills theoretically without real interaction with patients in real life. Despite their low level of satisfaction, they expect that distance e-learning can partially replace the traditional method in delivering theoretical but not clinical skills.
Limitations
The present study has several limitations owing to the nature of its methods. First, online surveys results in participants selection bias, 17 as participants with computer skills are more likely to participate in such surveys and therefore the findings of the survey may be biased as well. Second, the respondents to online surveys are anonymous, which makes it hard to describe them or know who actually filled the survey. For our study, we exclusively shared the survey in social media groups for medical students in the Gaza Strip. Moreover, the survey was open for only 10 days to decrease the chance of it being spread to other ineligible people who may pose as medical students in the survey.
We opted for convenience sampling in the study in order to obtain as many responses as possible from the students. We realize the convenience sampling present a limitation to the selection and representativeness of the larger population and may limit the generalizability of our findings. 18 However, given the small geographical size of the Gaza Strip and the largely similar characteristics of its inhabitants, in terms of beliefs, traditions, and socio-economic situation, we believe that this limitation may not be as concerning as it might be in other contexts.
A third limitation to our study is the low response rate. Around one out of four from the entire eligible population responded to our questionnaire. We realize this makes it hard to draw firm conclusions, especially when talking about experiences of nearly 2000 students. The low response rate, however, may be due to the challenges and difficulties in connectivity and accessing online platforms, which were described in the article. Also, the short period during which the questionnaire was available, for reasons discussed above, may have contributed to the low response rate.
Finally, we preferred to leave it up to each student to decide the level of their IT skills that allow them to access and navigate the online resources they need in order to achieve their individual educational goals. We felt that setting specific criteria for each level may not be fair to all students. We understand such subjective evaluation of skills may present a limitation to the findings as there were no reference points to such evaluation. However, we believe such subjectivity lends some strength to the findings by reflecting the honest and actual experiences of the students towards e-learning.
Policy Recommendations
In light of the findings of our study, we elaborated through an iterative discussion process among ourselves (comprising the two elements of the educational process: students and teachers) means to improve medical e-learning should it be implemented as part of the curriculum or as a solution to an emergency. The policy recommendations we offer below are actionable steps that are clear, and sometimes simple, and have the potential to significantly improve the experience of medical e-learning both for students and teachers. Moreover, by offering such recommendations, we intend to elicit the readers’ thinking, especially researchers and policymakers, into considering other relevant policies.
Conclusion
The emergence of COVID-19 in 2020 has forced considerable changes to all aspects of life, including all forms of educational processes at all levels. Medical education in Gaza was solely delivered face-to-face, and during COVID-19, it was mandatory to switch to e-learning for the first time to guarantee the continuation of the process. Although students managed to complete the academic year successfully, they were still reluctant to accept e-learning an essential part of medical education in the future. This was attributed in part to difficulty in interacting with teachers online and inability to apply clinical knowledge on real patients. The main challenges leading to such reluctance are related to poor living conditions in Gaza with frequent electricity cuts, poor internet infrastructure, inability of students to get personal computer and many others. This mandates a multidisciplinary cooperation between different institutions nationally and internationally to mitigate the impacts of the aforementioned problems should COVID-19 persist and e-learning continue to constitute a main method to deliver medical education in Gaza.
Supplemental Material
sj-pdf-1-mde-10.1177_23821205231164228 - Supplemental material for E-Learning Medical Education in Gaza During COVID-19: Students’ Experiences and Policy Recommendations
Supplemental material, sj-pdf-1-mde-10.1177_23821205231164228 for E-Learning Medical Education in Gaza During COVID-19: Students’ Experiences and Policy Recommendations by Alaa Ismail, Anas Ismail, Ameera Alazar, Mosab Saman, Ayham Abu-Elqomboz and Fawzi Khalil Sharaf in Journal of Medical Education and Curricular Development
Footnotes
Acknowledgements
The authors wish to thank all the students who took the time to participate in the study and fill out the questionnaire.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.